
The Slower Antibody Response in Myelofibrosis Patients after Two Doses of mRNA SARS-CoV-2 Vaccine Calls for a Third Dose

 ,
,  , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Material and Methods
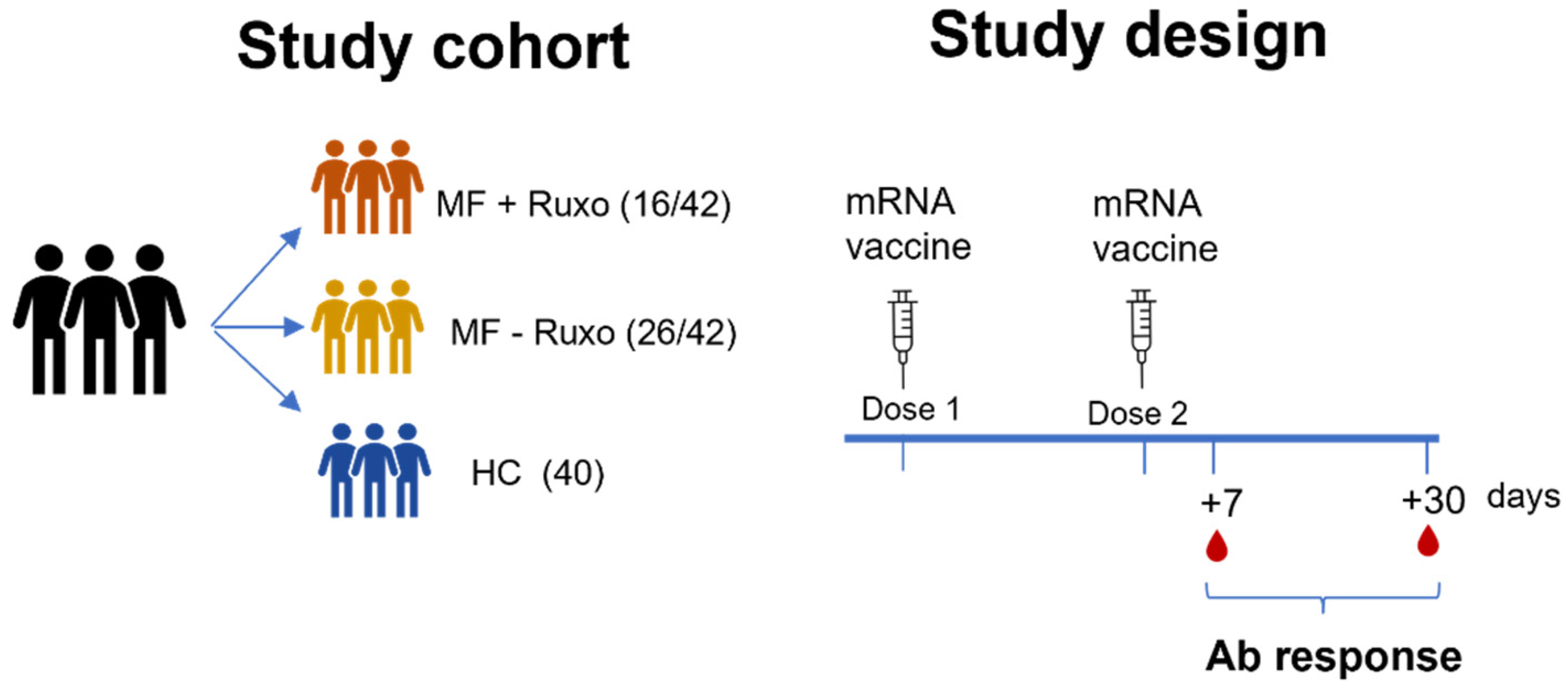
2.1. Study Design
2.2. ELISA
2.3. ACE2/RBD Binding Inhibition Assay
2.4. Statistical Analysis
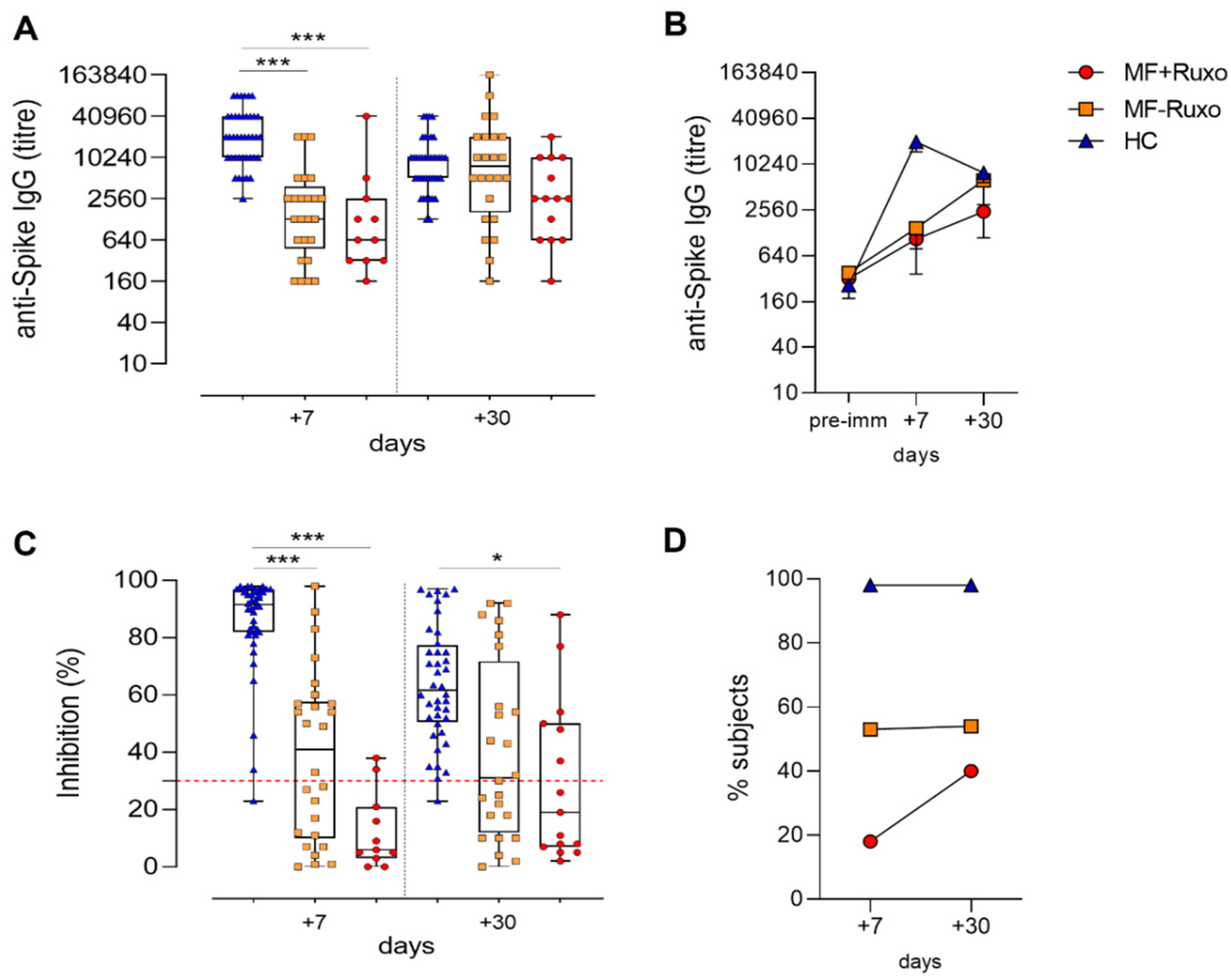
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Passamonti, F.; Cattaneo, C.; Arcaini, L.; Bruna, R.; Cavo, M.; Merli, F.; Angelucci, E.; Krampera, M.; Cairoli, R.; Porta, M.G.D.; et al. Clinical Characteristics and Risk Factors Associated with COVID-19 Severity in Patients with Haematological Malignancies in Italy: A Retrospective, Multicentre, Cohort Study. Lancet Haematol. 2020, 7, e737–e745. [Google Scholar] [CrossRef]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martín-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of Patients with Hematologic Malignancies and COVID-19: A Systematic Review and Meta-Analysis of 3377 Patients. Blood 2020, 136, 2881–2892. [Google Scholar] [CrossRef] [PubMed]
- Passamonti, F.; Romano, A.; Salvini, M.; Merli, F.; Porta, M.G.D.; Bruna, R.; Coviello, E.; Romano, I.; Cairoli, R.; Lemoli, R.; et al. COVID-19 Elicits an Impaired Antibody Response against SARS-CoV-2 in Patients with Haematological Malignancies. Br. J. Haematol. 2021. [Google Scholar] [CrossRef] [PubMed]
- McLornan, D.P.; Khan, A.A.; Harrison, C.N. Immunological Consequences of JAK Inhibition: Friend or Foe? Curr. Hematol. Malig. Rep. 2015, 10, 370–379. [Google Scholar] [CrossRef]
- Capochiani, E.; Frediani, B.; Iervasi, G.; Paolicchi, A.; Sani, S.; Roncucci, P.; Cuccaro, A.; Franchi, F.; Simonetti, F.; Carrara, D.; et al. Ruxolitinib Rapidly Reduces Acute Respiratory Distress Syndrome in COVID-19 Disease. Analysis of Data Collection From RESPIRE Protocol. Front. Med. 2020, 7, 466. [Google Scholar] [CrossRef]
- La Rosée, F.; Bremer, H.C.; Gehrke, I.; Kehr, A.; Hochhaus, A.; Birndt, S.; Fellhauer, M.; Henkes, M.; Kumle, B.; Russo, S.G.; et al. The Janus Kinase 1/2 Inhibitor Ruxolitinib in COVID-19 with Severe Systemic Hyperinflammation. Leukemia 2020, 34, 1805–1815. [Google Scholar] [CrossRef] [PubMed]
- Barbui, T.; Vannucchi, A.M.; Alvarez-Larran, A.; Iurlo, A.; Masciulli, A.; Carobbio, A.; Ghirardi, A.; Ferrari, A.; Rossi, G.; Elli, E.; et al. High Mortality Rate in COVID-19 Patients with Myeloproliferative Neoplasms after Abrupt Withdrawal of Ruxolitinib. Leukemia 2021, 35, 485–493. [Google Scholar] [CrossRef]
- Guglielmelli, P.; Mazzoni, A.; Maggi, L.; Kiros, S.T.; Zammarchi, L.; Pilerci, S.; Rocca, A.; Spinicci, M.; Borella, M.; Bartoloni, A.; et al. Impaired Response to First SARS-CoV-2 Dose Vaccination in Myeloproliferative Neoplasm Patients Receiving Ruxolitinib. Am. J. Hematol. 2021, E408–E410. [Google Scholar] [CrossRef]
- Caocci, G.; Mulas, O.; Mantovani, D.; Costa, A.; Galizia, A.; Barabino, L.; Greco, M.; Murru, R.; La Nasa, G. Ruxolitinib Does Not Impair Humoral Immune Response to COVID-19 Vaccination with BNT162b2 MRNA COVID-19 Vaccine in Patients with Myelofibrosis. Ann. Hematol. 2021, 1–3. [Google Scholar] [CrossRef]
- Pimpinelli, F.; Marchesi, F.; Piaggio, G.; Giannarelli, D.; Papa, E.; Falcucci, P.; Spadea, A.; Pontone, M.; Di Martino, S.; Laquintana, V.; et al. Lower Response to BNT162b2 Vaccine in Patients with Myelofibrosis Compared to Polycythemia Vera and Essential Thrombocythemia. J. Hematol. Oncol. 2021, 14, 119. [Google Scholar] [CrossRef] [PubMed]
- Harrington, P.; de Lavallade, H.; Doores, K.J.; O’Reilly, A.; Seow, J.; Graham, C.; Lechmere, T.; Radia, D.; Dillon, R.; Shanmugharaj, Y.; et al. Single Dose of BNT162b2 MRNA Vaccine against SARS-CoV-2 Induces High Frequency of Neutralising Antibody and Polyfunctional T-Cell Responses in Patients with Myeloproliferative Neoplasms. Leukemia 2021, 1–5. [Google Scholar] [CrossRef]
- Callaway, E. COVID Vaccine Boosters: The Most Important Questions. Nature 2021, 596, 178–180. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.-C.; Tiu, C.; Hu, Z.; Chen, V.C.-W.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 Surrogate Virus Neutralization Test Based on Antibody-Mediated Blockage of ACE2–Spike Protein–Protein Interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Ciabattini, A.; Pastore, G.; Fiorino, F.; Polvere, J.; Lucchesi, S.; Pettini, E.; Auddino, S.; Rancan, I.; Durante, M.; Miscia, M.; et al. Evidence of SARS-CoV-2-Specific Memory B Cells Six Months After Vaccination With the BNT162b2 MRNA Vaccine. Front. Immunol. 2021, 12, 3751. [Google Scholar] [CrossRef]
- Piano Mortari, E.; Russo, C.; Vinci, M.R.; Terreri, S.; Fernandez Salinas, A.; Piccioni, L.; Alteri, C.; Colagrossi, L.; Coltella, L.; Ranno, S.; et al. Highly Specific Memory B Cells Generation after the 2nd Dose of BNT162b2 Vaccine Compensate for the Decline of Serum Antibodies and Absence of Mucosal IgA. Cells 2021, 10, 2541. [Google Scholar] [CrossRef]
- Wheeler, S.E.; Shurin, G.V.; Yost, M.; Anderson, A.; Pinto, L.; Wells, A.; Shurin, M.R. Differential Antibody Response to MRNA COVID-19 Vaccines in Healthy Subjects. Microbiol. Spectr. 2021, 9, e0034121. [Google Scholar] [CrossRef] [PubMed]
- Dittadi, R.; Seguso, M.; Bertoli, I.; Afshar, H.; Carraro, P. Antibodies against SARS-CoV-2 Time Course in Patients and Vaccinated Subjects: An Evaluation of the Harmonization of Two Different Methods. Diagnostics 2021, 11, 1709. [Google Scholar] [CrossRef]
- Abe, K.T.; Li, Z.; Samson, R.; Samavarchi-Tehrani, P.; Valcourt, E.J.; Wood, H.; Budylowski, P.; Dupuis, A.P.; Girardin, R.C.; Rathod, B.; et al. A Simple Protein-Based Surrogate Neutralization Assay for SARS-CoV-2. JCI Insight 2020, 5, e142362. [Google Scholar] [CrossRef]
- Long, Q.-X.; Liu, B.-Z.; Deng, H.-J.; Wu, G.-C.; Deng, K.; Chen, Y.-K.; Liao, P.; Qiu, J.-F.; Lin, Y.; Cai, X.-F.; et al. Antibody Responses to SARS-CoV-2 in Patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Landtblom, A.R.; Andersson, T.M.-L.; Dickman, P.W.; Smedby, K.E.; Eloranta, S.; Batyrbekova, N.; Samuelsson, J.; Björkholm, M.; Hultcrantz, M. Risk of Infections in Patients with Myeloproliferative Neoplasms—A Population-Based Cohort Study of 8363 Patients. Leukemia 2021, 35, 476–484. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients’ Characteristics | Whole Cohort (n = 42) | Ruxolitinib (n = 16) | No Ruxolitinib (n = 26) |
|---|---|---|---|
| Median age at diagnosis (range) | 67 years (31–85) | 63.5 years (44–85) | 68.5 years (31–81) |
| Sex | |||
| Male | 21 (50%) | 9 (56%) | 12 (46%) |
| Female | 21 (50%) | 7 (44%) | 14 (54%) |
| Disease | |||
| Primary MF | 21/42 (50%) | 4/21 (19%) | 17/21 (81%) |
| Post-PV | 13/42 (31%) | 9/13 (69%) | 4/13 (31%) |
| Post-ET | 8/42 (19%) | 3/8 (37.5%) | 5/8 (62.5%) |
| IPSS SCORE | |||
| LOW | 11/42 (26.2%) | 4/11 (36%) | 7/11 (64%) |
| INT—1 | 15/42 (35.8%) | 6/15 (40%) | 9/15 (60%) |
| INT—2 | 8/42 (19%) | 4/8 (50%) | 4/8 (50%) |
| HIGH | 8/42 (19%) | 4/8 (50%) | 4/8 (50%) |
| Driver mutation | |||
| JAK2 | 29/42 (69.1%) | 15/29 (51.7%) | 14/29 (48.3%) |
| CALR | 9/42 (21.4%) | 1/9 (1.1%) | 8/9 (98.9%) |
| MPL | 1/42 (2.4%) | 0/1 (0%) | 1/1 (100%) |
| Triple negative | 3/42 (7.1%) | 0/3 (0%) | 3/3 (100%) |
| Time of exposition to ruxolitinib (range) | 26 months (4–48 ) | ||
| Spleen below costal margin, median (range) | 3 cm(0–20) | 3 cm (0–20) | 3.5 cm (0–20) |
| Hemoglobin g/dL, median (range) | 11.8 (6.2–15.5) | 11.6 (8.5–15.5) | 12.4 (6.2–15.3) |
| Platelets × 103/µL, median (range) | 306 (19–789) | 204 (19–724) | 362 (36–789) |
| WBC × 103/µL, median (range) | 7.39 (2.7–37.15) | 9.47 (3.5–37.15) | 6.7 (2.7–25.27) |
| Lymphocytes × 103/µL, median (range) | 1.55 (0.12–7.4) | 1.49 (0.51–7.4) | 1.6 (0.12–3.03) |
| Total protein g/dL, median (range) | 6.9 (5.8–8.5) | 7.05 (5.9–8.5) | 6.85 (5.8–7.8) |
| γ-Globulins (%), median (range) | 13 (5.8–23.9) | 13.2 (9–23.9) | 12.9 (5.8–22) |
| LDH U/L, median (range) | 415 (172–1430) | 377 (209–1019) | 498 (172–1430) |
| Subjects | Seroconversion | Binding Inhibition Activity of Seroconverted Subjects |
|---|---|---|
| Total MF | 32/42 (76%) | 22/42 (52%) |
| MF + Ruxo | 11/16 (68%) | 6/16 (37%) |
| MF − Ruxo | 21/26 (81%) | 16/26 (61%) |
| HC | 40/40 (100%) | 39/40 (98%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorino, F.; Sicuranza, A.; Ciabattini, A.; Santoni, A.; Pastore, G.; Simoncelli, M.; Polvere, J.; Galimberti, S.; Auddino, S.; Baratè, C.; et al. The Slower Antibody Response in Myelofibrosis Patients after Two Doses of mRNA SARS-CoV-2 Vaccine Calls for a Third Dose. Biomedicines 2021, 9, 1480. https://doi.org/10.3390/biomedicines9101480
Fiorino F, Sicuranza A, Ciabattini A, Santoni A, Pastore G, Simoncelli M, Polvere J, Galimberti S, Auddino S, Baratè C, et al. The Slower Antibody Response in Myelofibrosis Patients after Two Doses of mRNA SARS-CoV-2 Vaccine Calls for a Third Dose. Biomedicines. 2021; 9(10):1480. https://doi.org/10.3390/biomedicines9101480
Chicago/Turabian StyleFiorino, Fabio, Anna Sicuranza, Annalisa Ciabattini, Adele Santoni, Gabiria Pastore, Martina Simoncelli, Jacopo Polvere, Sara Galimberti, Stefano Auddino, Claudia Baratè, and et al. 2021. "The Slower Antibody Response in Myelofibrosis Patients after Two Doses of mRNA SARS-CoV-2 Vaccine Calls for a Third Dose" Biomedicines 9, no. 10: 1480. https://doi.org/10.3390/biomedicines9101480
APA StyleFiorino, F., Sicuranza, A., Ciabattini, A., Santoni, A., Pastore, G., Simoncelli, M., Polvere, J., Galimberti, S., Auddino, S., Baratè, C., Montagnani, F., Sammartano, V., Bocchia, M., & Medaglini, D. (2021). The Slower Antibody Response in Myelofibrosis Patients after Two Doses of mRNA SARS-CoV-2 Vaccine Calls for a Third Dose. Biomedicines, 9(10), 1480. https://doi.org/10.3390/biomedicines9101480