Air Contamination in Different Departments of a Tertiary Hospital. Assessment of Microbial Load and of Antimicrobial Susceptibility




 ,
, 
Abstract
:1. Background
2. Methods
2.1. Air Sampling Methodology
2.2. Identification of the Isolates
2.3. Drug Resistance Definitions
2.4. Antibiotic Sensitivity Assessment
2.5. Statistical Analysis
3. Results
3.1. Sampling Location
3.2. Environmental Parameters in the Four Settings
3.3. Identification of Microbes
3.4. Microbial Load
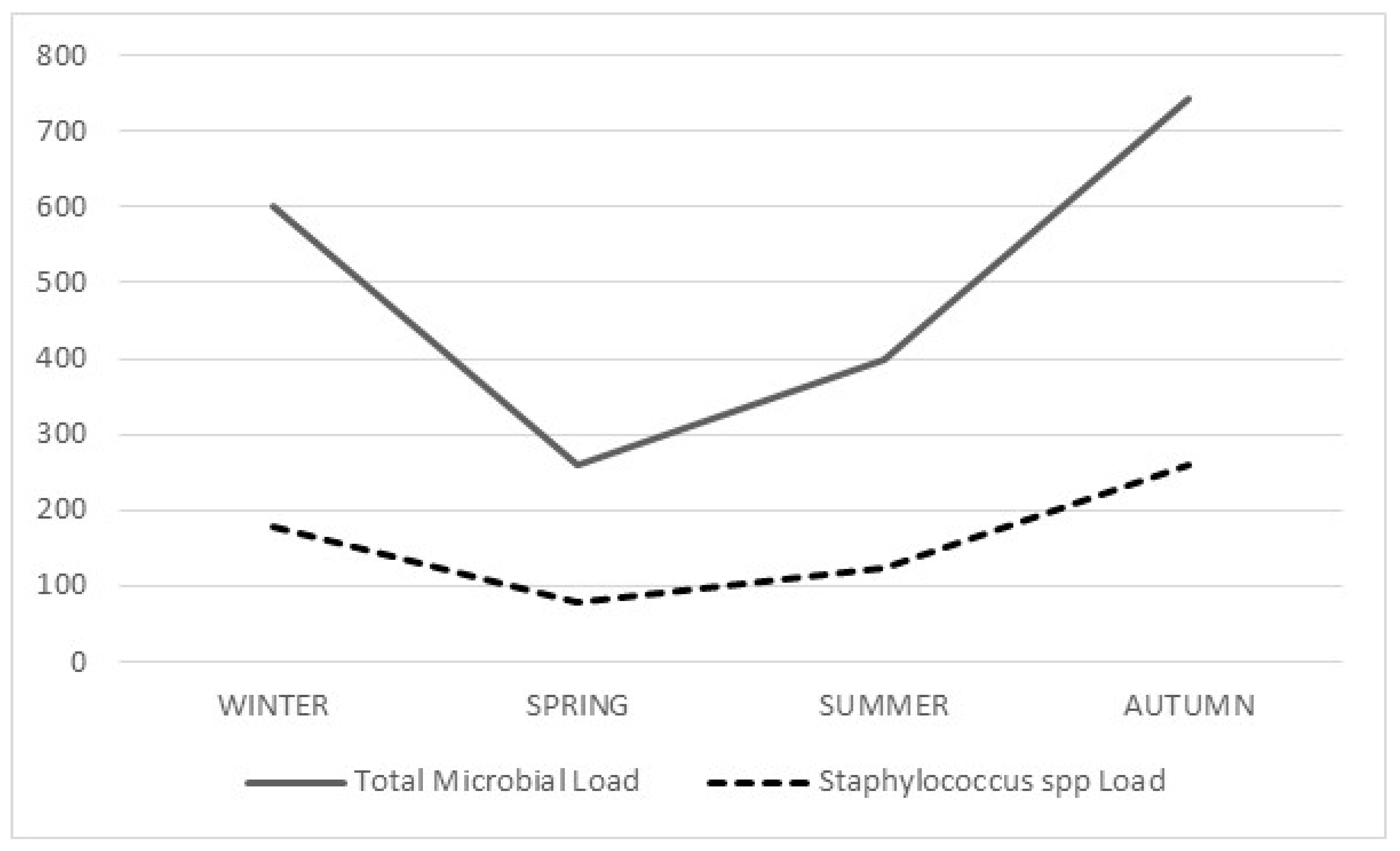
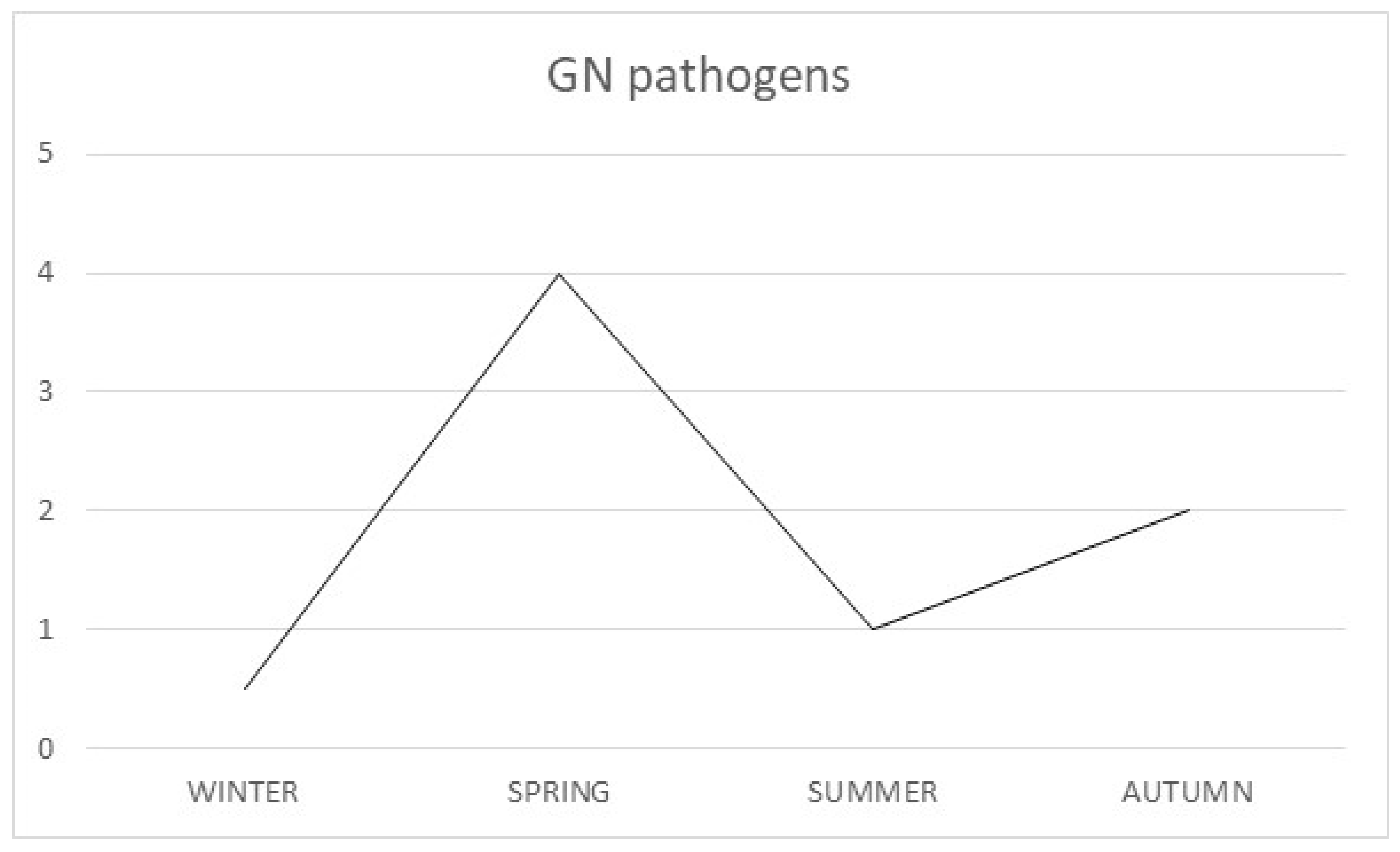
3.5. Comparison of Seasonal Variations in Airborne Pathogens, throughout the Year
3.6. Drug Resistance of the Microbes, Isolated from the Inanimate Environment Samples
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Health Care-Associated Infections Fact Sheet. Available online: http://www.who.int/gpsc/country_work/gpsc_ccisc_fact_sheet_en.pdf (accessed on 30 May 2016).
- Haddadin, A.S.; Fappiano, S.; Lipsett, P. Methicillin resistant staphylococcus aureus (MRSA) in the intensive care unit. Postgrad. Med. J. 2002, 78, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Park, D.-U.; Yeom, J.-K.; Lee, W.J.; Lee, K.-M. Assessment of the levels of airborne bacteria, Gram-negative bacteria, and fungi in hospital lobbies. Int. J. Environ. Res. Public Health. 2013, 10, 541–555. [Google Scholar] [CrossRef] [PubMed]
- Beggs, C.B. The airborne transmission of infection in hospital buildings: Fact or fiction? Indoor Built Environ. 2003, 12, 9–18. [Google Scholar] [CrossRef]
- Killingley, B.; Greatorex, J.; Digard, P.; Wise, H.; Garcia, F.; Varsani, H.; Cauchemez, S.; Enstone, J.E.; Hayward, A.; Curran, M.D.; et al. The environmental deposition of influenza virus from patients infected with influenza A(H1N1)pdm09: Implications for infection prevention and control. J. Infect. Public Health. 2016, 9, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Scaltriti, S.; Cencetti, S.; Rovesti, S.; Marchesi, I.; Bargellini, A.; Borella, P. Risk factors for particulate and microbial contamination of air in operating theatres. J. Hosp. Infect. 2007, 66, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.W.; Li, Y.; Eames, I.; Chan, P.K.; Ridgway, G. Factors involved in the aerosol transmission of infection and control of ventilation in healthcare premises. J. Hosp. Infect. 2006, 64, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.; Carmeli, Y.; Falagas, M.E.; Giske, C.; Harbarth, S.; Hindler, J.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augustowska, M.; Dutkiewicz, J. Variability of airborne microflora in a hospital ward within a period of one year. Ann. Agric. Environ. Med. 2006, 13, 99–106. [Google Scholar] [PubMed]
- Li, C.S.; Hou, P.A. Bioaerosol characteristics in hospital clean rooms. Sci. Total Environ. 2003, 305, 169–176. [Google Scholar] [CrossRef]
- Çakir, N.A.; Uçar, F.; Uztan, A.H.; Corbaci, C.; Akpinar, O. Determination and comparison of microbial loads in atmospheres of two hospitals in Izmir, Turkey. Ann. Agric. Environ. Med. 2013, 20, 106–110. [Google Scholar]
- Verde, S.C.; Almeida, S.M.; Matos, J.; Guerreiro, D.; Meneses, M.; Faria, T.; Botelho, D.; Santos, M.; Viegas, S. Microbiological assessment of indoor air quality at different hospital sites. Res. Microbiol. 2015, 166, 557–563. [Google Scholar] [CrossRef]
- Fekadu, S.; Getachewu, B. Microbiological assessment of indoor air of teaching hospital wards: A case of Jimma University specialized hospital. Ethiop. J. Health Sci. 2015, 25, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Fujiyoshi, S.; Tanaka, D.; Maruyama, F. Transmission of airborne bacteria across built environments and its measurement standards: A review. Front. Microbiol. 2017, 8, 2336. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.-L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin-Loeches, I.; Moreno, R.; Lipman, J.; Gomersall, C.D.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frankel, M.; Bekö, G.; Timm, M.; Gustavsen, S.; Hansen, E.W.; Madsen, A.M. Seasonal variations of indoor microbial exposures and their relation to temperature, relative humidity, and air exchange rate. Appl. Environ. Microbiol. 2012, 78, 8289–8297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vatopoulos, A. High rates of metallo-beta-lactamase-producing Klebsiella pneumoniae in Greece—A review of the current evidence. Eurosurveillance 2008, 13, 8023. [Google Scholar] [CrossRef] [PubMed]
- European Center for Disease Prevention and Control. Surveillance Report. Annual Epidemiological Report. Antimicrobial Resistance and Healthcare-Associated Infections 2014. Available online: http://ecdc.europa.eu/en/publications/Publications/antimicrobial-resistance-annual-epidemiological-report.pdf (accessed on 30 May 2016).
- Mirhoseini, S.H.; Nikaeen, M.; Shamsizadeh, Z.; Khanahmad, H. Hospital air: A potential route for transmission of infections caused by β-lactam-resistant bacteria. Am. J. Infect. Control 2016, 44, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Mirzaii, M.; Emaneini, M.; Jabalameli, F.; Halimi, S.; Taherikalani, M. Molecular investigation of Staphylococcus aureus isolated from the patients, personnel, air and environment of an ICU in a hospital in Tehran. J. Infect. Public Health 2015, 8, 202–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Górny, R.L.; Dutkiewicz, J.; Krysińska-Traczyk, E. Size distribution of bacterial and fungal bioaerosols in indoor air. Ann. Agric. Environ. Med. 1999, 6, 105–113. [Google Scholar] [PubMed]
- Hadapad, D.; Sonth, S.; Solabannavar, S.S. Indoor airborne bacterial load in neonatal, perinatal intensive care units and pediatric wards at tertiary care hospital Bagalkot, India. Int. J. Curr. Microbiol. Appl. Sci. 2015, 4, 136–142. [Google Scholar]



{kind=link}
{kind=link}
| Location | Central Hall | Isolated Rooms | Examination Room | Ward | Total Number of Samples |
|---|---|---|---|---|---|
| ICU | 12 | 24 | 36 | ||
| Surgical Ward | 12 | 12 | 24 | ||
| Internal Medicine Ward | 12 | 13 | 25 | ||
| Neonatal Unit | 16 | 16 |
| Number of Isolates | |||||
|---|---|---|---|---|---|
| ICU | IMW | SW | NU | Total | |
| GN (total) | 26 | 9 | 6 | 3 | 44 |
| Klebsiella pneumoniae | 6 | 0 | 0 | 0 | 6 |
| Acinetobacter baumanii | 2 | 0 | 1 | 0 | 3 |
| Pseudomonas aeruginosa | 1 | 1 | 0 | 0 | 2 |
| Pseudomonas stutzeri | 1 | 0 | 1 | 0 | 2 |
| Pseudomonas oryzihabitans | 6 | 3 | 1 | 2 | 12 |
| Pseudomonas fluorescens | 1 | 1 | 1 | 1 | 4 |
| Enterobacter cloacae | 1 | 0 | 1 | 0 | 2 |
| Pantoea agglomerans | 1 | 3 | 1 | 0 | 5 |
| Escherichia coli | 7 | 1 | 0 | 0 | 8 |
| GP (total) | 58 | 41 | 37 | 22 | 158 |
| Staphylococcus spp. | 36 | 25 | 24 | 15 | 100 |
| Staphylococcus aureus | 2 | 5 | 1 | 1 | 9 |
| Enterococcus spp. | 22 | 16 | 13 | 7 | 58 |
| MDR | XDR | TOTAL | |
|---|---|---|---|
| ICU | K. pneumoniae (n = 2) A. baumanii (n = 1) Enterococcus spp. (n = 1) | A. baumanii (n = 1) | 5 |
| IMW | S. aureus (n = 2) | 2 | |
| SW | S. aureus (n = 1) | A. baumanii (n = 1) | 2 |
| NU | Enterococcus spp. (n = 1) | 1 |
| 1 | 2 | ||
|---|---|---|---|
| Department | ICU | ICU | |
| Location | Isolated room | Isolated room | |
| Antibiotics | Aminoglycosides | R | R |
| Antipseudomonal penicillins and b-lactamase inhibitors | R | R | |
| Carbapenems | R | R | |
| Non-extended spectrum cephalosporins, 1st and 2nd generation cephalosporins | R | R | |
| Extended-spectrum cephalosporins; 3rd and 4th generation cephalosporins | R | R | |
| Cephamycins | R | R | |
| Fluoroquinolones | R | R | |
| Folate pathway inhibitors | R | R | |
| Glycylcyclines | S | S | |
| Monobactams | R | R | |
| Penicillins | R | R | |
| Penicillins + b-lactamase inhibitors | R | R | |
| Phenicols | S | S | |
| Phosphonic acids | S | S | |
| Polymyxins | S | S | |
| Tetracyclines | S | S | |
| Resistance type | MDR | MDR | |
| 1 | 2 | 3 | ||
|---|---|---|---|---|
| Department | ICU | ICU | SW | |
| Location | Isolated room | Central hall | Patient room | |
| Antibiotics | Aminoglycosides, | R | R | R |
| Antipseudomonal carbapenems | R | S | R | |
| Antipseudomonal fluoroquinolones | R | R | R | |
| Antipseudomonal penicillins and β-lactamase inhibitors | R | R | R | |
| Extended-spectrum cephalosporins | R | R | R | |
| Folate pathway inhibitors | S | S | R | |
| Penicillins + β-lactamase inhibitors | R | S | S | |
| Polymyxins | S | S | S | |
| Tetracyclines | R | R | R | |
| Resistance type | XDR | MDR | XDR | |
| 1 | 2 | 3 | |
|---|---|---|---|
| Department | IMW | IMW | SW |
| Location | Examination room | Patient room | Patient room |
| Aminoglycosides | S | S | S |
| Anti-MRSA cephalosporins | R | R | R |
| Anti-staphylococcal β-lactams (or cephamycins) | R | R | R |
| Fluoroquinolones | R | R | S |
| Folate pathway inhibitors | S | S | S |
| Glycopeptides | S | S | S |
| Glycylcyclines | S | S | S |
| Lincosamides | R | R | R |
| Lipopeptides | S | S | S |
| Macrolides | R | R | R |
| Oxazolidinones | S | S | S |
| Phenicols | S | S | S |
| Phosphonic acids | S | S | S |
| Streptogramins | S | S | S |
| Tetracyclines. | S | S | S |
| Type of resistance | MDR | MDR | MDR |
| 1 | 2 | ||
|---|---|---|---|
| Department | ICU | NU | |
| Location | Isolated room | Central Hall | |
| Antibiotics | Aminoglycosides (except streptomycin) | R | R |
| Streptomycin | S | S | |
| Carbapenems | S | S | |
| Fluoroquinolones | R | R | |
| Glycopeptides | S | S | |
| Glycylcyclines | S | S | |
| Lipopeptides | S | S | |
| Oxazolidinones | S | S | |
| Penicillins | R | R | |
| Streptogramins | R | R | |
| Tetracycline | S | S | |
| Type of resistance | MDR | MDR | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tselebonis, A.; Nena, E.; Panopoulou, M.; Kontogiorgis, C.; Bezirtzoglou, E.; Constantinidis, T. Air Contamination in Different Departments of a Tertiary Hospital. Assessment of Microbial Load and of Antimicrobial Susceptibility. Biomedicines 2020, 8, 163. https://doi.org/10.3390/biomedicines8060163
Tselebonis A, Nena E, Panopoulou M, Kontogiorgis C, Bezirtzoglou E, Constantinidis T. Air Contamination in Different Departments of a Tertiary Hospital. Assessment of Microbial Load and of Antimicrobial Susceptibility. Biomedicines. 2020; 8(6):163. https://doi.org/10.3390/biomedicines8060163
Chicago/Turabian StyleTselebonis, Athanasios, Evangelia Nena, Maria Panopoulou, Christos Kontogiorgis, Eugenia Bezirtzoglou, and Theodoros Constantinidis. 2020. "Air Contamination in Different Departments of a Tertiary Hospital. Assessment of Microbial Load and of Antimicrobial Susceptibility" Biomedicines 8, no. 6: 163. https://doi.org/10.3390/biomedicines8060163
APA StyleTselebonis, A., Nena, E., Panopoulou, M., Kontogiorgis, C., Bezirtzoglou, E., & Constantinidis, T. (2020). Air Contamination in Different Departments of a Tertiary Hospital. Assessment of Microbial Load and of Antimicrobial Susceptibility. Biomedicines, 8(6), 163. https://doi.org/10.3390/biomedicines8060163