
The Challenge of 3D Bioprinting of Composite Natural Polymers PLA/Bioglass: Trends and Benefits in Cleft Palate Surgery


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Facial Clefts
2.1. Prevalence and Etio-Pathogenesis
2.2. Current Care and Support
3. Bioglasses
3.1. A Few General Points
3.2. Shaping
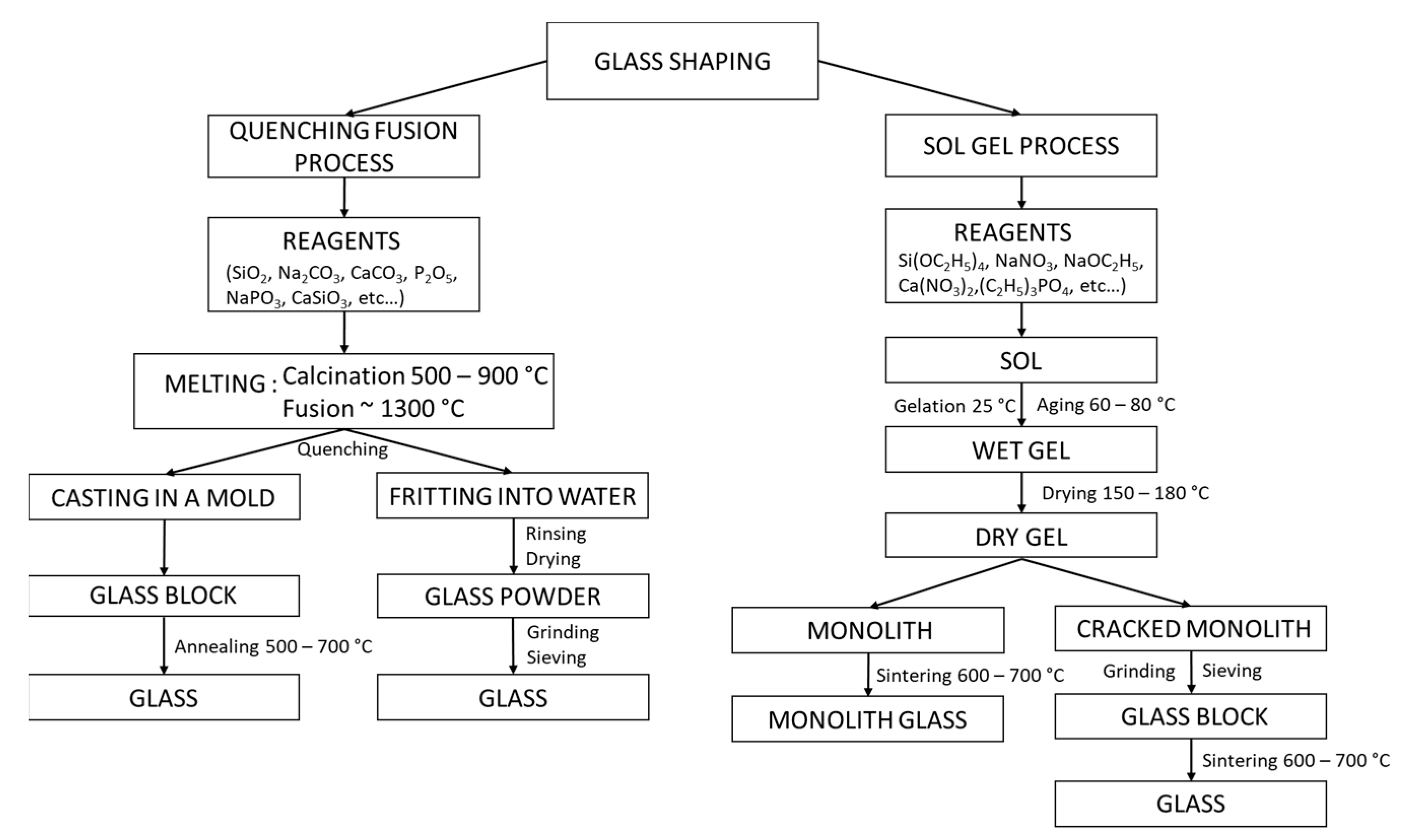
3.2.1. Shaping by Quenching Fusion Process
3.2.2. Shaping by Sol–Gel Process
- − Hydrolysis: Si-OR + H2O → Si-OH + ROH
- − Condensation: Si-OH + RO-Si → Si-O-Si + ROH or Si-OH + HO-Si → Si-O-Si + H2O
3.3. Biological Properties of Binding to Bone
- Rapid exchange of Na+ and/or Ca2+ cations with H+ from the solution, creating silanol (Si-OH) bonds on the glass surface;
- Attack of the silica glass network by OH−;
- Condensation of Si-OH groups near the glass surface: re-polymerization of the silica-rich layer;
- Migration of Ca2+ and groups to the surface through the silica-rich layer and from the solution, forming an amorphous CaO-P2O5-rich film on the silica-rich layer;
- Incorporation of hydroxyls and carbonate from solution and crystallization of the CaO-P2O5 film into hydroxyapatite.
4. Poly-Lactic Acid Matrices, Natural Polymers
4.1. Overview
4.2. Shaping and Sterilization
5. Shaping by 3D Printing for Biomaterials
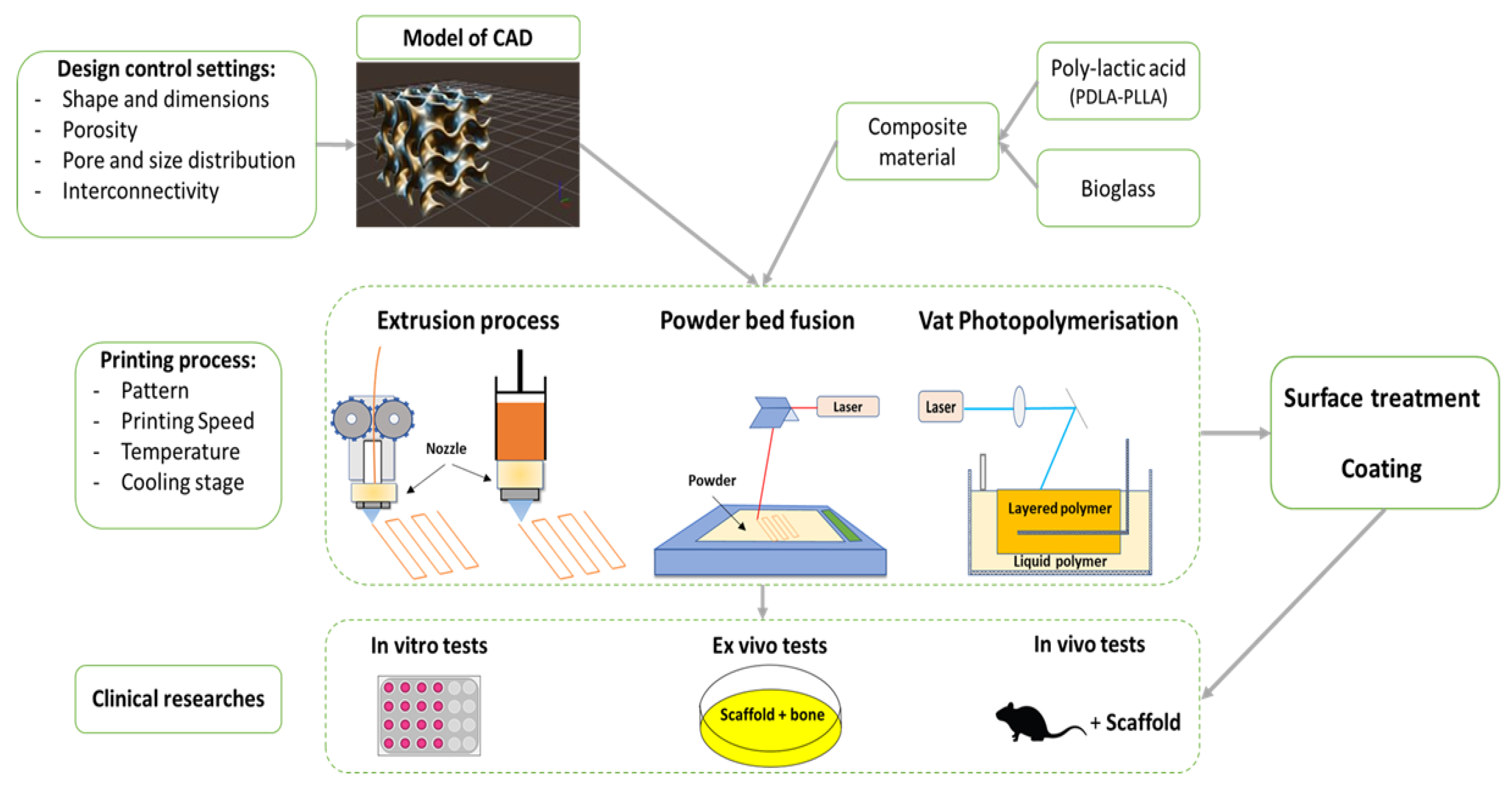
5.1. PLA–Bioglass Composite
5.2. Vat Photopolymerisation
5.3. Powder Bed Fusion
5.4. Extrusion Techniques
6. Application Perspective in Regenerative Medicine and Cleft Surgery
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ysunza, P.A.; Pamplona, M.C.; Repetto, G. Cleft Palate, Interdisciplinary Diagnosis, and Treatment. BioMed Res. Int. 2015, 2015, e701850. [Google Scholar] [CrossRef] [PubMed]
- Shkoukani, M.A.; Lawrence, L.A.; Liebertz, D.J.; Svider, P.F. Cleft Palate: A Clinical Review. Birth Defects Res. Part C Embryo Today Rev. 2014, 102, 333–342. [Google Scholar] [CrossRef]
- Schmitz, J.P.; Hollinger, J.O. The Critical Size Defect as an Experimental Model for Craniomandibulofacial Nonunions. Clin. Orthop. 1986, 299–308. [Google Scholar] [CrossRef]
- Sharif, F.; Ur Rehman, I.; Muhammad, N.; MacNeil, S. Dental Materials for Cleft Palate Repair. Mater. Sci. Eng. C 2016, 61, 1018–1028. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.V.; Dinopoulos, H.; Tsiridis, E. Bone Substitutes: An Update. Injury 2005, 36, S20–S27. [Google Scholar] [CrossRef] [PubMed]
- Graillon, N.; Degardin, N.; Foletti, J.M.; Seiler, M.; Alessandrini, M.; Gallucci, A. Bioactive Glass 45S5 Ceramic for Alveolar Cleft Reconstruction, about 58 Cases. J. Cranio-Maxillofac. Surg. Off. Publ. Eur. Assoc. Cranio-Maxillofac. Surg. 2018, 46, 1772–1776. [Google Scholar] [CrossRef] [PubMed]
- Distler, T.; Fournier, N.; Grünewald, A.; Polley, C.; Seitz, H.; Detsch, R.; Boccaccini, A.R. Polymer-Bioactive Glass Composite Filaments for 3D Scaffold Manufacturing by Fused Deposition Modeling: Fabrication and Characterization. Front. Bioeng. Biotechnol. 2020, 8, 552. [Google Scholar] [CrossRef]
- Mossey, P.A.; Little, J.; Munger, R.G.; Dixon, M.J.; Shaw, W.C. Cleft Lip and Palate. Lancet Lond. Engl. 2009, 374, 1773–1785. [Google Scholar] [CrossRef]
- Carinci, F.; Pezzetti, F.; Scapoli, L.; Martinelli, M.; Avantaggiato, A.; Carinci, P.; Padula, E.; Baciliero, U.; Gombos, F.; Laino, G.; et al. Recent Developments in Orofacial Cleft Genetics. J. Craniofac. Surg. 2003, 14, 130–143. [Google Scholar] [CrossRef]
- Merritt, L. Part 1. Understanding the Embryology and Genetics of Cleft Lip and Palate. Adv. Neonatal Care Off. J. Natl. Assoc. Neonatal Nurses 2005, 5, 64–71. [Google Scholar] [CrossRef]
- Harville, E.W.; Wilcox, A.J.; Lie, R.T.; Vindenes, H.; Åbyholm, F. Cleft Lip and Palate versus Cleft Lip Only: Are They Distinct Defects? Am. J. Epidemiol. 2005, 162, 448–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marazita, M.L.; Mooney, M.P. Current Concepts in the Embryology and Genetics of Cleft Lip and Cleft Palate. Clin. Plast. Surg. 2004, 31, 125–140. [Google Scholar] [CrossRef]
- Stanier, P.; Moore, G.E. Genetics of Cleft Lip and Palate: Syndromic Genes Contribute to the Incidence of Non-Syndromic Clefts. Hum. Mol. Genet. 2004, 13, R73–R81. [Google Scholar] [CrossRef]
- Dixon, M.J.; Marazita, M.L.; Beaty, T.H.; Murray, J.C. Cleft Lip and Palate: Understanding Genetic and Environmental Influences. Nat. Rev. Genet. 2011, 12, 167–178. [Google Scholar] [CrossRef] [Green Version]
- Murray, J.C. Gene/Environment Causes of Cleft Lip and/or Palate. Clin. Genet. 2002, 61, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Khoury, M.J. Evolving Methods in Genetic Epidemiology. III. Gene-Environment Interaction in Epidemiologic Research. Epidemiol. Rev. 1997, 19, 33–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianchi, F.; Calzolari, E.; Ciulli, L.; Cordier, S.; Gualandi, F.; Pierini, A.; Mossey, P. Environment and genetics in the etiology of cleft lip and cleft palate with reference to the role of folic acid. Epidemiol. Prev. 2000, 24, 21–27. [Google Scholar] [PubMed]
- Shkoukani, M.A.; Chen, M.; Vong, A. Cleft Lip—A Comprehensive Review. Front. Pediatr. 2013, 1, 53. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, M.; Palmieri, A.; Carinci, F.; Scapoli, L. Non-Syndromic Cleft Palate: An Overview on Human Genetic and Environmental Risk Factors. Front. Cell Dev. Biol. 2020, 8, 592271. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Bian, Z.; Torensma, R.; Von den Hoff, J.W. Biological Mechanisms in Palatogenesis and Cleft Palate. J. Dent. Res. 2009, 88, 22–33. [Google Scholar] [CrossRef]
- Karki, S.; Horváth, J.; Laitala, M.-L.; Vástyán, A.; Nagy, Á.; Sándor, G.K.; Anttonen, V. Validating and Assessing the Oral Health-Related Quality of Life among Hungarian Children with Cleft Lip and Palate Using Child-OIDP Scale. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2021, 22, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rando, G.M.; Jorge, P.K.; Vitor, L.L.R.; Carrara, C.F.C.; Soares, S.; Silva, T.C.; Rios, D.; Machado, M.A.A.M.; Gavião, M.B.; Oliveira, T.M. Oral Health-Related Quality of Life of Children with Oral Clefts and Their Families. J. Appl. Oral Sci. Rev. FOB 2018, 26, e20170106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapp-Simon, K.A. Psychological Issues in Cleft Lip and Palate. Clin. Plast. Surg. 2004, 31, 347–352. [Google Scholar] [CrossRef]
- Dao, A.M.; Goudy, S.L. Cleft Palate Repair, Gingivoperiosteoplasty, and Alveolar Bone Grafting. Facial Plast. Surg. Clin. N. Am. 2016, 24, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Leow, A.-M.; Lo, L.-J. Palatoplasty: Evolution and Controversies. Chang. Gung Med. J. 2008, 31, 335–345. [Google Scholar]
- Puente Espel, J.; Winters, R. Cleft Palate Repair. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Weissler, E.H.; Paine, K.M.; Ahmed, M.K.; Taub, P.J. Alveolar Bone Grafting and Cleft Lip and Palate: A Review. Plast. Reconstr. Surg. 2016, 138, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-L.; Shi, B.; Zheng, Q.; Li, C.-H. Alveolar Bone Grafting and Cleft Lip and Palate: A Review. Plast. Reconstr. Surg. 2017, 140, 359e–360e. [Google Scholar] [CrossRef]
- Matic, D.B.; Power, S.M. Evaluating the Success of Gingivoperiosteoplasty versus Secondary Bone Grafting in Patients with Unilateral Clefts. Plast. Reconstr. Surg. 2008, 121, 1343–1353. [Google Scholar] [CrossRef]
- Kasiri, N.; Bayani, M.; Mohammad-Rabei, E.; Ebrahimizadeh, H. Correlation between Alveolar Cleft Volume and Alveolar Bone Quality in Patients with Unilateral Cleft Lip and Palate: A Cone-Beam Computed Tomography Study. J. Stomatol. Oral Maxillofac. Surg. 2021. [Google Scholar] [CrossRef]
- Dissaux, C.; Bodin, F.; Grollemund, B.; Bridonneau, T.; Kauffmann, I.; Mattern, J.-F.; Bruant-Rodier, C. Evaluation of Success of Alveolar Cleft Bone Graft Performed at 5 Years versus 10 Years of Age. J. Cranio-Maxillofac. Surg. 2016, 44, 21–26. [Google Scholar] [CrossRef]
- Thuaksuban, N.; Nuntanaranont, T.; Pripatnanont, P. A Comparison of Autogenous Bone Graft Combined with Deproteinized Bovine Bone and Autogenous Bone Graft Alone for Treatment of Alveolar Cleft. Int. J. Oral Maxillofac. Surg. 2010, 39, 1175–1180. [Google Scholar] [CrossRef] [PubMed]
- Honma, K.; Kobayashi, T.; Nakajima, T.; Hayasi, T. Computed Tomographic Evaluation of Bone Formation after Secondary Bone Grafting of Alveolar Clefts. J. Oral Maxillofac. Surg. 1999, 57, 1209–1213. [Google Scholar] [CrossRef]
- Cricchio, G.; Lundgren, S. Donor Site Morbidity in Two Different Approaches to Anterior Iliac Crest Bone Harvesting. Clin. Implant Dent. Relat. Res. 2003, 5, 161–169. [Google Scholar] [CrossRef]
- Sbitany, H.; Koltz, P.F.; Waldman, J.; Girotto, J.A. Continuous Bupivacaine Infusion in Iliac Bone Graft Donor Sites to Minimize Pain and Hospitalization. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2010, 47, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Sequera-Ramos, L.; Ruby, J.M.; Jackson, O.A.; Ganesh, A.; Gurnaney, H.; Kraemer, F.W.; Muhly, W.T. Continuous Transversalis Fascia Plane Catheter Infusion in a Pediatric Patient Undergoing Alveolar Cleft Repair With Iliac Crest Bone Graft: A Case Report. AA Pract. 2019, 13, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.A.; Forrest, C.R.; Walsh, W.; Pétroz, G.C.; Adeli, K.; Bissonnette, B. Continuous Bupivacaine Infusion Post-Iliac Crest Bone Graft Harvesting in Pediatric Cleft Surgery: Role and Comparison with Ketorolac. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2011, 48, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Chang, B.L.; Wilson, A.J.; Chin, B.C.; Friedman, C.; Jackson, O.A. Influence of Standardized Orientation on Patient Perception of Perioperative Care Following Alveolar Cleft Repair: A Survey Based Study of Patients Treated in a Large Academic Medical Center. Cleft Palate. Craniofac. J. 2017, 54, 287–294. [Google Scholar] [CrossRef]
- Tache, A.; Mommaerts, M.Y. Pain Management at Iliac Donor Sites after Grafting of Alveolar Clefts. Int. J. Oral Maxillofac. Surg. 2021. [Google Scholar] [CrossRef]
- Liang, F.; Leland, H.; Jedrzejewski, B.; Auslander, A.; Maniskas, S.; Swanson, J.; Urata, M.; Hammoudeh, J.; Magee, W.I. Alternatives to Autologous Bone Graft in Alveolar Cleft Reconstruction: The State of Alveolar Tissue Engineering. J. Craniofac. Surg. 2018, 29, 584–593. [Google Scholar] [CrossRef]
- Wu, C.; Pan, W.; Feng, C.; Su, Z.; Duan, Z.; Zheng, Q.; Hua, C.; Li, C. Grafting Materials for Alveolar Cleft Reconstruction: A Systematic Review and Best-Evidence Synthesis. Int. J. Oral Maxillofac. Surg. 2018, 47, 345–356. [Google Scholar] [CrossRef]
- Osorio, C.C.; Escobar, L.M.; González, M.C.; Gamboa, L.F.; Chambrone, L. Evaluation of Density, Volume, Height and Rate of Bone Resorption of Substitutes of Autologous Bone Grafts for the Repair of Alveolar Clefts in Humans: A Systematic Review. Heliyon 2020, 6, e04646. [Google Scholar] [CrossRef] [PubMed]
- Ilharreborde, B.; Morel, E.; Fitoussi, F.; Presedo, A.; Souchet, P.; Penneçot, G.-F.; Mazda, K. Bioactive Glass as a Bone Substitute for Spinal Fusion in Adolescent Idiopathic Scoliosis: A Comparative Study With Iliac Crest Autograft. J. Pediatr. Orthop. 2008, 28, 347–351. [Google Scholar] [CrossRef] [Green Version]
- Syvänen, J.; Nietosvaara, Y.; Kohonen, I.; Koskimies, E.; Haara, M.; Korhonen, J.; Pajulo, O.; Helenius, I. Treatment of Aneurysmal Bone Cysts with Bioactive Glass in Children. Scand. J. Surg. SJS Off. Organ Finn. Surg. Soc. Scand. Surg. Soc. 2018, 107, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Välimäki, V.-V.; Aro, H.T. Molecular Basis for Action of Bioactive Glasses as Bone Graft Substitute. Scand. J. Surg. 2006, 95, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Hench, L.L.; Splinter, R.J.; Allen, W.C.; Greenlee, T.K. Bonding Mechanisms at the Interface of Ceramic Prosthetic Materials. J. Biomed. Mater. Res. 1971, 5, 117–141. [Google Scholar] [CrossRef]
- Hench, L.L. The Story of Bioglass®. J. Mater. Sci. Mater. Med. 2006, 17, 967–978. [Google Scholar] [CrossRef] [PubMed]
- Rahaman, M.N.; Day, D.E.; Bal, B.S.; Fu, Q.; Jung, S.B.; Bonewald, L.F.; Tomsia, A.P. Bioactive Glass in Tissue Engineering. Acta Biomater. 2011, 7, 2355–2373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehatlaf, A.A.; Farid, S.B.H.; Atiyah, A.A. Synthesis and Characterisation of Bioactive Glass 13-93 Scaffolds for Bone Tissue Regeneration. IOP Conf. Ser. Mater. Sci. Eng. 2021, 1067, 012136. [Google Scholar] [CrossRef]
- Drago, L.; De Vecchi, E.; Bortolin, M.; Toscano, M.; Mattina, R.; Romanò, C.L. Antimicrobial Activity and Resistance Selection of Different Bioglass S53P4 Formulations against Multidrug Resistant Strains. Future Microbiol. 2015, 10, 1293–1299. [Google Scholar] [CrossRef] [PubMed]
- Schott Guide to Glass; Pfaender, H.G. (Ed.) Springer: Dordrecht, The Netherlands, 1996; ISBN 978-94-010-9765-9. [Google Scholar]
- Sawangboon, N.; Nizamutdinova, A.; Uesbeck, T.; Limbach, R.; Meechoowas, E.; Tapasa, K.; Möncke, D.; Wondraczek, L.; Kamitsos, E.I.; van Wüllen, L.; et al. Modification of Silicophosphate Glass Composition, Structure, and Properties via Crucible Material and Melting Conditions. Int. J. Appl. Glass Sci. 2020, 11, 46–57. [Google Scholar] [CrossRef]
- Kaur, G.; Pickrell, G.; Sriranganathan, N.; Kumar, V.; Homa, D. Review and the State of the Art: Sol-Gel and Melt Quenched Bioactive Glasses for Tissue Engineering. J. Biomed. Mater. Res. B Appl. Biomater. 2016, 104, 1248–1275. [Google Scholar] [CrossRef] [PubMed]
- Kaur, A.; Khanna, A.; Kaur, A.; Hirdesh; Gonzàlez-Barriuso, M.; Gonzàlez, F. Effects of Annealing on Density, Glass Transition Temperature and Structure of Tellurite, Silicate and Borate Glasses. J. Non-Cryst. Solids 2018, 500, 443–452. [Google Scholar] [CrossRef]
- Baino, F.; Fiume, E.; Miola, M.; Verné, E. Bioactive Sol-Gel Glasses: Processing, Properties, and Applications. Int. J. Appl. Ceram. Technol. 2018, 15, 841–860. [Google Scholar] [CrossRef]
- Fiume, E.; Migneco, C.; Verné, E.; Baino, F. Comparison Between Bioactive Sol-Gel and Melt-Derived Glasses/Glass-Ceramics Based on the Multicomponent SiO2-P2O5-CaO-MgO-Na2O-K2O System. Materials 2020, 13, 540. [Google Scholar] [CrossRef] [Green Version]
- Zheng, K.; Boccaccini, A.R. Sol-Gel Processing of Bioactive Glass Nanoparticles: A Review. Adv. Colloid Interface Sci. 2017, 249, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Greasley, S.L.; Page, S.J.; Sirovica, S.; Chen, S.; Martin, R.A.; Riveiro, A.; Hanna, J.V.; Porter, A.E.; Jones, J.R. Controlling Particle Size in the Stöber Process and Incorporation of Calcium. J. Colloid Interface Sci. 2016, 469, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Xie, Y.; Li, A.; Shen, H.; Wu, D.; Qiu, D. Bioactive Nanoparticle through Postmodification of Colloidal Silica. ACS Appl. Mater. Interfaces 2014, 6, 4935–4939. [Google Scholar] [CrossRef] [PubMed]
- Liang, Q.; Hu, Q.; Miao, G.; Yuan, B.; Chen, X. A Facile Synthesis of Novel Mesoporous Bioactive Glass Nanoparticles with Various Morphologies and Tunable Mesostructure by Sacrificial Liquid Template Method. Mater. Lett. 2015, 148, 45–49. [Google Scholar] [CrossRef]
- Yun, H.; Kim, S.; Lee, S.; Song, I. Synthesis of High Surface Area Mesoporous Bioactive Glass Nanospheres. Mater. Lett. 2010, 64, 1850–1853. [Google Scholar] [CrossRef]
- Arcos, D.; López-Noriega, A.; Ruiz-Hernández, E.; Terasaki, O.; Vallet-Regí, M. Ordered Mesoporous Microspheres for Bone Grafting and Drug Delivery. Chem. Mater. 2009, 21, 1000–1009. [Google Scholar] [CrossRef]
- Li, X.; Chen, X.; Miao, G.; Liu, H.; Mao, C.; Yuan, G.; Liang, Q.; Shen, X.; Ning, C.; Fu, X. Synthesis of Radial Mesoporous Bioactive Glass Particles to Deliver Osteoactivin Gene. J. Mater. Chem. B 2014, 2, 7045–7054. [Google Scholar] [CrossRef] [PubMed]
- Sanders, D.M.; Hench, L.L. Mechanisms of Glass Corrosion. J. Am. Ceram. Soc. 1973, 56, 373–377. [Google Scholar] [CrossRef]
- Jones, J.R. Review of Bioactive Glass: From Hench to Hybrids. Acta Biomater. 2013, 9, 4457–4486. [Google Scholar] [CrossRef] [PubMed]
- Hench, L.L.; Polak, J.M. Third-Generation Biomedical Materials. Science 2002, 295, 1014–1017. [Google Scholar] [CrossRef] [Green Version]
- Juturu, V.; Wu, J.C. Microbial Production of Lactic Acid: The Latest Development. Crit. Rev. Biotechnol. 2016, 36, 967–977. [Google Scholar] [CrossRef] [PubMed]
- Nduko, J.M.; Taguchi, S. Microbial Production of Biodegradable Lactate-Based Polymers and Oligomeric Building Blocks From Renewable and Waste Resources. Front. Bioeng. Biotechnol. 2021, 8, 1548. [Google Scholar] [CrossRef] [PubMed]
- Snežana, I.-S.; Nikolić, L.; Vesna, N.; Ilić, D.; Ristić, I.S.; Tačić, A. Polymeric Matrix Systems for Drug Delivery. In Drug Delivery Approaches and Nanosystems; Apple Academic Press: Oakville, ON, Canada, 2017; ISBN 978-1-315-22537-1. [Google Scholar]
- Gupta, B.; Revagade, N.; Hilborn, J. Poly(Lactic Acid) Fiber: An Overview. Prog. Polym. Sci. 2007, 32, 455–482. [Google Scholar] [CrossRef]
- Benicewicz, B.C.; Hopper, P.K. Review: Polymers for Absorbable Surgical Sutures—Part I. J. Bioact. Compat. Polym. 1990, 5, 453–472. [Google Scholar] [CrossRef]
- Langer, R.; Peppas, N. Chemical and Physical Structure of Polymers as Carriers for Controlled Release of Bioactive Agents: A Review. J. Macromol. Sci. Part C 1983, 23, 61–126. [Google Scholar] [CrossRef]
- DeJong, L.E.S.; DeBerardino, L.T.M.; Brooks, D.E.; Judson, K. In Vivo Comparison of a Metal versus a Biodegradable Suture Anchor1 1Implants and Implant Instrumentation for This Project Were Provided via Material Transfer Agreement by Arthrex, Naples, Florida, U.S.A. Arthrosc. J. Arthrosc. Relat. Surg. 2004, 20, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Farah, S.; Anderson, D.G.; Langer, R. Physical and Mechanical Properties of PLA, and Their Functions in Widespread Applications—A Comprehensive Review. Adv. Drug Deliv. Rev. 2016, 107, 367–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naseem, R.; Tzivelekis, C.; German, M.J.; Gentile, P.; Ferreira, A.M.; Dalgarno, K. Strategies for Enhancing Polyester-Based Materials for Bone Fixation Applications. Molecules 2021, 26, 992. [Google Scholar] [CrossRef]
- Ajioka, M.; Enomoto, K.; Suzuki, K.; Yamaguchi, A. The Basic Properties of Poly(Lactic Acid) Produced by the Direct Condensation Polymerization of Lactic Acid. J. Environ. Polym. Degrad. 1995, 3, 225–234. [Google Scholar] [CrossRef]
- Kimura, Y. Molecular, Structural, and Material Design of Bio-Based Polymers. Polym. J. 2009, 41, 797–807. [Google Scholar] [CrossRef]
- Dorgan, J.R.; Lehermeier, H.; Mang, M. Thermal and Rheological Properties of Commercial-Grade Poly(Lactic Acid)s. J. Polym. Environ. 2000, 8, 1–9. [Google Scholar] [CrossRef]
- Lee, B.K.; Yun, Y.; Park, K. PLA Micro- and Nano-Particles. Adv. Drug Deliv. Rev. 2016, 107, 176–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valente, T.A.M.; Silva, D.M.; Gomes, P.S.; Fernandes, M.H.; Santos, J.D.; Sencadas, V. Effect of Sterilization Methods on Electrospun Poly(Lactic Acid) (PLA) Fiber Alignment for Biomedical Applications. ACS Appl. Mater. Interfaces 2016, 8, 3241–3249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savaris, M.; dos Santos, V.; Brandalise, R.N. Influence of Different Sterilization Processes on the Properties of Commercial Poly(Lactic Acid). Mater. Sci. Eng. C 2016, 69, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Jiang, M.; Zhou, Z.; Gou, J.; Hui, D. 3D Printing of Polymer Matrix Composites: A Review and Prospective. Compos. Part B Eng. 2017, 110, 442–458. [Google Scholar] [CrossRef]
- Carcreff, J.; Cheviré, F.; Galdo, E.; Lebullenger, R.; Gautier, A.; Adam, J.-L.; Coq, D.L.; Brilland, L.; Chahal, R.; Renversez, G.; et al. Elaboration of Chalcogenide Microstructured Optical Fibers Preform by 3D Additive Manufacturing. In Proceedings of the Optical Components and Materials XVIII, online, 5 March 2021; SPIE: Bellingham, WA, USA, 2021; Volume 11682, pp. 66–73. [Google Scholar]
- Baudet, E.; Ledemi, Y.; Larochelle, P.; Morency, S.; Messaddeq, Y. 3D-Printing of Arsenic Sulfide Chalcogenide Glasses. Opt. Mater. Express 2019, 9, 2307–2317. [Google Scholar] [CrossRef]
- Zaki, R.M.; Strutynski, C.; Kaser, S.; Bernard, D.; Hauss, G.; Faessel, M.; Sabatier, J.; Canioni, L.; Messaddeq, Y.; Danto, S.; et al. Direct 3D-Printing of Phosphate Glass by Fused Deposition Modeling. Mater. Des. 2020, 194, 108957. [Google Scholar] [CrossRef]
- Liu, C.; Qian, B.; Liu, X.; Tong, L.; Qiu, J. Additive Manufacturing of Silica Glass Using Laser Stereolithography with a Top-down Approach and Fast Debinding. RSC Adv. 2018, 8, 16344–16348. [Google Scholar] [CrossRef] [Green Version]
- Fateri, M.; Gebhardt, A. Selective Laser Melting of Soda-Lime Glass Powder. Int. J. Appl. Ceram. Technol. 2015, 12, 53–61. [Google Scholar] [CrossRef]
- Elomaa, L.; Kokkari, A.; Närhi, T.; Seppälä, J.V. Porous 3D Modeled Scaffolds of Bioactive Glass and Photocrosslinkable Poly(ε-Caprolactone) by Stereolithography. Compos. Sci. Technol. 2013, 74, 99–106. [Google Scholar] [CrossRef]
- Tan, K.H.; Chua, C.K.; Leong, K.F.; Cheah, C.M.; Cheang, P.; Abu Bakar, M.S.; Cha, S.W. Scaffold Development Using Selective Laser Sintering of Polyetheretherketone–Hydroxyapatite Biocomposite Blends. Biomaterials 2003, 24, 3115–3123. [Google Scholar] [CrossRef]
- Song, P.; Zhou, C.; Fan, H.; Zhang, B.; Pei, X.; Fan, Y.; Jiang, Q.; Bao, R.; Yang, Q.; Dong, Z.; et al. Novel 3D Porous Biocomposite Scaffolds Fabricated by Fused Deposition Modeling and Gas Foaming Combined Technology. Compos. Part B Eng. 2018, 152, 151–159. [Google Scholar] [CrossRef]
- Babilotte, J.; Guduric, V.; Le Nihouannen, D.; Naveau, A.; Fricain, J.-C.; Catros, S. 3D Printed Polymer–Mineral Composite Biomaterials for Bone Tissue Engineering: Fabrication and Characterization. J. Biomed. Mater. Res. B Appl. Biomater. 2019, 107, 2579–2595. [Google Scholar] [CrossRef]
- Coolen, A.-L.; Lacroix, C.; Mercier-Gouy, P.; Delaune, E.; Monge, C.; Exposito, J.-Y.; Verrier, B. Poly(Lactic Acid) Nanoparticles and Cell-Penetrating Peptide Potentiate MRNA-Based Vaccine Expression in Dendritic Cells Triggering Their Activation. Biomaterials 2019, 195, 23–37. [Google Scholar] [CrossRef]
- Jaidev, L.R.; Chatterjee, K. Surface Functionalization of 3D Printed Polymer Scaffolds to Augment Stem Cell Response. Mater. Des. 2019, 161, 44–54. [Google Scholar] [CrossRef]
- Pavia, F.C.; La Carrubba, V.; Ghersi, G.; Brucato, V. Poly-Left-Lactic Acid Tubular Scaffolds via Diffusion Induced Phase Separation: Control of Morphology. Polym. Eng. Sci. 2013, 53, 431–442. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Wu, P.; Feng, P.; Guo, W.; Yang, W.; Shuai, C. Interfacial Reinforcement in a Poly-l-Lactic Acid/Mesoporous Bioactive Glass Scaffold via Polydopamine. Colloids Surf. B Biointerfaces 2018, 170, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Goh, Y.; Akram, M.; Alshemary, A.; Hussain, R. Antibacterial Polylactic Acid/Chitosan Nanofibers Decorated with Bioactive Glass. Appl. Surf. Sci. 2016, 387, 1–7. [Google Scholar] [CrossRef]
- Blaker, J.J.; Gough, J.E.; Maquet, V.; Notingher, I.; Boccaccini, A.R. In Vitro Evaluation of Novel Bioactive Composites Based on Bioglass-Filled Polylactide Foams for Bone Tissue Engineering Scaffolds. J. Biomed. Mater. Res. A 2003, 67, 1401–1411. [Google Scholar] [CrossRef] [PubMed]
- Verrier, S.; Blaker, J.J.; Maquet, V.; Hench, L.L.; Boccaccini, A.R. PDLLA/Bioglass Composites for Soft-Tissue and Hard-Tissue Engineering: An in Vitro Cell Biology Assessment. Biomaterials 2004, 25, 3013–3021. [Google Scholar] [CrossRef] [PubMed]
- Blaker, J.J.; Nazhat, S.N.; Maquet, V.; Boccaccini, A.R. Long-Term in Vitro Degradation of PDLLA/Bioglass Bone Scaffolds in Acellular Simulated Body Fluid. Acta Biomater. 2011, 7, 829–840. [Google Scholar] [CrossRef]
- Maquet, V.; Boccaccini, A.R.; Pravata, L.; Notingher, I.; Jérôme, R. Preparation, Characterization, and in Vitro Degradation of Bioresorbable and Bioactive Composites Based on Bioglass-Filled Polylactide Foams. J. Biomed. Mater. Res. A 2003, 66, 335–346. [Google Scholar] [CrossRef]
- Yang, X.B.; Webb, D.; Blaker, J.; Boccaccini, A.R.; Maquet, V.; Cooper, C.; Oreffo, R.O.C. Evaluation of Human Bone Marrow Stromal Cell Growth on Biodegradable Polymer/Bioglass® Composites. Biochem. Biophys. Res. Commun. 2006, 342, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Kazarian, S.G.; Chan, K.L.A.; Maquet, V.; Boccaccini, A.R. Characterisation of Bioactive and Resorbable Polylactide/Bioglass Composites by FTIR Spectroscopic Imaging. Biomaterials 2004, 25, 3931–3938. [Google Scholar] [CrossRef]
- Zhang, K.; Wang, Y.; Hillmyer, M.A.; Francis, L.F. Processing and Properties of Porous Poly(l-Lactide)/Bioactive Glass Composites. Biomaterials 2004, 25, 2489–2500. [Google Scholar] [CrossRef]
- Pagac, M.; Hajnys, J.; Ma, Q.-P.; Jancar, L.; Jansa, J.; Stefek, P.; Mesicek, J. A Review of Vat Photopolymerization Technology: Materials, Applications, Challenges, and Future Trends of 3D Printing. Polymers 2021, 13, 598. [Google Scholar] [CrossRef]
- Ronca, A.; Ambrosio, L.; Grijpma, D.W. Preparation of Designed Poly(d,l-Lactide)/Nanosized Hydroxyapatite Composite Structures by Stereolithography. Acta Biomater. 2013, 9, 5989–5996. [Google Scholar] [CrossRef]
- Melchels, F.P.W.; Feijen, J.; Grijpma, D.W. A Poly(d,l-Lactide) Resin for the Preparation of Tissue Engineering Scaffolds by Stereolithography. Biomaterials 2009, 30, 3801–3809. [Google Scholar] [CrossRef] [Green Version]
- Seck, T.M.; Melchels, F.P.W.; Feijen, J.; Grijpma, D.W. Designed Biodegradable Hydrogel Structures Prepared by Stereolithography Using Poly(Ethylene Glycol)/Poly(D,L-Lactide)-Based Resins. J. Control. Release Off. J. Control. Release Soc. 2010, 148, 34–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcaute, K.; Mann, B.K.; Wicker, R.B. Stereolithography of Three-Dimensional Bioactive Poly(Ethylene Glycol) Constructs with Encapsulated Cells. Ann. Biomed. Eng. 2006, 34, 1429–1441. [Google Scholar] [CrossRef]
- Sun, S.; Brandt, M.; Easton, M. 2-Powder bed fusion processes: An overview. In Laser Additive Manufacturing; Brandt, M., Ed.; Woodhead Publishing Series in Electronic and Optical Materials; Woodhead Publishing: Sawston, UK, 2017; pp. 55–77. ISBN 978-0-08-100433-3. [Google Scholar]
- Shishkovsky, I.; Morozov, Y.; Smurov, I. Nanofractal Surface Structure under Laser Sintering of Titanium and Nitinol for Bone Tissue Engineering. Appl. Surf. Sci. 2007, 254, 1145–1149. [Google Scholar] [CrossRef]
- Loh, Q.L.; Choong, C. Three-Dimensional Scaffolds for Tissue Engineering Applications: Role of Porosity and Pore Size. Tissue Eng. Part B Rev. 2013, 19, 485–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, J.M.; Adewunmi, A.; Schek, R.M.; Flanagan, C.L.; Krebsbach, P.H.; Feinberg, S.E.; Hollister, S.J.; Das, S. Bone Tissue Engineering Using Polycaprolactone Scaffolds Fabricated via Selective Laser Sintering. Biomaterials 2005, 26, 4817–4827. [Google Scholar] [CrossRef]
- Gayer, C.; Ritter, J.; Bullemer, M.; Grom, S.; Jauer, L.; Meiners, W.; Pfister, A.; Reinauer, F.; Vučak, M.; Wissenbach, K.; et al. Development of a Solvent-Free Polylactide/Calcium Carbonate Composite for Selective Laser Sintering of Bone Tissue Engineering Scaffolds. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 101, 660–673. [Google Scholar] [CrossRef] [PubMed]
- Duan, B.; Wang, M.; Zhou, W.Y.; Cheung, W.L.; Li, Z.Y.; Lu, W.W. Three-Dimensional Nanocomposite Scaffolds Fabricated via Selective Laser Sintering for Bone Tissue Engineering. Acta Biomater. 2010, 6, 4495–4505. [Google Scholar] [CrossRef]
- Simpson, R.L.; Wiria, F.E.; Amis, A.A.; Chua, C.K.; Leong, K.F.; Hansen, U.N.; Chandrasekaran, M.; Lee, M.W. Development of a 95/5 Poly(L-Lactide-Co-Glycolide)/Hydroxylapatite and Beta-Tricalcium Phosphate Scaffold as Bone Replacement Material via Selective Laser Sintering. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 84, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Turner, B.N.; Strong, R.; Gold, S.A. A Review of Melt Extrusion Additive Manufacturing Processes: I. Process Design and Modeling. Rapid Prototyp. J. 2014, 20, 192–204. [Google Scholar] [CrossRef]
- Chiulan, I.; Frone, A.N.; Brandabur, C.; Panaitescu, D.M. Recent Advances in 3D Printing of Aliphatic Polyesters. Bioengineering 2017, 5, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Yang, G.; Johnson, B.N.; Jia, X. Three-Dimensional (3D) Printed Scaffold and Material Selection for Bone Repair. Acta Biomater. 2019, 84, 16–33. [Google Scholar] [CrossRef] [PubMed]
- Lobo, D.A.; Ginestra, P. Cell Bioprinting: The 3D-BioplotterTM Case. Materials 2019, 12, 4005. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.-J.; Ren, J.-A.; Wang, G.-F.; Li, Z.-A.; Wu, X.-W.; Ren, H.-J.; Liu, S. 3D-Printed “Fistula Stent” Designed for Management of Enterocutaneous Fistula: An Advanced Strategy. World J. Gastroenterol. 2017, 23, 7489–7494. [Google Scholar] [CrossRef]
- Horváth, L.; Umehara, Y.; Jud, C.; Blank, F.; Petri-Fink, A.; Rothen-Rutishauser, B. Engineering an In Vitro Air-Blood Barrier by 3D Bioprinting. Sci. Rep. 2015, 5, 7974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knowlton, S.; Onal, S.; Yu, C.H.; Zhao, J.J.; Tasoglu, S. Bioprinting for Cancer Research. Trends Biotechnol. 2015, 33, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Pati, F.; Jang, J.; Ha, D.-H.; Won Kim, S.; Rhie, J.-W.; Shim, J.-H.; Kim, D.-H.; Cho, D.-W. Printing Three-Dimensional Tissue Analogues with Decellularized Extracellular Matrix Bioink. Nat. Commun. 2014, 5, 3935. [Google Scholar] [CrossRef] [Green Version]
- Skoog, S.A.; Goering, P.L.; Narayan, R.J. Stereolithography in Tissue Engineering. J. Mater. Sci. Mater. Med. 2014, 25, 845–856. [Google Scholar] [CrossRef]
- Liu, Z.; Ge, Y.; Zhang, L.; Wang, Y.; Guo, C.; Feng, K.; Yang, S.; Zhai, Z.; Chi, Y.; Zhao, J.; et al. The Effect of Induced Membranes Combined with Enhanced Bone Marrow and 3D PLA-HA on Repairing Long Bone Defects in Vivo. J. Tissue Eng. Regen. Med. 2020, 14, 1403–1414. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Yassin, M.A.; Fuoco, T.; Liu, H.; Mohamed-Ahmed, S.; Mustafa, K.; Finne-Wistrand, A. Engineering 3D Degradable, Pliable Scaffolds toward Adipose Tissue Regeneration; Optimized Printability, Simulations and Surface Modification. J. Tissue Eng. 2020, 11, 2041731420954316. [Google Scholar] [CrossRef] [PubMed]
- Vallejos, R.; Contreras, J.; Aiyangar, A.; Palza, H.; Vivanco, J.F. Effect of 45s5 Bioglass on the Mechanical and Biological Performance of 3d-Printed Pcl Scaffolds. Orthop. Proc. 2020, 102-B, 118. [Google Scholar] [CrossRef]
- El-Rashidy, A.A.; Roether, J.A.; Harhaus, L.; Kneser, U.; Boccaccini, A.R. Regenerating Bone with Bioactive Glass Scaffolds: A Review of in Vivo Studies in Bone Defect Models. Acta Biomater. 2017, 62, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Lancellotta, V.; Pagano, S.; Tagliaferri, L.; Piergentini, M.; Ricci, A.; Montecchiani, S.; Saldi, S.; Chierchini, S.; Cianetti, S.; Valentini, V.; et al. Individual 3-Dimensional Printed Mold for Treating Hard Palate Carcinoma with Brachytherapy: A Clinical Report. J. Prosthet. Dent. 2019, 121, 690–693. [Google Scholar] [CrossRef] [PubMed]
- López-Torres, I.I.; Sanz-Ruíz, P.; León-Román, V.E.; Navarro-García, F.; Priego-Sánchez, R.; Vaquero-Martín, J. 3D Printing in Experimental Orthopaedic Surgery: Do It Yourself. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 967–973. [Google Scholar] [CrossRef]
- Moser, N.; Santander, P.; Quast, A. From 3D Imaging to 3D Printing in Dentistry—A Practical Guide. Int. J. Comput. Dent. 2018, 21, 345–356. [Google Scholar] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brézulier, D.; Chaigneau, L.; Jeanne, S.; Lebullenger, R. The Challenge of 3D Bioprinting of Composite Natural Polymers PLA/Bioglass: Trends and Benefits in Cleft Palate Surgery. Biomedicines 2021, 9, 1553. https://doi.org/10.3390/biomedicines9111553
Brézulier D, Chaigneau L, Jeanne S, Lebullenger R. The Challenge of 3D Bioprinting of Composite Natural Polymers PLA/Bioglass: Trends and Benefits in Cleft Palate Surgery. Biomedicines. 2021; 9(11):1553. https://doi.org/10.3390/biomedicines9111553
Chicago/Turabian StyleBrézulier, Damien, Louis Chaigneau, Sylvie Jeanne, and Ronan Lebullenger. 2021. "The Challenge of 3D Bioprinting of Composite Natural Polymers PLA/Bioglass: Trends and Benefits in Cleft Palate Surgery" Biomedicines 9, no. 11: 1553. https://doi.org/10.3390/biomedicines9111553
APA StyleBrézulier, D., Chaigneau, L., Jeanne, S., & Lebullenger, R. (2021). The Challenge of 3D Bioprinting of Composite Natural Polymers PLA/Bioglass: Trends and Benefits in Cleft Palate Surgery. Biomedicines, 9(11), 1553. https://doi.org/10.3390/biomedicines9111553