
The Association between Use of ICS and Psychiatric Symptoms in Patients with COPD—A Nationwide Cohort Study of 49,500 Patients

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
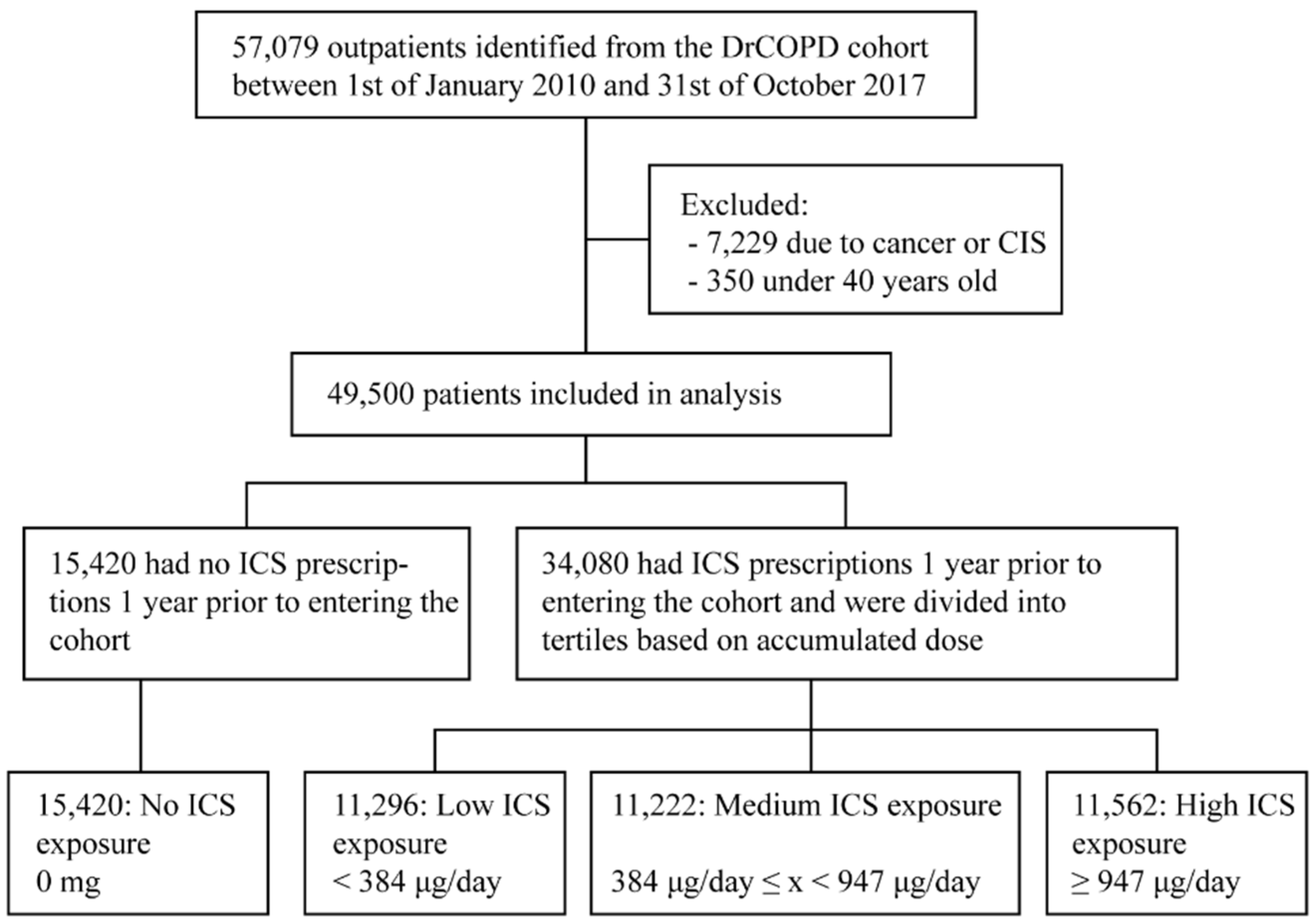
- (1)
- The Danish Register for Chronic Obstructive Pulmonary Disease (DrCOPD). A nationwide register of patients with specialist spirometry-verified COPD. The registry contains information about hospital admissions with acute COPD exacerbation and outpatient contacts. Hospitals began reporting data in 2008, and the register is monitored for consistency and completeness annually. The register contains clinical values such as forced expiratory volume in one second (FEV1), body mass index (BMI), Medical Research Council dyspnea scale (MRC) and smoking status [24].
- (2)
- The Danish National Patient Registry (DNPR). A nationwide register of all outpatient or inpatient contacts with the Danish Health Service. Each contact has a physician-coded primary diagnosis and one or more secondary diagnoses using the ICD (International Classification of Diseases), 10th revision (ICD-10). The register has received data from both the somatic and psychiatric sector since 1994 [25].
- (3)
- Danish National Database of Reimbursed Prescriptions (DNDRP). A nationwide register containing information about all collected prescriptions in community-pharmacies and hospital-based outpatient pharmacies since 2004. The register includes information on the strength, dose, product name and Anatomical Therapeutic Chemical (ATC) classification of each prescription [26].
3. Results
Sensitivity Analyses
4. Discussion
Strengths and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICS Class. | ATC Codes | Budesonide-Equivalent Conversion Factor |
|---|---|---|
| Budesonide | R03AK07, R03BA02 | 1 |
| Beclomethasone | R03BA01, R03AK08 | 1 (2 for ultrafine formulations) |
| Fluticasone | R03BA05, R03AK06, R03AK10, R03AK11 | 2 (10 for Fluticasonefuroate) |
| Ciclesonide | R03BA08 | 2.5 |
| Mometasone | R03BA07 | 1 |
| Antidepressant Class | ATC Codes |
|---|---|
| Tricarboxylic Acids (TCA) | N06AA |
| Serotonin Selective Reuptake Inhibitors (SSRI) | N06AB |
| Serotonin-Noradrenalin Reuptake Inhibitors (SNRI) | N06AX16, N06AX17, N06AX21, N06AX23 |
| Noradrenergic and Specific Serotonergic Antidepressants (NaSSA) | N06AX03, N06AX11 |
| Other | N06AX except those used to define SNRI and NaSSA drugs |
| No ICS Exposure N = 15,420 | Low ICS Exposure N = 11,296 <84 μg/day | Medium ICS Exposure N = 11,222 384 μg/day ≤ x <947 μg/day | High ICS Exposure N = 11,562 ≥947 μg/day | |
|---|---|---|---|---|
| Any antidepressant | 292.1 | 330.8 | 358.1 | 410.5 |
| Tricyclic antidepressants (TCA) | 13.0 | 13.0 | 11.1 | 12.8 |
| Selective serotonin reuptake inhibitors (SSRI) | 187.9 | 224.8 | 239.3 | 272.6 |
| Serotonin and noradrenaline reuptake inhibitors (SNRI) | 44.5 | 45.0 | 42.1 | 45.8 |
| Noradrenergic and specific serotonergic antidepressants (NaSSA) | 55.6 | 43.8 | 59.2 | 75.5 |
| Other | 2.4 | 3.8 | 3.2 | 3.8 |
| No ICS Exposure N = 15,420 | Low ICS Exposure N = 11,296 <384 μg/day | Medium ICS Exposure N = 11,222 384 μg/day ≤ x < 947 μg/day | High ICS Exposure N = 11,562 ≥947 μg/day | |
|---|---|---|---|---|
| Total | 1.5 | 2.3 | 3.0 | 1.9 |
| Depression | 0.7 | 1.2 | 1.8 | 1.3 |
| Bipolar disorder | 0.6 | 0.6 | 0.8 | 0.3 |
| Anxiety | 0.2 | 0.6 | 0.6 | 0.6 |
References
- Ernst, P.; Baltzan, M.; Deschenes, J.; Suissa, S. Low-dose inhaled and nasal corticosteroid use and the risk of cataracts. Eur. Respir. J. 2006, 27, 1168–1174. [Google Scholar] [CrossRef] [Green Version]
- Smeeth, L.; Boulis, M.; Hubbard, R.; Fletcher, A.E. A population based case-control study of cataract and inhaled corticosteroids. Br. J. Ophthalmol. 2003, 87, 1247–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kew, K.M.; Seniukovich, A. Inhaled steroids and risk of pneumonia for chronic obstructive pulmonary disease. Cochrane. Database Syst. Rev. 2014, CD010115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wedzicha, J.A.; Calverley, P.M.; Seemungal, T.A.; Hagan, G.; Ansari, Z.; Stockley, R.A.; Investigators, I. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am. J. Respir. Crit. Care Med. 2008, 177, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Calverley, P.M.; Anderson, J.A.; Celli, B.; Ferguson, G.T.; Jenkins, C.; Jones, P.W.; Yates, J.C.; Vestbo, J.; M.D. for the TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N. Engl. J. Med. 2007, 356, 775–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivapalan, P.; Ingebrigtsen, T.S.; Rasmussen, D.B.; Sorensen, R.; Rasmussen, C.M.; Jensen, C.B.; Allin, K.H.; Eklof, J.; Seersholm, N.; Vestbo, J.; et al. COPD exacerbations: The impact of long versus short courses of oral corticosteroids on mortality and pneumonia: Nationwide data on 67,000 patients with COPD followed for 12 months. BMJ Open Respir. Res. 2019, 6, e000407. [Google Scholar] [CrossRef]
- Matera, M.G.; Cardaci, V.; Cazzola, M.; Rogliani, P. Safety of inhaled corticosteroids for treating chronic obstructive pulmonary disease. Expert Opin. Drug Saf. 2015, 14, 533–541. [Google Scholar] [CrossRef]
- Park, H.Y.; Man, S.F.; Sin, D.D. Inhaled corticosteroids for chronic obstructive pulmonary disease. BMJ 2012, 345, e6843. [Google Scholar] [CrossRef]
- Brown, E.S.; Khan, D.A.; Nejtek, V.A. The psychiatric side effects of corticosteroids. Ann. Allergy Asthma Immunol. 1999, 83, 495–504. [Google Scholar] [CrossRef]
- Warrington, T.P.; Bostwick, J.M. Psychiatric adverse effects of corticosteroids. Mayo Clin. Proc. 2006, 81, 1361–1367. [Google Scholar] [CrossRef] [Green Version]
- Lewis, D.A.; Smith, R.E. Steroid-induced psychiatric syndromes. A report of 14 cases and a review of the literature. J. Affect. Disord. 1983, 5, 319–332. [Google Scholar] [CrossRef]
- Naber, D.; Sand, P.; Heigl, B. Psychopathological and neuropsychological effects of 8-days’ corticosteroid treatment. A prospective study. Psychoneuroendocrinology 1996, 21, 25–31. [Google Scholar] [CrossRef]
- Hudson, J.I.; Hudson, M.S.; Griffing, G.T.; Melby, J.C.; Pope, H.G., Jr. Phenomenology and family history of affective disorder in Cushing’s disease. Am. J. Psychiatry 1987, 144, 951–953. [Google Scholar] [CrossRef]
- Madalena, K.M.; Lerch, J.K. The Effect of Glucocorticoid and Glucocorticoid Receptor Interactions on Brain, Spinal Cord, and Glial Cell Plasticity. Neural Plast 2017, 2017, 8640970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matte, D.L.; Pizzichini, M.M.; Hoepers, A.T.; Diaz, A.P.; Karloh, M.; Dias, M.; Pizzichini, E. Prevalence of depression in COPD: A systematic review and meta-analysis of controlled studies. Respir. Med. 2016, 117, 154–161. [Google Scholar] [CrossRef]
- Papaioannou, A.I.; Bartziokas, K.; Tsikrika, S.; Karakontaki, F.; Kastanakis, E.; Banya, W.; Haniotou, A.; Papiris, S.; Loukides, S.; Polychronopoulos, V.; et al. The impact of depressive symptoms on recovery and outcome of hospitalised COPD exacerbations. Eur. Respir. J. 2013, 41, 815–823. [Google Scholar] [CrossRef] [Green Version]
- Iyer, A.S.; Bhatt, S.P.; Garner, J.J.; Wells, J.M.; Trevor, J.L.; Patel, N.M.; Kirkpatrick, D.; Williams, J.C.; Dransfield, M.T. Depression Is Associated with Readmission for Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Ann. Am. Thorac. Soc. 2016, 13, 197–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Leupoldt, A.; Taube, K.; Lehmann, K.; Fritzsche, A.; Magnussen, H. The impact of anxiety and depression on outcomes of pulmonary rehabilitation in patients with COPD. Chest 2011, 140, 730–736. [Google Scholar] [CrossRef] [PubMed]
- de Voogd, J.N.; Wempe, J.B.; Koeter, G.H.; Postema, K.; van Sonderen, E.; Ranchor, A.V.; Coyne, J.C.; Sanderman, R. Depressive symptoms as predictors of mortality in patients with COPD. Chest 2009, 135, 619–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyun, M.K.; Lee, N.R.; Jang, E.J.; Yim, J.J.; Lee, C.H. Effect of inhaled drugs on anxiety and depression in patients with chronic obstructive pulmonary disease: A prospective observational study. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 747–754. [Google Scholar] [CrossRef] [Green Version]
- Bonala, S.B.; Pina, D.; Silverman, B.A.; Amara, S.; Bassett, C.W.; Schneider, A.T. Asthma severity, psychiatric morbidity, and quality of life: Correlation with inhaled corticosteroid dose. J. Asthma 2003, 40, 691–699. [Google Scholar] [CrossRef] [PubMed]
- de Vries, T.W.; de Langen-Wouterse, J.J.; van Puijenbroek, E.; Duiverman, E.J.; de Jong-Van den Berg, L.T. Reported adverse drug reactions during the use of inhaled steroids in children with asthma in the Netherlands. Eur. J. Clin. Pharmacol. 2006, 62, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Childhood Asthma Management Program Research Group; Szefler, S.; Weiss, S.; Tonascia, J.; Adkinson, N.F.; Bender, B.; Cherniack, R.; Donithan, M.; Kelly, H.W.; Reisman, J.; et al. Long-term effects of budesonide or nedocromil in children with asthma. N. Engl. J. Med. 2000, 343, 1054–1063. [Google Scholar] [CrossRef] [PubMed]
- Lange, P.; Tottenborg, S.S.; Sorknaes, A.D.; Andersen, J.S.; Sogaard, M.; Nielsen, H.; Thomsen, R.W.; Nielsen, K.A. Danish Register of chronic obstructive pulmonary disease. Clin. Epidemiol. 2016, 8, 673–678. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.; Schmidt, S.A.; Sandegaard, J.L.; Ehrenstein, V.; Pedersen, L.; Sorensen, H.T. The Danish National Patient Registry: A review of content, data quality, and research potential. Clin. Epidemiol. 2015, 7, 449–490. [Google Scholar] [CrossRef] [Green Version]
- Johannesdottir, S.A.; Horvath-Puho, E.; Ehrenstein, V.; Schmidt, M.; Pedersen, L.; Sorensen, H.T. Existing data sources for clinical epidemiology: The Danish National Database of Reimbursed Prescriptions. Clin. Epidemiol. 2012, 4, 303–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCaffrey, D.F.; Griffin, B.A.; Almirall, D.; Slaughter, M.E.; Ramchand, R.; Burgette, L.F. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat. Med. 2013, 32, 3388–3414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, A.; Billionnet, C. Covariate adjustment of cumulative incidence functions for competing risks data using inverse probability of treatment weighting. Comput. Methods Programs Biomed. 2016, 129, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.; Schultheis, B.C.; Hanes, M.C.; Jolly, S.M.; Chakravarthy, K.V.; Deer, T.R.; Levy, R.M.; Hunter, C.W. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. 2019, 20, S2–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, J.; Motulsky, A.; Abrahamowicz, M.; Eguale, T.; Buckeridge, D.L.; Tamblyn, R. Off-label indications for antidepressants in primary care: Descriptive study of prescriptions from an indication based electronic prescribing system. BMJ 2017, 356, j603. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| No ICS Exposure N = 15,420 | Low ICS Exposure N = 11,296 <384 μg/day | Medium ICS Exposure N = 11,222 384 μg/day ≤ x <947 μg/day | High ICS Exposure N = 11,562 ≥947 μg/day | |
|---|---|---|---|---|
| Age, median (IQR) | 69 (60.75–76) | 70 (61–77) | 71 (64–78) | 71 (64–78) |
| Male, n (%) | 8102 (52.5) | 5525 (48.9) | 5102 (45.5) | 4728 (40.9) |
| Smoking | ||||
| Current smoker, n (%) | 5793 (37.6) | 3887 (34.4) | 3369 (30.0) | 3435 (29.7) |
| Former smoker, n (%) | 7257 (47.1) | 6254 (55.4) | 6994 (62.3) | 7347 (63.5) |
| Never smoker, n (%) | 306 (2.0) | 188 (1.7) | 146 (1.3) | 104 (0.9) |
| Smoking status unknown, n (%) | 2064 (13.4) | 967 (8.6) | 713 (6.4) | 676 (5.8) |
| Diagnosed with alcohol use disorder, n (%) | 920 (6.0) | 619 (5.5) | 512 (4.6) | 513 (4.4) |
| Diagnosed with substance abuse disorder other than alcohol, n (%) | 869 (5.6) | 601 (5.3) | 487 (4.3) | 501 (4.3) |
| BMI, median (IQR), kg·m−2 | 25 (22–29) | 25 (22–29.3) | 25 (21–29) | 24 (21–28) |
| <18.5, n (%) | 1085 (7.0) | 800 (7.1) | 1013 (9.0) | 1404 (12.1) |
| 18.5–24.9, n (%) | 4952 (32.1) | 3770 (33.4) | 4062 (36.2) | 4475 (38.7) |
| 25–29.9, n (%) | 4174 (27.1) | 3182 (28.2) | 3130 (27.9) | 2941 (25.4) |
| 30–34.9, n (%) | 2071 (13.4) | 1639 (14.5) | 1512 (13.5) | 1345 (11.6) |
| >=35, n (%) | 1153 (7.5) | 886 (7.8) | 779 (6.9) | 730 (6.3) |
| MRC, median (IQR) | 2 (2–3) | 3 (2–4) | 3 (2–4) | 3 (3–4) |
| 1, n (%) | 7130 (46.2) | 6193 (54.8) | 5761 (51.3) | 5533 (47.9) |
| 2, n (%) | 9796 (63.5) | 8275 (73.3) | 7635 (68.0) | 7041 (60.9) |
| 3, n (%) | 8709 (56.5) | 8248 (73.0) | 8539 (76.1) | 8382 (72.5) |
| 4, n (%) | 6921 (44.9) | 6855 (60.7) | 7391 (65.9) | 8022 (69.4) |
| 5, n (%) | 6005 (38.9) | 6026 (53.3) | 6563 (58.5) | 7299 (63.1) |
| FEV1 % predicted, median (IQR) | 58 (44–70) | 52 (40–65) | 45 (33–58) | 39 (29–52) |
| >=80, n (%) | 1642 (10.6) | 777 (6.9) | 431 (3.8) | 261 (2.3) |
| 50–79, n (%) | 7218 (46.8) | 4890 (43.3) | 3795 (33.8) | 2904 (25.1) |
| 30–49, n (%) | 3636 (23.6) | 3597 (31.8) | 4362 (38.9) | 4781 (41.4) |
| <30, n (%) | 872 (5.7) | 1006 (8.9) | 1860 (16.6) | 2867 (24.8) |
| Acute exacerbations requiring hospital admission in the past year, n (%) | ||||
| 0 | 13215 (85.7) | 8219 (72.8) | 7711 (68.7) | 7394 (64.0) |
| 1 | 1096 (7.1) | 1412 (12.5) | 1410 (12.6) | 1678 (14.5) |
| 2 or more | 1109 (7.2) | 1665 (14.7) | 2101 (18.7) | 2490 (21.5) |
| Charlson comorbidity index excluding HIV, median (IQR) | 4 (3–5) | 4 (3–5) | 4 (3–5) | 4 (3–5) |
| Myocardial infarction, n (%) | 1145 (7.4) | 870 (7.7) | 848 (7.6) | 813 (7.0) |
| Heart failure, n (%) | 2396 (15.5) | 1792 (15.9) | 1675 (14.9) | 1735 (15.0) |
| Peripheral vasc. disease, n (%) | 1943 (12.6) | 1343 (11.9) | 1274 (11.4) | 1219 (10.5) |
| Cerebrovasc. disease, n (%) | 1860 (12.1) | 1367 (12.1) | 1248 (11.1) | 1180 (10.2) |
| Dementia, n (%) | 265 (1.7) | 162 (1.4) | 177 (1.6) | 192 (1.7) |
| Rheumatic disease, n (%) | 792 (5.1) | 509 (4.5) | 470 (4.2) | 411 (3.6) |
| Peptic ulcers, n (%) | 779 (5.1) | 601 (5.3) | 554 (4.9) | 645 (5.6) |
| Mild liver disease, n (%) | 462 (3.0) | 296 (2.6) | 217 (1.9) | 224 (1.9) |
| Moderate or severe liver disease, n (%) | 109 (0.7) | 59 (0.5) | 49 (0.4) | 34 (0.3) |
| Diabetes mellitus without chronic complication, n (%) | 1874 (12.2) | 1347 (11.9) | 1166 (10.4) | 1200 (10.4) |
| Diabetes mellitus with chronic complication, n (%) | 645 (4.2) | 452 (4.0) | 369 (3.3) | 327 (2.8) |
| Kidney disease, n (%) | 729 (4.7) | 469 (4.2) | 374 (3.3) | 338 (2.9) |
| Asthma, n (%) | 1013 (6.6) | 1728 (15.3) | 2106 (18.8) | 2481 (21.5) |
| No ICS Exposure N = 15,420 | Low ICS Exposure N = 11,296 <384 μg/day | p-Value | Medium ICS Exposure N = 11,222 384 μg/day ≤ x <947 μg/day | p-Value | High ICS Exposure N = 11,562 ≥947 μg/day | p-Value | |
|---|---|---|---|---|---|---|---|
| Collection of any antidepressant within 5 years or all-cause mortality, HR (95% CI) | Reference | 1.05 (1.03–1.07) | 0.0472 | 1.10 (1.08–1.12) | <0.0001 | 1.15 (1.11–1.15) | <0.0001 |
| Collection of any antidepressant, HR (95% CI) a | Reference | 1.10 (1.07–1.13) | <0.0001 | 1.16 (1.13–1.19) | <0.0001 | 1.17 (1.15–1.20) | <0.0001 |
| All-cause mortality, HR (95% CI) a | Reference | 1.00 (0.97–1.02) | 0.77 | 1.06 (1.04–1.09) | <0.0001 | 1.12 (1.10–1.15) | <0.0001 |
| Admission with diagnosis depression, anxiety or bipolar disorder or all-cause mortality, HR (95% CI) | Reference | 1.00 (0.98–1.03) | 0.77 | 1.07 (1.05–1.10) | <0.0001 | 1.13 (1.10–1.15) | <0.0001 |
| Admission with diagnosis depression, anxiety or bipolar disorder, HR (95% CI)a | Reference | 1.21 (1.07–1.38) | 0.0035 | 1.32 (1.16–1.49) | <0.0001 | 1.22 (1.07–1.39) | 0.0027 |
| All-cause mortality, HR (95% CI)a | Reference | 1.00 (0.97–1.02) | 0.77 | 1.06 (1.04–1.09) | <0.0001 | 1.12 (1.10–1.15) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jordan, A.; Sivapalan, P.; Eklöf, J.; Vestergaard, J.B.; Meteran, H.; Saeed, M.I.; Biering-Sørensen, T.; Løkke, A.; Seersholm, N.; Jensen, J.U.S. The Association between Use of ICS and Psychiatric Symptoms in Patients with COPD—A Nationwide Cohort Study of 49,500 Patients. Biomedicines 2021, 9, 1492. https://doi.org/10.3390/biomedicines9101492
Jordan A, Sivapalan P, Eklöf J, Vestergaard JB, Meteran H, Saeed MI, Biering-Sørensen T, Løkke A, Seersholm N, Jensen JUS. The Association between Use of ICS and Psychiatric Symptoms in Patients with COPD—A Nationwide Cohort Study of 49,500 Patients. Biomedicines. 2021; 9(10):1492. https://doi.org/10.3390/biomedicines9101492
Chicago/Turabian StyleJordan, Alexander, Pradeesh Sivapalan, Josefin Eklöf, Jakob B. Vestergaard, Howraman Meteran, Mohamad Isam Saeed, Tor Biering-Sørensen, Anders Løkke, Niels Seersholm, and Jens Ulrik Stæhr Jensen. 2021. "The Association between Use of ICS and Psychiatric Symptoms in Patients with COPD—A Nationwide Cohort Study of 49,500 Patients" Biomedicines 9, no. 10: 1492. https://doi.org/10.3390/biomedicines9101492
APA StyleJordan, A., Sivapalan, P., Eklöf, J., Vestergaard, J. B., Meteran, H., Saeed, M. I., Biering-Sørensen, T., Løkke, A., Seersholm, N., & Jensen, J. U. S. (2021). The Association between Use of ICS and Psychiatric Symptoms in Patients with COPD—A Nationwide Cohort Study of 49,500 Patients. Biomedicines, 9(10), 1492. https://doi.org/10.3390/biomedicines9101492