Amino Acid Metabolites Associated with Chronic Kidney Disease: An Eight-Year Follow-Up Korean Epidemiology Study

Abstract
:1. Introduction
2. Methods
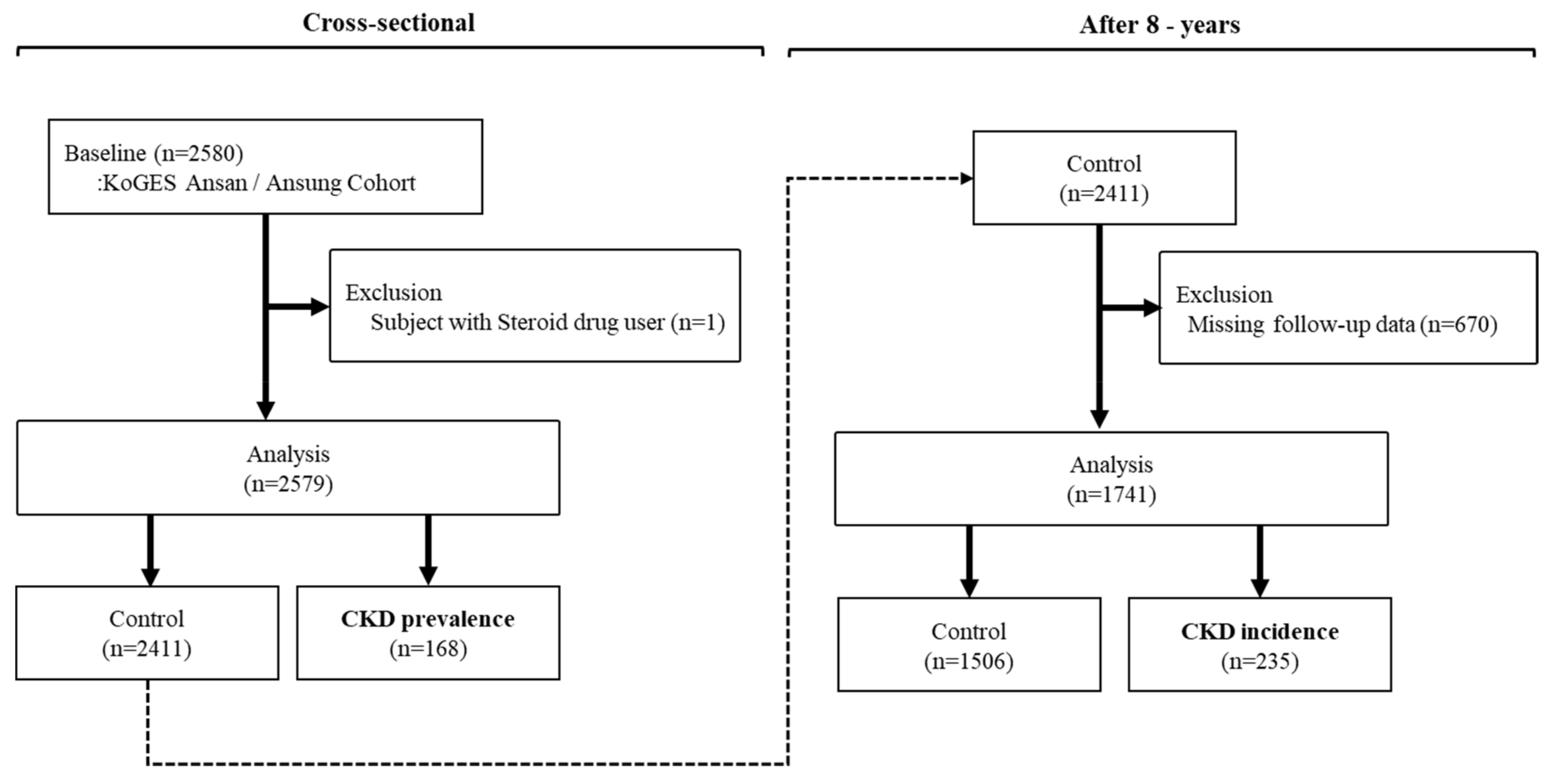
2.1. Study Population
2.2. Definitions of eGFR and CKD
2.3. General and Blood Parameters
2.4. Metabolite Level Measurements
2.5. Statistical Analyses
3. Results
3.1. Baseline Subject Characteristics
3.2. Correlations between Metabolites and eGFR
3.3. Metabolites Associated with CKD
3.4. Baseline Characteristics of Subjects with and without CKD after Eight Years
3.5. Amino Acid Metabolites as Predictive Markers of CKD
3.6. Association between Baseline hs-CRP and CKD Incidence Among Different Metabolites
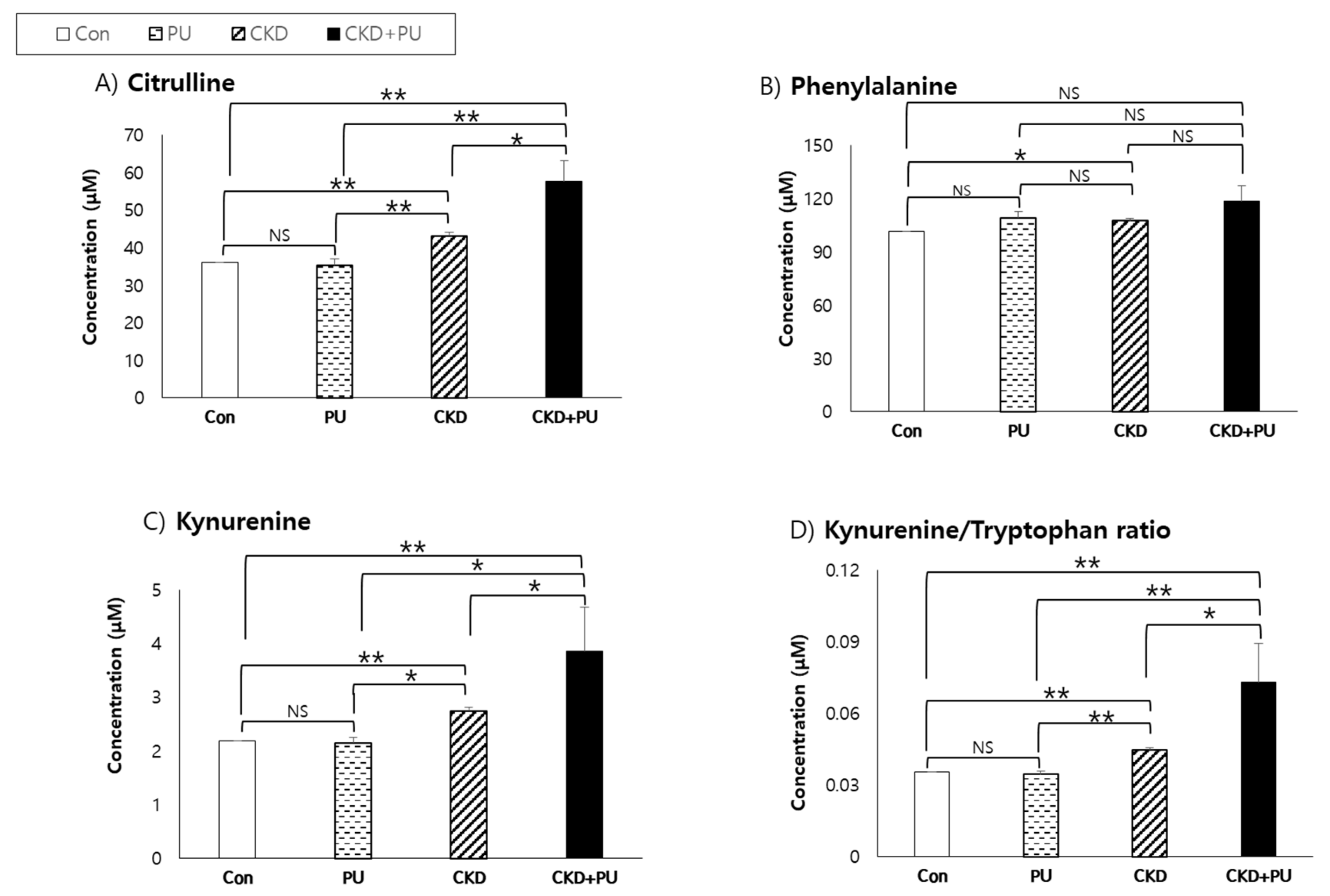
3.7. Comparison of Metabolite Concentration in Subjects with and without CKD or Proteinuria
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Richard Hobbs, F.D. Global prevalence of chronic kidney disease: A systematic review and meta-analysis. PLoS ONE 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Romagnani, P.; Remuzzi, G.; Glassock, R.; Levin, A.; Jager, K.J.; Tonelli, M.; Massy, Z.; Wanner, C.; Anders, H.J. Chronic kidney disease. Nat. Rev. Dis. Primers 2017, 3, 17088. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Massy, Z.; Argiles, A.; Spasovski, G.; Verbeke, F.; Lameire, N. Chronic kidney disease as cause of cardiovascular morbidity and mortality. Nephrol. Dial. Transplant. 2005, 20, 1048–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Astor, B.C.; Hallan, S.I.; Miller, E.R.; Yeung, E.; Coresh, J. Glomerular filtration rate, albuminuria, and risk of cardiovascular and all-cause mortality in the US population. Am. J. Epidemiol. 2008, 167, 1226–1234. [Google Scholar] [CrossRef] [Green Version]
- Abbiss, H.; Maker, G.L.; Trengove, R.D. Metabolomics approaches for the diagnosis and understanding of kidney diseases. Metabolites 2019, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, A.; Sun, H.; Qiu, S.; Wang, X. Metabolomics insights into pathophysiological mechanisms of nephrology. Int. Urol. Nephrol. 2014, 46, 1025–1030. [Google Scholar] [CrossRef]
- Weiss, R.H.; Kim, K. Metabolomics for clinical use and research in chronic kidney disease. Nat. Rev. Nephrol. 2012, 8, 22–33. [Google Scholar] [CrossRef]
- Bing, Y.U.; Zheng, Y.; Nettleton, J.A.; Alexander, D.; Coresh, J.; Boerwinkle, E. Serum metabolomic profiling and incident CKD among African Americans. Clin. J. Am. Soc. Nephrol. 2014, 9, 1410–1417. [Google Scholar]
- Rhee, E.P.; Clish, C.B.; Ghorbani, A.; Larson, M.G.; Elmariah, S.; McCabe, E.; Yang, Q.; Cheng, S.; Pierce, K.; Deik, A.; et al. A combined epidemiologic and metabolomic approach improves CKD prediction. J. Am. Soc. Nephrol. 2013, 24, 1330–1338. [Google Scholar] [CrossRef] [Green Version]
- Goek, O.N.; Prehn, C.; Sekula, P.; Romisch-Margl, W.; Doring, A.; Gieger, C.; Heier, M.; Koenig, W.; Wang-Sattler, R.; Illig, T.; et al. Metabolites associated with kidney function decline and incident chronic kidney disease in the general population. Nephrol. Dial. Transplant. 2013, 28, 2131–2138. [Google Scholar] [CrossRef] [Green Version]
- Shah, V.O.; Townsend, R.R.; Feldman, H.I.; Pappan, K.L.; Kensicki, E.; Vander, D.V. Plasma metabolomic profiles in different stages of CKD. Clin. J. Am. Soc. Nephrol. 2013, 8, 363–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duranton, F.; Lundin, U.; Gayrard, N.; Mischak, H.; Aparicio, M.; Mourad, G.; Daures, J.P.; Weinberger, K.M.; Argiles, A. Plasma and urinary amino acid metabolomic profiling in patients with different levels of kidney function. Clin. J. Am. Soc. Nephrol. 2014, 9, 37–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimura, T.; Yasuda, K.; Yamamoto, R.; Soga, T.; Rakugi, H.; Hayashi, T.; Isaka, Y. Identification of biomarkers for development of end-stage kidney disease in chronic kidney disease by metabolomic profiling. Sci. Rep. 2016, 6, 26138. [Google Scholar] [CrossRef] [PubMed]
- Breit, M.; Weinberger, K.M. Metabolic biomarkers for chronic kidney disease. Arch. Biochem. Biophys. 2016, 589, 62–80. [Google Scholar] [CrossRef]
- Kim, K.; Aronov, P.; Zakharkin, S.O.; Anderson, D.; Perroud, B.; Thompson, I.M.; Weiss, R.H. Urine metabolomics analysis for kidney cancer detection and biomarker discovery. Mol. Cell. Proteomics 2008, 8, 558–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Han, B.G. Cohort profile: The Korean genome and epidemiology study (KoGES) consortium. Int. J. Epidemiol. 2017, 46, 1350. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Lente, F.V.; Greene, T.; et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Lee, J.; Choi, J.Y.; Kwon, Y.K.; Lee, D.H.; Jung, H.Y.; Ryu, H.M.; Cho, J.H.; Ryu, D.H.; Kim, Y.L.; Hwang, G.S. Changes in serum metabolites with the stage of chronic kidney disease: Comparison of diabetes and non-diabetes. Clin. Chim. Acta 2016, 459, 123–131. [Google Scholar] [CrossRef]
- Rhee, E.P.; Clish, C.B.; Wenger, J.; Roy, J.; Elmariah, S.; Pierce, K.A.; Bullock, K.; Anderson, A.H.; Gerszten, R.E.; Feldman, H.I. Metabolomics of CKD progression: A case-control analysis in the chronic renal insufficiency cohort study. Am. J. Nephrol. 2016, 43, 366–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goek, O.N.; Doring, A.; Gieger, C.; Heier, M.; Koenig, W.; Prehn, C.; Romisch-Margl, W.; Wang-Sattler, R.; Illig, T.; Suhre, K.; et al. Serum metabolite concentrations and decreased GFR in the general population. Am. J. Kidney Dis. 2012, 60, 197–206. [Google Scholar] [CrossRef]
- Fouque, D.; Holt, S.; Guebre-Egziabher, F.; Nakamura, K.; Vianey-Saban, C.; Hadj-Aissa, A.; Hoppel, C.L.; Kopple, J.D. Relationship between serum carnitine, acylcarnitines, and renal function in patients with chronic renal disease. J. Ren. Nutr. 2006, 16, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Xia, F.Y.; Zhu, L.; Xu, C.; Wu, Q.Q.; Chen, W.J.; Zeng, R.; Deng, Y.Y. Plasma acylcarnitines could predict prognosis and evaluate treatment of lgA nephropathy. Nutr. Metab. 2019, 16, 2. [Google Scholar] [CrossRef] [Green Version]
- Shima, R.; Nakanishi-Ueda, T.; Yamamoto, Y. Simultaneous determination of methionine sulfoxide and methionine in blood plasma using gas chromatography-mass spectrometry. Anal. Biochem. 2003, 313, 28–33. [Google Scholar]
- Morris, S.M.; Gao, T.; Cooper, T.K.; Kepka-Lenhart, D.; Awad, A.S. Arginase-2 mediates diabetic renal injury. Diabetes 2011, 60, 3015–3022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curis, E.; Nicolis, I.; Moinard, C.; Osowska, S.; Zerrouk, N.; Benazeth, S.; Cynober, L. Almost all about citrulline in mammals. Amino Acids 2005, 29, 177–205. [Google Scholar] [CrossRef]
- Solomonson, L.P.; Flam, R.F.; Pendleton, L.C.; Goodwin, B.L.; Eichler, D.C. The caveolar nitric oxide synthase/arginine regeneration system for NO production in endothelial cells. J. Exp. Biol. 2003, 206, 2083–2087. [Google Scholar] [CrossRef] [Green Version]
- Campos, K.L.; Giovanelli, J.; Kaufman, S. Characteristics of the nitric oxide synthase-catalyzed conversion of arginine to N-hydroxyarginine, the first oxygenation step in the enzymic synthesis of nitric oxide. J. Biol. Chem. 1995, 270, 1721–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saito, K.; Fujigaki, S.; Heyes, M.P.; Shibata, K.; Takemura, M.; Fujii, H.; Wada, H.; Noma, A.; Seishima, M. Mechanism of increases in L-kynurenine and quinolinic acid in renal insufficiency. Am. J. Physiol. Renal. Physiol. 2000, 279, F565–F572. [Google Scholar] [CrossRef] [Green Version]
- Emmanouel, D.S.; Jaspan, J.B.; Kuku, S.F.; Rubenstein, A.H.; Katz, A.I.; Huen, A.H. Pathogenesis and characterization of hyperglucagonemia in the uremic rat. J. Clin. Investig. 1976, 58, 1266–1272. [Google Scholar] [CrossRef] [Green Version]
- Mawal, M.R.; Deshmukh, D.R. Purification and properties of kynurenine aminotransferase from rat kidney. Biochem. J. 1991, 279, 595–599. [Google Scholar] [CrossRef] [Green Version]
- Buchi, R.; Alberati-Gani, D.; Malherbe, P.; Kohler, C.; Broger, C.; Cesura, A.M. Cloning and functional expression of a soluble form of kynurenine/-aminoadipate aminotransferase from rat kidney. J. Biol. Chem. 1995, 270, 29330–29335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debnath, S.; Velagapudi, C.; Redus, L.; Thameem, F.; Kasinath, B.; Hura, C.E.; Lorenzo, C.; Abboud, H.E.; O’Connor, J.C. Tryptophan metabolism in patients with chronic kidney disease secondary to type 2 diabetes: Relationship to inflammatory markers. Int. J. Tryptophan. Res. 2017, 10, 1–9. [Google Scholar] [CrossRef]
- Christmas, D.M.; Potokar, J.; Davies, S.J. A biological pathway linking inflammation and depression: Acibation of indoleamine 2,3-dioxygenase. Neuropsychiatr. Dis. Treat. 2011, 7, 431–439. [Google Scholar]
- Stone, T.W.; Darlington, L.G. The kynurenine pathway as a therapeutic target in cognitive and neurodegenerative disorders. Br. J. Pharmacol. 2013, 169, 1211–1227. [Google Scholar] [CrossRef]
- Shankar, A.; Sun, L.; Klein, B.E.; Lee, K.E.; Muntner, P.; Nieto, F.J.; Tsai, M.Y.; Cruickshanks, K.J.; Schubert, C.R.; Brazy, P.C.; et al. Markers of inflammation predict the long-term risk of developing chronic kidney disease: A population-based cohort study. Kidney Int. 2011, 80, 1231–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, L.W.; Hoy, W.E.; Wang, Z. The association between C-reactive protein levels and the risk for chronic kidney disease hospitalizations in adults of a remote indigenous Australian community: A prospective cohort study. Nephrology 2017, 22, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Kugler, E.; Cohen, E.; Goldberg, E.; Nardi, Y.; Leve, A.; Krause, I.; Garty, M.; Krause, I. C reactive protein and long-term risk for chronic kidney disease: A historical prospective study. J. Nephrol. 2015, 28, 321–327. [Google Scholar] [CrossRef]
- Schefold, J.C.; Zeden, J.P.; Fotopoulou, C.; von Haehling, S.; Pschowski, R.; Hasper, D.; Volk, H.D.; Schuett, C.; Reinke, P. Increased IDO activity and elevated serum levels of tryptophanh carabolities in patients with CKD a possible mechanism. Nephrol. Dial. Transplant. 2009, 24, 1901–1908. [Google Scholar] [CrossRef] [Green Version]
- Møller, N.; Meek, S.; Bigelow, M.; Andrews, J.; Nair, K.S. The kidney is an important site for in vivo phenylalanine-to-tyrosine conversion in adult humans: A metabolic role of the kidney. Proc. Natl. Acad. Sci. USA 2000, 97, 1242–1246. [Google Scholar] [CrossRef] [Green Version]
- Tizianello, A.; Ferrari, G.D.; Garibotto, G.; Gurreri, G.; Robaudo, C. Renal metabolism of amino acids and ammonia in subjects with normal renal function and in patients with chronic renal insufficiency. J. Clin. Investig. 1980, 65, 1162–1173. [Google Scholar] [CrossRef]
- Wang, M.; Vyhmeister, I.; Swendseid, M.E.; Kopple, J.D. Phenylalanine hydroxylase and tyrosine aminotransferase activities in chronically uremic rats. J. Nutr. 1975, 105, 122–127. [Google Scholar] [CrossRef]
- Jones, M.R.; Kopple, J.D.; Swendseid, M.E. Phenylalanine metabolism in uremic and normal man. Kidney Int. 1978, 14, 169–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furst, P.; Alvesstrand, A.; Bergstrom, J. Effects of nutrition and catabolic stress on intracellular amino acid pools in uremia. Am. J. Clin. Nutr. 1980, 33, 1387–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopple, J.D.; Blumenkrantz, M.J.; Jones, M.R.; Moran, J.K.; Coburn, J.W. Plasma amino acid levels and amino acid losses during continuous ambulatory peritoneal dialysis. Am. J. Clin. Nutr. 1982, 36, 395–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenda, R.; Hemmelgarn, M.D.; Braden, J.M.; Anita, L.; Matthew, T.J.; Scott, K.; Robert, R.; Quinn, N.W.; Math, P.; Marcello, T. Relation between kidney function, proteinuria, and adverse outcomes. JAMA 2010, 303, 423–429. [Google Scholar]
- Methven, S.; MacGregor, M.S.; Traynor, J.P.; Hair, M.; O’Reilly, D.S.; Deighan, C.J. Comparison of urinary albumin and urinary total protein as predictors of patient outcomes in CKD. Am. J. Kidney Dis. 2011, 57, 21–28. [Google Scholar] [CrossRef]
- Luo, S.; Coresh, J.; Tin, A.; Rebholz, M.C.; Appel, L.J.; Chen, J.; Vasan, R.S.; Anderson, A.H.; Feldman, H.I.; Kimmel, P.L.; et al. Serum metabolomic alterations associated with proteinuria in CKD. Clin. J. Am. Soc. Nephrol. 2019, 14, 342–353. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Control | CKD | p† | p†† | |
|---|---|---|---|---|
| Participants (%) | 2411 (93.5) | 168 (6.5) | – | – |
| Age (years) | 56.5 ± 8.9 | 65.2 ± 6.8 | <0.0001 | – |
| Sex (%) | 0.0983 | – | ||
| Male | 1149 (47.7) | 69 (41.1) | ||
| Female | 1262 (52.3) | 99 (58.9) | ||
| Drinking status (%) | <0.0001 | – | ||
| Never | 1124 (46.4) | 101 (60.1) | ||
| Former | 123 (5.1) | 16 (9.5) | ||
| Current | 1163 (48.3) | 51 (30.4) | ||
| Smoking status (%) | 0.3250 | – | ||
| Never | 1472 (61.1) | 104 (61.9) | ||
| Former | 437 (18.1) | 36 (21.4) | ||
| Current | 501 (20.8) | 28 (16.7) | ||
| Proteinuria | <0.0001 | |||
| Urine protein < 1 | 2368 (98.4) | 156 (92.9) | ||
| Urine protein ≥ 1+ | 39 (1.6) | 12 (7.1) | ||
| Comorbidities | ||||
| Hypertension (%) | 810 (33.6) | 102 (60.7) | <0.0001 | – |
| Diabetes mellitus (%) | 533 (22.2) | 55 (32.7) | 0.0016 | – |
| Body mass index (kg/m2) | 24.5 ± 3.2 | 25.1 ± 3.4 | 0.0538 | 0.1130 |
| Systolic blood pressure (mm Hg) | 117.8 ± 16.7 | 122.0 ± 16.9 | 0.0009 | 0.0042 |
| Diastolic blood pressure (mm Hg) | 78.6 ± 10.3 | 78.9 ± 9.5 | 0.5560 | 0.0088 |
| Blood urea nitrogen (mg/dL) | 15.5 ± 4.1 | 18.4 ± 5.5 | <0.0001 | <0.0001 |
| Creatinine (mg/dL) | 0.96 ± 0.14 | 1.25 ± 0.49 | <0.0001 | <0.0001 |
| e-GFR (mL/min/1.73 m2) | 79.3 ± 11.0 | 53.0 ± 7.2 | <0.0001 | <0.0001 |
| Glucose (mg/dL) | 95.7 ± 19.3 | 97.7 ± 27.5 | 0.3983 | 0.5775 |
| HbA1C (%) | 5.7 ± 0.8 | 5.9 ± 0.7 | <0.0001 | 0.8804 |
| Hs-CRP (mg/L) | 1.6 ± 3.5 | 2.3 ± 5.9 | 0.0003 | 0.4572 |
| Metabolite | r * | p |
|---|---|---|
| C3 (Propionylcarnitine) | –0.10 | <0.0001 |
| C4 (Butyrylcarnitine) | –0.20 | <0.0001 |
| C7-DC (Pimelylcarnitine) | –0.10 | <0.0001 |
| C8 (Octanoylcarnitine) | –0.11 | <0.0001 |
| C14:2 (Tetradecadienylcarnitine) | –0.09 | <0.0001 |
| Alanine | –0.10 | <0.0001 |
| Arginine | –0.12 | <0.0001 |
| Asparagine | –0.10 | <0.0001 |
| Citrulline | –0.21 | <0.0001 |
| Glutamine | –0.09 | <0.0001 |
| Glycine | –0.11 | <0.0001 |
| Histidine | –0.08 | <0.0001 |
| Isoleucine | –0.13 | <0.0001 |
| Leucine | –0.10 | <0.0001 |
| Methionine | –0.10 | <0.0001 |
| Phenylalanine | –0.09 | <0.0001 |
| Proline | –0.12 | <0.0001 |
| Valine | –0.09 | <0.0001 |
| Acetylornithine | –0.16 | <0.0001 |
| Kynurenine | –0.24 | <0.0001 |
| Putrescine | –0.09 | <0.0001 |
| Sarcosine | –0.09 | <0.0001 |
| PCaaC28:1 | –0.07 | 0.0003 |
| PCaaC42:5 | 0.08 | 0.0001 |
| SMOHC14:1 | –0.09 | <0.0001 |
| SMOHC16:1 | –0.08 | <0.0001 |
| SMOHC22:2 | –0.08 | <0.0001 |
| SMC18:1 | –0.08 | <0.0001 |
| Metabolites | OR (CIs) † |
|---|---|
| C3 (Propionylcarnitine) | 3.41 (2.08–5.60) |
| C4 (Butyrylcarnitine) | 4.76 (3.06–7.40) |
| C7-DC (Pimelylcarnitine) | 1.94 (1.27–2.97) |
| C8 (Octanoylcarnitine) | 1.92 (1.26–2.91) |
| C14:2 (Tetradecadienylcarnitine) | 1.39 (0.99–1.95) |
| Alanine | 4.37 (2.06–9.29) |
| Arginine | 4.94 (2.66–9.20) |
| Asparagine | 3.75 (1.72–8.15) |
| Citrulline | 10.42 (5.34–20.14) |
| Glutamine | 2.20 (0.99–4.87) |
| Glycine | 2.56 (1.25–5.23) |
| Histidine | 3.23 (1.37–7.62) |
| Isoleucine | 4.29 (2.00–9.19) |
| Leucine | 3.83 (1.65–8.92) |
| Methionine | 5.35 (2.78–10.29) |
| Phenylalanine | 4.33 (1.57–11.88) |
| Proline | 3.71 (2.08–6.60) |
| Valine | 2.75 (1.08–7.01) |
| Acetylornithine | 2.38 (1.77–3.20) |
| Kynurenine | 13.81 (7.38–25.86) |
| Putrescine | 1.37 (1.05–1.78) |
| Sarcosine | 1.70 (1.19–2.44) |
| PCaaC28:1 | 2.16 (1.12–4.16) |
| PCaaC40:5 | 0.98 (0.64–1.52) |
| SMOHC14:1 | 1.35 (0.69–2.65) |
| SMOHC16:1 | 1.23 (0.65–2.33) |
| SMOHC22:2 | 1.53 (0.77–3.04) |
| SMC18:1 | 2.09 (1.07–4.08) |
| Citrulline/Arginine | 1.41 (0.88–2.27) |
| Glycine/Serine | 12.37 (4.79–31.96) |
| Phenylalanine/Tyrosine | 5.65 (1.88–17.00) |
| Kynurenine/Tryptophan | 12.65 (6.55–24.44) |
| Control | CKD Incidence | p† | p†† | |
|---|---|---|---|---|
| Participants (%) | 1506 (86.5) | 235 (13.5) | – | – |
| Age (years) | 54.8 ± 8.3 | 62.3 ± 7.6 | <0.0001 | – |
| Sex (%) | 0.1338 | – | ||
| Male | 707 (47.0) | 98 (41.7) | ||
| Female | 799 (53.0) | 137 (58.3) | ||
| Drinking status (%) | 0.0009 | – | ||
| Never | 698 (45.1) | 135 (57.5) | ||
| Former | 61 (4.1) | 14 (6.0) | ||
| Current | 747 (49.6) | 86 (36.6) | ||
| Smoking status (%) | 0.2660 | – | ||
| Never | 945 (62.8) | 160 (68.1) | ||
| Former | 270 (17.9) | 38 (16.2) | ||
| Current | 291 (19.3) | 37 (15.7) | ||
| Proteinuria | <0.0001 | |||
| Urine protein < 1 | 1484 (99.1%) | 223 (95.7%) | ||
| Urine protein ≥ 1+ | 13 (0.9%) | 10 (4.3%) | ||
| Comorbidities | ||||
| Hypertension (%) | 449 (29.8) | 111 (47.2) | <0.0001 | – |
| Diabetes mellitus (%) | 297 (19.8) | 53 (22.6) | 0.3208 | – |
| Body mass index (kg/m2) | 24.6 ± 3.1 | 25.1 ± 3.6 | 0.0372 | 0.0274 |
| Systolic blood pressure (mm Hg) | 116.6 ± 15.9 | 121.4 ± 16.8 | <0.0001 | 0.7207 |
| Diastolic blood pressure (mm Hg) | 78.4 ± 10.1 | 79.5 ± 10.1 | 0.1843 | 0.8209 |
| Blood urea nitrogen (mg/dL) | 15.4 ± 4.0 | 16.3 ± 3.9 | 0.0002 | 0.1366 |
| Creatinine (mg/dL) | 0.95 ± 0.14 | 0.99 ± 0.14 | 0.0008 | <0.0001 |
| e-GFR (mL/min/1.73 m2) | 91.1 ± 14.2 | 85.3 ± 13.2 | <0.0001 | <0.0001 |
| Glucose (mg/dL) | 95.4 ± 18.7 | 96.1 ± 18.9 | 0.4086 | 0.7544 |
| Hemoglobin A1C (%) | 5.7 ± 0.7 | 5.9 ± 0.8 | <0.0001 | 0.0023 |
| Hs-CRP (mg/L) | 1.5 ± 2.6 | 2.5 ± 6.6 | <0.0001 | 0.0033 |
| Metabolites | OR (95% CI) † |
|---|---|
| Citrulline | 2.41 (1.26–4.59) |
| Kynurenine | 1.98 (1.05–3.73) |
| Phenylalanine | 2.68 (1.00–7.16) |
| Kynurenine:tryptophan | 3.20 (1.57–6.51) |
| Variables | Multiple Amino Acid Metabolites † | C Statistics | p | |
|---|---|---|---|---|
| Base Model | Base Model + Metabolites | |||
| OR per SD | 1.06 (1.04–1.09) | 0.76 | 0.85 | <0.0001 †† |
| Net reclassification improvement (Category-free) | 0.84 (0.72–0.96) | <0.0001 | ||
| Integrated discrimination improvement | 0.12 (0.10–0.14) | <0.0001 | ||
| OR (95% CI) | |
|---|---|
| Model 1 † | 1.045 (1.005–1.086) |
| Model 2 †† | |
| Adj. Model 1 + kynurenine | 1.042 (1.003–1.083) |
| Adj. Model 1 + kynurenine:tryptophan | 1.033 (0.996–1.073) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Jang, H.B.; Yoo, M.-G.; Park, S.I.; Lee, H.-J. Amino Acid Metabolites Associated with Chronic Kidney Disease: An Eight-Year Follow-Up Korean Epidemiology Study. Biomedicines 2020, 8, 222. https://doi.org/10.3390/biomedicines8070222
Lee H, Jang HB, Yoo M-G, Park SI, Lee H-J. Amino Acid Metabolites Associated with Chronic Kidney Disease: An Eight-Year Follow-Up Korean Epidemiology Study. Biomedicines. 2020; 8(7):222. https://doi.org/10.3390/biomedicines8070222
Chicago/Turabian StyleLee, Hansongyi, Han Byul Jang, Min-Gyu Yoo, Sang Ick Park, and Hye-Ja Lee. 2020. "Amino Acid Metabolites Associated with Chronic Kidney Disease: An Eight-Year Follow-Up Korean Epidemiology Study" Biomedicines 8, no. 7: 222. https://doi.org/10.3390/biomedicines8070222
APA StyleLee, H., Jang, H. B., Yoo, M. -G., Park, S. I., & Lee, H. -J. (2020). Amino Acid Metabolites Associated with Chronic Kidney Disease: An Eight-Year Follow-Up Korean Epidemiology Study. Biomedicines, 8(7), 222. https://doi.org/10.3390/biomedicines8070222