Association between Serum Zinc and Calcification Propensity (T50) in Patients with Type 2 Diabetes Mellitus and In Vitro Effect of Exogenous Zinc on T50

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethics Statement
2.3. Participants of the Cross Sectional Study
2.4. Physical and Laboratory Measurements, and Other Clinical Infromation
2.5. Devices, Plastic Materials, and Chemicals
2.6. Determination of Calcification Propensity (T50)
2.7. In Vitro Experiment to Examine Direct Effect of Exogenous Zinc on T50
2.8. Statistics
3. Results
3.1. Clinical Characteristics of Type 2 Diabetes Patients
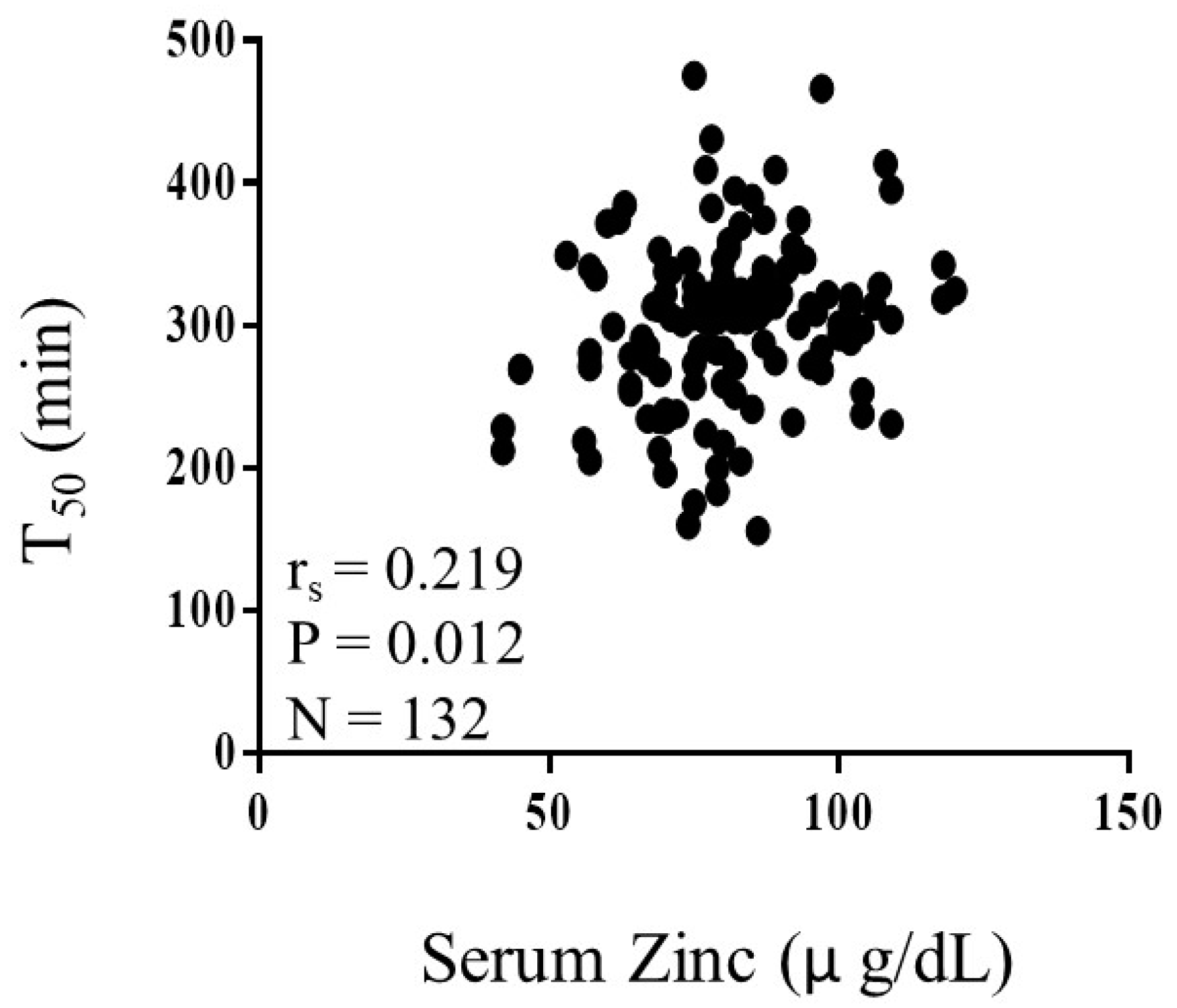
3.2. Correlations between Serum Calcification Propensity and Clinical Factors in Patients with Type 2 Diabetes Mellitus
3.3. Independent Association between Serum Calcification Propensity and Zinc in Patients with Type 2 Diabetes Mellitus
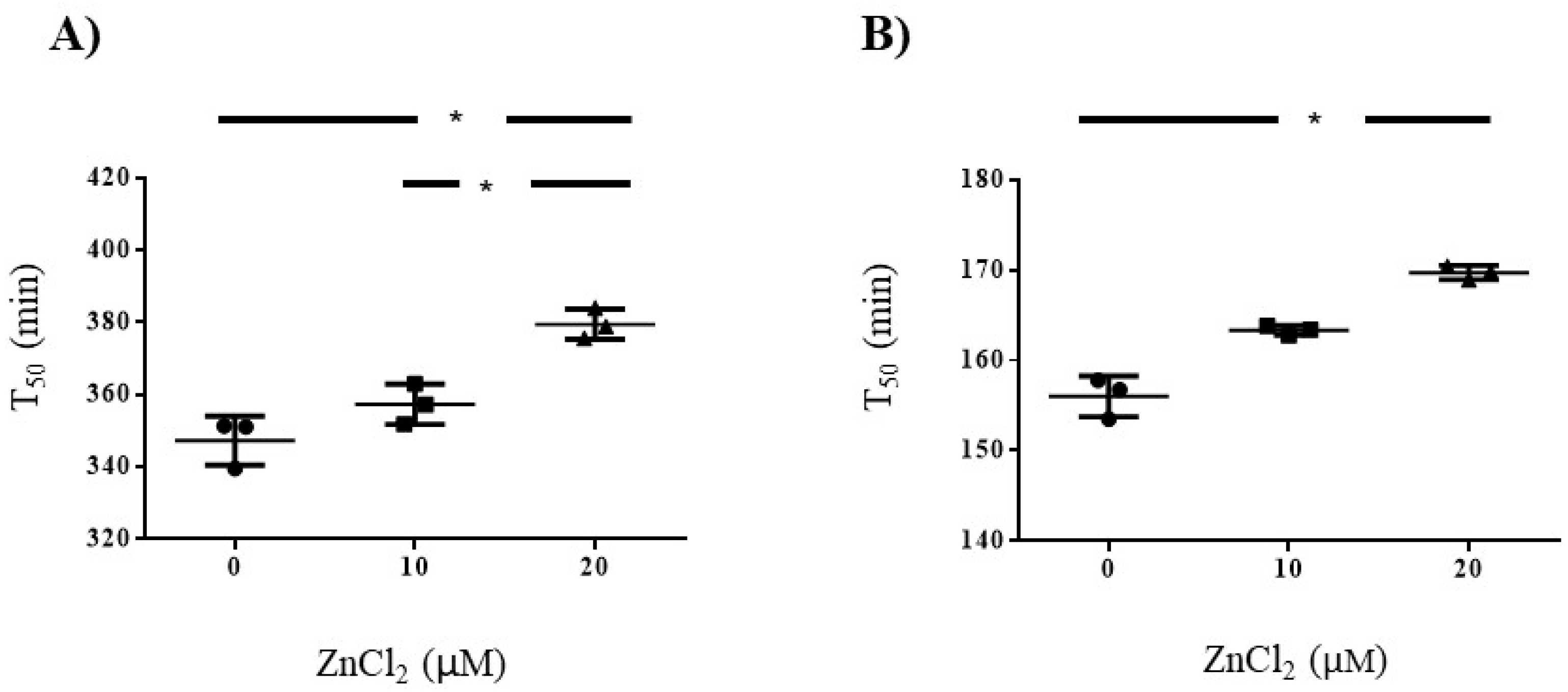
3.4. Influence of Zinc on Serum Calcification Propensity in Pooled Serum Samples Volunterres from Healthy Volunteers and Patients with Hemodialysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Raghavan, S.; Vassy, J.L.; Ho, Y.; Song, R.J.; Gagnon, D.R.; Cho, K.; Wilson, P.W.F.; Phillips, L.S. Diabetes Mellitus–Related All-Cause and Cardiovascular Mortality in a National Cohort of Adults. J. Am. Heart Assoc. 2019, 8, e011295. [Google Scholar] [CrossRef] [Green Version]
- Niskanen, L.; Siitonen, O.; Suhonen, M.; Uusitupa, M.I. Medial Artery Calcification Predicts Cardiovascular Mortality in Patients with NIDDM. Diabetes Care 1994, 17, 1252–1256. [Google Scholar] [CrossRef] [PubMed]
- Go, A.; Chertow, G.; Fan, D.; McCulloch, C.; Hsu, C. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef]
- Gorriz, J.L.; Molina, P.; Cerverón, M.J.; Vila, R.; Bover, J.; Nieto, J.; Barril, G.; Martínez-Castelao, A.; Fernández, E.; Escudero, V.; et al. Vascular Calcification in Patients with Nondialysis CKD over 3 Years. Clin. J. Am. Soc. Nephrol. 2015, 10, 654–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanzer, P.; Boehm, M.; Sorribas, V.; Thiriet, M.; Janzen, J.; Zeller, T.; Hilaire, C.S.; Shanahan, C.M. Medial vascular calcification revisited: Review and perspectives. Eur. Heart J. 2014, 35, 1515–1525. [Google Scholar] [CrossRef] [PubMed]
- Avogaro, A.; Fadini, G.P. Mechanisms of ectopic calcification: Implications for diabetic vasculopathy. Cardiovasc. Diagn. Ther. 2015, 5, 343–352. [Google Scholar]
- Houben, E.; Neradova, A.; Schurgers, L.J.; Vervloet, M. The influence of phosphate, calcium and magnesium on matrix Gla-protein and vascular calcification: A systematic review. G. Ital. Nefrol. 2016, 33, gin/33.6.5. [Google Scholar]
- Reynolds, J.L.; Joannides, A.J.; Skepper, J.N.; McNair, R.; Schurgers, L.J.; Proudfoot, D.; Jahnen-Dechent, W.; Weissberg, P.L.; Shanahan, C.M. Human Vascular Smooth Muscle Cells Undergo Vesicle-Mediated Calcification in Response to Changes in Extracellular Calcium and Phosphate Concentrations: A Potential Mechanism for Accelerated Vascular Calcification in ESRD. J. Am. Soc. Nephrol. 2004, 15, 2857–2867. [Google Scholar] [CrossRef] [Green Version]
- London, G.M. Mechanisms of arterial calcifications and consequences for cardiovascular function. Kidney Int. Suppl. 2013, 3, 442–445. [Google Scholar] [CrossRef] [Green Version]
- Demer, L.L.; Tintut, Y. Mineral exploration: Search for the mechanism of vascular calcification and beyond: The 2003 Jeffrey M. Hoeg Award lecture. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 1739–1743. [Google Scholar] [CrossRef] [Green Version]
- Wallin, R.; Wajih, N.; Greenwood, G.T.; Sane, D.C. Arterial calcification: A review of mechanisms, animal models, and the prospects for therapy. Med. Res. Rev. 2001, 21, 274–301. [Google Scholar] [CrossRef] [PubMed]
- Jablonski, K.L.; Chonchol, M. Vascular calcification in end-stage renal disease. Hemodial. Int. 2013, 17, S17–S21. [Google Scholar] [CrossRef] [Green Version]
- Cozzolino, M.; Gallieni, M.; Brancaccio, D. Vascular Calcification in Uremic Conditions: New Insights into Pathogenesis. Semin. Nephrol. 2006, 26, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Sato, H.; Doi, H.; Yoshida, C.A.; Shimizu, T.; Matsui, H.; Yamazaki, M.; Akiyama, H.; Kawai-Kowase, K.; Iso, T.; et al. Runx2 Represses Myocardin-Mediated Differentiation and Facilitates Osteogenic Conversion of Vascular Smooth Muscle Cells. Mol. Cell. Biol. 2007, 28, 1147–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, K.; Inaba, M. Diabetees and Vascular Calcification: Diabetes and Aging-Related Complications; Springer: Tokyo, Japan, 2017; pp. 59–68. [Google Scholar]
- Sinha, A.; Vyavahare, N. High-glucose levels and elastin degradation products accelerate osteogenesis in vascular smooth muscle cells. Diabetes Vasc. Dis. Res. 2013, 10, 410–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiss, A.; Jahnen-Dechent, W.; Endo, H.; Schwahn, D. Structural dynamics of a colloidal protein-mineral complex bestowing on calcium phosphate a high solubility in biological fluids. Biointerphases 2007, 2, 16–20. [Google Scholar] [CrossRef] [Green Version]
- Heiss, A.; Duchesne, A.; Denecke, B.; Grötzinger, J.; Yamamoto, K.; Renné, T.; Jahnen-Dechent, W. Structural Basis of Calcification Inhibition by α2-HS Glycoprotein/Fetuin-A formation of colloidal calciprotein particles. J. Biol. Chem. 2003, 278, 13333–13341. [Google Scholar] [CrossRef] [Green Version]
- Pasch, A.; Farese, S.; Gräber, S.; Wald, J.; Richtering, W.; Floege, J.; Jahnen-Dechent, W. Nanoparticle-Based Test Measures Overall Propensity for Calcification in Serum. J. Am. Soc. Nephrol. 2012, 23, 1744–1752. [Google Scholar] [CrossRef]
- Smith, E.R.; Ford, M.L.; Tomlinson, L.A.; Bodenham, E.; McMahon, L.P.; Farese, S.; Rajkumar, C.; Holt, S.G.; Pasch, A. Serum Calcification Propensity Predicts All-Cause Mortality in Predialysis CKD. J. Am. Soc. Nephrol. 2014, 25, 339–348. [Google Scholar] [CrossRef]
- Pasch, A.; Block, G.A.; Bachtler, M.; Smith, E.R.; Jahnen-Dechent, W.; Arampatzis, S.; Chertow, G.M.; Parfrey, P.; Ma, X.; Floege, J. Blood Calcification Propensity, Cardiovascular Events, and Survival in Patients Receiving Hemodialysis in the EVOLVE Trial. Clin. J. Am. Soc. Nephrol. 2017, 12, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Keyzer, C.A.; De Borst, M.H.; van den Berg, E.; Jahnen-Dechent, W.; Arampatzis, S.; Farese, S.; Bergmann, I.P.; Floege, J.; Navis, G.; Bakker, S.J.; et al. Calcification Propensity and Survival among Renal Transplant Recipients. J. Am. Soc. Nephrol. 2016, 27, 239–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahle, D.O.; Åsberg, A.; Hartmann, A.; Holdaas, H.; Bachtler, M.; Jenssen, T.G.; Dionisi, M.; Pasch, A. Serum Calcification Propensity Is a Strong and Independent Determinant of Cardiac and All-Cause Mortality in Kidney Transplant Recipients. Am. J. Transplant. 2016, 16, 204–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silaghi, C.N.; Ilyés, T.; Van Ballegooijen, A.J.; Crăciun, A.M. Calciprotein Particles and Serum Calcification Propensity: Hallmarks of Vascular Calcifications in Patients with Chronic Kidney Disease. J. Clin. Med. 2020, 9, 1287. [Google Scholar] [CrossRef] [PubMed]
- Bielesz, B.; Reiter, T.; Marculescu, R.; Gleiss, A.; Bojic, M.; Kieweg, H.; Cejka, D. Calcification Propensity of Serum is Independent of Excretory Renal Function. Sci. Rep. 2017, 7, 17941. [Google Scholar] [CrossRef] [Green Version]
- Jono, S.; McKee, M.D.; Murry, C.E.; Shioi, A.; Nishizawa, Y.; Mori, K.; Morii, H.; Giachelli, C.M. Phosphate regulation of vascular smooth muscle cell calcification. Circ. Res. 2000, 87, e10–e17. [Google Scholar] [CrossRef]
- Block, G.A.; Hulbert-Shearon, T.E.; Levin, N.W.; Port, F.K. Association of serum phosphorus and calcium x phosphate product with mortality risk in chronic hemodialysis patients: A national study. Am. J. Kidney Dis. 1998, 31, 607–617. [Google Scholar] [CrossRef]
- Foley, R.N.; Collins, A.J.; Ishani, A.; Kalra, P.A. Calcium-phosphate levels and cardiovascular disease in community-dwelling adults: The Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 2008, 156, 556–563. [Google Scholar] [CrossRef]
- Chasapis, C.; Loutsidou, A.C.; Spiliopoulou, C.; Stefanidou, M.E. Zinc and human health: An update. Arch. Toxicol. 2012, 86, 521–534. [Google Scholar] [CrossRef]
- Kodama, H.; Tanaka, M.; Naito, Y.; Katayama, K.; Moriyama, M. Japan’s Practical Guidelines for Zinc Deficiency with a Particular Focus on Taste Disorders, Inflammatory Bowel Disease, and Liver Cirrhosis. Int. J. Mol. Sci. 2020, 21, 2941. [Google Scholar] [CrossRef]
- Kondaiah, P.; Yaduvanshi, P.S.; Sharp, P.A.; Pullakhandam, R. Iron and Zinc Homeostasis and Interactions: Does Enteric Zinc Excretion Cross-Talk with Intestinal Iron Absorp:tion? Nutrients 2019, 11, 1885. [Google Scholar] [CrossRef] [Green Version]
- Kiilerich, S.; Hvid-Jacobsen, K.; Vaag, A.; Sørensen, S.S. 65 Zinc absorption in patients with insulin-dependent diabetes mellitus assessed by whole-body counting technique. Clin. Chim. Acta 1990, 189, 13–18. [Google Scholar] [CrossRef]
- Cunningham, J.J.; Fu, A.; Mearkle, P.L.; Brown, R.G. Hyperzincuria in individuals with insulin-dependent diabetes mellitus: Concurrent zinc status and the effect of high-dose zinc supplementation. Metabolism 1994, 43, 1558–1562. [Google Scholar] [CrossRef]
- Kazi, T.G.; Afridi, H.I.; Kazi, N.; Jamali, M.K.; Arain, M.B.; Jalbani, N.; Kandhro, G.A. Copper, Chromium, Manganese, Iron, Nickel, and Zinc Levels in Biological Samples of Diabetes Mellitus Patients. Biol. Trace Element Res. 2008, 122, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Makhlough, A.; Makhlough, M.; Shokrzadeh, M.; Mohammadian, M.; Sedighi, O.; Faghihan, M. Comparing the Levels of Trace Elements in Patients with Diabetic Nephropathy and Healthy Individuals. Nephro-Urol. Mon. 2015, 7, 28576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, J.; Karges, W.; Rink, L. Zinc and diabetes—Clinical links and molecular mechanisms. J. Nutr. Biochem. 2009, 20, 399–417. [Google Scholar] [CrossRef]
- Jayawardena, R.; Ranasinghe, P.; Galappatthy, P.; Malkanthi, R.; Constantine, G.R.; Katulanda, P. Effects of zinc supplementation on diabetes mellitus: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2012, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voelkl, J.; Tuffaha, R.; Luong, T.T.D.; Zickler, D.; Masyout, J.; Feger, M.; Verheyen, N.; Blaschke, F.; Kuro, O.M.; Tomaschitz, A.; et al. Zinc Inhibits Phosphate-Induced Vascular Calcification through TNFAIP3-Mediated Suppression of NF-kappaB. J. Am. Soc. Nephrol. 2018, 29, 1636–1648. [Google Scholar] [CrossRef] [Green Version]
- Sonoda, M.; Shoji, T.; Kuwamura, Y.; Okute, Y.; Naganuma, T.; Shima, H.; Motoyama, K.; Morioka, T.; Mori, K.; Fukumoto, S.; et al. Plasma homocysteine and cerebral small vessel disease as possible mediators between kidney and cognitive functions in patients with diabetes mellitus. Sci. Rep. 2017, 7, 4382. [Google Scholar] [CrossRef] [Green Version]
- Seino, Y.; Nanjo, K.; Tajima, N.; Kadowaki, T.; Kashiwagi, A.; Araki, E.; Ito, C.; Inagaki, N.; Iwamoto, Y.; Kasuga, M.; et al. Report of the committee on the classification and diagnostic criteria of diabetes mellitus. J. Diabetes Investig. 2010, 1, 212–228. [Google Scholar] [CrossRef] [Green Version]
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2002, 25, s5–s20. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised Equations for Estimated GFR From Serum Creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Payne, R.B.; Little, A.J.; Williams, R.B.; Milner, J.R. Interpretation of Serum Calcium in Patients with Abnormal Serum Proteins. Br. Med. J. 1973, 4, 643–646. [Google Scholar] [CrossRef] [Green Version]
- Schweikle, M.; Bjørnøy, S.H.; Van Helvoort, A.T.J.; Haugen, H.J.; Sikorski, P.; Tiainen, H. Stabilisation of amorphous calcium phosphate in polyethylene glycol hydrogels. Acta Biomater. 2019, 90, 132–145. [Google Scholar] [CrossRef] [PubMed]
- Gross, K.A.; Komarovska, L.; Viksna, A. Efficient zinc incorporation into hydroxyapatite through crystallization of an amorphous phase could extend the properties of zinc apatites. J. Aust. Ceram. Soc. 2013, 49, 129–135. [Google Scholar]
- Kanazaki, N.; Onuma, K.; Trboux, G.; Tusumi, S.; Ito, A. Inhibitory Effect of Magnesium and Zinc on Crystallization Kinetics of Hydroxyapatite (0001) Face. J. Phys. Chem. B 2000, 104, 4189–4194. [Google Scholar] [CrossRef]
- Pham, P.-C.T.; Pham, S.V.; Miller, J.M. Hypomagnesemia in Patients with Type 2 Diabetes. Clin. J. Am. Soc. Nephrol. 2007, 2, 366–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wälti, M.K.; Zimmermann, M.B.; Walczyk, T.; Spinas, G.A.; Hurrell, R.F. Measurement of magnesium absorption and retention in type 2 diabetic patients with the use of stable isotopes. Am. J. Clin. Nutr. 2003, 78, 448–453. [Google Scholar] [CrossRef] [Green Version]
- Barbagallo, M.; Dominguez, L.J.; Galioto, A.; Ferlisi, A.; Cani, C.; Malfa, L.; Pineo, A.; Busardo, A.; Paolisso, G. Role of magnesium in insulin action, diabetes and cardio-metabolic syndrome X. Mol. Asp. Med. 2003, 24, 39–52. [Google Scholar] [CrossRef]
- Louvet, L.; Büchel, J.; Steppan, S.; Passlick-Deetjen, J.; Massy, Z.A. Magnesium prevents phosphate-induced calcification in human aortic vascular smooth muscle cells. Nephrol. Dial. Transplant. 2013, 28, 869–878. [Google Scholar] [CrossRef] [Green Version]
- Nagy, A.; Pethő, D.; Gáll, T.; Zavaczki, E.; Nyitrai, M.; Posta, J.; Zarjou, A.; Agarwal, A.; Balla, G.; Balla, J. Zinc Inhibits HIF-Prolyl Hydroxylase Inhibitor-Aggravated VSMC Calcification Induced by High Phosphate. Front. Physiol. 2019, 10, 1584. [Google Scholar] [CrossRef] [Green Version]
- Blaine, J.; Chonchol, M.; Levi, M. Renal Control of Calcium, Phosphate, and Magnesium Homeostasis. Clin. J. Am. Soc. Nephrol. 2015, 10, 1257–1272. [Google Scholar] [CrossRef]
- Bressendorff, I.; Hansen, D.; Schou, M.; Silver, B.; Pasch, A.; Bouchelouche, P.; Pedersen, L.; Rasmussen, L.M.; Brandi, L. Oral Magnesium Supplementation in Chronic Kidney Disease Stages 3 and 4: Efficacy, Safety, and Effect on Serum Calcification Propensity—A Prospective Randomized Double-Blinded Placebo-Controlled Clinical Trial. Kidney Int. Rep. 2017, 2, 380–389. [Google Scholar] [CrossRef] [Green Version]
- Giroux, E.L.; Henkin, R.I. Competition for zinc among serum albumin and amino acids. Biochim. Biophys. Acta (BBA) Gen. Subj. 1972, 273, 64–72. [Google Scholar] [CrossRef]
- Handing, K.B.; Shabalin, I.G.; Kassaar, O.; Khazaipoul, S.; Blindauer, C.A.; Stewart, A.J.; Chruszcz, M.; Minor, W. Circulatory zinc transport is controlled by distinct interdomain sites on mammalian albumins. Chem. Sci. 2016, 7, 6635–6648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruthur, N.; Clark, J.M.; Fu, M.; Kao, W.H.L.; Shuldiner, A.R. Effect of zinc supplementation on insulin secretion: Interaction between zinc and SLC30A8 genotype in Old Order Amish. Diabetologia 2014, 58, 295–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidarian, E.; Amini, M.; Parham, M.; Aminorroaya, A. Effect of Zinc Supplementation on Serum Homocysteine in Type 2 Diabetic Patients with Microalbuminuria. Rev. Diabet. Stud. 2009, 6, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Parham, M.; Amini, M.; Aminorroaya, A.; Heidarian, E. Effect of Zinc Supplementation on Microalbuminuria in Patients With Type 2 Diabetes: A Double Blind, Randomized, Placebo-Controlled, Cross-Over Trial. Rev. Diabet. Stud. 2008, 5, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Roussel, A.-M.; Kerkeni, A.; Zouari, N.; Mahjoub, S.; Matheau, J.-M.; Anderson, R.A. Antioxidant Effects of Zinc Supplementation in Tunisians with Type 2 Diabetes Mellitus. J. Am. Coll. Nutr. 2003, 22, 316–321. [Google Scholar] [CrossRef]
- Capdor, J.; Foster, M.; Petocz, P.; Samman, S. Zinc and glycemic control: A meta-analysis of randomised placebo controlled supplementation trials in humans. J. Trace Elem. Med. Biol. 2013, 27, 137–142. [Google Scholar] [CrossRef]
- Foster, M.; Petocz, P.; Samman, S. Effects of zinc on plasma lipoprotein cholesterol concentrations in humans: A meta-analysis of randomised controlled trials. Atherosclerosis 2010, 210, 344–352. [Google Scholar] [CrossRef]
- Soinio, M.; Marniemi, J.; Laakso, M.; Lehto, S.; Rönnemaa, T.; Pyöräla, K. Serum Zinc Level and Coronary Heart Disease Events in Patients With Type 2 Diabetes. Diabetes Care 2007, 30, 523–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, S.; Samman, S. The effect of zinc supplementation in humans on plasma lipids, antioxidant status and thrombogenesis. J. Am. Coll. Nutr. 2006, 25, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Leitzmann, M.F.; Stampfer, M.J.; Wu, K.; Colditz, G.A.; Willett, W.C.; Giovannucci, E.L. Zinc supplement use and risk of prostate cancer. J. Natl. Cancer Inst. 2003, 95, 1004–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandra, R.K. Excessive intake of zinc impairs immune responses. JAMA 1984, 252, 1443–1446. [Google Scholar] [CrossRef]
- Ciceri, P.; Elli, F.; Braidotti, P.; Falleni, M.; Tosi, D.; Bulfamante, G.; Block, G.A.; Cozzolino, M. Iron citrate reduces high phosphate-induced vascular calcification by inhibiting apoptosis. Atherosclerosis 2016, 254, 93–101. [Google Scholar] [CrossRef]
- Mammadova-Bach, E.; Braun, A. Zinc Homeostasis in Platelet-Related Diseases. Int. J. Mol. Sci. 2019, 20, 5258. [Google Scholar] [CrossRef] [Green Version]
- Marx, G. Zinc binding to fibrinogen and fibrin. Arch. Biochem. Biophys. 1988, 266, 285–288. [Google Scholar] [CrossRef]
- Knez, M.; Pantovic, A.; Zekovic, M.; Pavlovic, Z.; Glibetić, M.; Zec, M.M. Is There a Link between Zinc Intake and Status with Plasma Fatty Acid Profile and Desaturase Activities in Dyslipidemic Subjects? Nutrients 2019, 12, 93. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, M.; Tonelli, J.; Kishore, P.; Stein, D.; Ragucci, E.; Gitig, A.; Reddy, K. Contribution of elevated free fatty acid levels to the lack of glucose effectiveness in type 2 diabetes. Diabetes 2003, 52, 2748–2758. [Google Scholar] [CrossRef] [Green Version]
- Salgin, B.; Ong, K.K.; Thankamony, A.; Emmett, P.; Wareham, N.J.; Dunger, D.B.; Thankamony, A.; Taylor-Robinson, D. Higher Fasting Plasma Free Fatty Acid Levels Are Associated with Lower Insulin Secretion in Children and Adults and a Higher Incidence of Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2012, 97, 3302–3309. [Google Scholar] [CrossRef] [Green Version]
- Coverdale, J.P.C.; Khazaipoul, S.; Arya, S.; Stewart, A.J.; Blindauer, C.A. Crosstalk between zinc and free fatty acids in plasma. Biochim. Biophys. Acta (BBA) Mol. Cell Biol. Lipids 2019, 1864, 532–542. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Stewart, A.J.; Sleep, D.; Sadler, P.J.; Pinheiro, T.J.T.; Blindauer, C.A. A Molecular Mechanism for Modulating Plasma Zn Speciation by Fatty Acids. J. Am. Chem. Soc. 2012, 134, 1454–1457. [Google Scholar] [CrossRef] [PubMed]
- Barnett, J.P.; Blindauer, C.A.; Kassaar, O.; Khazaipoul, S.; Martin, E.M.; Sadler, P.J.; Stewart, A.J. Allosteric modulation of zinc speciation by fatty acids. Biochim. Biophys. Acta (BBA) Gen. Subj. 2013, 1830, 5456–5464. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Measurement | Median (IQR) or Percentage |
|---|---|
| Age (years) | 71 (65–75) |
| Male/female, n (%) | 78 (59.1)/54 (40.9) |
| Body mass index (kg/m2) | 24.5 (21.8–27.0) |
| T50 (min) | 306 (269–332) |
| eGFR (mL/min/1.73 m2) | 59.0 (37.6–73.9) |
| Creatinine (mg/dL) | 0.87 (0.69–1.36) |
| Blood urea nitrogen (mg/dL) | 17 (15–23) |
| Serum albumin (g/dL) | 4.1 (3.8–4.3) |
| Fasting plasma glucose (mg/dL) | 119 (99–143) |
| HbA1c (%) | 8.0 (7.1–9.2) |
| Corrected calcium (mg/dL) | 9.4 (9.2–9.7) |
| Phosphate (mg/dL) | 3.8 (3.4–4.2) |
| Magnesium (mg/dL) | 2.1 (2.0–2.3) |
| Zinc (µg/dL) | 80.0 (70.1–89.8) |
| Whole PTH (pg/mL) | 21.6 (16.4–31.2) |
| Intact PTH (pg/mL) | 36 (27–54) |
| Urine albumin to creatinine ratio (mg/gCr) | 17 (6–212) |
| Systolic blood pressure (mmHg) | 125 (110–138) |
| Diastolic blood pressure (mmHg) | 65 (60–74) |
| Current smoker (%) | 65 (49.2) |
| Use of mediations | |
| Antihypertensive (%) | 79 (59.8) |
| Statin (%) | 64 (48.4) |
| Insulin (%) | 63 (47.7) |
| Anti-diabetic agent (%) | 98 (74.2) |
| Complications | |
| Retinopathy (%) | 37 (28.2) |
| Neuropathy (%) | 66 (50.0) |
| Any prior cardiovascular disease (%) | 21 (15.9) |
| Clinical Variables | Correlation with T50 | |
|---|---|---|
| rs | p | |
| Age | −0.222 | 0.010 |
| Body mass index | 0.013 | 0.886 |
| eGFR | 0.199 | 0.022 |
| Creatinine | −0.170 | 0.051 |
| Blood urea nitrogen | −0.213 | 0.011 |
| Serum albumin | 0.313 | 0.0003 |
| Fasting plasma glucose | 0.282 | 0.001 |
| HbA1 | 0.166 | 0.057 |
| Corrected calcium | 0.132 | 0.132 |
| Phosphate | −0.227 | 0.009 |
| Magnesium | 0.113 | 0.195 |
| Zinc | 0.219 | 0.012 |
| Whole-PTH | −0.117 | 0.183 |
| Intact-PTH | −0.110 | 0.183 |
| Urine albumin to creatinine ratio | −0.247 | 0.004 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| β | p | β | p | |
| Age | −0.077 | 0.412 | −0.056 | 0.544 |
| Sex (female = 0. male = 1) | 0.042 | 0.633 | 0.035 | 0.692 |
| Any Prior cardiovascular disease | −0.143 | 0.112 | −0.139 | 0.117 |
| Current smoking (no = 0, yes = 1) | −0.142 | 0.094 | −0.135 | 0.105 |
| eGFR | 0.172 | 0.155 | 0.096 | 0.438 |
| Urinary albumin-creatinine ratio | 0.004 | 0.968 | 0.028 | 0.783 |
| Corrected calcium | 0.228 | 0.010 | 0.199 | 0.021 |
| Phosphate | −0.328 | 0.0007 | −0.317 | 0.0008 |
| Magnesium | 0.226 | 0.009 | 0.216 | 0.011 |
| Zinc | 0.213 | 0.038 | 0.229 | 0.024 |
| HbA1c | –0.054 | 0.537 | - | - |
| Fasting plasma glucose | - | - | 0.171 | 0.053 |
| R2 | 0.244 | 0.265 | ||
| (p < 0.001) | (p < 0.001) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakatani, S.; Mori, K.; Sonoda, M.; Nishide, K.; Uedono, H.; Tsuda, A.; Emoto, M.; Shoji, T. Association between Serum Zinc and Calcification Propensity (T50) in Patients with Type 2 Diabetes Mellitus and In Vitro Effect of Exogenous Zinc on T50. Biomedicines 2020, 8, 337. https://doi.org/10.3390/biomedicines8090337
Nakatani S, Mori K, Sonoda M, Nishide K, Uedono H, Tsuda A, Emoto M, Shoji T. Association between Serum Zinc and Calcification Propensity (T50) in Patients with Type 2 Diabetes Mellitus and In Vitro Effect of Exogenous Zinc on T50. Biomedicines. 2020; 8(9):337. https://doi.org/10.3390/biomedicines8090337
Chicago/Turabian StyleNakatani, Shinya, Katsuhito Mori, Mika Sonoda, Kozo Nishide, Hideki Uedono, Akihiro Tsuda, Masanori Emoto, and Tetsuo Shoji. 2020. "Association between Serum Zinc and Calcification Propensity (T50) in Patients with Type 2 Diabetes Mellitus and In Vitro Effect of Exogenous Zinc on T50" Biomedicines 8, no. 9: 337. https://doi.org/10.3390/biomedicines8090337
APA StyleNakatani, S., Mori, K., Sonoda, M., Nishide, K., Uedono, H., Tsuda, A., Emoto, M., & Shoji, T. (2020). Association between Serum Zinc and Calcification Propensity (T50) in Patients with Type 2 Diabetes Mellitus and In Vitro Effect of Exogenous Zinc on T50. Biomedicines, 8(9), 337. https://doi.org/10.3390/biomedicines8090337