
Somatostatin and Somatostatin Receptors: From Signaling to Clinical Applications in Neuroendocrine Neoplasms

 , ,
, ,  , and
, and
Abstract
:1. Introduction
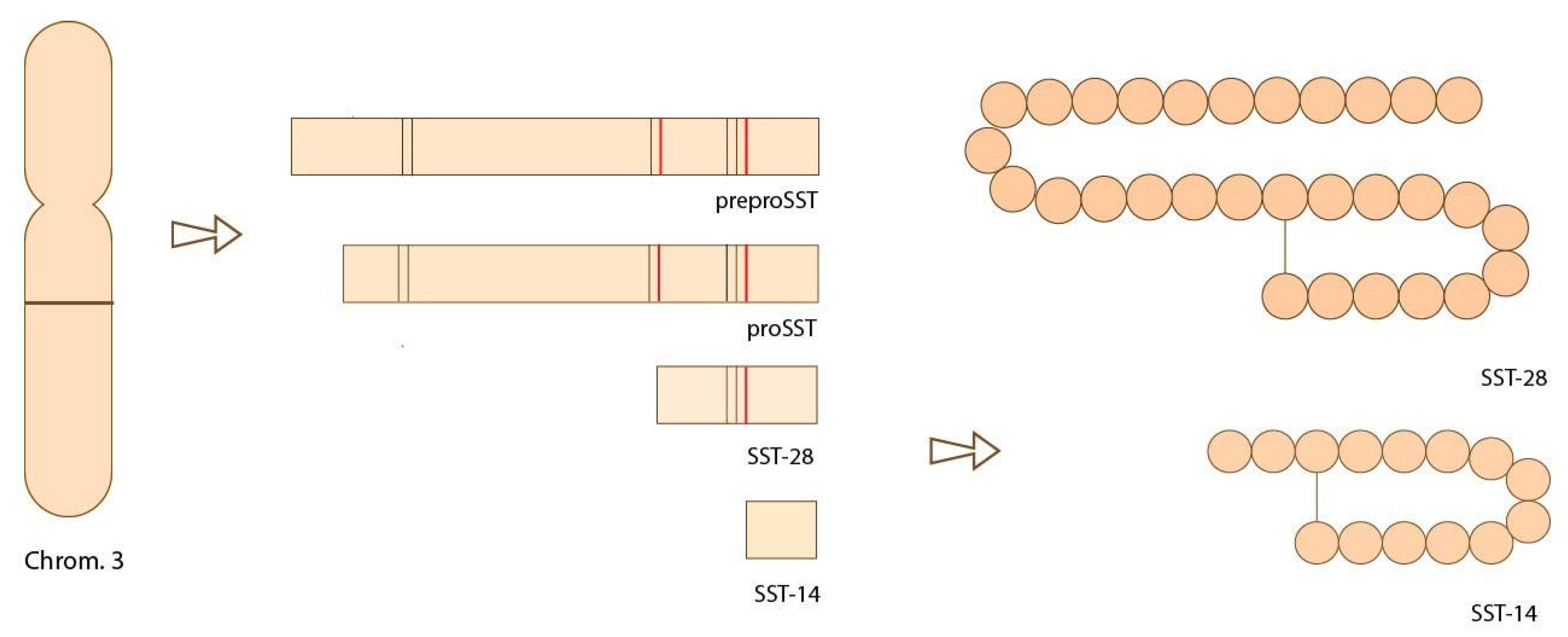
2. Somatostatin and Somatostatin Receptors
3. Somatostatin Receptors as Targets for Imaging Diagnosis on Neuroendocrine Neoplasms
4. Somatostatin Analogues as Treatment for NENs
5. Peptide Receptor Radionuclide Therapy
6. Future Use of Alfa-Emmitters Binded to Somatostatin Antagonists
7. Future of the Use of Somatostatin Receptors as Targets on Neuroendocrine Tumors: Somatostatin Antagonists
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Harris, C.; Baeg, K.J.; Aronson, A.; Wisnivesky, J.P.; Kim, M.K. Incidence Trends of Gastroenteropancreatic Neuroendocrine Tumors in the United States. Clin. Gastroenterol. Hepatol. 2019, 17, 2212–2217.e1. [Google Scholar] [CrossRef] [Green Version]
- WHO. Classification of Tumours Editorial Board, 5th ed.; WHO Classification of Tumours Series; WHO: Geneva, Switzerland, 2019; Volume 1. [Google Scholar]
- Günther, T.; Tulipano, G.; Dournaud, P.; Bousquet, C.; Csaba, Z.; Kreienkamp, H.J.; Lupp, A.; Korbonits, M.; Castaño, J.P.; Wester, H.J.; et al. International Union of Basic and Clinical Pharmacology. CV. Somatostatin Receptors: Structure, Function, Ligands, and New Nomenclature. Pharmacol. Rev. 2018, 70, 763–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, L.P.; Rutter, W.J. Sequence of the human somatostatin I gene. Science 1984, 224, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Cakir, M.; Dworakowska, D.; Grossman, A. Somatostatin receptor biology in neuroendocrine and pituitary tumours: Part 1—Molecular pathways. J. Cell. Mol. Med. 2010, 14, 2570–2584. [Google Scholar] [CrossRef] [Green Version]
- Theodoropoulou, M.; Stalla, G.K. Somatostatin receptors: From signaling to clinical practice. Front. Neuroendocrinol. 2013, 34, 228–252. [Google Scholar] [CrossRef] [PubMed]
- Strowski, M.Z.; Blake, A.D. Function and expression of somatostatin receptors of the endocrine pancreas. Mol. Cell. Endocrinol. 2008, 286, 169–179. [Google Scholar] [CrossRef] [Green Version]
- Messchendorp, A.L.; Spithoven, E.M.; Casteleijn, N.F.; Dam, W.A.; van den Born, J.; Tonnis, W.F.; Gaillard, C.A.J.M.; Meijer, E.; DIPAK Consortium. Association of plasma somatostatin with disease severity and progression in patients with autosomal dominant polycystic kidney disease. BMC Nephrol. 2018, 19, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Encyclopædia Britannica, Inc. Hormones Secreted by the Glands of the Endocrine System Are Carried in the Bloodstream. Available online: https://www.britannica.com/video/72950/Hormones-glands-endocrine-system-target-cells-bloodstream (accessed on 20 October 2021).
- Gatto, F. Biological and Biochemical Basis of the Differential Efficacy of First and Second Generation Somatostatin Receptor Ligands in Neuroendocrine Neoplasms. Int. J. Mol. Sci. 2019, 20, 3940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krenning, E.P.; Bakker, W.H.; Breeman, W.A.; Koper, J.W.; Kooij, P.P.; Ausema, L.; Lameris, J.S.; Reubi, J.C.; Lamberts, S.W. Localisation of endocrine-related tumours with radioiodinated analogue of somatostatin. Lancet 1989, 1, 242–244. [Google Scholar] [CrossRef]
- Bombardieri, E.; Coliva, A.; Maccauro, M.; Seregni, E.; Orunesu, E.; Chiti, A.; Lucignani, G. Imaging of neuroendocrine tumours with gamma-emitting radiopharmaceuticals. Quart. J. Nucl. Med. Mol. Imag. 2010, 54, 3–15. [Google Scholar]
- Ambrosini, V.; Fani, M.; Fanti, S.; Forrer, F.; Maecke, H.R. Radiopeptide imaging and therapy in Europe. Eur. J. Nucl. Med. 2011, 52, 42–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artiko, V.; Afgan, A.; Petrović, J.; Radović, B.; Petrović, N.; Vlajković, M.; Šobić-Šaranović, D.; Obradović, V. Evaluation of neuroendocrine tumors with 99mTc-EDDA/HYNIC TOC. Nucl. Med. Rev. 2016, 19, 99–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutsikou, E.; Porpodis, K.; Chatzipavlidou, V.; Hardavella, G.; Gerasimou, G.; Domvri, K.; Papadopoulos, N.; Avramidou, V.; Spyratos, D.; Kontakiotis, T.; et al. Predictive Value of 99MTC-hynic-toc Scintigraphy in Lung Neuroendocrine Tumor Diagnosis. Technol. Cancer Res. Treat. 2019, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Yamaga, L.Y.; Neto, G.C.; da Cunha, M.L.; Osawa, A.; Silveira, J.C.; Fonseca, R.Q.; Nogueira, S.A.; Wagner, J.; Funari, M.G. 99mTc-HYNIC-TOC increased uptake can mimic malignancy in the pancreas uncinate process at somatostatin receptor SPECT/CT. Radiol. Med. 2016, 121, 225–228. [Google Scholar] [CrossRef]
- Garai, I.; Barna, S.; Nagy, G.; Forgacs, A. Limitations and pitfalls of 99mTc-EDDA/HYNIC-TOC (Tektrotyd) scintigraphy. Nucl. Med. Rev. 2016, 19, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Sergieva, S.; Robev, B.; Dimcheva, M.; Fakirova, A.; Hristoskova, R. Clinical application of SPECT-CT with 99mTc-Tektrotyd in bronchial and thymic neuroendocrine tumors (NETs). Nucl. Med. Rev. 2016, 19, 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briganti, V.; Cuccurullo, V.; Berti, V.; Di Stasio, G.D.; Linguanti, F.; Mungai, F.; Mansi, L. 99mTc-EDDA/HYNIC-TOC is a New Opportunity in Neuroendocrine Tumors of the Lung (and in other Malignant and Benign Pulmonary Diseases). Curr. Radiopharm. 2020, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- De Herder, W.W. Functional localisation and scintigraphy in neuroendocrine tumours of the gastrointestinal tract and pancreas (GEP-NETs). Eur. J. Endocrinol. 2014, 170, 173–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deppen, S.A.; Liu, E.; Blume, J.D.; Clanton, J.; Shi, C.; Jones-Jackson, L.B.; Lakhani, V.; Baum, R.P.; Berlin, J.; Smith, G.T.; et al. Safety and Efficacy of 68Ga-DOTATATE PET/CT for Diagnosis, Staging, and Treatment Management of Neuroendocrine Tumors. J. Nucl. Med. 2016, 57, 708–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geijer, H.; Breimer, L.H. Somatostatin receptor PET/CT in neuroendocrine tumours: Update on systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1770–1780. [Google Scholar] [CrossRef] [PubMed]
- Barrio, M.; Czernin, J.; Fanti, S.; Ambrosini, V.; Binse, I.; Du, L.; Eiber, M.; Herrmann, K.; Fendler, W.P. The Impact of Somatostatin Receptor–Directed PET/CT on the Management of Patients with Neuroendocrine Tumor: A Systematic Review and Meta-Analysis. J. Nucl. Med. 2017, 58, 756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Jensen, R.T. Molecular imaging in neuroendocrine tumors: Recent advances, controversies, unresolved issues, and roles in management. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 15–24. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.; Ito, T.; Jensen, R.T. Imaging of pancreatic neuroendocrine tumors: Recent advances, current status, and controversies. Expert Rev. Anticancer Ther. 2018, 18, 837–860. [Google Scholar] [CrossRef] [PubMed]
- Carideo, L.; Prosperi, D.; Panzuto, F.; Magi, L.; Pratesi, M.S.; Rinzivillo, M.; Annibale, B.; Signore, A. Role of Combined [68Ga]Ga-DOTA-SST Analogues and [18F]FDG PET/CT in the Management of GEP-NENs: A Systematic Review. JCM 2019, 8, 1032. [Google Scholar] [CrossRef] [Green Version]
- Merola, E.; Pavel, M.E.; Panzuto, F.; Capurso, G.; Cicchese, N.; Rinke, A.; Gress, T.M.; Iannicelli, E.; Prosperi, D.; Pizzichini, P.; et al. Functional Imaging in the Follow-Up of Enteropancreatic Neuroendocrine Tumors: Clinical Usefulness and Indications. J. Clin. Endocrinol. Metab. 2017, 102, 1486–1494. [Google Scholar] [CrossRef]
- Marazuela, M.; Bernabéu, I. Tratamiento farmacológico de los tumores neuroendocrinos gastroenteropancreaticos: Análogos de somatostatina. Endocrinol. Nutr. 2007, 54 (Suppl. S1), 44–50. [Google Scholar] [CrossRef]
- Gomes-Porras, M.; Cárdenas-salas, J.; Álvarez-Escolá, C. Somatostatin Analogs in Clinical Practice: A review. Int. J. Mol. Sci. 2020, 21, 1682. [Google Scholar] [CrossRef] [Green Version]
- Stueven, A.K.; Kayser, A.; Wetz, C.; Amthauer, A.W.; Wree, A.; Tacke, F.; Wiedenmann, B.; Roderburg, C.; Jann, H. Somatostatin Analogues in the Treatment of Neuroendocrine Tumors: Past, Present and Future. Int. J. Mol. Sci. 2019, 20, 3049. [Google Scholar] [CrossRef] [Green Version]
- Plöckinger, U.; Wiedenmann, B. Neuroendocrine Tumors. Biotherapy. Best Prac. Res. Clin. Endocrinol. Metab. 2007, 21, 145–162. [Google Scholar] [CrossRef]
- Keskin, O.; Yalcin, S. A review of the use of somatostatin analogs in oncology. Onco Targets Ther. 2013, 6, 471–483. [Google Scholar] [PubMed] [Green Version]
- Hofland, J.; Herrera-Martínez, A.D.; Zandee, W.T.; de Herder, W. Management of carcinoid syndrome: A systematic review and meta-analysis. Endocr. Relat. Cancer 2019, 26, R145–R156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cives, M.; Strosberg, J. The expanding role of somatostatin analogs in gastroenteropancreatic and lung neuroendocrine tumors. Drugs 2015, 75, 847–858. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.N.; Rashid, A.; et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plöckinger, U.; Wiedenmann, B. Treatment of gastroenteropancreatic neuroendocrine tumors. Virchows Arch. 2007, 451, 71–80. [Google Scholar] [CrossRef]
- Arnold, R.; Benning, R.; Neuhaus, C.; Rolwage, M.; Trautmann, M.E. Gastroenteropancreatic endocrine tumors: Effect of Sandostatin on tumor growth. The German Sandostatin Study Group. Metab. Clin. Exp. 1992, 41, 116–118. [Google Scholar] [CrossRef]
- Arnold, R.; Trautmann, M.E.; Creutzfeldt, W.; Benning, R.; Benning, M.; Neuhaus, C.; Jurgensen, R.; Stein, K.; Schafer, H.; Bruns, C.; et al. Somatostatin analogue octreotide and inhibition of tumour growth in metastatic endocrine gastroenteropancreatic tumours. Gut 1996, 38, 430–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ducreux, M.; Ruszniewski, P.; Chayvialle, J.A.; Blumberg, J.; Cloarec, D.; Michel, H.; Raymond, J.M.; Dupas, J.L.; Gouerou, H.; Jian, R.; et al. The antitumoral effect of the long-acting somatostatin analog lanreotide in neuroendocrine tumors. Am. J. Gastroenterol. 2000, 95, 3276–3281. [Google Scholar] [CrossRef] [PubMed]
- Wymenga, A.N.; Eriksson, B.; Salmela, P.I.; Jacobsen, M.B.; Van Cutsem, E.J.; Fiasse, R.H.; Valimaki, M.J.; Renstrup, J.; de Vries, E.G.; Oberg, K.E. Efficacy and safety of prolonged-release lanreotide in patients with gastrointestinal neuroendocrine tumors and hormone-related symptoms. J. Clin. Oncol. 1999, 17, 1111. [Google Scholar] [CrossRef] [PubMed]
- Rinke, A.; Müller, H.-H.; Schade-Brittinger, C.; Klose, K.-J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.-F.; Bläker, M.; et al. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors: A Report from the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef]
- Caplin, M.E.; Pavel, M.; Ćwikła, J.B.; Phan, A.T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Anti-tumour effects of lanreotide for pancreatic and intestinal neuroendocrine tumours: The CLARINET open-label extension study. Endocr. Relat. Cancer 2016, 23, 191–199. [Google Scholar] [CrossRef]
- NCT02683941, Efficacy and Safety of Lanreotide Autogel/Depot 120 mg vs. Placebo in Subjects With Lung Neuroendocrine Tumors (SPINET). 2016. Available online: http://clinicaltrials.gov/ct2/show/NCT02683941 (accessed on 25 October 2021).
- Chan, D.L.; Ferone, D.; Albertelli, M.; Pavlakis, N.; Segelov, E.; Singh, S. Escalated-dose somatostatin analogues for antiproliferative effect in GEPNETS: A systematic review. Endocrine 2017, 57, 366–375. [Google Scholar] [CrossRef]
- Pavel, M.; Ćwikła, J.B.; Lombard-Bohas, C.; Borbath, I.; Shah, T.; Pape, U.F.; Capdevila, J.; Panzuto, F.; Truong Thanh, X.M.; Houchard, A.; et al. Efficacy and safety of high-dose lanreotide autogel in patients with progressive pancreatic or midgut neuroendocrine tumours: CLARINET FORTE phase 2 study results. Eur. J. Cancer 2021, 157, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Cives, M.; Kunz, P.L.; Morse, B.; Coppola, D.; Schell, M.J.; Campos, T.; Nguyen, P.T.; Nandoskar, P.; Khandelwal, V.; Strosberg, J.R. Phase II clinical trial of pasireotide long-acting repeatable in patients with metastatic neuroendocrine tumors. Endocr. Relat. Cancer 2015, 22, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kulke, M.H.; Ruszniewski, P.; Van Cutsem, E.; Lombard-Bohas, C.; Valle, J.W.; De Herder, W.W.; Pavel, M.; Degtyarev, E.; Brase, J.C.; Bubuteishvili-Pacaud, L.; et al. A randomized, open-label, phase 2 study of everolimus in combination with pasireotide LAR or everolimus alone in advanced, well-differentiated, progressive pancreatic neuroendocrine tumors: COOPERATE-2 trial. Ann. Oncol. 2017, 28, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Ferolla, P.; Brizzi, M.P.; Meyer, T.; Mansoor, W.; Mazieres, J.; Do Cao, C.; Lena, H.; Berruti, A.; Damiano, V.; Buikhuisen, W.; et al. Efficacy and safety of long-acting pasireotide or everolimus alone or in combination in patients with advanced carcinoids of the lung and thymus (LUNA): An open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2017, 18, 1652–1664. [Google Scholar] [CrossRef]
- Eychenne, R.; Chèrel, M.; Haddad, F.; Guérard, F.; Gestin, J.F. Overview of the Most Promising Radionuclides for Targeted Alpha Therapy: The “Hopeful Eight”. Pharmaceutics 2021, 13, 906. [Google Scholar] [CrossRef]
- Werner, R.A.; Weich, A.; Kircher, M.; Solnes, L.B.; Javadi, M.S.; Higuchi, T.; Buck, A.K.; Pomper, M.G.; Rowe, S.P.; Lapa, C. The theranostic promise for neuroendocrine tumors in the late 2010s-Where do we stand, where do we go? Theranostics 2018, 8, 6088–6100. [Google Scholar] [CrossRef]
- Bodei, L.; Mueller-Brand, J.; Baum, R.P.; Pavel, M.E.; Hörsch, D.; O’Dorisio, O.M.; O’Dorisio, T.M.; Howe, J.R.; Cremonesi, M.; Kwekkeboom, D.J.; et al. The joint IAEA, EANM, and SNMMI practical guidance on peptide receptor radionuclide therapy (PRRNT) in neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 800–816. [Google Scholar] [CrossRef] [PubMed]
- Bodei, L.; Kwekkeboom, D.J.; Kidd, M.; Modlin, I.M.; Krenning, E.P. Radiolabeled somatostatin analogue therapy of gastroenteropancreatic cancer. Semin. Nucl. Med. 2016, 46, 225–238. [Google Scholar] [CrossRef]
- Kwekkeboom, D.; Bakker, W.; Kooij, P.; Konijnenberg, M.; Srinivasan, A.; Erion, J.L.; Schmidt, M.A.; Bugaj, J.L.; de Jong, M.; Krenning, E.P. [177Lu-DOTA0,Tyr3] octreotate: Comparison with [111In-DTPA0]octreotide in patients. Eur. J. Nucl. Med. 2001, 28, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Kwekkeboom, D.J.; de Herder, W.W.; Kam, B.L.; Srinivasan, A.; Erion, J.L.; Schmidt, M.A.; Bugaj, J.L.; de Jong, M.; Krenning, E.P. Treatment with the radiolabeled somatostatin analog [177Lu-DOTA0,Tyr3] octreotate: Toxicity, efficacy, and survival. J. Clin. Oncol. 2008, 26, 2124–2130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodei, L.; Cremonesi, M.; Grana, C.M.; Fazio, N.; Iodice, S.; Baio, S.M.; Bartolomei, M.; Lombardo, D.; Ferrari, M.E.; Sansovini, M.; et al. Peptide receptor radionuclide therapy with 177Lu-DOTATATE:The IEO phaseI-II study. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 2125–2135. [Google Scholar] [CrossRef] [PubMed]
- Sansovini, M.; Severi, S.; Ambrosetti, A.; Monti, M.; Nanni, O.; Sarnelli, A.; Bodei, L.; Garaboldi, L.; Bartolomei, M.; Paganelli, G. Treatment with the radiolabelled somatostatin analog Lu-DOTATATE for advanced pancreatic neuroendocrine tumors. Neuroendocrinology 2013, 97, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Paganelli, G.; Sansovini, M.; Ambrosetti, A.; Severi, S.; Monti, M.; Scarpi, E.; Donati, C.; Ianniello, A.; Matteucci, F.; Amadori, D. 177Lu-Dota-octreotate radionuclide therapy of advanced gastrointestinal neuroendocrine tumors: Results from a phase II study. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1845–1851. [Google Scholar] [CrossRef]
- Sabe, A.; Dautzenberg, K.; Haslerud, T.; Aouf, A.; Sabet, A.; Simon, B.; Mayer, K.; Biersack, H.J.; Ezziddin, S. Specific efficacy of peptide receptor radionuclide therapy with (177)Lu-octreotate in advanced neuroendocrine tumours of the small intestine. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1238–1246. [Google Scholar] [CrossRef] [PubMed]
- Delpassand, E.; Samarghandi, A.; Zamanian, S.; Wolin, E.M.; Hamiditabar, M.; Espenan, G.D.; Erion, J.L.; O’Dorisio, T.M.; Kvols, L.K.; Simon, J.; et al. Peptide receptor radionuclide therapy with 177Lu-DOTATATE for patients with somatostatin receptor-expressing neuroendocrine tumors: The first US phase 2 experience. Pancreas 2014, 43, 518–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.J.; Pak, K.; Koo, P.J.; Kwak, J.J.; Chang, S. The efficacy of 177 Lu-labelled peptide receptor radionuclide therapy in patients with neuroendocrine tumours: A meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1964–1970. [Google Scholar] [CrossRef] [PubMed]
- Brabander, T.; van der Zwan, W.; Teunissen, J.; Kam, B.L.R.; Feelders, R.A.; de Herder, W.W.; van Eijck, C.H.J.; Franssen, G.J.H.; Krenning, E.P.; Kwekkeboom, D.J. Long-Term Efficacy, Survival, and Safety of [ 177 Lu-DOTA 0,Tyr 3]octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors. Clin. Cancer Res. 2017, 23, 4617–4624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baum, R.; Kulkarni, H.; Singh, A.; Kaemmerer, D.; Mueller, D.; Prasad, V.; Hommann, M.; Robiller, F.C.; Niepsch, K.; Franz, H.; et al. Results and adverse events of personalized peptide receptor radionuclide therapy with 90 Yttrium and 177 Lutetium in 1048 patients with neuroendocrine neoplasms. Oncotarget 2018, 9, 16932–16950. [Google Scholar] [CrossRef] [Green Version]
- Sward, C.; Bernhardt, P.; Ahlman, H.; Wangberg, B.; Forssell-Aronsson, E.; Larsson, M.; Svensson, J.; Rossi-Norrlund, R.; Kolby, L. [177Lu-DOTA 0-Tyr 3]-octreotate treatment in patients with disseminated gastroenteropancreatic neuroendocrine tumors: The value of measuring absorbed dose to the kidney. World J. Surg. 2010, 34, 1368–1372. [Google Scholar] [CrossRef] [PubMed]
- Van Vliet, E.I.; Krenning, E.P.; Teunissen, J.J.; Bergsma, H.; Kam, B.L.; Kwekkeboom, D.J. Comparison of response evaluation in patients with gastroenteropancreatic and thoracic neuroendocrine tumors after treatment with [177Lu-DOTA0, Tyr3]octreotate. J. Nucl. Med. 2013, 54, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Ezziddin, S.; Khalaf, F.; Vanezi, M.; Haslerud, T.; Mayer, K.; Zreiqat, A.; Willinek, W.; Biersack, H.J.; Sabet, A. Outcome of peptide receptor radionuclide therapy with 177Lu-octreotate in advanced grade 1/2 pancreatic neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 925–933. [Google Scholar] [CrossRef]
- Bodei, L.; Kidd, M.; Modlin, I.M.; Severi, S.; Drozdov, I.; Nicolini, S.; Kwekkeboom, D.J.; Krenning, E.P.; Baum, R.P.; Paganelli, G. Measurement of circulating transcripts and gene cluster analysis predicts and defines therapeutic efficacy of peptide receptor radionuclide therapy (PRRT) in neuroendocrine tumors. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 839–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soydal, C.; Peker, A.; Ozkan, E.; Kucuk, O.N.; Kir, M.K. The role of baseline Ga-68 DOTATATE positron emission tomography/computed tomography in the prediction of response to fixed-dose peptide receptor radionuclide therapy with Lu-177 DOTATATE. Turk. J. Med. Sci. 2016, 46, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Hamiditabar, M.; Ali, M.; Roys, J.; Wolin, E.M.; O’Dorisio, T.M.; Ranganathan, D.; Tworowska, I.; Strosberg, J.R.; Delpassand, E.S. Peptide receptor radionuclide therapy with 177Lu-octreotate in patients with somatostatin receptor expressing neuroendocrine tumors: Six years’ assessment. Clin. Nucl. Med. 2017, 42, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Del Prete, M.; Buteau, F.A.; Beauregard, J.M. Personalized 177Luoctreotate peptide receptor radionuclide therapy of neuroendocrine tumours: A simulation study. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1490–1500. [Google Scholar] [CrossRef]
- Del Prete, M.; Buteau, F.A.; Arsenault, F.; Saighi, N.; Bouchard, L.O.; Beaulieu, A.; Beauregard, J.M. Personalized 177Lu-octreotate peptide receptor radionuclide therapy of neuroendocrine tumours: Initial results from the P-PRRT trial. Eur. J. Nucl. Med. Mol. Imaging 2018, 46, 728–742. [Google Scholar] [CrossRef] [PubMed]
- Kalshetty, A.; Ramaswamy, A.; Ostwal, V.; Basu, S. Resistant functioning and/or progressive symptomatic metastatic gastroenteropancreatic neuroendocrine tumors: Efficacy of 177Lu-DOTATATE peptide receptor radionuclide therapy in this setting. Nucl. Med. Commun. 2018, 39, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Kulkarni, H.; Singh, A.; Niepsch, K.; Müller, D.; Baum, R. Peptide Receptor Radionuclide Therapy in Grade 3 Neuroendocrine Neoplasms: Safety and Survival Analysis in 69 Patients. J. Nucl. Med. 2019, 60, 377–385. [Google Scholar] [CrossRef]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of (177)Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Strosberg, J.; Caplin, M.; Kunz, P.; Ruszniewski, P.; Bodei, L.; Hendifar, A.E.; Mittra, E.; Wolin, E.M.; Yao, J.C.; Pavel, M.E.; et al. Final overall survival in the phase 3 NETTER-1 study of lutetium-177-DOTATATE in patients with midgut neuroendocrine tumors. In Proceedings of the 2021 ASCO Annual Meeting, Chicago, IL, USA, 4–8 June 2021. [Google Scholar]
- Caplin, M.E.; Baudin, E.; Ferolla, P.; Filosso, P.; Garcia-Yuste, M.; Lim, E.; Oberg, K.; Pelosi, G.; Perren, A.; Rossi, R.E.; et al. Pulmonary neuroendocrine (carcinoid) tumors: European Neuroendocrine Tumor Society expert consensus and recommendations for best practice for typical and atypical pulmonary carcinoids. Ann. Oncol. 2015, 26, 1604–1620. [Google Scholar] [CrossRef]
- Delle Fave, G.; O’Toole, D.; Sundin, A.; Taal, B.; Ferolla, P.; Ramage, J.K.; Ferone, D.; Ito, T.; Weber, W.; Zheng-Pei, Z.; et al. ENETS Consensus Guidelines Update for Gastroduodenal Neuroendocrine Neoplasms. Neuroendocrinology 2016, 103, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fassnacht, M.; Assie, G.; Baudin, E.; Eisenhofer, G.; de la Fouchardiere, C.; Haak, H.R.; de Krijger, R.; Porpiglia, F.; Terzolo, M.; Berruti, A. Adrenocortical carcinomas and malignant phaeochromocytomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1476–1490. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carbonero, R.; Sorbye, H.; Baudin, E.; Raymond, E.; Wiedenmann, B.; Niederle, B.; Sedlackova, E.; Toumpanakis, C.; Anlauf, M.; Cwikla, J.B.; et al. ENETS Consensus Guidelines for High-Grade Gastroenteropancreatic Neuroendocrine Tumors and Neuroendocrine Carcinomas. Neuroendocrinology 2016, 103, 186–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Flores, E.; Serrano, R.; Sevilla, I.; Viudez, A.; Barriuso, J.; Benavent, M.; Capdevila, J.; Jimenez-Fonseca, P.; López, C.; Garcia-Carbonero, R. SEOM clinical guidelines for the diagnosis and treatment of gastroenteropancreatic and bronchial neuroendocrine neoplasms (NENs) (2018). Clin. Transl. Oncol. 2019, 21, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.; Sundin, A.; Perren, A.; Berruti, A. Gastroenteropancreatic Neuroendocrine Neoplasms: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef] [PubMed]
- Brabander, T.; Nonnekens, J.; Hofland, J. The next generation of peptide receptor radionuclide therapy. Endocr. Relat. Cancer 2019, 26, C7–C11. [Google Scholar] [CrossRef] [Green Version]
- Kratochwil, C.; Giesel, F.L.; Bruchertseifer, F.; Mier, W.; Apostolidis, C.; Boll Murphy, K.; Haberkorn, U.; Morgenstern, A. Bi-DOTATOC receptor-targeted alpha-radionuclide therapy induces remission in neuroendocrine tumours refractory to beta radiation: A first-inhuman experience. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 2106–2119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCT03466216, Phase 1 Study of AlphaMedix™ in Adult Subjects With SSTR (+) NET. 2018. Available online: http://clinicaltrials.gov/ct2/show/NCT03466216 (accessed on 22 August 2021).
- Ginj, M.; Zhang, H.; Waser, B.; Cescato, R.; Wild, D.; Wang, X.; Erchegyi, J.; Rivier, J.; Mäcke, H.R.; Reubi, J.C. Radiolabeled somatostatin receptor antagonists are preferable to agonists for in vivo peptide receptor targeting of tumors. Proc. Natl. Acad. Sci. USA 2006, 103, 16436–16441. [Google Scholar] [CrossRef] [Green Version]
- Wild, D.; Fani, M.; Behe, M.; Brink, I.; Rivier, J.E.; Reubi, J.C.; Maecke, H.R.; Weber, W.A. First clinical evidence that imaging with somatostatin receptor antagonists is feasible. J. Nucl. Med. 2011, 52, 1412–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bass, R.T.; Buckwalter, B.L.; Patel, B.P.; Pausch, M.H.; Price, L.A.; Strnad, J.; Hadcock, J.R. Identification and characterization of novel somatostatin antagonists. Mol. Pharmacol. 1996, 50, 709–715. [Google Scholar] [PubMed]
- Fani, M.; Nicolas, G.P.; Wild, D. Somatostatin Receptor Antagonists for Imaging and Therapy. J. Nucl. Med. 2017, 58 (Suppl. S2), 61S–66S. [Google Scholar] [CrossRef] [PubMed]
- Dalm, S.U.; Nonnekens, J.; Doeswijk, G.N.; de Blois, E.; van Gent, D.C.; Konijnenberg, M.W.; de Jong, M. Comparison of the Therapeutic Response to Treatment with a 177Lu-Labeled Somatostatin Receptor Agonist and Antagonist in Preclinical Models. J. Nucl. Med. 2016, 57, 260–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fani, M.; Del Pozzo, L.; Abiraj, K.; Mansi, R.; Tamma, M.L.; Cescato, R.; Waser, B.; Weber, W.A.; Reubi, J.C.; Maecke, H.R. PET of somatostatin receptor–positive tumors using 64Cu- and 68Ga-somatostatin antagonists: The chelate makes the difference. J. Nucl. Med. 2011, 52, 1110–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wild, D.; Fani, M.; Fischer, R.; Del Pozzo, L.; Kaul, F.; Krebs, S.; Fischer, R.; Rivier, J.E.; Reubi, J.C.; Maecke, H.R.; et al. Comparison of somatostatin receptor agonist and antagonist for peptide receptor radionuclide therapy: A pilot study. J. Nucl. Med. 2014, 55, 1248–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCT02609737, Theranostics of Radiolabeled Somatostatin Antagonists 68Ga-DOTA-JR11 and 177Lu-DOTA-JR11 in Patients With Neuroendocrine Tumors. 2015. Available online: http://clinicaltrials.gov/ct2/show/NCT02609737 (accessed on 25 October 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SSTR Imaging | Sensitivity | Specificity |
|---|---|---|
| 68Ga-DOTA-SSA PET/CT | 93% (70–100%) [22] | 96% (67–100%) |
| 111In-DTPA-Pentetreotide SPECT/CT | 72% (58–75%) [23] | 93% (77–99%) |
| Characteristics | Promid | Clarinet |
|---|---|---|
| Number of patients | 85 | 204 |
| Localization | Midgut | Midgut, foregut, pancreas, primary unknown |
| Grade | 1 (Ki-67 ≤ 2%) | 1, 2 (ki67 < 10%) |
| Funcionality | Functioning (38.8% carcinoid síndrome) Non functioning | Non functioning (Except gastrinomas well-controlled with PPI) |
| Liver burden | ≤25%: 67.1% <10%: 67.2% | ≤25%: 66% <10%: 51.9% |
| SSTR expression | Positive/negative | Positive (Krenning score 2–4) |
| Treatment | Octreotide LAR 30 mg/28 days versus Placebo | Lanreotide 120 mg/28 days versus Placebo |
| Primary objective | Time to progression (months) | Progression free survival (months) |
| Results | Stable disease: 66.7% vs. 37.2% Time to progression: 14.3 m vs. 6 m | Progression free survival 32.8 m vs. 18 m |
| Study | Study Design | Dose (GBq) | Number of Cycles | Nº Patients | Disease Response Rate (%) | Disease Control Rate (%) |
|---|---|---|---|---|---|---|
| Sward (2010) [64] | Retrospective | 8 | 4–5 | 16 | RECIST 37.5 | RECIST 87.5 |
| Van Vliet (2013) [65] | Retrospective | 3.7–7.4 | 4 | 257 | RECIST 27.6 SWOG 25.3 | RECIST 76.2 SWOG 74 |
| Ezziddin et al. (2014) [66] | Retrospective | 8 | 4 | 68 | RECIST 57.4 SWOG 60.3 | RECIST 85.3 SWOG 85.3 |
| Sabe et al. (2015) [59] | Retrospective | 7.9 | 4 | 61 | RECIST 16.4 SWOG 13 | RECIST 90 SWOG 91.2 |
| Bodei et al. (2016) [67] | Retrospective | 3.7–6.5 | 4 | 54 | RECIST 18.5 | RECIST 72.2 |
| Soydal et al. (2016) [68] | Retrospective | 7.4 | 4–8 | 29 | RECIST 27.6 | RECIST 89.6 |
| Hamditibar et al. (2017) [69] | Retrospective | 7.4 | 1–6 | 28 | RECIST 28.6 | RECIST 114.3 |
| de Prette et al. (2017) [70] | Retrospective | 5.9–15.9 | 4 | 23 | RECIST 8.7 SWOG 8.7 | RECIST 73.9 SWOG 73.9 |
| Khalshetty et al. (2019) [72] | Retrospective | 5.55 | 4 | 46 | RECIST 43.5 | RECIST 80.4 |
| Sansovini et al. (2013) [57] | Prospective | 3.7–5.5 | 5 | 52 | SWOG 28.8 | SWOG 80.7 |
| Bodei et al. (2011) [56] | Phase I/II | 3.7–7.4 | 4–6 | 51 | RECIST 29.4 | RECIST 82.3 |
| Delpassand et al. (2014) [60] | Phase II | 7.4 | 1–4 | 32 | RECIST 28.1 | RECIST 71.9 |
| Paganelli et al. (2014) [58] | Phase II | 3.7–5.5 | 5 | 43 | SWOG 7 | SWOG 83.7 |
| del Prete et al. (2018) [71] | Phase II | 7.4 | 4 | 11 | RECIST 18.2 SWOG 9 | RECIST 81.8 SWOG 81.8 |
| Strosberg et al. (2016) [74] | Phase III | 7.4 | 4 | 101 | RECIST 17.8 | RECIST 17.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
del Olmo-Garcia, M.I.; Prado-Wohlwend, S.; Andres, A.; Soriano, J.M.; Bello, P.; Merino-Torres, J.F. Somatostatin and Somatostatin Receptors: From Signaling to Clinical Applications in Neuroendocrine Neoplasms. Biomedicines 2021, 9, 1810. https://doi.org/10.3390/biomedicines9121810
del Olmo-Garcia MI, Prado-Wohlwend S, Andres A, Soriano JM, Bello P, Merino-Torres JF. Somatostatin and Somatostatin Receptors: From Signaling to Clinical Applications in Neuroendocrine Neoplasms. Biomedicines. 2021; 9(12):1810. https://doi.org/10.3390/biomedicines9121810
Chicago/Turabian Styledel Olmo-Garcia, Maria Isabel, Stefan Prado-Wohlwend, Alexia Andres, Jose M. Soriano, Pilar Bello, and Juan Francisco Merino-Torres. 2021. "Somatostatin and Somatostatin Receptors: From Signaling to Clinical Applications in Neuroendocrine Neoplasms" Biomedicines 9, no. 12: 1810. https://doi.org/10.3390/biomedicines9121810
APA Styledel Olmo-Garcia, M. I., Prado-Wohlwend, S., Andres, A., Soriano, J. M., Bello, P., & Merino-Torres, J. F. (2021). Somatostatin and Somatostatin Receptors: From Signaling to Clinical Applications in Neuroendocrine Neoplasms. Biomedicines, 9(12), 1810. https://doi.org/10.3390/biomedicines9121810