

Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge

Abstract
:1. Background
2. Methods
2.1. Data Collection, Patients—Ethics, Enrolment Criteria
2.2. Study Protocol
2.3. Ultrasonography
2.4. Statistical Analysis
3. Results
3.1. Change of Monitored Parameters during Hospitalization and Follow-Up
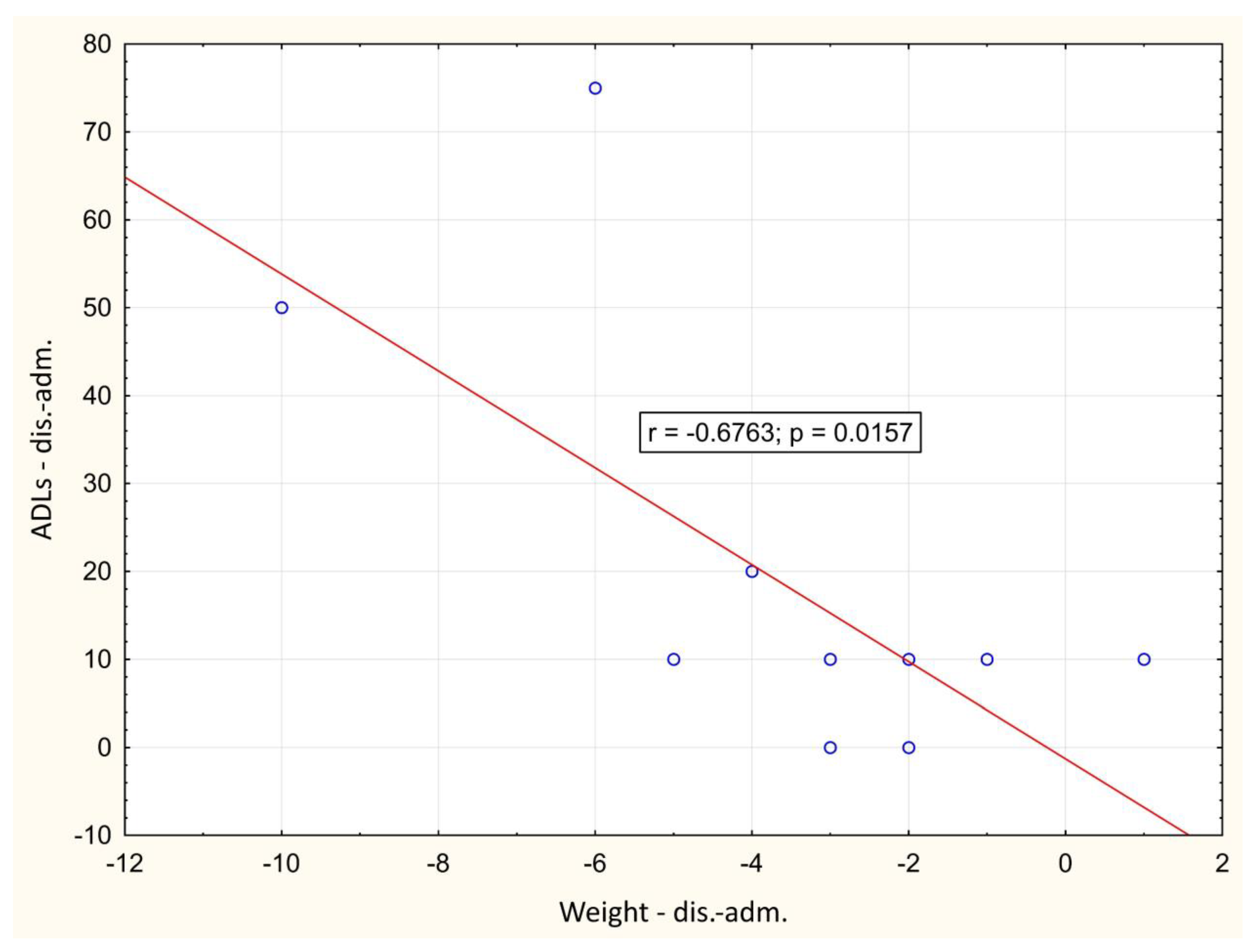
3.2. Correlation between Monitored Parameters
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Anka, A.U.; Tahir, M.I.; Abubakar, S.D.; Alsabbagh, M.; Zian, Z.; Hamedifar, H.; Sabzevari, A.; Azizi, G. Coronavirus disease 2019 (COVID-19): An overview of the immunopathology, serological diagnosis and management. Scand. J. Immunol. 2021, 93, e12998. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Li, X.; Gu, X.; Zhang, H.; Ren, L.; Guo, L.; Liu, M.; Wang, Y.; Cui, D.; Wang, Y.; et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: A longitudinal cohort study. Lancet Respir. Med. 2022, 10, 863–876. [Google Scholar] [CrossRef] [PubMed]
- Carod-Artal, F.J. Post-COVID-19 syndrome: Epidemiology, diagnostic criteria and pathogenic mechanisms involved. Rev. Neurol. 2021, 72, 384–396. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Malik, P.; Patel, K.; Pinto, C.; Jaiswal, R.; Tirupathi, R.; Pillai, S.; Patel, U. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)—A systematic review and meta-analysis. J. Med. Virol. 2022, 94, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, L.; De Lorenzo, R.; D’Amico, M.; Sofia, V.; Roveri, L.; Mele, R.; Saibene, A.; Rovere-Querini, P.; Conte, C. COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clin. Nutr. 2021, 40, 2420–2426. [Google Scholar] [CrossRef]
- Wierdsma, N.J.; Kruizenga, H.M.; Konings, L.A.; Krebbers, D.; Jorissen, J.R.; Joosten, M.-H.I.; van Aken, L.H.; Tan, F.M.; van Bodegraven, A.A.; Soeters, M.R.; et al. Poor nutritional status, risk of sarcopenia and nutrition related complaints are prevalent in COVID-19 patients during and after hospital admission. Clin. Nutr. ESPEN 2021, 43, 369–376. [Google Scholar] [CrossRef]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.-Y.; Bruyère, O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Looijaard, W.G.; Molinger, J.; Weijs, P.J. Measuring and monitoring lean body mass in critical illness. Curr. Opin. Crit. Care 2018, 24, 241–247. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.; Umbrello, M.; Pelosi, P.; Battaglini, D. Update on Lean Body Mass Diagnostic Assessment in Critical Illness. Diagnostics 2023, 13, 888. [Google Scholar] [CrossRef] [PubMed]
- Perkisas, S.; Bastijns, S.; Baudry, S.; Bauer, J.; Beaudart, C.; Beckwée, D.; Cruz-Jentoft, A.; Gasowski, J.; Hobbelen, H.; Jager-Wittenaar, H.; et al. Application of ultrasound for muscle assessment in sarcopenia: 2020 SARCUS update. Eur. Geriatr. Med. 2021, 12, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wu, J.; Gu, Q.; Gu, Y.; Zhao, Y.; Ge, X.; Sun, X.; Lian, J.; Zeng, Q. Changes in muscle ultrasound for the diagnosis of intensive care unit acquired weakness in critically ill patients. Sci. Rep. 2021, 11, 18280. [Google Scholar] [CrossRef] [PubMed]
- Tillquist, M.; Kutsogiannis, D.J.; Wischmeyer, P.E.; Kummerlen, C.; Leung, R.; Stollery, D.; Karvellas, C.J.; Preiser, J.; Bird, N.; Kozar, R.; et al. Bedside Ultrasound Is a Practical and Reliable Measurement Tool for Assessing Quadriceps Muscle Layer Thickness. J. Parenter. Enter. Nutr. 2013, 38, 886–890. [Google Scholar] [CrossRef] [PubMed]
- Hadda, V.; Kumar, R.; Khilnani, G.C.; Kalaivani, M.; Madan, K.; Tiwari, P.; Mittal, S.; Mohan, A.; Bhalla, A.S.; Guleria, R. Trends of loss of peripheral muscle thickness on ultrasonography and its relationship with outcomes among patients with sepsis. J. Intensive Care 2018, 6, 81. [Google Scholar] [CrossRef]
- Umbrello, M.; Guglielmetti, L.; Formenti, P.; Antonucci, E.; Cereghini, S.; Filardo, C.; Montanari, G.; Muttini, S. Qualitative and quantitative muscle ultrasound changes in patients with COVID-19–related ARDS. Nutrition 2021, 91–92, 111449. [Google Scholar] [CrossRef]
- Damanti, S.; Cilla, M.; Tuscano, B.; De Lorenzo, R.; Manganaro, G.; Merolla, A.; Pacioni, G.; Pomaranzi, C.; Tiraferri, V.; Martinenghi, S.; et al. Evaluation of Muscle Mass and Stiffness with Limb Ultrasound in COVID-19 Survivors. Front. Endocrinol. 2022, 13, 801133. [Google Scholar] [CrossRef]
- Martín, C.A.G.; Zepeda, E.M.; Méndez, O.A.L. Bedside Ultrasound Measurement of Rectus Femoris: A Tutorial for the Nutrition Support Clinician. J. Nutr. Metab. 2017, 2017, 2767232. [Google Scholar] [CrossRef]
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Padhke, R.; Dew, T.; Sidhu, P.S.; et al. Acute Skeletal Muscle Wasting in Critical Illness. JAMA 2013, 310, 1591–1600. [Google Scholar] [CrossRef] [PubMed]
- Koratala, A.; Ronco, C.; Kazory, A. Diagnosis of Fluid Overload: From Conventional to Contemporary Concepts. Cardiorenal Med. 2022, 12, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Moonen, H.P.F.X.; Van Zanten, A.R.H. Bioelectric impedance analysis for body composition measurement and other potential clinical applications in critical illness. Curr. Opin. Crit. Care 2021, 27, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Peolsson, A.; Hedlund, R.; Öberg, B. Intra-and inter-tester reliability and reference values for hand strength. J. Rehabil. Med. 2001, 33, 36–41. [Google Scholar] [CrossRef]
- Bittner, E.A.; Martyn, J.A.; George, E.; Frontera, W.R.; Eikermann, M. Measurement of muscle strength in the intensive care unit. Crit. Care Med. 2009, 37, S321–S330. [Google Scholar] [CrossRef] [PubMed]
- Cottereau, G.; Messika, J.; Megarbane, B.; Guérin, L.; da Silva, D.; Bornstain, C.; Santos, M.; Ricard, J.-D.; Sztrymf, B. Handgrip strength to predict extubation outcome: A prospective multicenter trial. Ann. Intensiv. Care 2021, 11, 144. [Google Scholar] [CrossRef]
- Mayer, K.P.; Bastin, M.L.T.; Montgomery-Yates, A.A.; Pastva, A.M.; Dupont-Versteegden, E.E.; Parry, S.M.; Morris, P.E. Acute skeletal muscle wasting and dysfunction predict physical disability at hospital discharge in patients with critical illness. Crit. Care 2020, 24, 637. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.N.; Eggelbusch, M.; Naddaf, E.; Gerrits, K.H.L.; van der Schaaf, M.; van den Borst, B.; Wiersinga, W.J.; van Vugt, M.; Weijs, P.J.M.; Murray, A.J.; et al. Skeletal muscle alterations in patients with acute Covid-19 and post-acute sequelae of Covid-19. J. Cachex. Sarcopenia Muscle 2022, 13, 11–22. [Google Scholar] [CrossRef]
- Sanaie, S.; Hosseini, M.-S.; Karrubi, F.; Iranpour, A.; Mahmoodpoor, A. Impact of Body Mass Index on the Mortality of Critically Ill Patients Admitted to the Intensive Care Unit: An Observational Study. Anesthesiol. Pain Med. 2020, 11, e108561. [Google Scholar] [CrossRef]
- Prescott, H.C.; Chang, V.W.; O’Brien, J.M., Jr.; Langa, K.M.; Iwashyna, T.J. Obesity and 1-Year Outcomes in Older Americans with Severe Sepsis. Crit. Care Med. 2014, 42, 1766–1774. [Google Scholar] [CrossRef]
- Akinnusi, M.E.; Pineda, L.A.; El Solh, A.A. Effect of obesity on intensive care morbidity and mortality: A meta-analysis. Crit. Care Med. 2008, 36, 151–158. [Google Scholar] [CrossRef]
- de Leeuw, A.J.M.; Luttikhuis, M.A.M.O.; Wellen, A.C.; Müller, C.; Calkhoven, C.F. Obesity and its impact on COVID-19. J. Mol. Med. 2021, 99, 899–915. [Google Scholar] [CrossRef] [PubMed]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef]
- Bivona, G.; Agnello, L.; Ciaccio, M. Biomarkers for Prognosis and Treatment Response in COVID-19 Patients. Ann. Lab. Med. 2021, 41, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Paces, J.; Strizova, Z.; Smrz, D.; Cerny, J. COVID-19 and the Immune System. Physiol. Res. 2020, 69, 379–388. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The Role of Cytokines including Interleukin-6 in COVID-19 induced Pneumonia and Macrophage Activation Syndrome-Like Disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.; Huang, Y.; Guo, Y.; Yin, M.; Chen, X.; Xiao, L.; Deng, G. Association of inflammatory markers with the severity of COVID-19: A meta-analysis. Int. J. Infect. Dis. 2020, 96, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Annetta, M.G.; Pittiruti, M.; Silvestri, D.; Grieco, D.L.; Maccaglia, A.; La Torre, M.F.; Magarelli, N.; Mercurio, G.; Caricato, A.; Antonelli, M. Ultrasound assessment of rectus femoris and anterior tibialis muscles in young trauma patients. Ann. Intensive Care 2017, 7, 104. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.M.; Burtin, C.; Denehy, L.; Puthucheary, Z.A.; Bear, D. Ultrasound Evaluation of Quadriceps Muscle Dysfunction in Respiratory Disease. Cardiopulm. Phys. Ther. J. 2019, 30, 15–23. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 16) | |
|---|---|
| Sex | Male (n = 13), Female (n = 3) |
| Age (years) | 64 ± 9.5 |
| Length of hospital stay (days) | 15.9 ± 7.1 |
| Delay from symptoms onset to hospital admission (days) | 10.6 ± 3.4 |
| Weight (kg) | 96.83 ± 10.2 |
| BMI (kg m−2) | 29.93 ± 2.4 |
| Hand grip strength (N) | 35.13 ± 8.9 |
| US RF (mm) | 15.19 ± 3.9 |
| US RF+VI (mm) | 27.01 ± 6.3 |
| LBM (kg) | 66.66 ± 8.7 |
| EQ-5D | 57.50 ± 20.1 |
| ADLs | 82.92 ± 22.6 |
| CRP (mg/L) | 128.70 ± 51.6 |
| Albumin (g/L) | 28.52 ± 4 |
| NLR | 8.03 ± 2.8 |
| AVG (adm.) | AVG (dis.) | AVG (1. Check-Up) | AVG (2. Check-Up) | AVG (3. Check-Up) | |
|---|---|---|---|---|---|
| Weight (kg) | 96.83 ± 10.2 | 93.50 ± 9.92 * | 96.59 ± 9.58 * | 99.33 ± 10.55 | 100.28 ± 10.82 |
| BMI (kg m−2) | 29.93 ± 2.4 | 28.88 ± 2.4 * | 29.96 ± 2.17 * | 30.65 ± 2.25 | 31.29 ± 2.74 |
| Hand grip (N) | 35.13 ± 8.9 | 36.55 ± 6.7 | 39.67 ± 6.9 * | 41.59 ± 7.2 | 42.30 ± 7.0 |
| US RF (mm) | 15.19 ± 3.9 | 13.91 ± 2.8 * | 15.55 ± 2.6 * | 16.36 ± 2.5 | 16.87 ± 2.3 |
| US RF + VI (mm) | 27.01 ± 6.3 | 25.26 ± 5.3 * | 30.04 ± 5.7 * | 31.66 ± 5.5 | 32.04 ± 5.6 |
| LBM (kg) | 66.66 ± 8.7 | 64.66 ± 8.7 * | 67.05 ± 8.4 * | 68.66 ± 8.9 | 69.06 ± 9.5 |
| EQ-5D | 57.50 ± 20.1 | 72.08 ± 12.4 * | 79.58 ± 8.6 | 82.00 ± 11.0 | 84.92 ± 8.6 |
| ADLs | 82.92 ± 22.6 | 100.00 ± 0 * | 100.00 ± 0 | 100.00 ± 0 | 100.00 ± 0 |
| CRP (mg/L) | 128.70 ± 51.6 | 15.59 ± 26.2 * | 3.18 ± 2.0 | 10.86 ± 30.9 | 6.90 ± 17.3 |
| Albumin (g/L) | 28.52 ± 4 | 28.52 ± 7.1 | 44.23 ± 6.5 * | 46.39 ± 2.9 | 45.40 ± 2.4 |
| NLR | 8.03 ± 2.8 | 3.31 ± 2.6 * | 1.68 ± 1.0 | 1.87 ± 0.9 | 1.93 ± 0.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Psenicka, O.; Brutvan, T.; Kratky, J.; Krizova, J. Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge. Biomedicines 2024, 12, 460. https://doi.org/10.3390/biomedicines12020460
Psenicka O, Brutvan T, Kratky J, Krizova J. Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge. Biomedicines. 2024; 12(2):460. https://doi.org/10.3390/biomedicines12020460
Chicago/Turabian StylePsenicka, Otakar, Tomas Brutvan, Jan Kratky, and Jarmila Krizova. 2024. "Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge" Biomedicines 12, no. 2: 460. https://doi.org/10.3390/biomedicines12020460
APA StylePsenicka, O., Brutvan, T., Kratky, J., & Krizova, J. (2024). Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge. Biomedicines, 12(2), 460. https://doi.org/10.3390/biomedicines12020460