
Extracorporeal Shock Wave Enhanced Exogenous Mitochondria into Adipose-Derived Mesenchymal Stem Cells and Further Preserved Heart Function in Rat Dilated Cardiomyopathy

 , , , , and
, , , , and 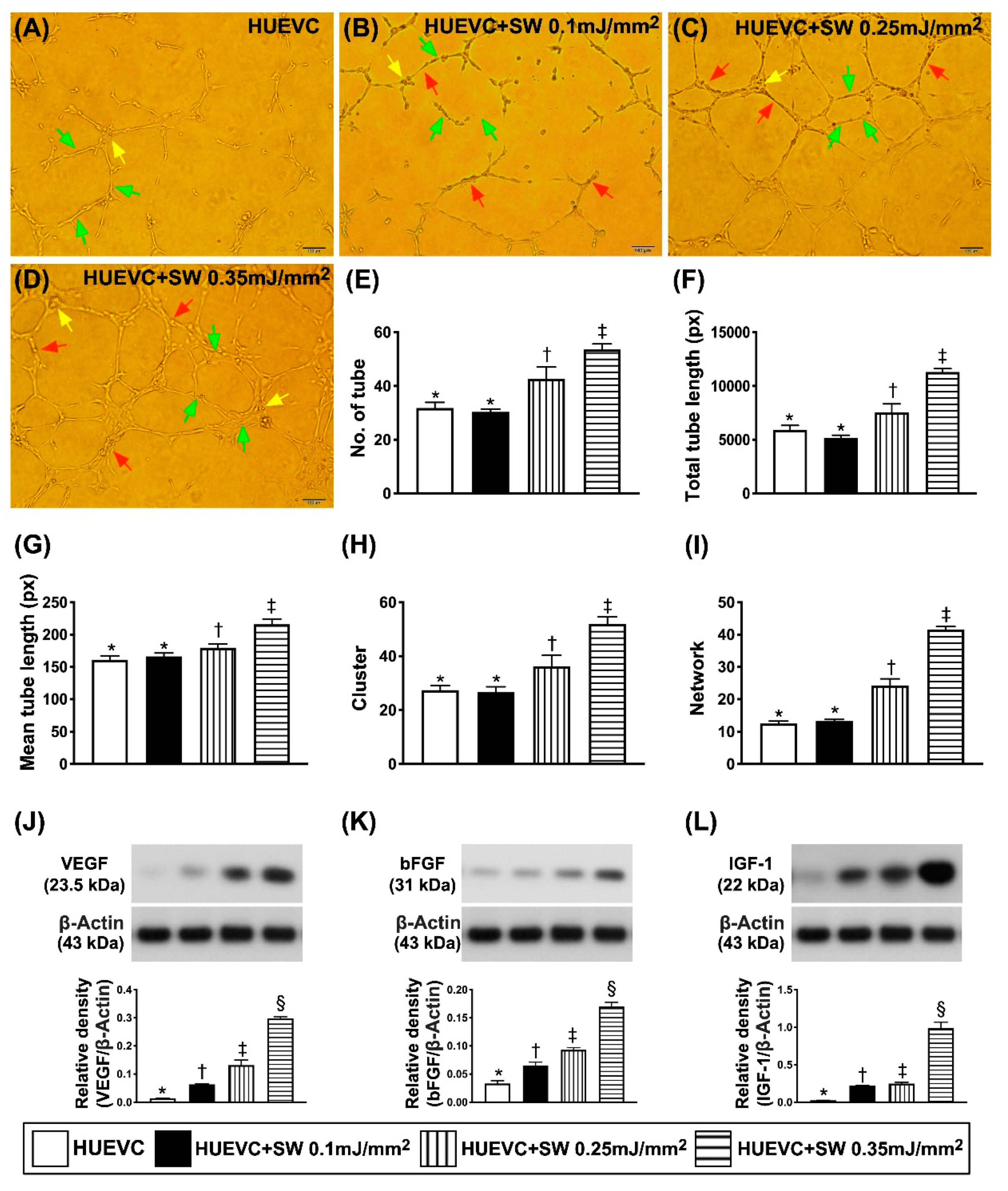{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. In Vitro Study Using the Human Umbilical Vein Endothelial Cells (Huvecs) to Determine the Impact of Stepwise Increased Ecsw on Augmenting Angiogenesis
2.3. Procedure and Protocol of DCM Induction by Doxorubicin and Animal Grouping
2.4. Mito Isolation and MitoTracker Staining for Mito
2.5. Mito DNA Copy Number in ADMSCs
2.6. Measurement of Left Ventricular Ejection Fraction by Echocardiography
2.7. Western Blot Analysis of Left Ventricular Tissues
2.8. Immunofluorescent (IF) Staining
2.9. Histological Quantification of Myocardial Size and Myocardial Fibrosis Area
2.10. Flow Cytometric Analysis for Assessment of Circulating Levels of Endothelial Progenitor Cells (EPCs) and Mesenchymal Stem Cells (MSCs) Based on Surface Markers
2.11. Statistical Analysis
3. Results
3.1. An Increase in Angiogenesis in Cellular and Protein Levels was Energy-Dependent Undergoing ECSW Therapy
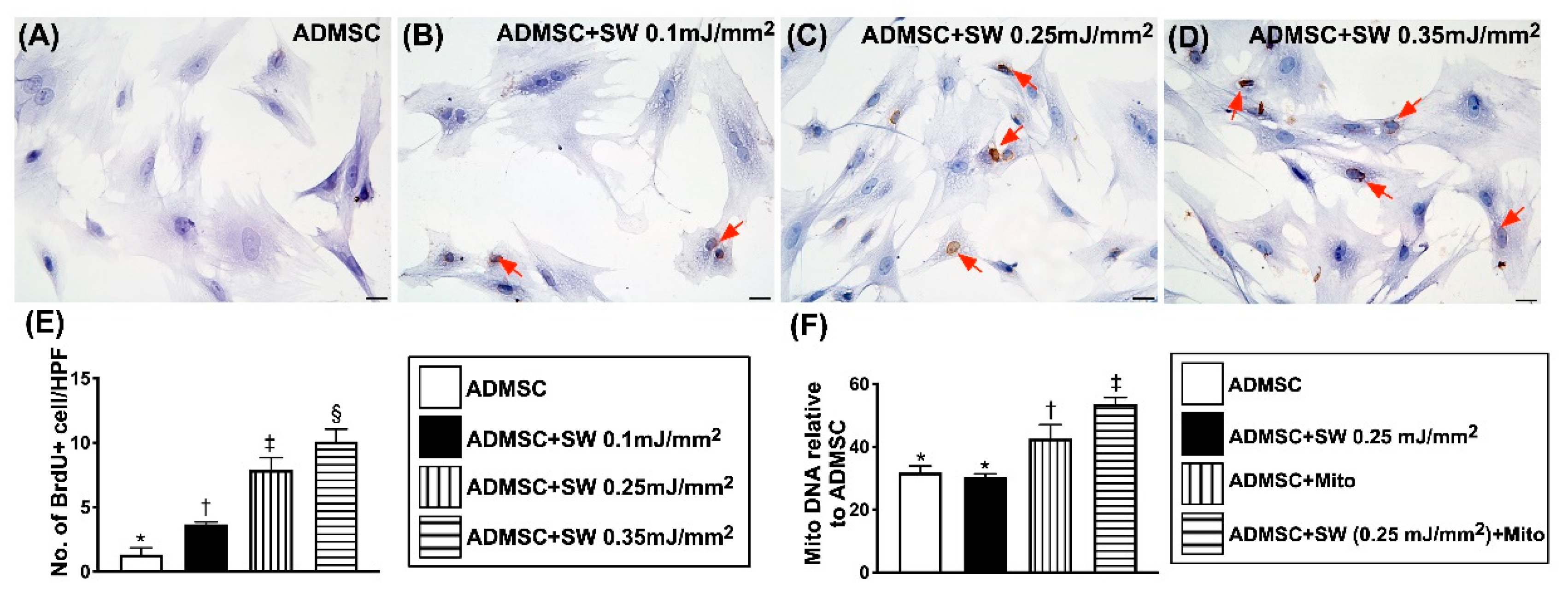
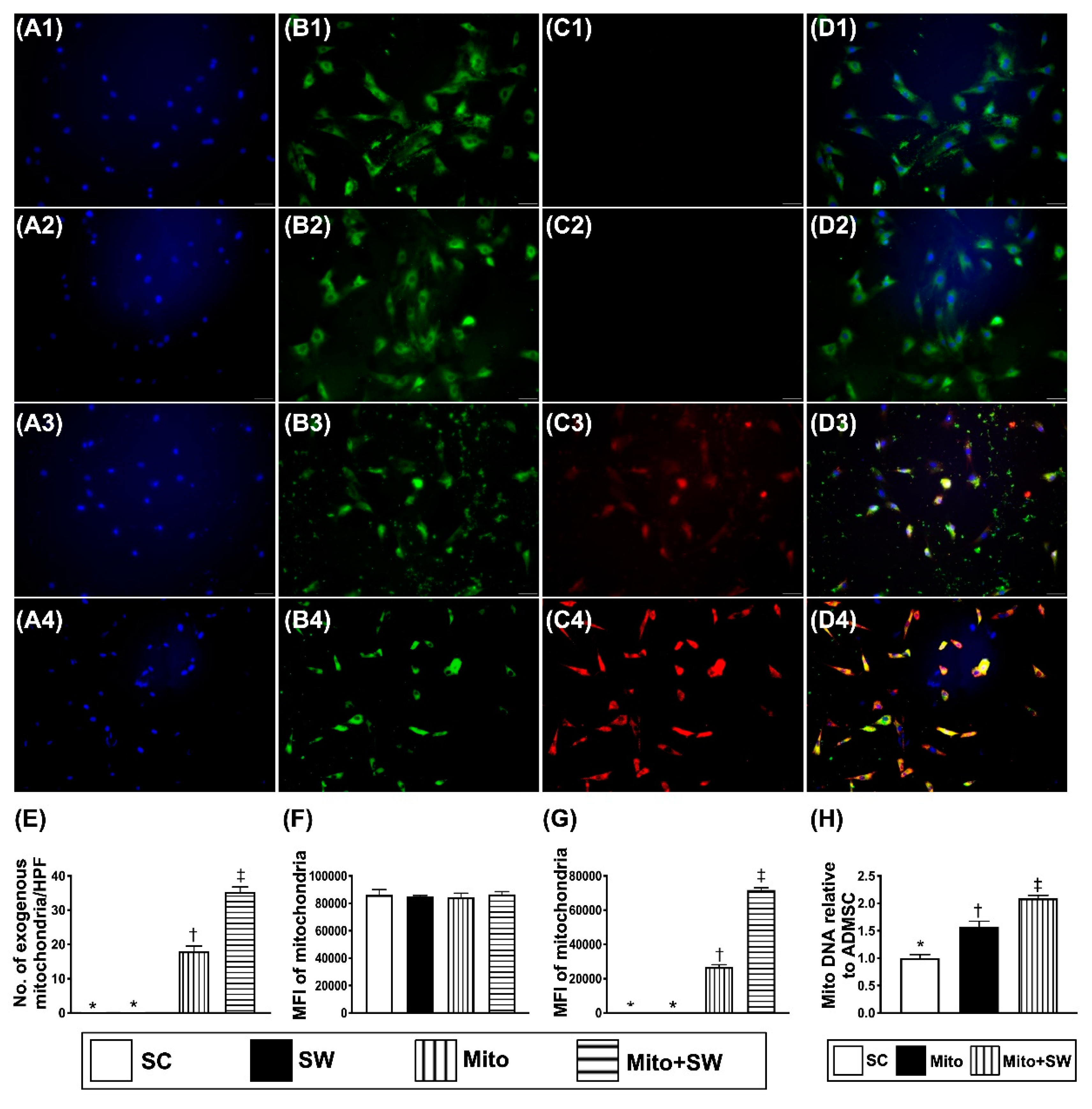
3.2. ECSW Therapy Augmented Exogenous Mitochondria into ADMSCs
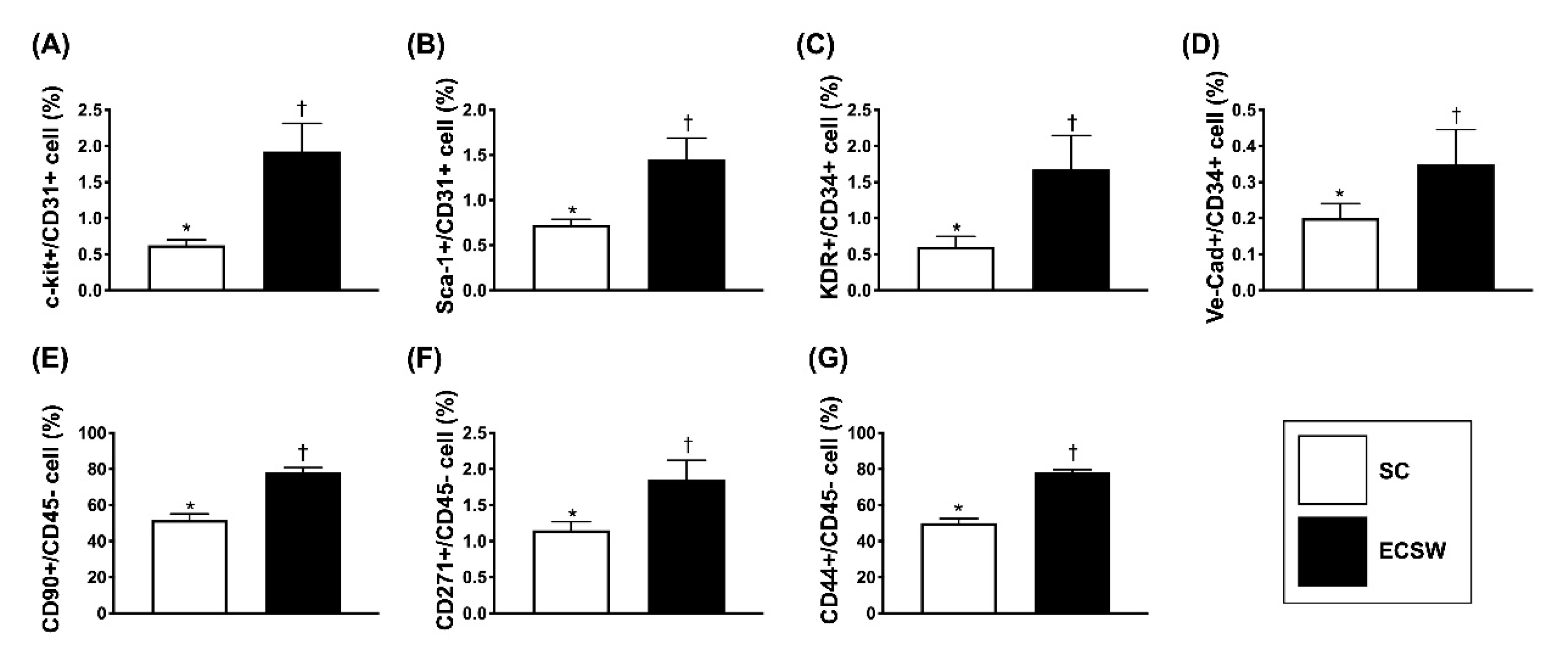
3.3. The ECSW Therapy Enhanced Circulating Levels of Endothelial Progenitor Cells (EPCs) and MSCs
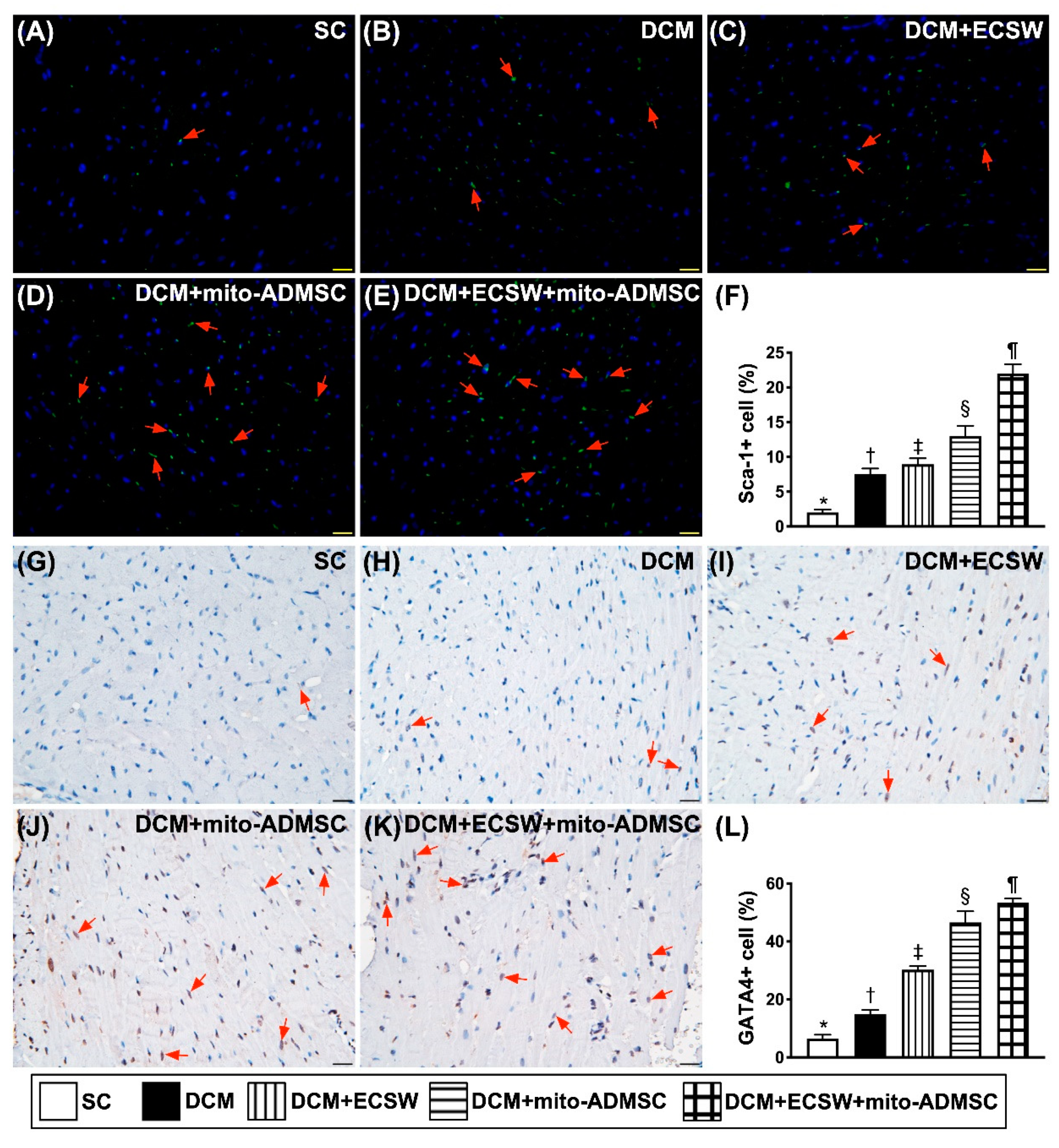
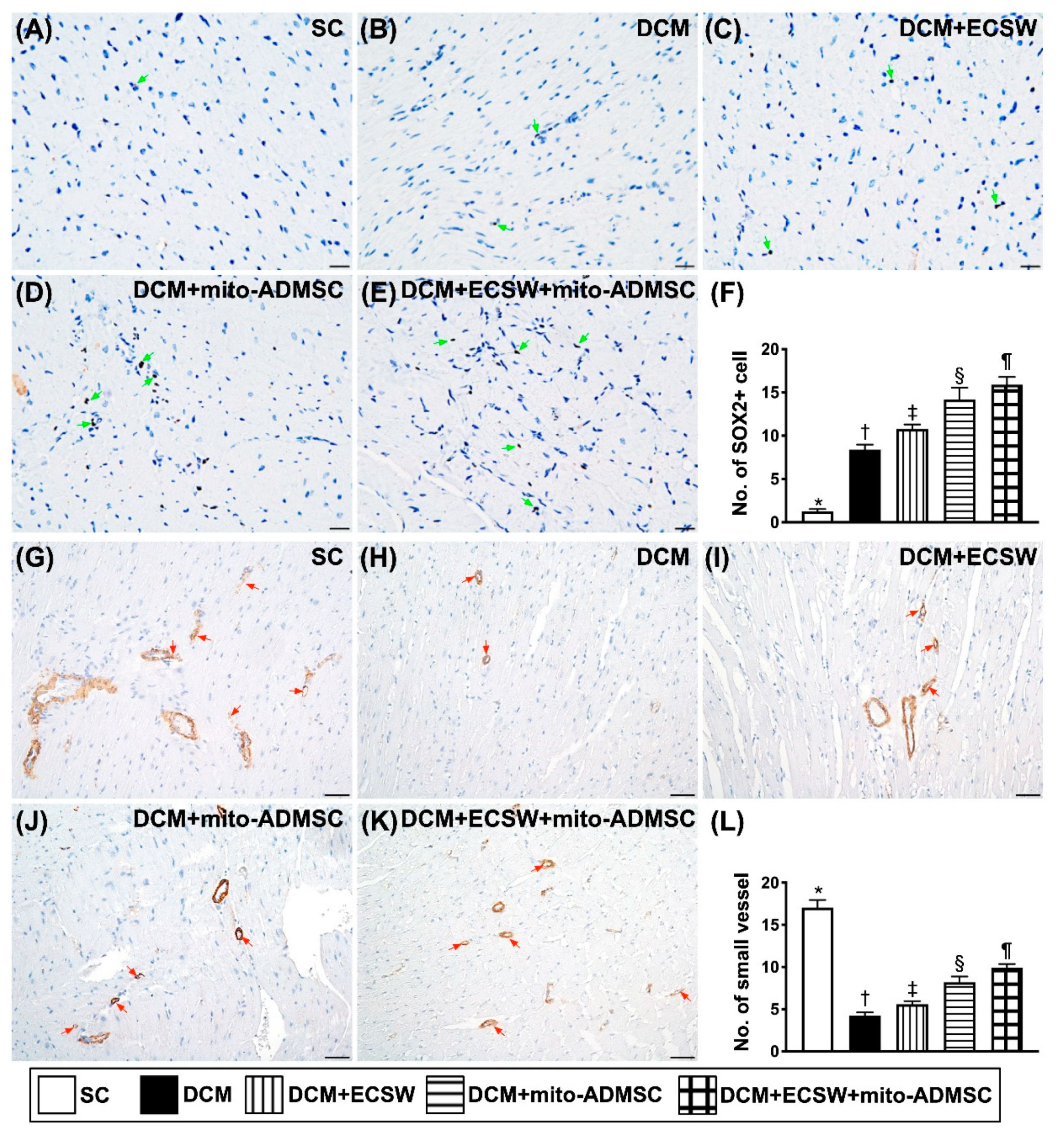
3.4. Cardiac Stem Cells (CSCs), Cardiac and Pluripotent Markers and Small Vessel Number Were Upregulated by Combined ECSW-Assisted Mitochondrial Delivery into ADMSCs + ECSW Therapy in LV Myocardium 7 Weeks after DCM Induction
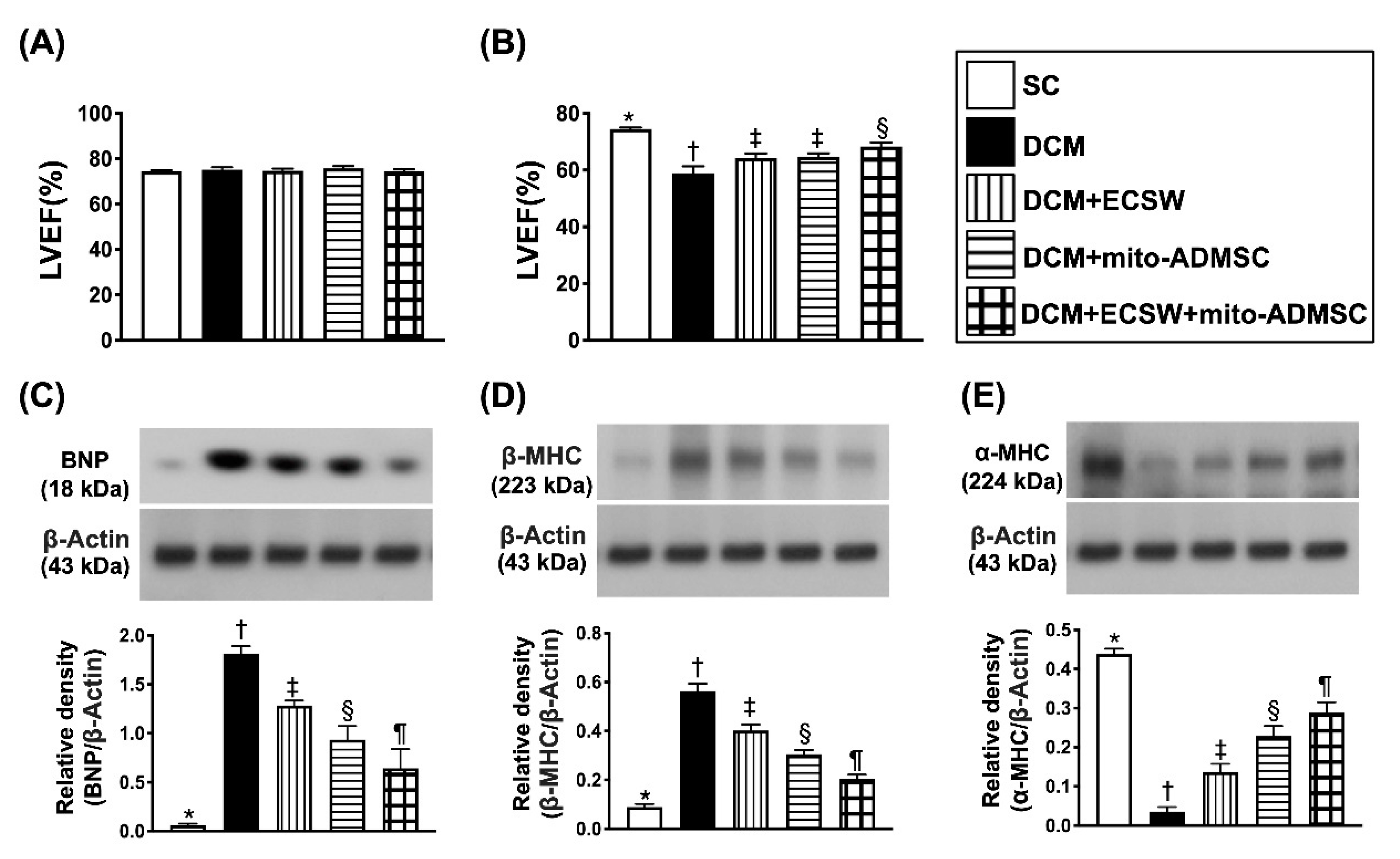
3.5. Combined ECSW-Assisted Mitochondrial Delivery into ADMSCs + ECSW Therapy Improved LVEF and Ameliorated the Heart Failure/Pressure Overload Biomarkers in LV Myocardium 7 Weeks after DCM Induction
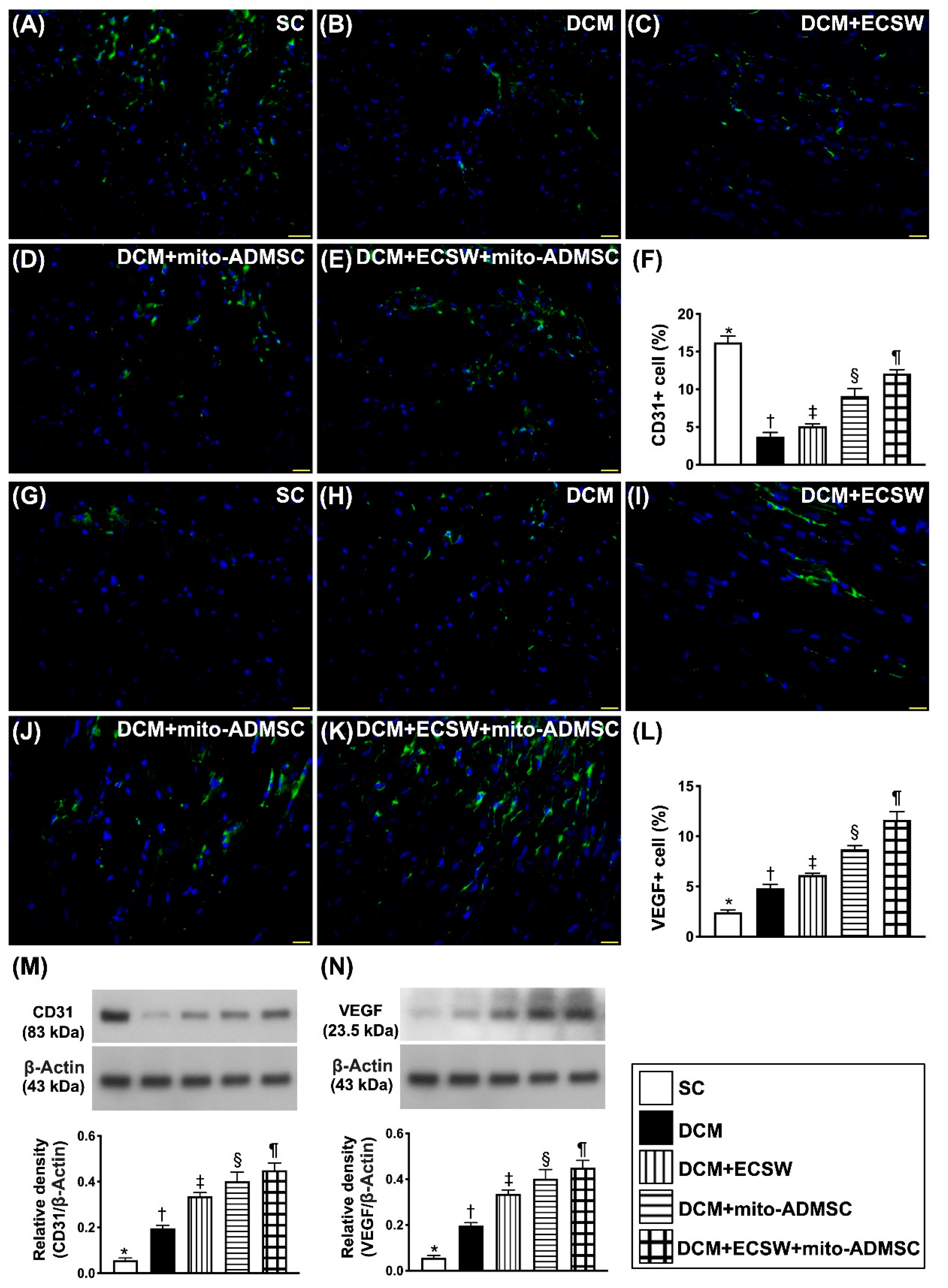
3.6. Combined ECSW-Assisted Mitochondrial Delivery into ADMSCs + ECSW Therapy Upregulated Angiogenesis in LV Myocardium of 7 Weeks after DCM Induction
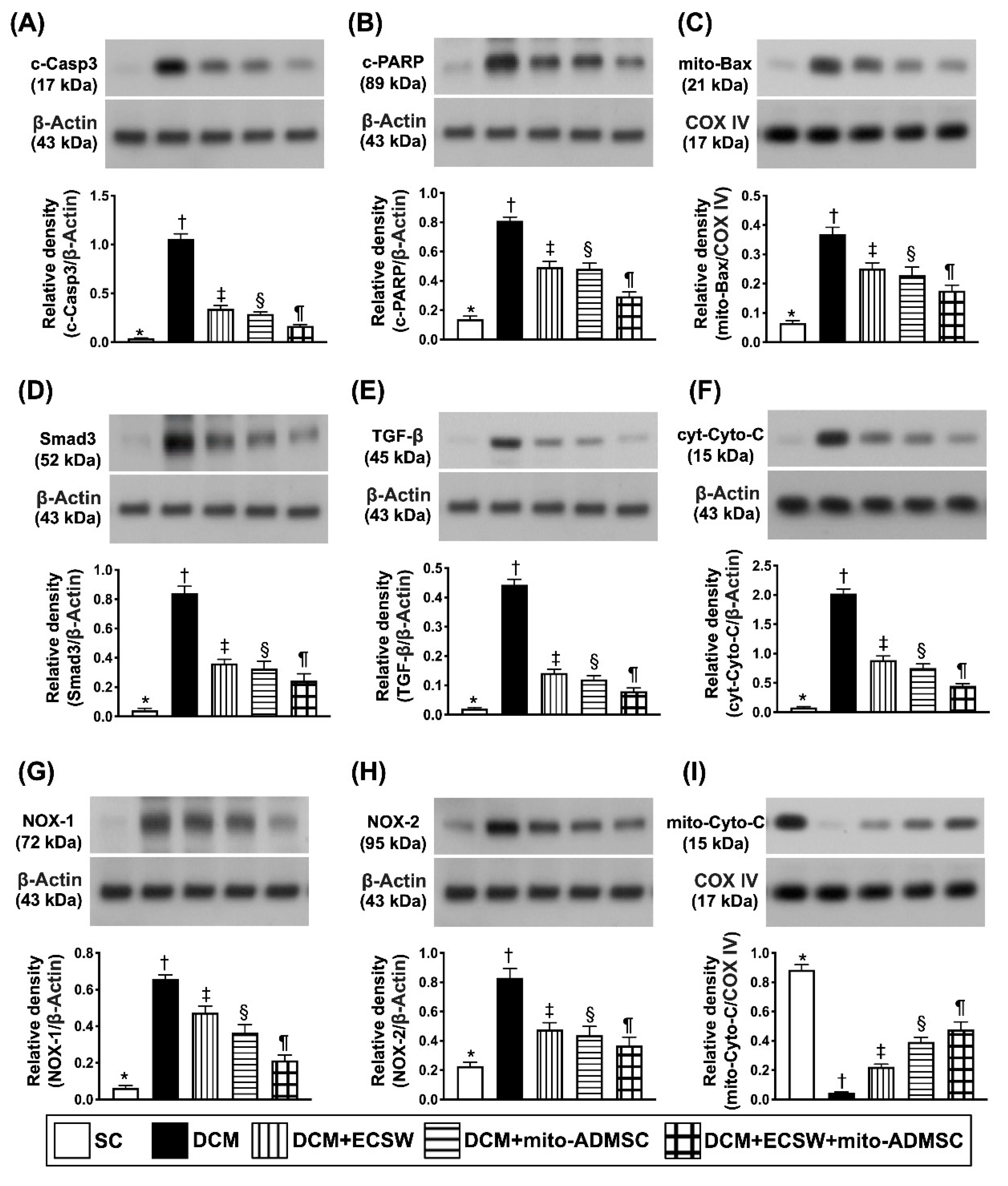
3.7. Combined ECSW-Assisted Mitochondrial Delivery into ADMSCs + ECSW Therapy Downregulated Apoptosis, Fibrosis and Oxidative Stress and Preserved Mitochondrial Integrity in LV Myocardium 7 Weeks after DCM Induction
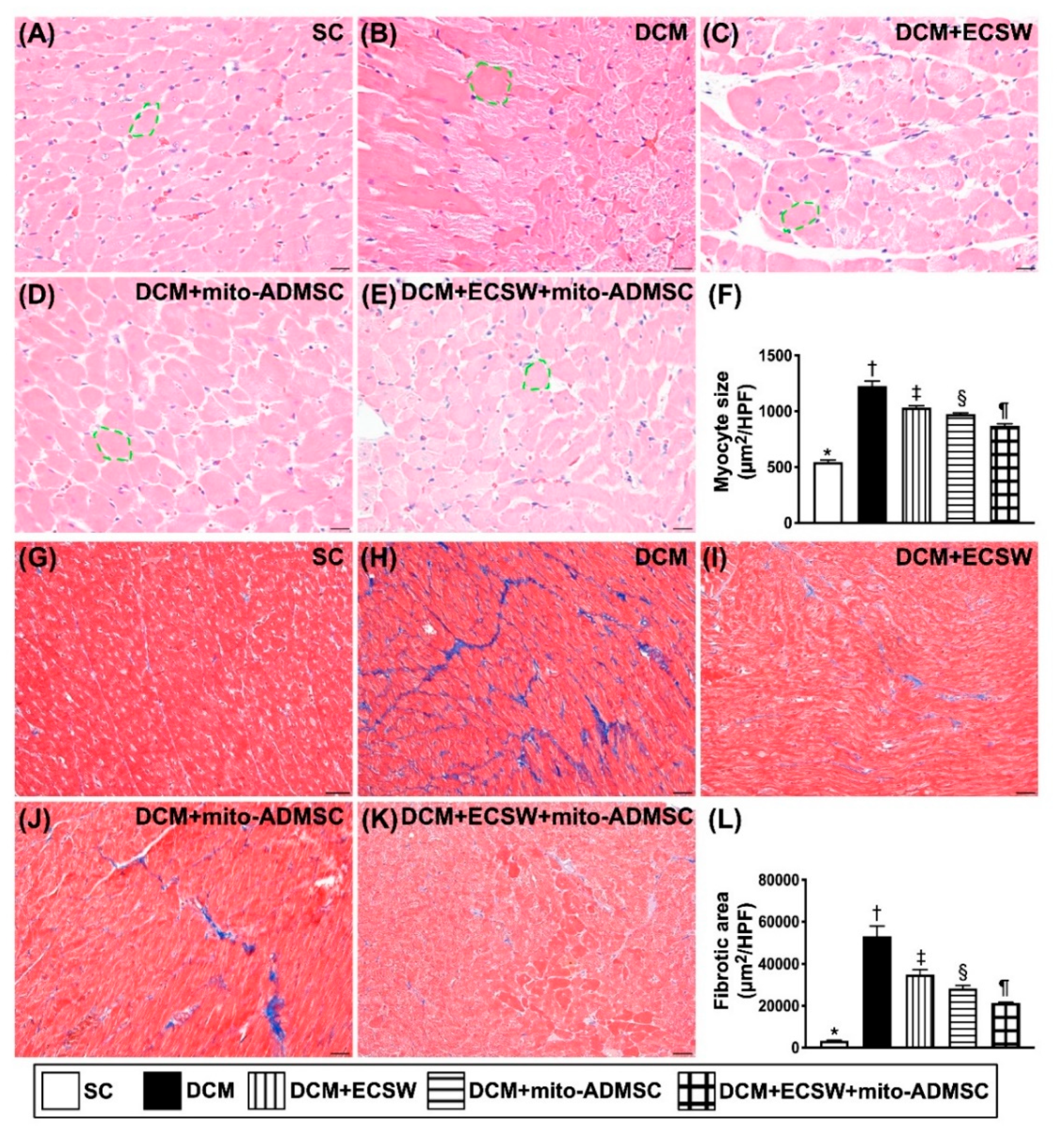
3.8. Cardiomyocyte Size and Cellular Expression of Fibrosis among the Five Groups by Day 49 after DCM Induction
4. Discussion
5. Conclusions
5.1. Study Limitation
5.2. In Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dec, G.W.; Fuster, V. Idiopathic dilated cardiomyopathy. N. Engl. J. Med. 1994, 331, 1564–1575. [Google Scholar] [CrossRef]
- Gigli, M.; Stolfo, D.; Merlo, M.; Barbati, G.; Ramani, F.; Brun, F.; Pinamonti, B.; Sinagra, G. Insights into mildly dilated cardiomyopathy: Temporal evolution and long-term prognosis. Eur. J. Heart Fail. 2017, 19, 531–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishida, J.; Konishi, M.; von Haehling, S. The appropriate dose of angiotensin-converting-enzyme inhibitors or angiotensin receptor blockers in patients with dilated cardiomyopathy. The higher, the better? ESC Heart Fail. 2015, 2, 103–105. [Google Scholar] [CrossRef]
- Manolio, T.A.; Baughman, K.L.; Rodeheffer, R.; Pearson, T.A.; Bristow, J.D.; Michels, V.V.; Abelmann, W.H.; Harlan, W.R. Prevalence and etiology of idiopathic dilated cardiomyopathy (summary of a National Heart, Lung, and Blood Institute workshop. Am. J. Cardiol. 1992, 69, 1458–1466. [Google Scholar] [CrossRef]
- Schultheiss, H.P.; Fairweather, D.; Caforio, A.L.P.; Escher, F.; Hershberger, R.E.; Lipshultz, S.E.; Liu, P.P.; Matsumori, A.; Mazzanti, A.; McMurray, J.; et al. Dilated cardiomyopathy. Nat. Rev. Dis. Primers 2019, 5, 32. [Google Scholar] [CrossRef] [PubMed]
- Towbin, J.A.; Lowe, A.M.; Colan, S.D.; Sleeper, L.A.; Orav, E.J.; Clunie, S.; Messere, J.; Cox, G.F.; Lurie, P.R.; Hsu, D.; et al. Incidence, causes, and outcomes of dilated cardiomyopathy in children. JAMA 2006, 296, 1867–1876. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, R.G.; Semsarian, C.; Macdonald, P. Dilated cardiomyopathy. Lancet 2017, 390, 400–414. [Google Scholar] [CrossRef]
- McKenna, W.J.; Maron, B.J.; Thiene, G. Classification, Epidemiology, and Global Burden of Cardiomyopathies. Circ. Res. 2017, 121, 722–730. [Google Scholar] [CrossRef] [Green Version]
- Chan, Y.K.; Tuttle, C.; Ball, J.; Teng, T.K.; Ahamed, Y.; Carrington, M.J.; Stewart, S. Current and projected burden of heart failure in the Australian adult population: A substantive but still ill-defined major health issue. BMC Health Serv. Res. 2016, 16, 501. [Google Scholar] [CrossRef]
- Rakar, S.; Sinagra, G.; Di Lenarda, A.; Poletti, A.; Bussani, R.; Silvestri, F.; Camerini, F. Epidemiology of dilated cardiomyopathy. A prospective post-mortem study of 5252 necropsies. The Heart Muscle Disease Study Group. Eur. Heart J. 1997, 18, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Dandel, M.; Weng, Y.; Siniawski, H.; Potapov, E.; Lehmkuhl, H.B.; Hetzer, R. Long-term results in patients with idiopathic dilated cardiomyopathy after weaning from left ventricular assist devices. Circulation 2005, 112, I37–I45. [Google Scholar] [CrossRef]
- Jennings, D.L. Heart Failure Therapy in 2016: SHIFTing the PARADIGM From Antiquated Therapies Toward Novel Agents. Ann. Pharmacother. 2017, 51, 79–82. [Google Scholar] [CrossRef]
- Pitt, B.; Poole-Wilson, P.A.; Segal, R.; Martinez, F.A.; Dickstein, K.; Camm, A.J.; Konstam, M.A.; Riegger, G.; Klinger, G.H.; Neaton, J.; et al. Effect of losartan compared with captopril on mortality in patients with symptomatic heart failure: Randomised trial—The Losartan Heart Failure Survival Study ELITE II. Lancet 2000, 355, 1582–1587. [Google Scholar] [CrossRef]
- Taylor, M.R.; Carniel, E.; Mestroni, L. Cardiomyopathy, familial dilated. Orphanet J. Rare Dis. 2006, 1, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, F.Y.; Shao, P.L.; Wallace, C.G.; Chua, S.; Sung, P.H.; Ko, S.F.; Chai, H.T.; Chung, S.Y.; Chen, K.H.; Lu, H.I.; et al. Combined Therapy with SS31 and Mitochondria Mitigates Myocardial Ischemia-Reperfusion Injury in Rats. Int. J. Mol. Sci. 2018, 19, 2782. [Google Scholar] [CrossRef] [Green Version]
- Oh, H.; Ito, H.; Sano, S. Challenges to success in heart failure: Cardiac cell therapies in patients with heart diseases. J. Cardiol. 2016, 68, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Kotamraju, S.; Konorev, E.A.; Joseph, J.; Kalyanaraman, B. Doxorubicin-induced apoptosis in endothelial cells and cardiomyocytes is ameliorated by nitrone spin traps and ebselen. Role of reactive oxygen and nitrogen species. J. Biol. Chem. 2000, 275, 33585–33592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurian, G.A.; Rajagopal, R.; Vedantham, S.; Rajesh, M. The Role of Oxidative Stress in Myocardial Ischemia and Reperfusion Injury and Remodeling: Revisited. Oxid. Med. Cell. Longev. 2016, 2016, 1656450. [Google Scholar] [CrossRef] [Green Version]
- Simeunovic, D.; Seferovic, P.M.; Ristic, A.D.; Nikolic, D.; Risimic, D.; Seferovic, J.; Maksimovic, R.; Nedeljkovic, I.; Karan, R.; Bajcetic, M. Evaluation of Oxidative Stress Markers and Catecholamine Changes in Patients with Dilated Cardiomyopathy Before and After Cardiopulmonary Exercise Testing. Hellenic. J. Cardiol. 2015, 56, 394–401. [Google Scholar]
- Wang, S.; Ding, L.; Ji, H.; Xu, Z.; Liu, Q.; Zheng, Y. The Role of p38 MAPK in the Development of Diabetic Cardiomyopathy. Int. J. Mol. Sci. 2016, 17, 1037. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.H.; Landry, A.B., 3rd; Lee, Y.S.; Katz, A.M. Doxorubicin-induced calcium release from cardiac sarcoplasmic reticulum vesicles. J. Mol. Cell. Cardiol. 1989, 21, 433–436. [Google Scholar] [CrossRef]
- Galloway, C.A.; Yoon, Y. Mitochondrial dynamics in diabetic cardiomyopathy. Antioxid. Redox Signal. 2015, 22, 1545–1562. [Google Scholar] [CrossRef] [Green Version]
- Kubli, D.A.; Gustafsson, A.B. Unbreak my heart: Targeting mitochondrial autophagy in diabetic cardiomyopathy. Antioxid. Redox Signal. 2015, 22, 1527–1544. [Google Scholar] [CrossRef] [PubMed]
- Westermeier, F.; Navarro-Marquez, M.; Lopez-Crisosto, C.; Bravo-Sagua, R.; Quiroga, C.; Bustamante, M.; Verdejo, H.E.; Zalaquett, R.; Ibacache, M.; Parra, V.; et al. Defective insulin signaling and mitochondrial dynamics in diabetic cardiomyopathy. Biochim. Biophys. Acta 2015, 1853, 1113–1118. [Google Scholar] [CrossRef] [Green Version]
- Won, S.; Davies-Venn, C.; Liu, S.; Bluemke, D.A. Noninvasive imaging of myocardial extracellular matrix for assessment of fibrosis. Curr. Opin. Cardiol. 2013, 28, 282–289. [Google Scholar] [CrossRef]
- Yang, R.; Ernst, P.; Song, J.; Liu, X.M.; Huke, S.; Wang, S.; Zhang, J.J.; Zhou, L. Mitochondrial-Mediated Oxidative Ca(2+)/Calmodulin-Dependent Kinase II Activation Induces Early Afterdepolarizations in Guinea Pig Cardiomyocytes: An In Silico Study. J. Am. Heart Assoc. 2018, 7, e008939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltis, A.R.; Saucerman, J.J. Synergy between CaMKII substrates and beta-adrenergic signaling in regulation of cardiac myocyte Ca(2+) handling. Biophys. J. 2010, 99, 2038–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutanto, H.; Lyon, A.; Lumens, J.; Schotten, U.; Dobrev, D.; Heijman, J. Cardiomyocyte calcium handling in health and disease: Insights from in vitro and in silico studies. Prog. Biophys. Mol. Biol. 2020, 157, 54–75. [Google Scholar] [CrossRef]
- Chai, H.T.; Sheu, J.J.; Chiang, J.Y.; Shao, P.L.; Wu, S.C.; Chen, Y.L.; Li, Y.C.; Sung, P.H.; Lee, F.Y.; Yip, H.K. Early administration of cold water and adipose derived mesenchymal stem cell derived exosome effectively protects the heart from ischemia-reperfusion injury. Am. J. Transl. Res. 2019, 11, 5375–5389. [Google Scholar]
- Sun, C.K.; Zhen, Y.Y.; Leu, S.; Tsai, T.H.; Chang, L.T.; Sheu, J.J.; Chen, Y.L.; Chua, S.; Chai, H.T.; Lu, H.I.; et al. Direct implantation versus platelet-rich fibrin-embedded adipose-derived mesenchymal stem cells in treating rat acute myocardial infarction. Int. J. Cardiol. 2014, 173, 410–423. [Google Scholar] [CrossRef]
- Fu, M.; Sun, C.K.; Lin, Y.C.; Wang, C.J.; Wu, C.J.; Ko, S.F.; Chua, S.; Sheu, J.J.; Chiang, C.H.; Shao, P.L.; et al. Extracorporeal shock wave therapy reverses ischemia-related left ventricular dysfunction and remodeling: Molecular-cellular and functional assessment. PLoS ONE 2011, 6, e24342. [Google Scholar] [CrossRef]
- Sung, P.H.; Yin, T.C.; Wallace, C.G.; Chen, K.H.; Shao, P.L.; Lee, F.Y.; Sun, C.K.; Sheu, J.J.; Chen, Y.L.; Omran, M.M.; et al. Extracorporeal Shock Wave-Supported Adipose-Derived Fresh Stromal Vascular Fraction Preserved Left Ventricular (LV) Function and Inhibited LV Remodeling in Acute Myocardial Infarction in Rat. Oxid. Med. Cell. Longev. 2018, 2018, 7518920. [Google Scholar] [CrossRef] [Green Version]
- Yin, T.C.; Sung, P.H.; Chen, K.H.; Li, Y.C.; Luo, C.W.; Huang, C.R.; Sheu, J.J.; Chiang, J.Y.; Lee, M.S.; Yip, H.K. Extracorporeal shock wave-assisted adipose-derived fresh stromal vascular fraction restores the blood flow of critical limb ischemia in rat. Vascul. Pharmacol. 2019, 113, 57–69. [Google Scholar] [CrossRef]
- Yip, H.K.; Shao, P.L.; Wallace, C.G.; Sheu, J.J.; Sung, P.H.; Lee, M.S. Early intramyocardial implantation of exogenous mitochondria effectively preserved left ventricular function in doxorubicin-induced dilated cardiomyopathy rat. Am. J. Transl. Res. 2020, 12, 4612–4627. [Google Scholar]
- Lin, K.C.; Wallace, C.G.; Yin, T.C.; Sung, P.H.; Chen, K.H.; Lu, H.I.; Chai, H.T.; Chen, C.H.; Chen, Y.L.; Li, Y.C.; et al. Shock Wave Therapy Enhances Mitochondrial Delivery into Target Cells and Protects against Acute Respiratory Distress Syndrome. Mediat. Inflamm. 2018, 2018, 5425346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, C.K.; Lee, F.Y.; Kao, Y.H.; Chiang, H.J.; Sung, P.H.; Tsai, T.H.; Lin, Y.C.; Leu, S.; Wu, Y.C.; Lu, H.I.; et al. Systemic combined melatonin-mitochondria treatment improves acute respiratory distress syndrome in the rat. J. Pineal Res. 2015, 58, 137–150. [Google Scholar] [CrossRef]
- Yeh, K.H.; Sheu, J.J.; Lin, Y.C.; Sun, C.K.; Chang, L.T.; Kao, Y.H.; Yen, C.H.; Shao, P.L.; Tsai, T.H.; Chen, Y.L.; et al. Benefit of combined extracorporeal shock wave and bone marrow-derived endothelial progenitor cells in protection against critical limb ischemia in rats. Crit. Care Med. 2012, 40, 169–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, H.T.; Chen, K.H.; Wallace, C.G.; Chen, C.H.; Sung, P.H.; Chen, Y.L.; Yuen, C.M.; Shao, P.L.; Sun, C.K.; Chang, H.W.; et al. Extracorporeal shock wave therapy effectively protects brain against chronic cerebral hypo-perfusion-induced neuropathological changes. Am. J. Transl. Res. 2017, 9, 5074–5093. [Google Scholar] [PubMed]
- Huang, T.H.; Sun, C.K.; Chen, Y.L.; Wang, C.J.; Yin, T.C.; Lee, M.S.; Yip, H.K. Shock Wave Enhances Angiogenesis through VEGFR2 Activation and Recycling. Mol. Med. 2017, 22, 850–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, F.Y.; Zhen, Y.Y.; Yuen, C.M.; Fan, R.; Chen, Y.T.; Sheu, J.J.; Chen, Y.L.; Wang, C.J.; Sun, C.K.; Yip, H.K. The mTOR-FAK mechanotransduction signaling axis for focal adhesion maturation and cell proliferation. Am. J. Transl. Res. 2017, 9, 1603–1617. [Google Scholar]











Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, P.-H.; Lee, M.S.; Chai, H.-T.; Chiang, J.Y.; Li, Y.-C.; Chu, Y.-C.; Huang, C.-R.; Yip, H.-K. Extracorporeal Shock Wave Enhanced Exogenous Mitochondria into Adipose-Derived Mesenchymal Stem Cells and Further Preserved Heart Function in Rat Dilated Cardiomyopathy. Biomedicines 2021, 9, 1362. https://doi.org/10.3390/biomedicines9101362
Sung P-H, Lee MS, Chai H-T, Chiang JY, Li Y-C, Chu Y-C, Huang C-R, Yip H-K. Extracorporeal Shock Wave Enhanced Exogenous Mitochondria into Adipose-Derived Mesenchymal Stem Cells and Further Preserved Heart Function in Rat Dilated Cardiomyopathy. Biomedicines. 2021; 9(10):1362. https://doi.org/10.3390/biomedicines9101362
Chicago/Turabian StyleSung, Pei-Hsun, Mel S. Lee, Han-Tan Chai, John Y. Chiang, Yi-Chen Li, Yi-Ching Chu, Chi-Ruei Huang, and Hon-Kan Yip. 2021. "Extracorporeal Shock Wave Enhanced Exogenous Mitochondria into Adipose-Derived Mesenchymal Stem Cells and Further Preserved Heart Function in Rat Dilated Cardiomyopathy" Biomedicines 9, no. 10: 1362. https://doi.org/10.3390/biomedicines9101362
APA StyleSung, P. -H., Lee, M. S., Chai, H. -T., Chiang, J. Y., Li, Y. -C., Chu, Y. -C., Huang, C. -R., & Yip, H. -K. (2021). Extracorporeal Shock Wave Enhanced Exogenous Mitochondria into Adipose-Derived Mesenchymal Stem Cells and Further Preserved Heart Function in Rat Dilated Cardiomyopathy. Biomedicines, 9(10), 1362. https://doi.org/10.3390/biomedicines9101362