
Real-Life Effectiveness of Mepolizumab on Forced Expiratory Flow between 25% and 75% of Forced Vital Capacity in Patients with Severe Eosinophilic Asthma

 ,
,  , ,
, ,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Asthma-Specific Outcome Variables
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Population
3.2. Response to Mepolizumab
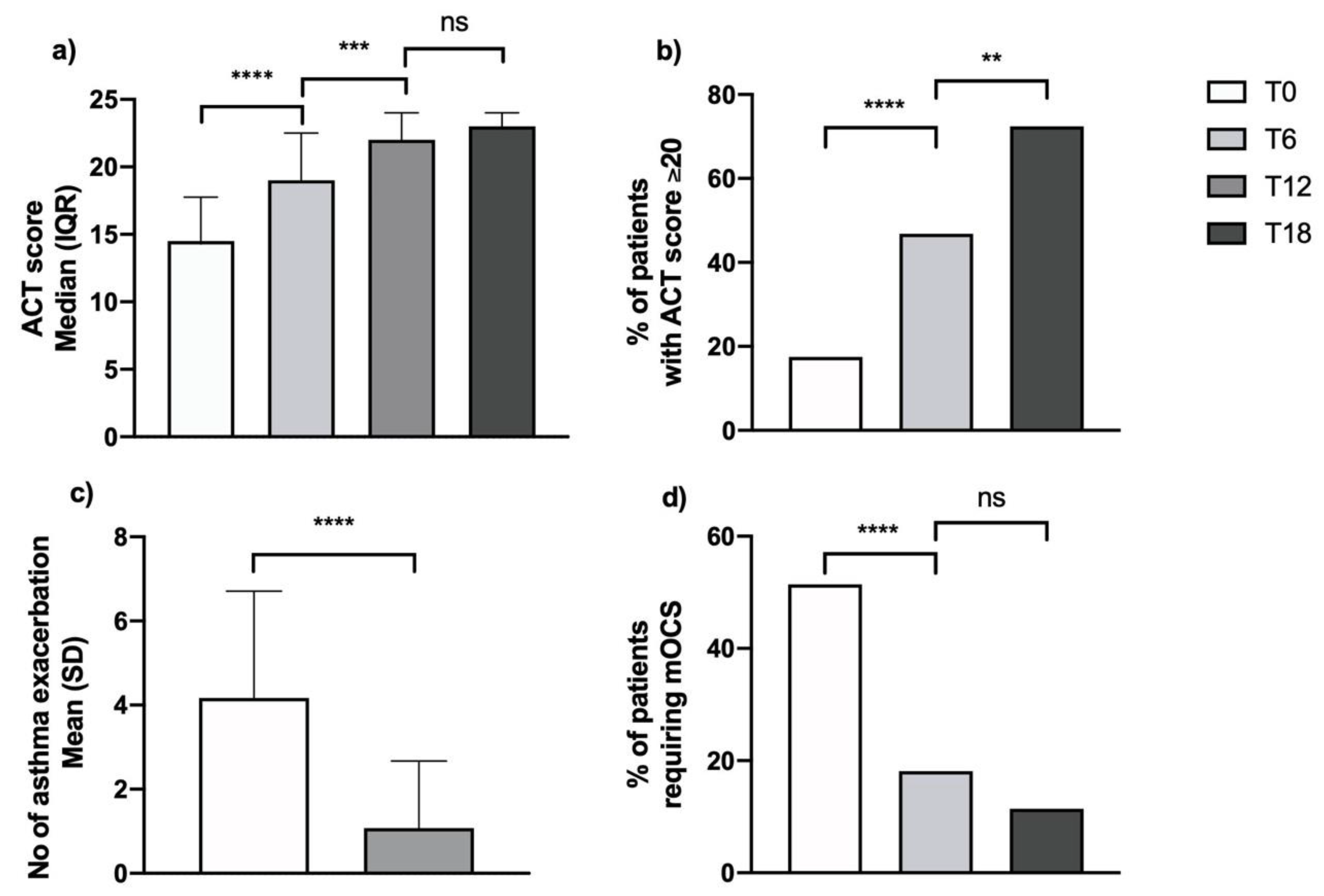
3.2.1. Clinical Effects
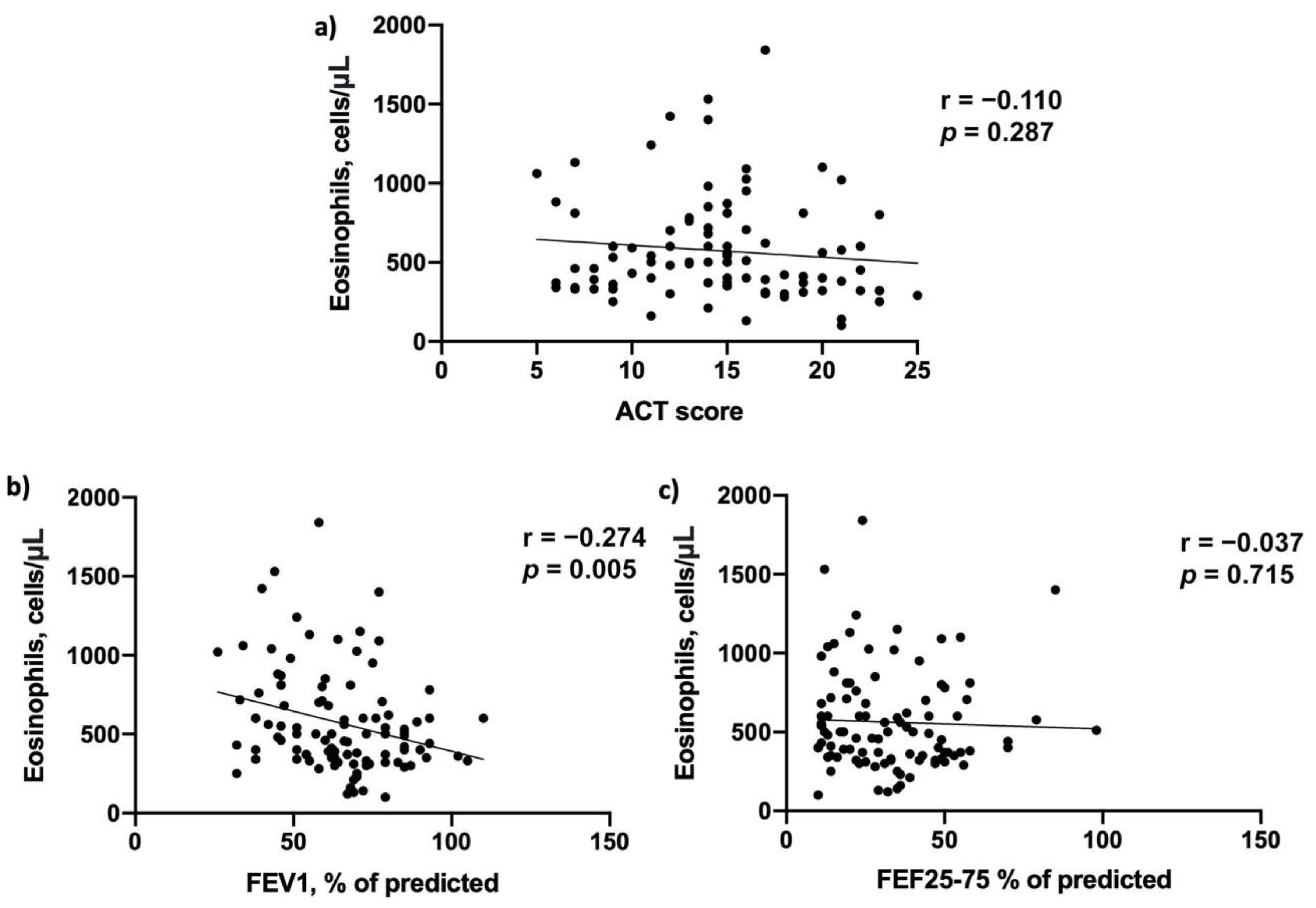
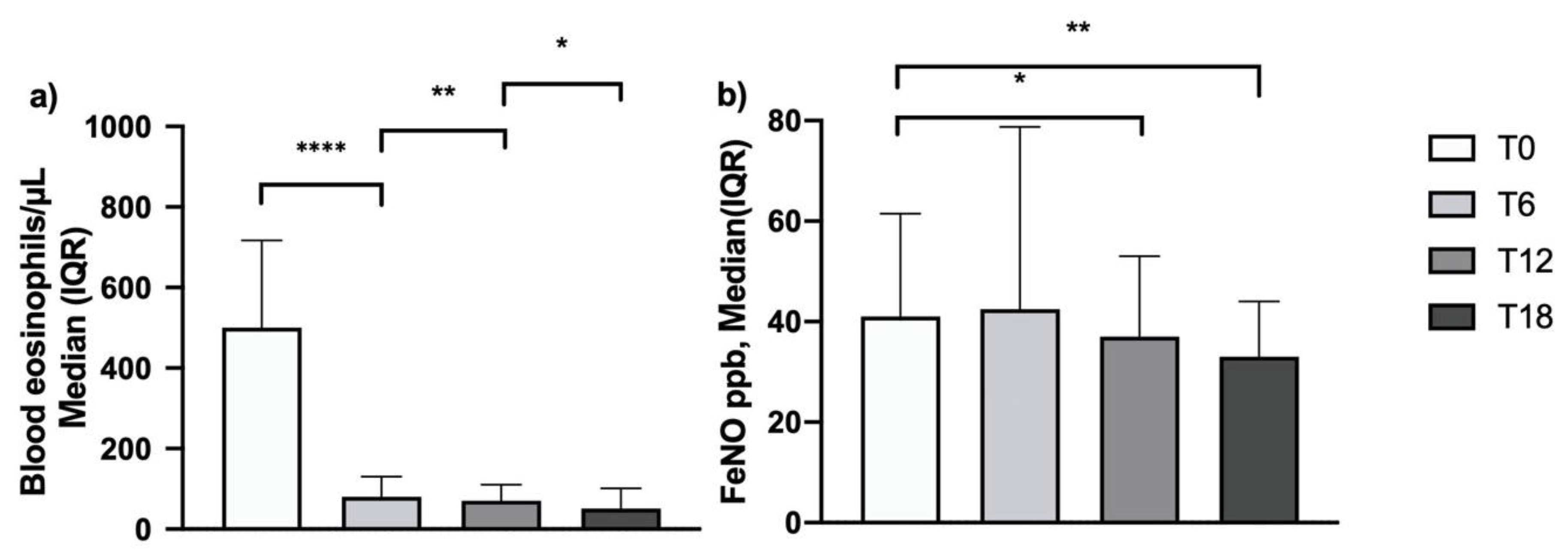
3.2.2. Biological Effects
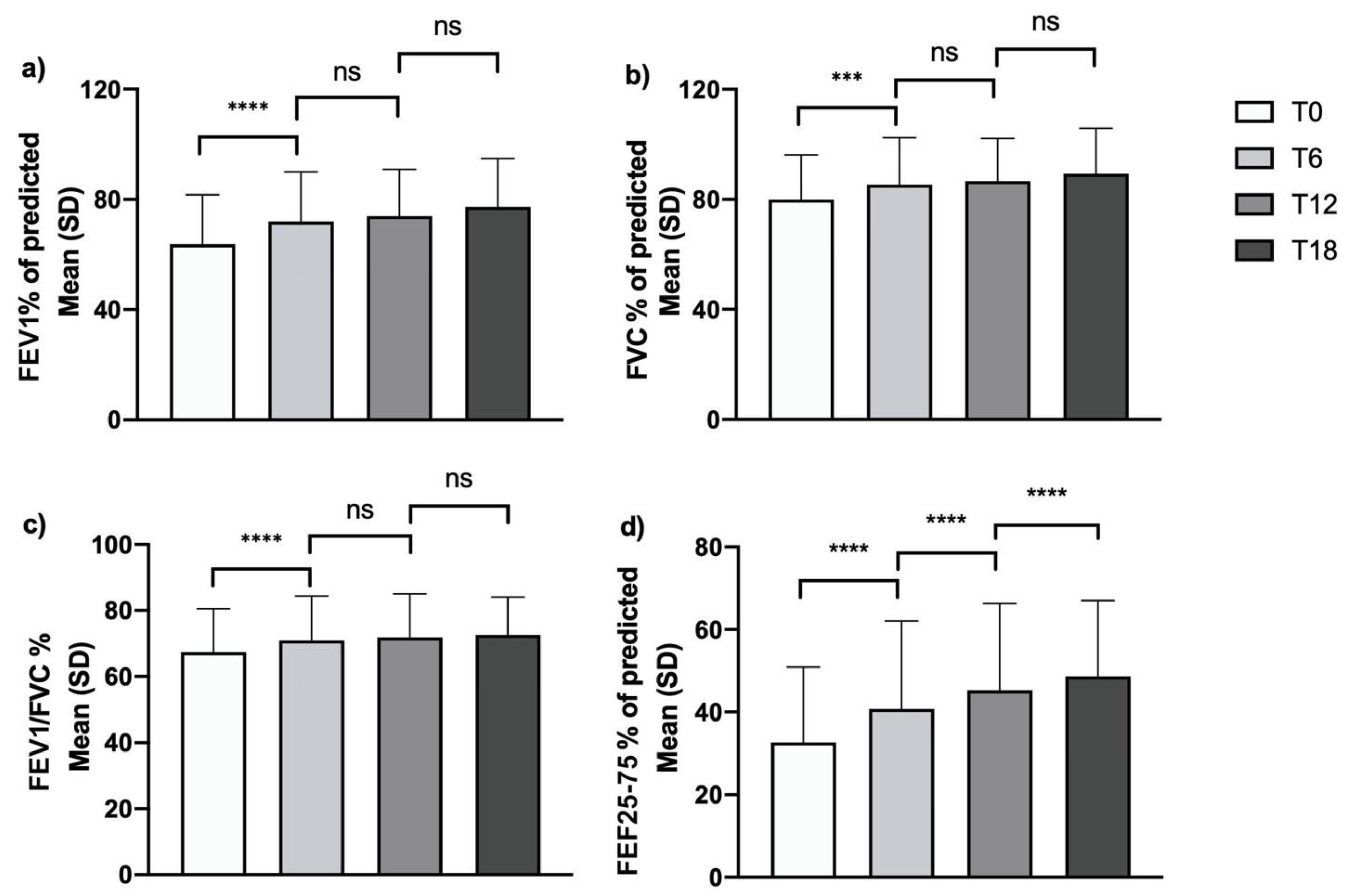
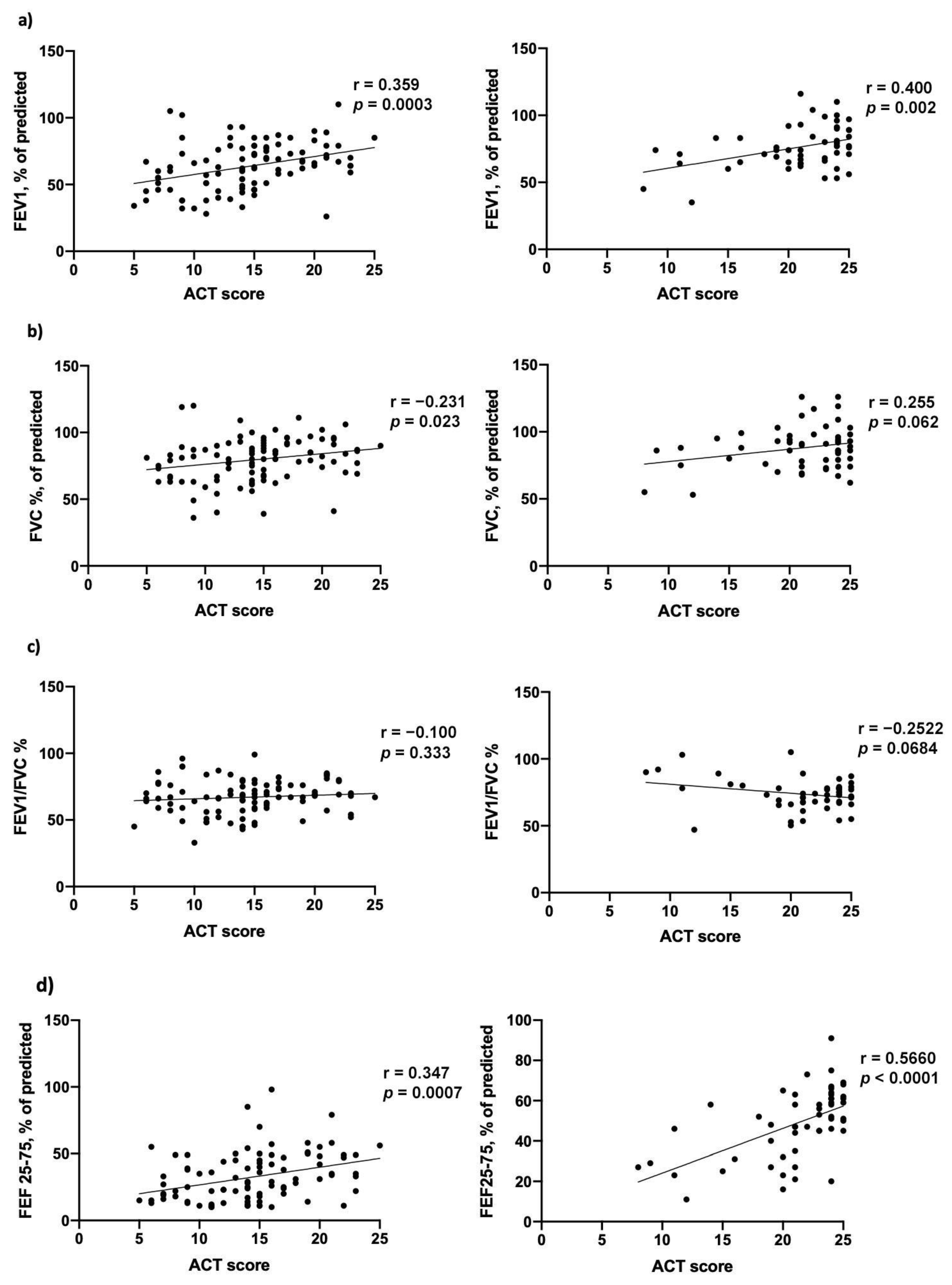
3.2.3. Effects on Pulmonary Function Tests
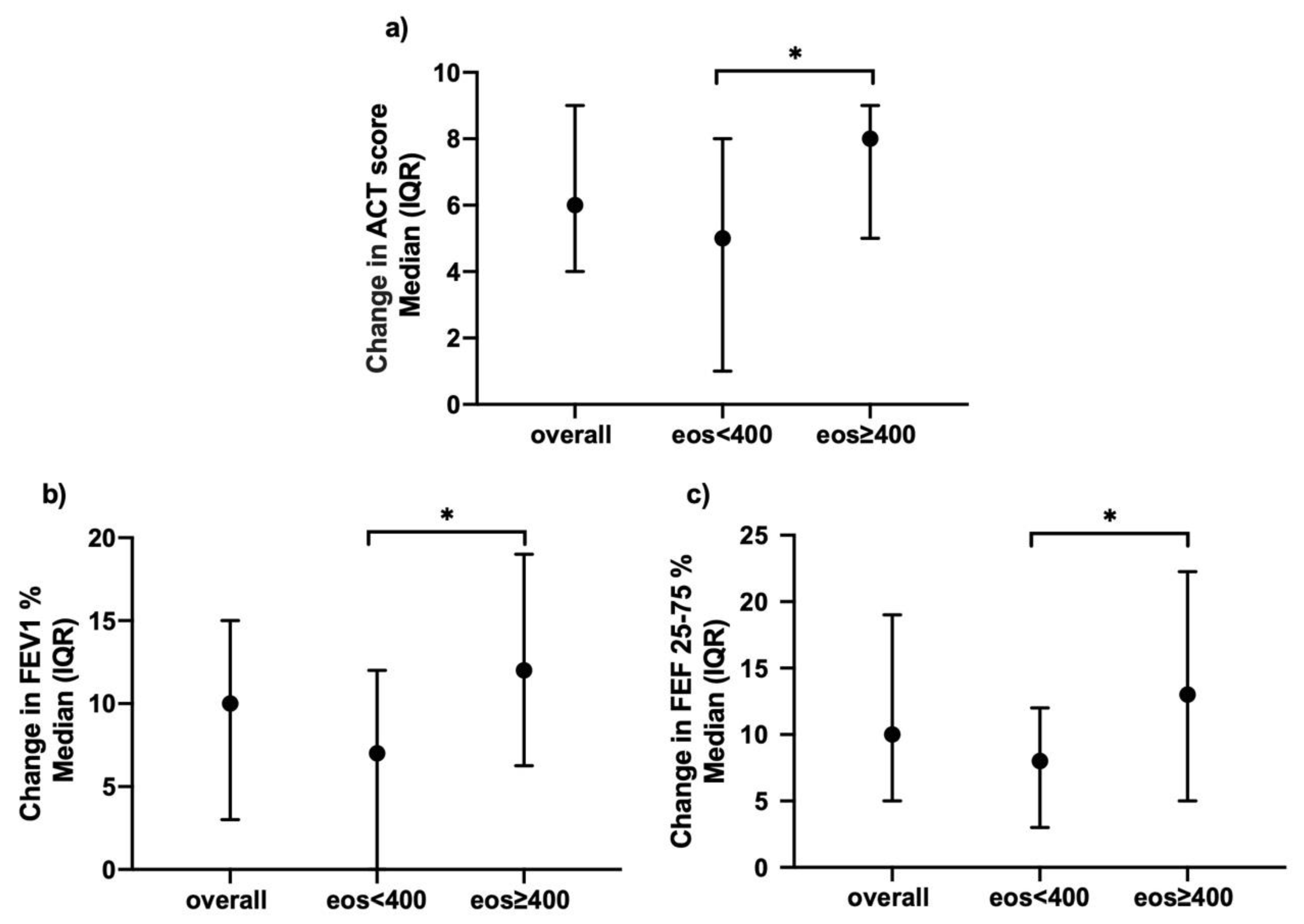
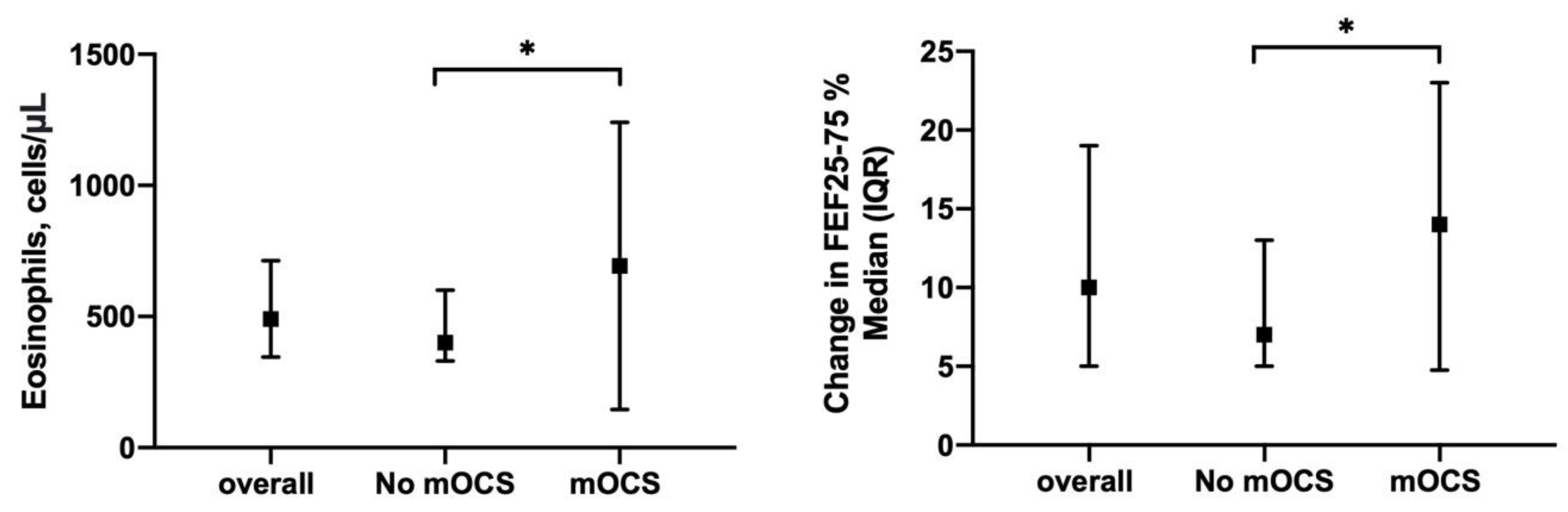
3.2.4. Efficacy of Mepolizumab across Different Subgroups of Asthmatic Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vatrella, A.; Maglio, A.; Pelaia, C.; Pelaia, G.; Vitale, C. Pharmacotherapeutic Strategies for Critical Asthma Syndrome: A Look at the State of the Art. Expert Opin. Pharmacother. 2020, 21, 1505–1515. [Google Scholar] [CrossRef]
- 2020 GINA Main Report. Available online: https://ginasthma.org/gina-reports/ (accessed on 15 January 2021).
- Vatrella, A.; Maglio, A.; Pellegrino, S.; Pelaia, C.; Stellato, C.; Pelaia, G.; Vitale, C. Phenotyping Severe Asthma: A Rationale for Biologic Therapy. Expert Rev. Precis. Med. Drug Dev. 2020, 5, 265–274. [Google Scholar] [CrossRef]
- Pelaia, C.; Vatrella, A.; Busceti, M.T.; Gallelli, L.; Terracciano, R.; Savino, R.; Pelaia, G. Severe Eosinophilic Asthma: From the Pathogenic Role of Interleukin-5 to the Therapeutic Action of Mepolizumab. DDDT 2017, 11, 3137–3144. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.C.; Wenzel, S.E. Intersection of Biology and Therapeutics: Type 2 Targeted Therapeutics for Adult Asthma. Lancet 2020, 395, 371–383. [Google Scholar] [CrossRef]
- Kuruvilla, M.E.; Lee, F.E.-H.; Lee, G.B. Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clin. Rev. Allerg. Immunol. 2019, 56, 219–233. [Google Scholar] [CrossRef]
- Ortega, H.; Llanos, J.-P.; Lafeuille, M.-H.; Duh, M.S.; Germain, G.; Lejeune, D.; Sama, S.; Bell, C.; Hahn, B. Effects of Systemic Corticosteroids on Blood Eosinophil Counts in Asthma: Real-World Data. J. Asthma. 2019, 56, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.C.; Kerr, S.; Dunican, E.M.; Woodruff, P.G.; Fajt, M.L.; Levy, B.D.; Israel, E.; Phillips, B.R.; Mauger, D.T.; Comhair, S.A.; et al. Refractory Airway Type 2 Inflammation in a Large Subgroup of Asthmatic Patients Treated with Inhaled Corticosteroids. J. Allergy Clin. Immunol. 2019, 143, 104–113.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, C.-J.; Huang, M.-T. Asthma in the Precision Medicine Era: Biologics and Probiotics. Int. J. Mol. Sci. 2021, 22, 4528. [Google Scholar] [CrossRef]
- Postma, D.S.; Brightling, C.; Baldi, S.; Van den Berge, M.; Fabbri, L.M.; Gagnatelli, A.; Papi, A.; Van der Molen, T.; Rabe, K.F.; Siddiqui, S.; et al. Exploring the Relevance and Extent of Small Airways Dysfunction in Asthma (ATLANTIS): Baseline Data from a Prospective Cohort Study. Lancet Respir. Med. 2019, 7, 402–416. [Google Scholar] [CrossRef] [Green Version]
- Farah, C.S.; King, G.G.; Brown, N.J.; Downie, S.R.; Kermode, J.A.; Hardaker, K.M.; Peters, M.J.; Berend, N.; Salome, C.M. The Role of the Small Airways in the Clinical Expression of Asthma in Adults. J. Allergy Clin. Immunol. 2012, 129, 381–387.e1. [Google Scholar] [CrossRef]
- Chupp, G.L.; Bradford, E.S.; Albers, F.C.; Bratton, D.J.; Wang-Jairaj, J.; Nelsen, L.M.; Trevor, J.L.; Magnan, A.; Ten Brinke, A. Efficacy of Mepolizumab Add-on Therapy on Health-Related Quality of Life and Markers of Asthma Control in Severe Eosinophilic Asthma (MUSCA): A Randomised, Double-Blind, Placebo-Controlled, Parallel-Group, Multicentre, Phase 3b Trial. Lancet Respir. Med. 2017, 5, 390–400. [Google Scholar] [CrossRef]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; FitzGerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab Treatment in Patients with Severe Eosinophilic Asthma. N. Engl. J. Med. 2014, 371, 1198–1207. [Google Scholar] [CrossRef] [Green Version]
- Pavord, I.D.; Korn, S.; Howarth, P.; Bleecker, E.R.; Buhl, R.; Keene, O.N.; Ortega, H.; Chanez, P. Mepolizumab for Severe Eosinophilic Asthma (DREAM): A Multicentre, Double-Blind, Placebo-Controlled Trial. Lancet 2012, 380, 651–659. [Google Scholar] [CrossRef]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS Guidelines on Definition, Evaluation and Treatment of Severe Asthma. Eur. Respir. J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, M.; Zangrilli, J.; Wechsler, M.E.; Bateman, E.D.; Brusselle, G.G.; Bardin, P.; Murphy, K.; Maspero, J.F.; O’Brien, C.; Korn, S. Reslizumab for Inadequately Controlled Asthma with Elevated Blood Eosinophil Counts: Results from Two Multicentre, Parallel, Double-Blind, Randomised, Placebo-Controlled, Phase 3 Trials. Lancet Respir. Med. 2015, 3, 355–366. [Google Scholar] [CrossRef]
- Price, D.B.; Rigazio, A.; Campbell, J.D.; Bleecker, E.R.; Corrigan, C.J.; Thomas, M.; Wenzel, S.E.; Wilson, A.M.; Small, M.B.; Gopalan, G.; et al. Blood Eosinophil Count and Prospective Annual Asthma Disease Burden: A UK Cohort Study. Lancet Respir. Med. 2015, 3, 849–858. [Google Scholar] [CrossRef]
- Pelaia, C.; Busceti, M.T.; Solinas, S.; Terracciano, R.; Pelaia, G. Real-Life Evaluation of the Clinical, Functional, and Hematological Effects of Mepolizumab in Patients with Severe Eosinophilic Asthma: Results of a Single-Centre Observational Study. Pulm. Pharmacol. Ther. 2018, 53, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Schleich, F.; Graff, S.; Nekoee, H.; Moermans, C.; Henket, M.; Sanchez, C.; Paulus, V.; Guissard, F.; Donneau, A.-F.; Louis, R. Real-Word Experience with Mepolizumab: Does It Deliver What It Has Promised? Clin. Exp. Allergy 2020, 50, 687–695. [Google Scholar] [CrossRef]
- van Toor, J.J.; van der Mark, S.C.; Kappen, J.H.; Veen, J.C.C.M.I.; Braunstahl, G.J. Mepolizumab Add-on Therapy in a Real World Cohort of Patients with Severe Eosinophilic Asthma: Response Rate, Effectiveness, and Safety. J. Asthma 2020, 58, 651–658. [Google Scholar] [CrossRef]
- Harvey, E.S.; Langton, D.; Katelaris, C.; Stevens, S.; Farah, C.S.; Gillman, A.; Harrington, J.; Hew, M.; Kritikos, V.; Radhakrishna, N.; et al. Mepolizumab Effectiveness and Identification of Super-Responders in Severe Asthma. Eur. Respir. J. 2020, 55. [Google Scholar] [CrossRef]
- Pertzov, B.; Unterman, A.; Shtraichman, O.; Shitenberg, D.; Rosengarten, D.; Kramer, M.R. Efficacy and Safety of Mepolizumab in a Real-World Cohort of Patients with Severe Eosinophilic Asthma. J. Asthma 2019, 58, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Calzetta, L.; Aiello, M.; Frizzelli, A.; Bertorelli, G.; Ritondo, B.L.; Rogliani, P.; Chetta, A. The Impact of Monoclonal Antibodies on Airway Smooth Muscle Contractility in Asthma: A Systematic Review. Biomedicines 2021, 9, 1281. [Google Scholar] [CrossRef] [PubMed]
- Farne, H.; Wilson, A.; Powell, C.; Bax, L.; Milan, S. Anti-IL5 Therapies for Asthma. Cochrane Database Syst. Rev. 2017, 9, 4. [Google Scholar] [CrossRef]
- Pelaia, G.; Vatrella, A.; Busceti, M.T.; Gallelli, L.; Preianò, M.; Lombardo, N.; Terracciano, R.; Maselli, R. Role of Biologics in Severe Eosinophilic Asthma—Focus on Reslizumab. Ther. Clin. Risk Manag. 2016, 12, 1075–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelaia, C.; Calabrese, C.; Vatrella, A.; Busceti, M.T.; Garofalo, E.; Lombardo, N.; Terracciano, R.; Pelaia, G. Benralizumab: From the Basic Mechanism of Action to the Potential Use in the Biological Therapy of Severe Eosinophilic Asthma. BioMed Res. Int. 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Ortega, H.G.; Yancey, S.W.; Mayer, B.; Gunsoy, N.B.; Keene, O.N.; Bleecker, E.R.; Brightling, C.E.; Pavord, I.D. Severe Eosinophilic Asthma Treated with Mepolizumab Stratified by Baseline Eosinophil Thresholds: A Secondary Analysis of the DREAM and MENSA Studies. Lancet Respir. Med. 2016, 4, 549–556. [Google Scholar] [CrossRef]
- Cottini, M.; Licini, A.; Lombardi, C.; Bagnasco, D.; Comberiati, P.; Berti, A. Small Airway Dysfunction and Poor Asthma Control: A Dangerous Liaison. Clin. Mol. Allergy 2021, 19, 7. [Google Scholar] [CrossRef]
- Riley, C.M.; Wenzel, S.E.; Castro, M.; Erzurum, S.C.; Chung, K.F.; Fitzpatrick, A.M.; Gaston, B.; Israel, E.; Moore, W.C.; Bleecker, E.R.; et al. Clinical Implications of Having Reduced Mid Forced Expiratory Flow Rates (FEF25-75), Independently of FEV1, in Adult Patients with Asthma. PLoS ONE 2015, 10, e0145476. [Google Scholar] [CrossRef] [Green Version]
- Tosca, M.A.; Silvestri, M.; Solari, N.; Rossi, G.A.; Ciprandi, G. Inflammation Markers and FEF25-75: A Relevant Link in Children With Asthma. Allergy Asthma Immunol. Res. 2016, 8, 84–85. [Google Scholar] [CrossRef] [Green Version]
- Malerba, M.; Radaeli, A.; Olivini, A.; Damiani, G.; Ragnoli, B.; Sorbello, V.; Ricciardolo, F.L.M. Association of FEF25-75% Impairment with Bronchial Hyperresponsiveness and Airway Inflammation in Subjects with Asthma-Like Symptoms. Respiration 2016, 91, 206–214. [Google Scholar] [CrossRef]
- de Groot, J.C.; Storm, H.; Amelink, M.; de Nijs, S.B.; Eichhorn, E.; Reitsma, B.H.; Bel, E.H.D.; ten Brinke, A. Clinical Profile of Patients with Adult-Onset Eosinophilic Asthma. ERJ Open Res. 2016, 2. [Google Scholar] [CrossRef]
- Farah, C.S.; Badal, T.; Reed, N.; Rogers, P.G.; King, G.G.; Thamrin, C.; Peters, M.J.; Seccombe, L.M. Mepolizumab Improves Small Airway Function in Severe Eosinophilic Asthma. Respir. Med. 2019, 148, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Sposato, B.; Camiciottoli, G.; Bacci, E.; Scalese, M.; Carpagnano, G.E.; Pelaia, C.; Santus, P.; Maniscalco, M.; Masieri, S.; Corsico, A.; et al. Mepolizumab Effectiveness on Small Airway Obstruction, Corticosteroid Sparing and Maintenance Therapy Step-down in Real Life. Pulm. Pharmacol. Ther. 2020, 61, 101899. [Google Scholar] [CrossRef]
- Hamid, Q.A. Peripheral Inflammation Is More Important than Central Inflammation. Respir. Med. 1997, 91, 11–12. [Google Scholar] [CrossRef] [Green Version]
- Pons, N.T.; Boven, J.F.V.; Román-Rodríguez, M.; Millán, A.; Kocks, J.W.H.; Soriano, J.B.; Cosio, B.G. Eosinophil Distribution and Description in a Population Cohort of Asthmatic Patients. Eur. Respir. J. 2019, 54. [Google Scholar] [CrossRef]
- 1 Recommendations|Mepolizumab for Treating Severe Refractory Eosinophilic Asthma|Guidance|NICE. Available online: https://www.nice.org.uk/guidance/ta431/chapter/1-Recommendations (accessed on 21 July 2020).
- Prazma, C.M.; Wenzel, S.; Barnes, N.; Douglass, J.A.; Hartley, B.F.; Ortega, H. Characterisation of an OCS-Dependent Severe Asthma Population Treated with Mepolizumab. Thorax 2014, 69, 1141–1142. [Google Scholar] [CrossRef] [Green Version]
- Pelaia, C.; Crimi, C.; Pelaia, G.; Nolasco, S.; Campisi, R.; Heffler, E.; Valenti, G.; Crimi, N. Real-Life Evaluation of Mepolizumab Efficacy in Patients with Severe Eosinophilic Asthma, According to Atopic Trait and Allergic Phenotype. Clin. Exp. Allergy 2020, 50, 780–788. [Google Scholar] [CrossRef]
- Miethe, S.; Guarino, M.; Alhamdan, F.; Simon, H.-U.; Renz, H.; Dufour, J.-F.; Potaczek, D.P.; Garn, H. Effects of Obesity on Asthma: Immunometabolic Links. Pol. Arch. Intern. Med. 2018, 128, 469–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhamdan, F.; Marsh, L.M.; Pedersen, F.; Alhamwe, B.A.; Thölken, C.; Pfefferle, P.I.; Bahmer, T.; Greulich, T.; Potaczek, D.P.; Garn, H. Differential Regulation of Interferon Signaling Pathways in CD4+ T Cells of the Low Type-2 Obesity-Associated Asthma Phenotype. Int. J. Mol. Sci. 2021, 22, 10144. [Google Scholar] [CrossRef]
- Tashiro, H.; Shore, S.A. Obesity and Severe Asthma. Allergol. Int. 2019, 68, 135–142. [Google Scholar] [CrossRef]
- Nair, P.; O’Byrne, P.M. Measuring Eosinophils to Make Treatment Decisions in Asthma. Chest 2016, 150, 485–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busse, W.; Chupp, G.; Nagase, H.; Albers, F.C.; Doyle, S.; Shen, Q.; Bratton, D.J.; Gunsoy, N.B. Anti–IL-5 Treatments in Patients with Severe Asthma by Blood Eosinophil Thresholds: Indirect Treatment Comparison. J. Allergy Clin. Immunol. 2019, 143, 190–200.e20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Measurement of FEF25–75% and FEF75% Does Not Contribute to Clinical Decision Making|European Respiratory Society. Available online: https://erj.ersjournals.com/content/43/4/1051 (accessed on 19 November 2020).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics (n = 105) | |
| Age | 58.5 ± 11.0 |
| Gender (female) | 67 (63.8%) |
| Smoking habit (n = 102) | |
| Never | 58 (56.86%) |
| Smokers | 19 (18.63%) |
| Ex-smokers | 25 (24.51%) |
| Body Mass Index kg/m2, n = 105 | 27.4 ± 4.2 |
| Asthma duration, years, n = 93 | 21.5 ± 13.7 |
| Age of asthma onset, years, n = 93 | 37.4 ± 14.3 |
| Atopy * | 58 (55.2%) |
| Comorbidities | |
| Obesity (BMI ≥ 30 kg/m2) | 24 (22.7%) |
| Chronic rhinosinusitis both allergic and not allergic | 55 (57.75%) |
| Nasal polyposis | 35 (33.3%) |
| Gastroesophageal reflux disease | 29 (27.6%) |
| Biomarkers | |
| Peripheral Blood Eosinophils/μL | 500 (340; 727.8) |
| Total IgE, IU/mL (n = 78) | 182 (73.5; 406.5) |
| FeNO, ppb (n = 73) | 41 (25, 61) |
| Lung function | |
| FEV1% predicted | 63.7 ± 17.9 |
| FVC% predicted | 79.9 ± 16.2 |
| FEV1/FVC% | 67.5 ± 13 |
| FEF25-75% predicted | 32.7 ± 18.2 |
| ACT (n = 98) | 14.5 (11; 17.7) |
| Exacerbation history (previous year) (n = 84) | 4.2 ± 2.5 |
| Maintenance therapy | |
| ICS/LABA | 105 (100%) |
| LAMA | 63 (60%) |
| OCS | 54 (51.43%) |
| LTRA | 4 (3.80%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maglio, A.; Vitale, C.; Pellegrino, S.; Calabrese, C.; D’Amato, M.; Molino, A.; Pelaia, C.; Triggiani, M.; Pelaia, G.; Stellato, C.; et al. Real-Life Effectiveness of Mepolizumab on Forced Expiratory Flow between 25% and 75% of Forced Vital Capacity in Patients with Severe Eosinophilic Asthma. Biomedicines 2021, 9, 1550. https://doi.org/10.3390/biomedicines9111550
Maglio A, Vitale C, Pellegrino S, Calabrese C, D’Amato M, Molino A, Pelaia C, Triggiani M, Pelaia G, Stellato C, et al. Real-Life Effectiveness of Mepolizumab on Forced Expiratory Flow between 25% and 75% of Forced Vital Capacity in Patients with Severe Eosinophilic Asthma. Biomedicines. 2021; 9(11):1550. https://doi.org/10.3390/biomedicines9111550
Chicago/Turabian StyleMaglio, Angelantonio, Carolina Vitale, Simona Pellegrino, Cecilia Calabrese, Maria D’Amato, Antonio Molino, Corrado Pelaia, Massimo Triggiani, Girolamo Pelaia, Cristiana Stellato, and et al. 2021. "Real-Life Effectiveness of Mepolizumab on Forced Expiratory Flow between 25% and 75% of Forced Vital Capacity in Patients with Severe Eosinophilic Asthma" Biomedicines 9, no. 11: 1550. https://doi.org/10.3390/biomedicines9111550
APA StyleMaglio, A., Vitale, C., Pellegrino, S., Calabrese, C., D’Amato, M., Molino, A., Pelaia, C., Triggiani, M., Pelaia, G., Stellato, C., & Vatrella, A. (2021). Real-Life Effectiveness of Mepolizumab on Forced Expiratory Flow between 25% and 75% of Forced Vital Capacity in Patients with Severe Eosinophilic Asthma. Biomedicines, 9(11), 1550. https://doi.org/10.3390/biomedicines9111550