
What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art




Abstract
:1. Introduction
2. Methods
3. Basal Weekly Insulin
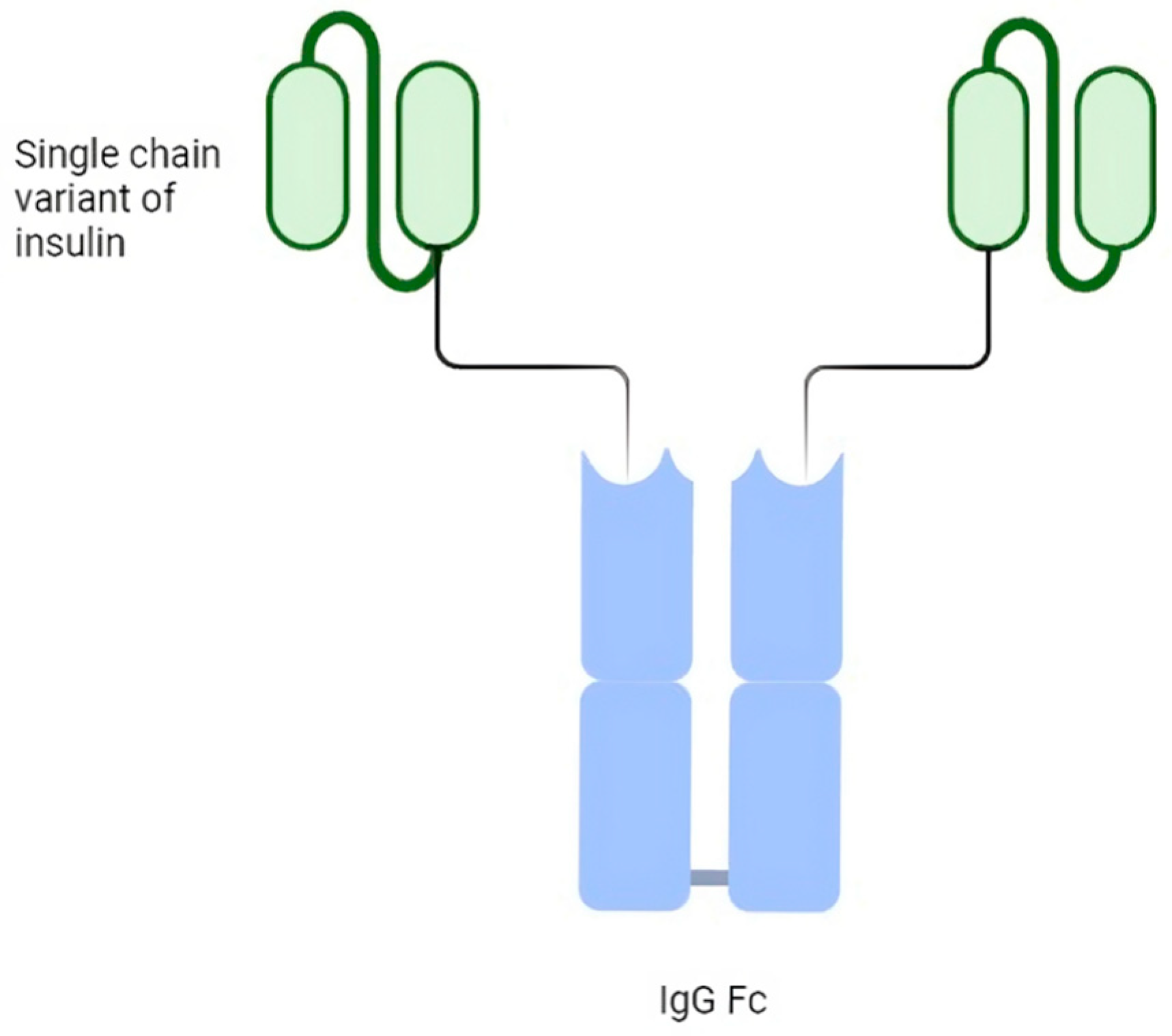
4. Basal Insulin Fc (BIF, LY3209590)
5. Insulin Icodec
6. Type 2 Diabetes Mellitus and Weekly Insulin
7. Type 1 Diabetes Mellitus and Weekly Insulin
8. Discussion
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ong, K.L.; Stafford, L.K.; McLaughlin, S.A.; Boyko, E.J.; Vollset, S.E.; Smith, A.E.; Dalton, B.E.; Duprey, J.; Cruz, J.A.; Hagins, H.; et al. Global, Regional, and National Burden of Diabetes from 1990 to 2021, with Projections of Prevalence to 2050: A Systematic Analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef] [PubMed]
- IDF Diabetes Atlas 2021 | IDF Diabetes Atlas. Available online: https://diabetesatlas.org/atlas/tenth-edition/ (accessed on 13 February 2024).
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Argano, C.; Natoli, G.; Mularo, S.; Nobili, A.; Monaco, M.L.; Mannucci, P.M.; Perticone, F.; Pietrangelo, A.; Corrao, S. Impact of Diabetes Mellitus and Its Comorbidities on Elderly Patients Hospitalized in Internal Medicine Wards: Data from the RePoSi Registry. Healthcare 2022, 10, 86. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Natoli, G.; Nobili, A.; Mannucci, P.M.; Perticone, F.; Arcoraci, V.; Argano, C. The “Diabetes Comorbidome”: A Different Way for Health Professionals to Approach the Comorbidity Burden of Diabetes. Healthcare 2022, 10, 1459. [Google Scholar] [CrossRef] [PubMed]
- National Diabetes Statistics Report | Diabetes | CDC. Available online: https://www.cdc.gov/diabetes/data/statistics-report/index.html (accessed on 10 February 2024).
- Europe Diabetes Report 2000–2045. Available online: https://www.diabetesatlas.org/data/ (accessed on 10 February 2024).
- Russell-Jones, D.; Pouwer, F.; Khunti, K. Identification of Barriers to Insulin Therapy and Approaches to Overcoming Them. Diabetes Obes. Metab. 2018, 20, 488–496. [Google Scholar] [CrossRef]
- Khunti, K.; Gomes, M.B.; Pocock, S.; Shestakova, M.V.; Pintat, S.; Fenici, P.; Hammar, N.; Medina, J. Therapeutic Inertia in the Treatment of Hyperglycaemia in Patients with Type 2 Diabetes: A Systematic Review. Diabetes Obes. Metab. 2018, 20, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Boye, K.S.; Curtis, S.E.; Lage, M.J.; Garcia-Perez, L.-E. Associations between Adherence and Outcomes among Older, Type 2 Diabetes Patients: Evidence from a Medicare Supplemental Database. Patient Prefer. Adherence 2016, 10, 1573–1581. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, L.A.; Morris, A.D.; Evans, J.M.M.; DARTS/MEMO Collaboration. Adherence to Insulin and Its Association with Glycaemic Control in Patients with Type 2 Diabetes. J. Assoc. Physicians 2007, 100, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Kuritzky, L.; Reid, T.S.; Wysham, C.H. Practical Guidance on Effective Basal Insulin Titration for Primary Care Providers. Clin. Diabetes 2019, 37, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Peyrot, M.; Rubin, R.R.; Kruger, D.F.; Travis, L.B. Correlates of Insulin Injection Omission. Diabetes Care 2010, 33, 240–245. [Google Scholar] [CrossRef]
- Peyrot, M.; Barnett, A.H.; Meneghini, L.F.; Schumm-Draeger, P.-M. Factors Associated with Injection Omission/Non-Adherence in the Global Attitudes of Patients and Physicians in Insulin Therapy Study. Diabetes Obes. Metab. 2012, 14, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Sugumar, V.; Ang, K.P.; Alshanon, A.F.; Sethi, G.; Yong, P.V.C.; Looi, C.Y.; Wong, W.F. A Comprehensive Review of the Evolution of Insulin Development and Its Delivery Method. Pharmaceutics 2022, 14, 1406. [Google Scholar] [CrossRef]
- Qiao, Q.; Ouwens, M.J.; Grandy, S.; Johnsson, K.; Kostev, K. Adherence to GLP-1 Receptor Agonist Therapy Administered by Once-Daily or Once-Weekly Injection in Patients with Type 2 Diabetes in Germany. Diabetes Metab. Syndr. Obes. 2016, 9, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Chen, S.; Flood, E.; Shaunik, A.; Romero, B.; de la Cruz, M.; Alvarez, C.; Grandy, S. Glucagon-Like Peptide-1 Receptor Agonist Treatment Attributes Important to Injection-Experienced Patients with Type 2 Diabetes Mellitus: A Preference Study in Germany and the United Kingdom. Diabetes Ther. 2017, 8, 335–353. [Google Scholar] [CrossRef] [PubMed]
- Weeda, E.R.; Muraoka, A.K.; Brock, M.D.; Cannon, J.M. Medication Adherence to Injectable Glucagon-like Peptide-1 (GLP-1) Receptor Agonists Dosed Once Weekly vs Once Daily in Patients with Type 2 Diabetes: A Meta-Analysis. Int. J. Clin. Pract. 2021, 75, e14060. [Google Scholar] [CrossRef] [PubMed]
- Weiss, T.; Carr, R.D.; Pal, S.; Yang, L.; Sawhney, B.; Boggs, R.; Rajpathak, S.; Iglay, K. Real-World Adherence and Discontinuation of Glucagon-Like Peptide-1 Receptor Agonists Therapy in Type 2 Diabetes Mellitus Patients in the United States. Patient Prefer. Adherence 2020, 14, 2337–2345. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, J.; Bajaj, H.S.; Janež, A.; Silver, R.; Begtrup, K.; Hansen, M.V.; Jia, T.; Goldenberg, R.; NN1436-4383 Investigators. Once-Weekly Insulin for Type 2 Diabetes without Previous Insulin Treatment. N. Engl. J. Med. 2020, 383, 2107–2116. [Google Scholar] [CrossRef] [PubMed]
- Skyler, J.S. Weekly Insulin Becoming a Reality. Diabetes Care 2021, 44, 1459–1461. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Colomba, D.; Arnone, S.; Argano, C.; Di Chiara, T.; Scaglione, R.; Licata, G. Improving Efficacy of PubMed Clinical Queries for Retrieving Scientifically Strong Studies on Treatment. J. Am. Med. Inf. Assoc. 2006, 13, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Colomba, D.; Argano, C.; Calvo, L.; Scaglione, R.; Licata, G. Optimized Search Strategy for Detecting Scientifically Strong Studies on Treatment through PubMed. Intern. Emerg. Med. 2012, 7, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.B.; McKibbon, K.A.; Wilczynski, N.L.; Walter, S.D.; Werre, S.R.; Hedges Team. Optimal Search Strategies for Retrieving Scientifically Strong Studies of Treatment from Medline: Analytical Survey. BMJ 2005, 330, 1179. [Google Scholar] [CrossRef] [PubMed]
- Rubino, A.; McQuay, L.J.; Gough, S.C.; Kvasz, M.; Tennis, P. Delayed Initiation of Subcutaneous Insulin Therapy after Failure of Oral Glucose-Lowering Agents in Patients with Type 2 Diabetes: A Population-Based Analysis in the UK. Diabet. Med. 2007, 24, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Fisher, L.; Hessler, D.; Bruhn, D.; Best, J.H. Patient Perspectives on Once-Weekly Medications for Diabetes. Diabetes Obes. Metab. 2011, 13, 144–149. [Google Scholar] [CrossRef]
- Paley, R.G.; Scott, M.H. Severe Insulin Lipodystrophy as a Possible Cause of Instability in Diabetics. Br. Med. J. 1958, 2, 1331–1334. [Google Scholar] [CrossRef] [PubMed]
- Watson, E.M. Non-Hypoglycaemic (Allergic) Insulin Reactions. Can. Med. Assoc. J. 1942, 47, 336–339. [Google Scholar] [PubMed]
- American Diabetes Association 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S98–S110. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Henry, R.R. Poor Medication Adherence in Type 2 Diabetes: Recognizing the Scope of the Problem and Its Key Contributors. Patient Prefer. Adherence 2016, 10, 1299–1307. [Google Scholar] [CrossRef]
- Howard, V.; Church, C.; Oldham, S.; Hornigold, D.; Trevaskis, J.; Baker, D.; Rhodes, C.; Rossi, A.; Naylor, J.; Dhillon, J.; et al. 1086-P: Preclinical Development of an Ultralong-Acting Insulin for Once-Weekly Dosing. Diabetes 2019, 68, 1086-P. [Google Scholar] [CrossRef]
- Rezolute, Inc. Announces Top-Line Results from Phase 1 Trial Evaluating AB101 in Patients with Diabetes. Available online: https://www.biospace.com/article/rezolute-inc-announces-top-line-results-from-phase-1-trial-evaluating-ab101-in-patients-with-diabetes-/ (accessed on 17 February 2024).
- Insulin Long-Acting (HM 12470)—Hanmi Pharmaceutical—AdisInsight. Available online: https://adisinsight.springer.com/drugs/800040862 (accessed on 17 February 2024).
- Hanmi | Hanmi Pharmaceutical’s Official Site. Available online: https://www.hanmipharm.com/main.hm (accessed on 17 February 2024).
- Kurtzhals, P.; Nishimura, E.; Haahr, H.; Høeg-Jensen, T.; Johansson, E.; Madsen, P.; Sturis, J.; Kjeldsen, T. Commemorating Insulin’s Centennial: Engineering Insulin Pharmacology towards Physiology. Trends Pharmacol. Sci. 2021, 42, 620–639. [Google Scholar] [CrossRef] [PubMed]
- Marquez, F.; Brazg, R.; Christiansen, M.; Free, A.; Matson, M.; Jones, S.; Georgopoulos, L.; Malatesta, J.; Arnold, S.; Kramer, W.; et al. PE0139, the First Recombinant Fully Human Monomeric Super-Long-Acting Basal Insulin to Display a Sustained Nearly Peakless Insulin Profile Following a Single Subcutaneous Dose in Subjects with T2DM Supporting Weekly Dosing. In Proceedings of the 75th Scientific Sessions of the American Diabetes Association, Boston, MA, USA, 5–9 June 2014; p. A26. [Google Scholar]
- Moyers, J.S.; Hansen, R.J.; Day, J.W.; Dickinson, C.D.; Zhang, C.; Ruan, X.; Ding, L.; Brown, R.M.; Baker, H.E.; Beals, J.M. Preclinical Characterization of LY3209590, a Novel Weekly Basal Insulin Fc-Fusion Protein. J. Pharmacol. Exp. Ther. 2022, 382, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Heise, T.; Chien, J.; Beals, J.M.; Benson, C.; Klein, O.; Moyers, J.S.; Haupt, A.; Pratt, E.J. Pharmacokinetic and Pharmacodynamic Properties of the Novel Basal Insulin Fc (Insulin Efsitora Alfa), an Insulin Fusion Protein in Development for Once-Weekly Dosing for the Treatment of Patients with Diabetes. Diabetes Obes. Metab. 2023, 25, 1080–1090. [Google Scholar] [CrossRef] [PubMed]
- Philis-Tsimikas, A.; Bajaj, H.S.; Begtrup, K.; Cailleteau, R.; Gowda, A.; Lingvay, I.; Mathieu, C.; Russell-Jones, D.; Rosenstock, J. Rationale and Design of the Phase 3a Development Programme (ONWARDS 1-6 Trials) Investigating Once-Weekly Insulin Icodec in Diabetes. Diabetes Obes. Metab. 2023, 25, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, E.; Pridal, L.; Glendorf, T.; Hansen, B.F.; Hubálek, F.; Kjeldsen, T.; Kristensen, N.R.; Lützen, A.; Lyby, K.; Madsen, P.; et al. Molecular and Pharmacological Characterization of Insulin Icodec: A New Basal Insulin Analog Designed for Once-Weekly Dosing. BMJ Open Diabetes Res. Care 2021, 9, e002301. [Google Scholar] [CrossRef] [PubMed]
- Danne, T.; Heinemann, L.; Pieber, T.R. New Insulins, Biosimilars, and Insulin Therapy. Diabetes Technol. Ther. 2023, 25, S44–S69. [Google Scholar] [CrossRef] [PubMed]
- Belal, H.; Gandhi, G.Y. In T2DM Uncontrolled with Noninsulin Glucose-Lowering Agents, Weekly Icodec Reduced HbA1c vs. Daily Degludec at 26 Wk. Ann. Intern. Med. 2023, 176, JC112. [Google Scholar] [CrossRef] [PubMed]
- Lingvay, I.; Asong, M.; Desouza, C.; Gourdy, P.; Kar, S.; Vianna, A.; Vilsbøll, T.; Vinther, S.; Mu, Y. Once-Weekly Insulin Icodec vs Once-Daily Insulin Degludec in Adults with Insulin-Naive Type 2 Diabetes: The ONWARDS 3 Randomized Clinical Trial. JAMA 2023, 330, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Bue-Valleskey, J.M.; Kazda, C.M.; Ma, C.; Chien, J.; Zhang, Q.; Chigutsa, E.; Landschulz, W.; Haupt, A.; Frias, J.P. Once-Weekly Basal Insulin Fc Demonstrated Similar Glycemic Control to Once-Daily Insulin Degludec in Insulin-Naive Patients with Type 2 Diabetes: A Phase 2 Randomized Control Trial. Diabetes Care 2023, 46, 1060–1067. [Google Scholar] [CrossRef]
- Roussel, R.; Charbonnel, B.; Behar, M.; Gourmelen, J.; Emery, C.; Detournay, B. Persistence with Insulin Therapy in Patients with Type 2 Diabetes in France: An Insurance Claims Study. Diabetes Ther. 2016, 7, 537–549. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, D.G.; Ozcan, S.; Deyneli, O. Adherence to Insulin Treatment in Insulin-Naïve Type 2 Diabetic Patients Initiated on Different Insulin Regimens. Patient Prefer. Adherence 2015, 9, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Morrison, F.; Zhao, Z.; Haynes, G.; He, X.; Ali, A.K.; Shubina, M.; Malmasi, S.; Ge, W.; Peng, X.; et al. Reasons for Discontinuing Insulin and Factors Associated with Insulin Discontinuation in Patients with Type 2 Diabetes Mellitus: A Real-World Evidence Study. Clin. Diabetes Endocrinol. 2021, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, J.; Bain, S.C.; Gowda, A.; Jódar, E.; Liang, B.; Lingvay, I.; Nishida, T.; Trevisan, R.; Mosenzon, O.; ONWARDS 1 Trial Investigators. Weekly Icodec versus Daily Glargine U100 in Type 2 Diabetes without Previous Insulin. N. Engl. J. Med. 2023, 389, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Philis-Tsimikas, A.; Asong, M.; Franek, E.; Jia, T.; Rosenstock, J.; Stachlewska, K.; Watada, H.; Kellerer, M. Switching to Once-Weekly Insulin Icodec versus Once-Daily Insulin Degludec in Individuals with Basal Insulin-Treated Type 2 Diabetes (ONWARDS 2): A Phase 3a, Randomised, Open Label, Multicentre, Treat-to-Target Trial. Lancet Diabetes Endocrinol. 2023, 11, 414–425. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhang, Y.; Xu, W.; He, J.; Peng, L.; Feng, Y.; Xu, P.; Chong, W.; Hai, Y.; Jia, L.; et al. Efficacy and Safety of Once-Weekly Insulin Regimes on Glycemic Control for Type 2 Diabetes: A Systematic Review and Network Meta-Analysis. Diabetol. Metab. Syndr. 2024, 16, 3. [Google Scholar] [CrossRef] [PubMed]
- Frias, J.; Chien, J.; Zhang, Q.; Chigutsa, E.; Landschulz, W.; Syring, K.; Wullenweber, P.; Haupt, A.; Kazda, C. Safety and Efficacy of Once-Weekly Basal Insulin Fc in People with Type 2 Diabetes Previously Treated with Basal Insulin: A Multicentre, Open-Label, Randomised, Phase 2 Study. Lancet Diabetes Endocrinol. 2023, 11, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Lingvay, I.; Buse, J.B.; Franek, E.; Hansen, M.V.; Koefoed, M.M.; Mathieu, C.; Pettus, J.; Stachlewska, K.; Rosenstock, J. A Randomized, Open-Label Comparison of Once-Weekly Insulin Icodec Titration Strategies Versus Once-Daily Insulin Glargine U100. Diabetes Care 2021, 44, 1595–1603. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Nobili, A.; Natoli, G.; Mannucci, P.M.; Perticone, F.; Pietrangelo, A.; Argano, C.; REPOSI Investigators. Hyperglycemia at admission, comorbidities, and in-hospital mortality in elderly patients hospitalized in internal medicine wards: Data from the RePoSI Registry. Acta Diabetol. 2021, 58, 1225–1236, Correction in Acta Diabetol. 2021, 58, 1237. [Google Scholar] [CrossRef]
- Candido, R.; Nicolucci, A.; Larosa, M.; Rossi, M.C.; Napoli, R.; Gabellieri, E.; Tortato, E.; Rabini, R.A.; Crazzolara, D.; Lucibelli, L.; et al. Treatment Intensification Following Glucagon-like Peptide-1 Receptor Agonist Treatment in Type 2 Diabetes: The RESTORE-G Real-World Study. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 2294–2305. [Google Scholar] [CrossRef]
- Guerci, B.; Chanan, N.; Kaur, S.; Jasso-Mosqueda, J.G.; Lew, E. Lack of Treatment Persistence and Treatment Nonadherence as Barriers to Glycaemic Control in Patients with Type 2 Diabetes. Diabetes Ther. 2019, 10, 437–449. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, J.; Del Prato, S. Basal Weekly Insulins: The Way of the Future! Metabolism 2022, 126, 154924. [Google Scholar] [CrossRef] [PubMed]
- Baser, O.; Tangirala, K.; Wei, W.; Xie, L. Real-World Outcomes of Initiating Insulin Glargine-Based Treatment versus Premixed Analog Insulins among US Patients with Type 2 Diabetes Failing Oral Antidiabetic Drugs. Clin. Outcomes Res. 2013, 5, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, C.; Ásbjörnsdóttir, B.; Bajaj, H.S.; Lane, W.; Matos, A.L.S.A.; Murthy, S.; Stachlewska, K.; Rosenstock, J. Switching to Once-Weekly Insulin Icodec versus Once-Daily Insulin Glargine U100 in Individuals with Basal-Bolus Insulin-Treated Type 2 Diabetes (ONWARDS 4): A Phase 3a, Randomised, Open-Label, Multicentre, Treat-to-Target, Non-Inferiority Trial. Lancet 2023, 401, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, H.S.; Aberle, J.; Davies, M.; Donatsky, A.M.; Frederiksen, M.; Yavuz, D.G.; Gowda, A.; Lingvay, I.; Bode, B. Once-Weekly Insulin Icodec with Dosing Guide App versus Once-Daily Basal Insulin Analogues in Insulin-Naive Type 2 Diabetes (ONWARDS 5): A Randomized Trial. Ann. Intern. Med. 2023, 176, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, M.J.; Dinneen, S.F. In Type 2 Diabetes, Weekly Basal Insulin Fc Was Noninferior to Daily Insulin Degludec for HbA1c at 26 Wk. Ann. Intern. Med. 2023, 176, JC81. [Google Scholar] [CrossRef] [PubMed]
- Kazda, C.M.; Bue-Valleskey, J.M.; Chien, J.; Zhang, Q.; Chigutsa, E.; Landschulz, W.; Wullenweber, P.; Haupt, A.; Dahl, D. Novel Once-Weekly Basal Insulin Fc Achieved Similar Glycemic Control with a Safety Profile Comparable to Insulin Degludec in Patients with Type 1 Diabetes. Diabetes Care 2023, 46, 1052–1059. [Google Scholar] [CrossRef] [PubMed]
- Russell-Jones, D.; Babazono, T.; Cailleteau, R.; Engberg, S.; Irace, C.; Kjaersgaard, M.I.S.; Mathieu, C.; Rosenstock, J.; Woo, V.; Klonoff, D.C. Once-Weekly Insulin Icodec versus Once-Daily Insulin Degludec as Part of a Basal-Bolus Regimen in Individuals with Type 1 Diabetes (ONWARDS 6): A Phase 3a, Randomised, Open-Label, Treat-to-Target Trial. Lancet 2023, 402, 1636–1647. [Google Scholar] [CrossRef] [PubMed]
- Fifer, S.; Rose, J.; Hamrosi, K.K.; Swain, D. Valuing Injection Frequency and Other Attributes of Type 2 Diabetes Treatments in Australia: A Discrete Choice Experiment. BMC Health Serv. Res. 2018, 18, 675. [Google Scholar] [CrossRef] [PubMed]
- Blonde, L.; Meneghini, L.; Peng, X.V.; Boss, A.; Rhee, K.; Shaunik, A.; Kumar, S.; Balodi, S.; Brulle-Wohlhueter, C.; McCrimmon, R.J. Probability of Achieving Glycemic Control with Basal Insulin in Patients with Type 2 Diabetes in Real-World Practice in the USA. Diabetes Ther. 2018, 9, 1347–1358. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Nikolajsen, A.; Thorsted, B.L.; Andersen, M.; Davies, M.J.; Paul, S.K. Clinical Inertia with Regard to Intensifying Therapy in People with Type 2 Diabetes Treated with Basal Insulin. Diabetes Obes. Metab. 2016, 18, 401. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhang, H.; Li, X.; Chen, M.; Wang, D.; Ji, L. Factors and Outcomes Associated with Discontinuation of Basal Insulin Therapy in Patients with Type 2 Diabetes Mellitus. Endocrinol. Diabetes Metab. 2020, 3, e00122. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Giorgino, F.; Berard, L.; Mauricio, D.; Harris, S.B. The Importance of the Initial Period of Basal Insulin Titration in People with Diabetes. Diabetes Obes. Metab. 2020, 22, 722–733. [Google Scholar] [CrossRef] [PubMed]
- Abuelazm, M.; Ibrahim, A.A.; Khlidj, Y.; Badr, A.; Amin, A.M.; Elzeftawy, M.A.; Gowaily, I.; Elsaeidy, A.S.; Abdelazeem, B. Once-weekly Insulin Icodec versus Once-daily Long-acting Insulin for Type II Diabetes: A Meta-analysis of Randomized Controlled Trials. J. Endocr. Soc. 2023, 8, bvad177. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, H.S.; Bergenstal, R.M.; Christoffersen, A.; Davies, M.J.; Gowda, A.; Isendahl, J.; Lingvay, I.; Senior, P.A.; Silver, R.J.; Trevisan, R.; et al. Switching to Once-Weekly Insulin Icodec versus Once-Daily Insulin Glargine U100 in Type 2 Diabetes Inadequately Controlled on Daily Basal Insulin: A Phase 2 Randomized Controlled Trial. Diabetes Care 2021, 44, 1586–1594. [Google Scholar] [CrossRef] [PubMed]
- Sciacca, L.; Vella, V.; Frittitta, L.; Tumminia, A.; Manzella, L.; Squatrito, S.; Belfiore, A.; Vigneri, R. Long-actinginsulinanalogs and cancer. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Aktas, G.; Taslamacioglu Duman, T. Current usage of long-acting insulin analogs in patients with type 2 diabetes mellitus. Expert Rev. Endocrinol. Metab. 2024, 19, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Argano, C.; Natoli, G.; Nobili, A.; Corazza, G.R.; Mannucci, P.M.; Perticone, F.; REPOSI Investigators. Sex-Differences in the Pattern of Comorbidities, Functional Independence, and Mortality in Elderly Inpatients: Evidence from the RePoSI Register. J. Clin. Med. 2019, 8, 81. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Insulin Fc vs. Degludec in DMt2 Patients Previously Treated with Basal Insulin [40] | Insulin Fc vs. Degludec in DMt2 Patients Insulino-Naïve [43] | Insulin Fc vs. Degludec in DMt1 Patients [44] | |
|---|---|---|---|
| Study design |
|
|
|
| Period | November 2018–February 2020 | 5 March 2021–19 July 2023 | 6 June 2020–22 January 2021 |
| Endpoint I | HbA1c reduction at 32 weeks | HbA1c reduction at 26 weeks | HbA1c reduction at 26 weeks |
| Endpoint II |
|
|
|
| Titration protocol | The loading and initial weekly doses were based on their previous daily basal insulin dose and their glycemic control according to baseline HbA1c (using a threshold of 8.5. BIF dosing in the Phase 2 program used mg increments and not insulin international units (IU)) | Initial dose 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL | Titration was based on mean fasting blood glucose levels using CGM measurements on at least 3 days of the week using a paper-based algorithm. BIF was titrated weekly for weeks 1–12 and then every 4 weeks until the end of the treatment period |
| Numbers of patients |
|
|
|
| Population |
|
|
|
| Results |
|
|
|
| Hypoglycemic events | The event rates of all documented hypoglycemia were about 25% lower in the Fc groups, and those for nocturnal hypoglycemia were at least 33% lower from baseline to week 32 compared with insulin degludec | The rate of severe hypoglycemic events was not significant between treatment groups (p 0.64) | Hypoglycemia occurrence over 24 h was similar for BIF and degludec for level 1 (p = 0.960) or level 2 (p = 0.517) hypoglycemia during treatment. The occurrence of serious adverse events was similar between the BIF and degludec groups. |
| Adverse events | Mostly mild/moderate events and not associated with treatment Deaths: 3 (2%) in degludec, 1 (1%) in glargine No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment: Fc 5.6% (n = 143) Degludec 3% (n = 135) Deaths: 2 (1%) in Fc, 3 (1.5%) in degludec | Mostly mild/moderate events and not associated with treatment. The occurrence of serious adverse events was similar between the BIF and degludec groups. |
| ONWARDS 1 Icodec vs. Glargine U100 in DT2 Insulino-Naïve [45] | ONWARDS 2 Icodec vs. Degludec U100 in Basal Bolus [46] | ONWARDS 3 Icodec vs. Degludec in DT2 Insulino-Naïve [47] | ONWARDS 4 Icodec vs. Glargine U100 in DT2 in Basal Bolus [48] | ONWARDS 5 Icodec vs. Once-Daily Insulin in DT2 Insulino-Naïve with Dosing Guide App [49] | ONWARDS 6 Icodec vs. Degludec in T1D [50] | |
|---|---|---|---|---|---|---|
| Study design |
|
|
|
|
|
|
| Period | November 2020–May 2023 | 5 March 2021–19 July 2023 | March 2021–June 2022 | March 2021–October 2021 | 1 March 2021–12 August 2022 | 30 April 2021–15 October 2021 |
| Endpoint I | HbA1c reduction at 52 weeks | HbA1c reduction at 26 weeks | HbA1c reduction at 26 weeks | HbA1c reduction at 26 weeks | HbA1c reduction at 52 weeks | HbA1c reduction at 26 weeks |
| Endpoint II |
|
|
|
|
|
|
| Titration protocol | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL Increments of 3 IU/day (20 IU/week for icodec) | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL | Icodec titrated with a dosing guide app (icodec with app) | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL Increments of 3 IU/day (20 IU/week for icodec) |
| Numbers of patients |
|
|
|
|
|
|
| Population |
|
|
|
|
|
|
| Results |
|
|
| At week 26, the mean change in HbA1c was −1.16 percentage points in the icodec group (baseline 8.29%) and −1.18 percentage points in the glargine U100 group (baseline 8.31%). Combined level 2 and level 3 hypoglycemia rates were similar between treatment groups. | At week 52, insulin icodec used in conjunction with the dosing guide app demonstrated non-inferiority and superiority versus the basal insulin analogues in reducing the estimated mean HbA1c from baseline |
|
| Hypoglycemic events | Icodecs:
Glargine:
| Clinically significant hypoglycemia rates were not significant between the two groups at week 31 | Icodecs:
Degludec:
| Icodecs:
Degludec U100:
| Clinically significant or severe hypoglycemia rates were not significantly different between the treatment groups at week 57 | Icodecs:
Degludec:
|
| Adverse events | Mostly mild/moderate events and not associated with treatment Deaths: 5 in icodec, 4 in glargine No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment Deaths: 5 in icodec, 4 in glargine No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment Deaths: 2 in icodec, 1 in degludec 8.5 vs. 4.4% injection site reactions for icodec vs. degludec Usage errors <5% | Mostly mild/moderate events and not associated with treatment No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment Deaths: 1 in icodec, 0 in degludec 0.07% vs. 0.06% injection site reactions for icodec vs. degludec |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argano, C.; Priola, L.; Manno, F.; Corrao, S. What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art. Biomedicines 2024, 12, 900. https://doi.org/10.3390/biomedicines12040900
Argano C, Priola L, Manno F, Corrao S. What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art. Biomedicines. 2024; 12(4):900. https://doi.org/10.3390/biomedicines12040900
Chicago/Turabian StyleArgano, Christiano, Laura Priola, Francesco Manno, and Salvatore Corrao. 2024. "What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art" Biomedicines 12, no. 4: 900. https://doi.org/10.3390/biomedicines12040900
APA StyleArgano, C., Priola, L., Manno, F., & Corrao, S. (2024). What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art. Biomedicines, 12(4), 900. https://doi.org/10.3390/biomedicines12040900