
Analysis of Potential Vitamin D Molecule Biomarkers: Association of Calcitriol and Its Hydroxylation Efficiency Ratio with Cardiovascular Disease Risk in Rheumatoid Arthritis Patients
 , , , , , , ,
, , , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. RA Clinical Disease Activity Indexes
2.3. Quantification of Calcidiol, Calcitriol, sVDR, CRP, and Biochemical Variables
2.4. Vitamin D Molecules Cutoff Values and CVD Risk Criteria Classification
2.5. Statistical Analysis
3. Results
3.1. Anthropometric, Biochemical, and Clinical Variables in RA and HS
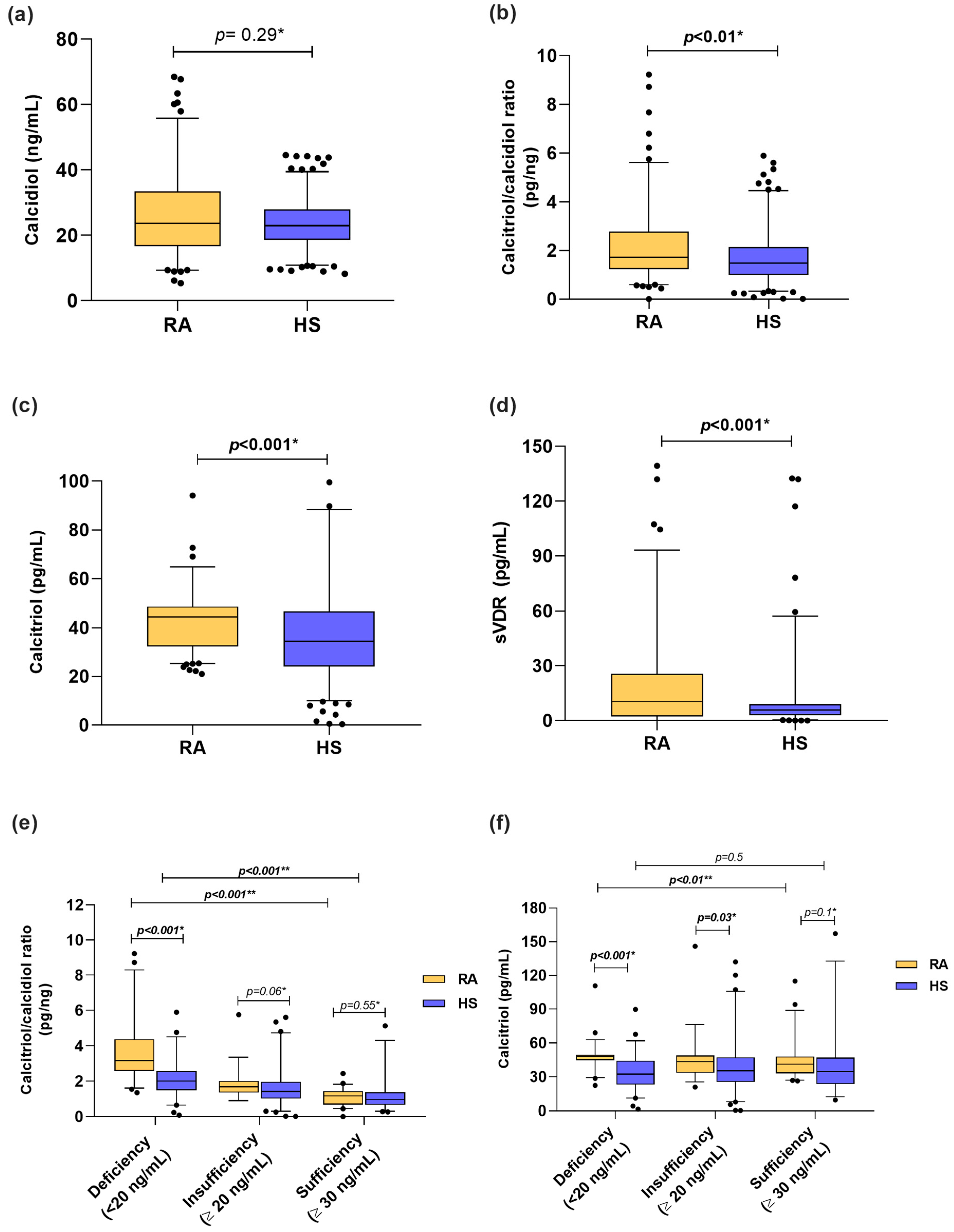
3.2. Vitamin D Molecules in RA Patients and HS
3.3. Anthropometric, Biochemical, Clinical Variables, and Vitamin D Metabolites Stratified by sVDR Tertiles
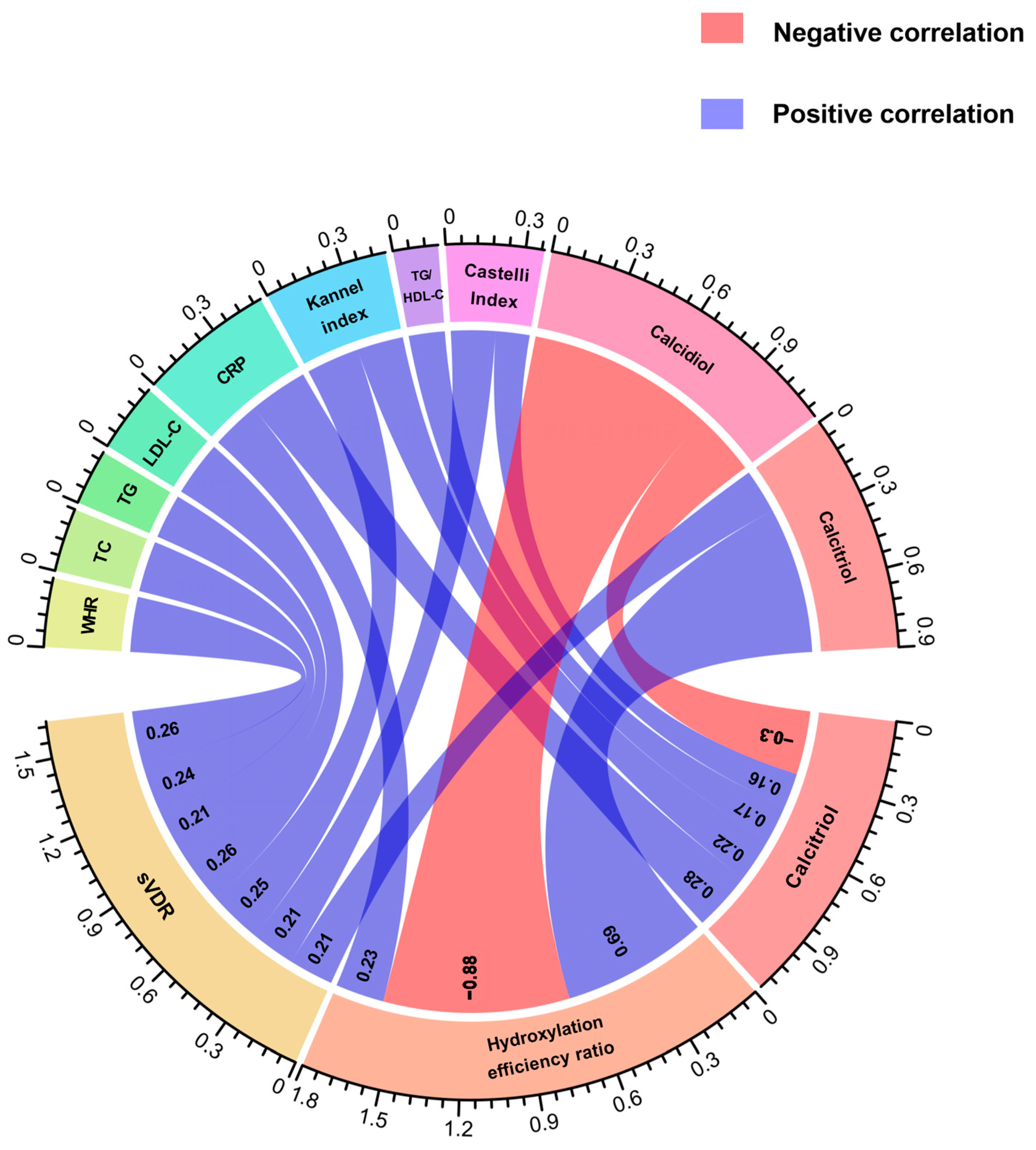
3.4. Correlations between Vitamin D Molecules with Anthropometrical, Biochemical, and Clinical Variables in RA Patients and HS
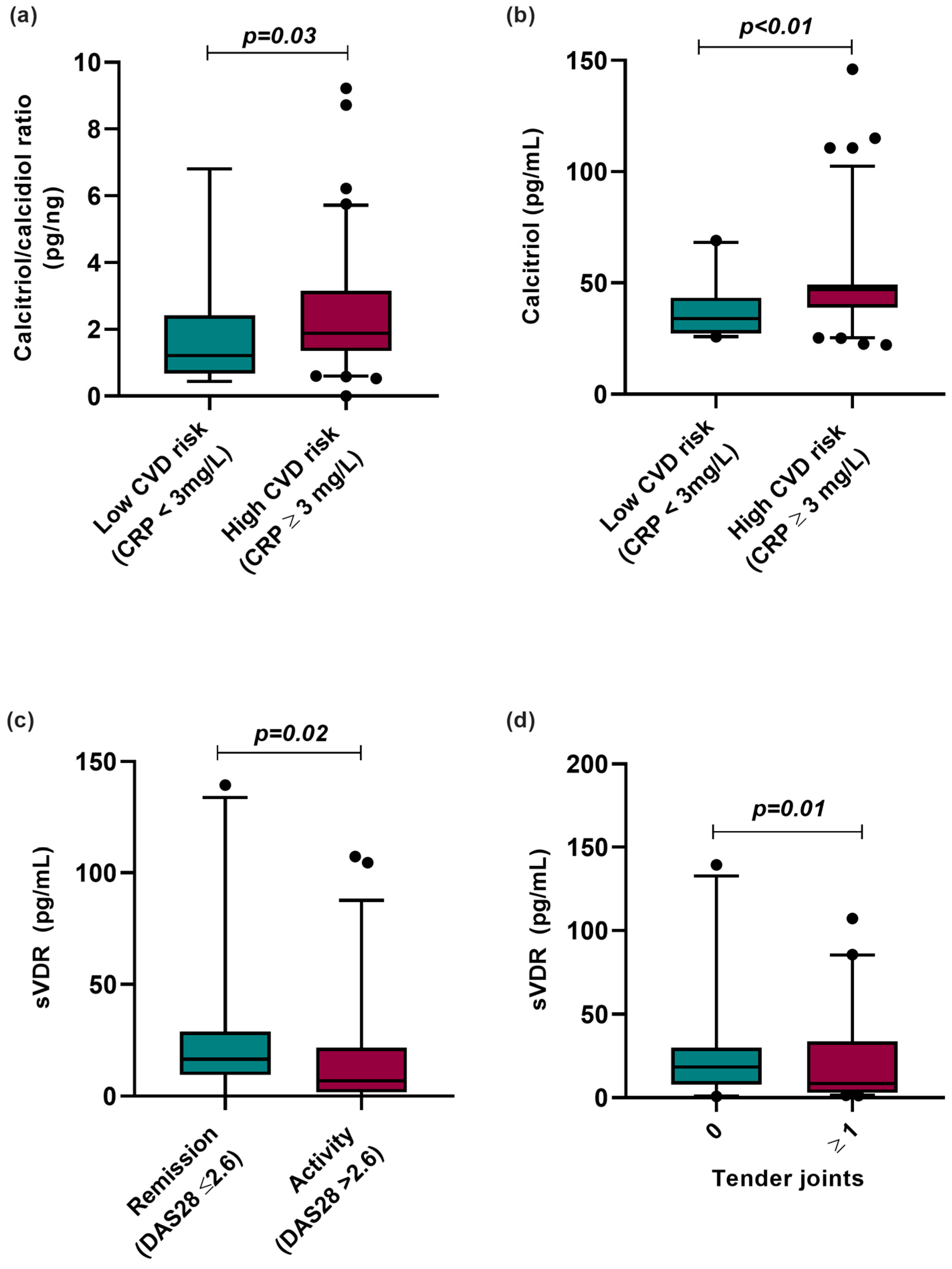
3.5. Vitamin D Molecules Stratified by CVD Risk and Clinical Variables
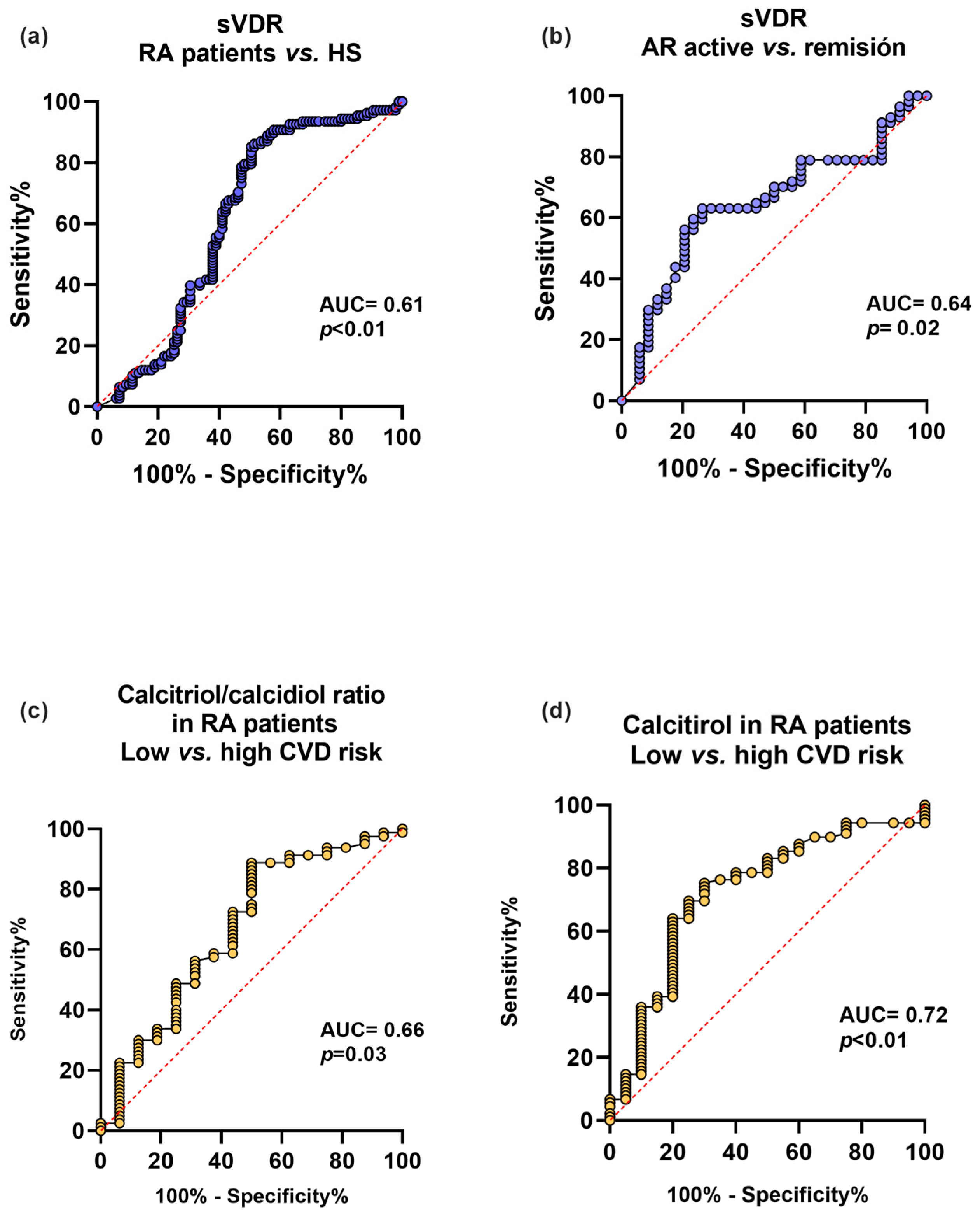
3.6. Associations of Potential Vitamin D Molecules Biomarkers with RA Disease and CVD Risk in RA Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; Barton, A.; Burmester, G.R.; Emery, P.; Firestein, G.S.; Kavanaugh, A.; McInnes, I.B.; Solomon, D.H.; Strand, V.; et al. Rheumatoid arthritis. Nat. Rev. Dis. Primers 2018, 4, 18001. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, M.; Farrell, C.-J.L.; Pusceddu, I.; Fabregat-Cabello, N.; Cavalier, E. Assessment of vitamin D status—A changing landscape. Clin. Chem. Lab. Med. (CCLM) 2017, 55, 3–26. [Google Scholar] [CrossRef] [PubMed]
- Alonso, N.; Zelzer, S.; Eibinger, G.; Herrmann, M. Vitamin D Metabolites: Analytical Challenges and Clinical Relevance. Calcif. Tissue Int. 2022, 112, 158–177. [Google Scholar] [CrossRef] [PubMed]
- Athanassiou, L.; Kostoglou-Athanassiou, I.; Koutsilieris, M.; Shoenfeld, Y. Vitamin D and Autoimmune Rheumatic Diseases. Biomolecules 2023, 13, 709. [Google Scholar] [CrossRef] [PubMed]
- De La Guía-Galipienso, F.; Martínez-Ferran, M.; Vallecillo, N.; Lavie, C.J.; Sanchis-Gomar, F.; Pareja-Galeano, H. Vitamin D and cardiovascular health. Clin. Nutr. 2021, 40, 2946–2957. [Google Scholar] [CrossRef]
- Wang, L.; Song, Y.; Manson, J.E.; Pilz, S.; März, W.; Michaëlsson, K.; Lundqvist, A.; Jassal, S.K.; Barrett-Connor, E.; Zhang, C.; et al. Circulating 25-Hydroxy-Vitamin D and Risk of Cardiovascular Disease: A Meta-Analysis of Prospective Studies. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 819–829. [Google Scholar] [CrossRef]
- Parker, J.; Hashmi, O.; Dutton, D.; Mavrodaris, A.; Stranges, S.; Kandala, N.-B.; Clarke, A.; Franco, O.H. Levels of vitamin D and cardiometabolic disorders: Systematic review and meta-analysis. Maturitas 2010, 65, 225–236. [Google Scholar] [CrossRef]
- Zhang, R.; Li, B.; Gao, X.; Tian, R.; Pan, Y.; Jiang, Y.; Gu, H.; Wang, Y.; Wang, Y.; Liu, G. Serum 25-hydroxyvitamin D and the risk of cardiovascular disease: Dose-response meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 810–819. [Google Scholar] [CrossRef]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O.; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of Inflammation and Cardiovascular Disease: Application to Clinical and Public Health Practice: A Statement for Healthcare Professionals From the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef]
- Pope, J.E.; Choy, E.H. C-reactive protein and implications in rheumatoid arthritis and associated comorbidities. Semin. Arthritis Rheum. 2021, 51, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Wulandari, D.; Barlianto, W.; Sari, T.L. Low Level of Vitamin D is Correlated with High C-Reactive Protein (CRP) and Disease Activity in Indonesian Juvenile Idiopathic Arthritis (JIA) Patients. Indones. Biomed. J. 2020, 12, 149–156. [Google Scholar] [CrossRef]
- Jorde, R.; Grimnes, G. Vitamin D and metabolic health with special reference to the effect of vitamin D on serum lipids. Prog. Lipid Res. 2011, 50, 303–312. [Google Scholar] [CrossRef]
- Meza-Meza, M.R.; Muñoz-Valle, J.F.; Ruiz-Ballesteros, A.I.; Vizmanos-Lamotte, B.; Parra-Rojas, I.; Martínez-López, E.; Oregon-Romero, E.; Márquez-Sandoval, Y.F.; Cerpa-Cruz, S.; de la Cruz-Mosso, U. Association of High Calcitriol Serum Levels and Its Hydroxylation Efficiency Ratio with Disease Risk in SLE Patients with Vitamin D Deficiency. J. Immunol. Res. 2021, 2021, 2808613. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghafari, A.B.; Balamash, K.S.; Al Doghaither, H.A. Serum vitamin D receptor (VDR) levels as a potential diagnostic marker for colorectal cancer. Saudi J. Biol. Sci. 2020, 27, 827–832. [Google Scholar] [CrossRef]
- Altun, H.; Kurutaş, E.B.; Şahin, N.; Güngör, O.; Fındıklı, E. The Levels of Vitamin D, Vitamin D Receptor, Homocysteine and Complex B Vitamin in Children with Autism Spectrum Disorders. Clin. Psychopharmacol. Neurosci. 2018, 16, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Tekeli, S.Ö.; Yağmur Tekeli, F.; Erol, O.; Ellidag, H.Y.; Eren, E.; Yılmaz, N. Serum vitamin D receptor levels in gestational diabetes mellitus. LaboratoriumsMedizin 2018, 42, 149–154. [Google Scholar] [CrossRef]
- Börekci, E.; Kılıç, M.; Ozan, Z.; Börekci, H.; Yıldırım, T.; Göçmen, Y.; Baş, H. Increased vitamin D binding protein levels are associated with irritable bowel syndrome. Turk. J. Biochem. 2021, 46, 415–424. [Google Scholar] [CrossRef]
- Kültür, T. The relationship of serum vitamin D receptor levels with disease activity and clinical parameters in patients with ankylosing spondylitis. Turk. J. Phys. Med. Rehab. 2019, 65, 389–393. [Google Scholar] [CrossRef]
- Meza-Meza, M.R.; Ruiz-Ballesteros, A.I.; de la Cruz-Mosso, U. Functional effects of vitamin D: From nutrient to immunomodulator. Crit. Rev. Food Sci. Nutr. 2022, 62, 3042–3062. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef]
- Wells, G.; Becker, J.-C.; Teng, J.; Dougados, M.; Schiff, M.; Smolen, J.; Aletaha, D.; Van Riel, P.L.C.M. Validation of the 28-joint Disease Activity Score (DAS28) and European League Against Rheumatism response criteria based on C-reactive protein against disease progression in patients with rheumatoid arthritis, and comparison with the DAS28 based on erythrocyte sedimentation rate. Ann. Rheum. Dis. 2009, 68, 954–960. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Pasquali, M.; Tartaglione, L.; Rotondi, S.; Muci, M.L.; Mandanici, G.; Farcomeni, A.; Marangella, M.; Mazzaferro, S. Calcitriol/calcifediol ratio: An indicator of vitamin D hydroxylation efficiency? BBA Clin. 2015, 3, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Campos-López, B.; Meza-Meza, M.R.; Parra-Rojas, I.; Ruiz-Ballesteros, A.I.; Vizmanos-Lamotte, B.; Muñoz-Valle, J.F.; Montoya-Buelna, M.; Cerpa-Cruz, S.; Bernal-Hernández, L.E.; De la Cruz-Mosso, U. Association of cardiometabolic risk status with clinical activity and damage in systemic lupus erythematosus patients: A cross-sectional study. Clin. Immunol. 2021, 222, 108637. [Google Scholar] [CrossRef] [PubMed]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed]
- Azzeh, F.S.; Kensara, O.A. Vitamin D Is a Good Marker for Disease Activity of Rheumatoid Arthritis Disease. Dis. Markers 2015, 2015, 260725. [Google Scholar] [CrossRef] [PubMed]
- Meena, N.; Singh Chawla, S.; Garg, R.; Batta, A.; Kaur, S. Assessment of Vitamin D in rheumatoid arthritis and its correlation with disease activity. J. Nat. Sci. Biol. Med. 2018, 9, 54. [Google Scholar] [CrossRef]
- Barnes, P.F.; Modlin, R.L.; Bikle, D.D.; Adams, J.S. Transpleural gradient of 1,25-dihydroxyvitamin D in tuberculous pleuritis. J. Clin. Investig. 1989, 83, 1527–1532. [Google Scholar] [CrossRef]
- Anisiewicz, A.; Łabędź, N.; Krauze, I.; Wietrzyk, J. Calcitriol in the Presence of Conditioned Media from Metastatic Breast Cancer Cells Enhances Ex Vivo Polarization of M2 Alternative Murine Bone Marrow-Derived Macrophages. Cancers 2020, 12, 3485. [Google Scholar] [CrossRef]
- Zenata, O.; Vrzal, R. Fine tuning of vitamin D receptor (VDR) activity by post-transcriptional and post-translational modifications. Oncotarget 2017, 8, 35390–35402. [Google Scholar] [CrossRef]
- Zmijewski, M.A.; Carlberg, C. Vitamin D receptor(s): In the nucleus but also at membranes? Exp. Dermatol. 2020, 29, 876–884. [Google Scholar] [CrossRef]
- Pesqueda-Cendejas, K.; Parra-Rojas, I.; Mora-García, P.E.; Montoya-Buelna, M.; Ruiz-Ballesteros, A.I.; Meza-Meza, M.R.; Campos-López, B.; Rivera-Escoto, M.; Vizmanos-Lamotte, B.; Cerpa-Cruz, S.; et al. CRP Serum Levels Are Associated with High Cardiometabolic Risk and Clinical Disease Activity in Systemic Lupus Erythematosus Patients. JCM 2022, 11, 1849. [Google Scholar] [CrossRef]
- Chung, C.P.; Giles, J.T.; Kronmal, R.A.; Post, W.S.; Gelber, A.C.; Petri, M.; Szklo, M.; Detrano, R.; Budoff, M.J.; Blumenthal, R.S.; et al. Progression of coronary artery atherosclerosis in rheumatoid arthritis: Comparison with participants from the Multi-Ethnic Study of Atherosclerosis. Arthritis Res. Ther. 2013, 15, R134. [Google Scholar] [CrossRef]
- Avina-Zubieta, J.A.; Thomas, J.; Sadatsafavi, M.; Lehman, A.J.; Lacaille, D. Risk of incident cardiovascular events in patients with rheumatoid arthritis: A meta-analysis of observational studies. Ann. Rheum. Dis. 2012, 71, 1524–1529. [Google Scholar] [CrossRef]
- Saghir Afifeh, A.M.; Verdoia, M.; Nardin, M.; Negro, F.; Viglione, F.; Rolla, R.; De Luca, G. Determinants of vitamin D activation in patients with acute coronary syndromes and its correlation with inflammatory markers. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 36–43. [Google Scholar] [CrossRef]
- Zittermann, A.; Schleithoff, S.S.; Frisch, S.; Götting, C.; Kuhn, J.; Koertke, H.; Kleesiek, K.; Tenderich, G.; Koerfer, R. Circulating Calcitriol Concentrations and Total Mortality. Clin. Chem. 2009, 55, 1163–1170. [Google Scholar] [CrossRef]
- Klaus, G.; May, T.; Hügel, U.; Von Eichel, B.; Rodriguez, J.; Fernandez, P.; Reichrath, J.; Ritz, E.; Mehls, O. Parathyroid hormone prevents 1,25(OH)2D3 induced down-regulation of the vitamin D receptor in growth plate chondrocytes in vitro. Kidney Int. 1997, 52, 45–51. [Google Scholar] [CrossRef]
- Wu, J.; Garami, M.; Cheng, T.; Gardner, D.G. 1,25(OH)2 vitamin D3, and retinoic acid antagonize endothelin-stimulated hypertrophy of neonatal rat cardiac myocytes. J. Clin. Investig. 1996, 97, 1577–1588. [Google Scholar] [CrossRef]
- Bossard, M.; Pumpol, K.; Van Der Lely, S.; Aeschbacher, S.; Schoen, T.; Krisai, P.; Lam, T.; Todd, J.; Estis, J.; Risch, M.; et al. Plasma endothelin-1 and cardiovascular risk among young and healthy adults. Atherosclerosis 2015, 239, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D Deficiency and Risk of Cardiovascular Disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef]
- Ziv, E.; Koren, R.; Zahalka, M.A.; Ravid, A. TNF-α increases the expression and activity of vitamin D receptor in keratinocytes: Role of c-Jun N-terminal kinase. Derm.-Endocrinol. 2016, 8, e1137399. [Google Scholar] [CrossRef] [PubMed]
- Pojednic, R.M.; Ceglia, L.; Lichtenstein, A.H.; Dawson-Hughes, B.; Fielding, R.A. Vitamin D receptor protein is associated with interleukin-6 in human skeletal muscle. Endocrine 2015, 49, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, M.; Gangestad, S.W. Rethinking IL-6 and CRP: Why they are more than inflammatory biomarkers, and why it matters. Brain Behav. Immun. 2018, 70, 61–75. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | RA Patients (n = 154) | HS (n = 201) | p-Value |
|---|---|---|---|
| Age (years) a | 35 (19–59) | 48 (27–65) | <0.001 |
| Height(cm) b | 1.57 ± 0.05 | 1.61 ± 0.06 | <0.01 |
| Weight (kg) a | 67.3 (48.9–93.4) | 62.5 (47.7–86.7) | <0.01 |
| BMI (kg/m2) a | 27.48 (19.78–36.27) | 24.06 (18.75–34.89) | <0.001 |
| Waist circumference (cm) a | 87.7 (69–108) | 77.7 (61.5–105) | <0.001 |
| Hip circumference (cm) a | 103.5 (88–127) | 100 (88.2–119.2) | <0.01 |
| WHR a | 0.84 (0.74–0.98) | 0.77 (0.68–0.93) | <0.001 |
| Glucose (mg/dL) a | 88 (72.58–127) | 88.44 (75.14–114.23) | 0.24 |
| Albumin (g/dL) a | 3.91 (3.25–4.48) | 3.81 (3.39–4.42) | <0.05 |
| Triglycerides (mg/dL) a | 96.72 (44.65–195) | 76.63 (39.41–198.72) | <0.001 |
| Cholesterol (mg/dL) a | 169.5 (114–237) | 174.46 (125.25–243.82) | 0.17 |
| HDL-C (mg/dL) a | 49.2 (30.1–76.24) | 51.34 (35.28–75.93) | 0.07 |
| LDL-C (mg/dL) a | 94.39 (55.37–147.14) | 95.23 (61.61–157.25) | 0.22 |
| Disease duration (years) a | 6.5 (1–22) | ||
| DAS28 (CRP) a | 3.07 (1.46–5.83) | - | - |
| DAS28 (ESR) b | 3.7 ± 1.3 | - | - |
| Tender joints a | 0.5 (0–10) | - | - |
| Swollen joints a | 1.5 (0–12) | - | - |
| Remission (DAS28-CRP ≤ 2.6) c | 36 (51/142) | - | - |
| Activity (DAS28-CRP > 2.6) c | 64 (91/142) | - | - |
| Hs-CRP (mg/L) a | 4.4 (0.5–29.42) | 1.19 (0–12.4) | <0.001 |
| ESR (mm/h) a | 35.5 (8–79) | - | - |
| ACPAs (UI/mL) a | 208 (13.4–289) | - | - |
| RF (UI/mL) a | 114 (11–500) | - | - |
| Vitamin D Molecules | RA Patients vs. HS | CVD Risk (CRP ≥ 3 mg/L) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Without Adjusted | Multiple Models ∞ | Without Adjusted | Multiple Models ∞ | |||||||
| % (n) | OR (CI 95%) | p-Value | OR (CI 95%) | p-Value | OR (CI 95%) | p-Value | OR (CI 95%) | p-Value | ||
| Calcidiol (ng/mL) | Deficiency * | 36 (36) | 1 | - | 1 | - | 1 | - | 1 | - |
| Insufficiency | 15 (15) | 0.65 (0.38–0.79) | 0.11 | 0.73 (0.41–1.3) | 0.29 | 0.7 (0.18–2.77) | 0.6 | 0.8 (0.21–3.36) | 0.8 | |
| Sufficiency | 48 (48) | 1.63 (0.92–2.87) | 0.09 | 1.6 (0.91–3.13) | 0.09 | 0.67 (0.18–2.47) | 0.55 | 0.8 (0.21–3.39) | 0.8 | |
| Calcitriol/calcidiol ratio (pg/ng) | Low * | 26 (34) | 1 | - | 1 | - | 1 | - | 1 | - |
| Mild | 34 (43) | 1.28 (0.73–2.26) | 0.38 | 1.76 (0.95–3.31) | 0.07 | 3.37 (0.87–13.02) | 0.07 | 3.58 (0.86–14.9) | 0.08 | |
| High | 40 (51) | 1.90 (1.08–3.35) | 0.02 | 2.02 (1.09–3.75) | 0.02 | 4.62 (1.22–17.6) | 0.03 | 4.51 (1.09–18.6) | 0.04 | |
| Calcitriol (pg/mL) | Low * | 35 (50) | 1 | - | 1 | - | 1 | - | 1 | - |
| Mild | 30 (43) | 2.4 (1.18–3.5) | 0.01 | 2.68 (1.45–4.98) | <0.01 | 3.9 (1.08–14.14) | 0.04 | 4.02 (1.09–14.7) | 0.04 | |
| High | 35 (51) | 2.73 (1.59–4.69) | <0.001 | 2.95 (1.62–5.39) | <0.001 | 5.8 (1.63–20.6) | <0.01 | 5.6 (1.49–21) | 0.01 | |
| sVDR (pg/mL) | Low * | 36 (36) | 1 | - | 1 | - | 1 | - | 1 | - |
| Mild | 15 (15) | 0.4 (0.18–0.79) | <0.01 | 0.98 (0.38–2.48) | 0.97 | - | - | - | - | |
| High | 48 (48) | 3.75 (1.83–7.7) | <0.001 | 5.57 (2.23–13.9) | <0.001 | 5.3 (0.93–30.1) | 0.06 | 8.43 (1.08–65.4) | 0.04 | |
| Without Adjusted | Multiple Models 1 | |||
|---|---|---|---|---|
| ◊ β (95% CI) | p-Value * | β (95% CI) | p-Value * | |
| RA disease | ||||
| Calcidiol (ng/mL) | 2.89 (0.56–5.23) | 0.01 | 2.84 (0.32–5.37) | 0.03 |
| Calcitriol/calcidiol ratio (pg/ng) | 0.45 (0.04–0.85) | 0.03 | 0.31 (−0.11–0.75) | 0.15 |
| Calcitriol (pg/mL) | 2.53 (−5.8–10.87) | 0.55 | −0.62 (−9.73–8.49) | 0.89 |
| sVDR (pg/mL) | 14.39 (−27.06–55.86) | 0.49 | 29.77 (−22.89–82.44) | 0.26 |
| CVD risk (CRP ≥ 3 mg/L) | ||||
| Calcidiol (ng/mL) | −5.9 (−13.5–1.66) | 0.12 | −6.1 (−13.6–1.45) | 0.11 |
| Calcitriol/calcidiol ratio (pg/ng) | 0.69 (−0.21–1.59) | 0.13 | 0.71 (−0.20–1.63) | 0.13 |
| Calcitriol (pg/mL) | 10.74 (1.84–19.65) | 0.02 | 11.56 (2.56–20.55) | 0.01 |
| sVDR (pg/mL) | 35.34 (−71.7–142.47) | 0.51 | 47.69 (−64.55–159.94) | 0.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera-Escoto, M.; Campos-López, B.; Pesqueda-Cendejas, K.; Ruiz-Ballesteros, A.I.; Mora-García, P.E.; Meza-Meza, M.R.; Parra-Rojas, I.; Oregon-Romero, E.; Cerpa-Cruz, S.; De la Cruz-Mosso, U. Analysis of Potential Vitamin D Molecule Biomarkers: Association of Calcitriol and Its Hydroxylation Efficiency Ratio with Cardiovascular Disease Risk in Rheumatoid Arthritis Patients. Biomedicines 2024, 12, 273. https://doi.org/10.3390/biomedicines12020273
Rivera-Escoto M, Campos-López B, Pesqueda-Cendejas K, Ruiz-Ballesteros AI, Mora-García PE, Meza-Meza MR, Parra-Rojas I, Oregon-Romero E, Cerpa-Cruz S, De la Cruz-Mosso U. Analysis of Potential Vitamin D Molecule Biomarkers: Association of Calcitriol and Its Hydroxylation Efficiency Ratio with Cardiovascular Disease Risk in Rheumatoid Arthritis Patients. Biomedicines. 2024; 12(2):273. https://doi.org/10.3390/biomedicines12020273
Chicago/Turabian StyleRivera-Escoto, Melissa, Bertha Campos-López, Karen Pesqueda-Cendejas, Adolfo I. Ruiz-Ballesteros, Paulina E. Mora-García, Mónica R. Meza-Meza, Isela Parra-Rojas, Edith Oregon-Romero, Sergio Cerpa-Cruz, and Ulises De la Cruz-Mosso. 2024. "Analysis of Potential Vitamin D Molecule Biomarkers: Association of Calcitriol and Its Hydroxylation Efficiency Ratio with Cardiovascular Disease Risk in Rheumatoid Arthritis Patients" Biomedicines 12, no. 2: 273. https://doi.org/10.3390/biomedicines12020273
APA StyleRivera-Escoto, M., Campos-López, B., Pesqueda-Cendejas, K., Ruiz-Ballesteros, A. I., Mora-García, P. E., Meza-Meza, M. R., Parra-Rojas, I., Oregon-Romero, E., Cerpa-Cruz, S., & De la Cruz-Mosso, U. (2024). Analysis of Potential Vitamin D Molecule Biomarkers: Association of Calcitriol and Its Hydroxylation Efficiency Ratio with Cardiovascular Disease Risk in Rheumatoid Arthritis Patients. Biomedicines, 12(2), 273. https://doi.org/10.3390/biomedicines12020273