
Fas-Fas Ligand Interplay in the Periphery of Salivary Gland Carcinomas as a New Checkpoint Predictor for Disease Severity and Immunotherapy Response

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
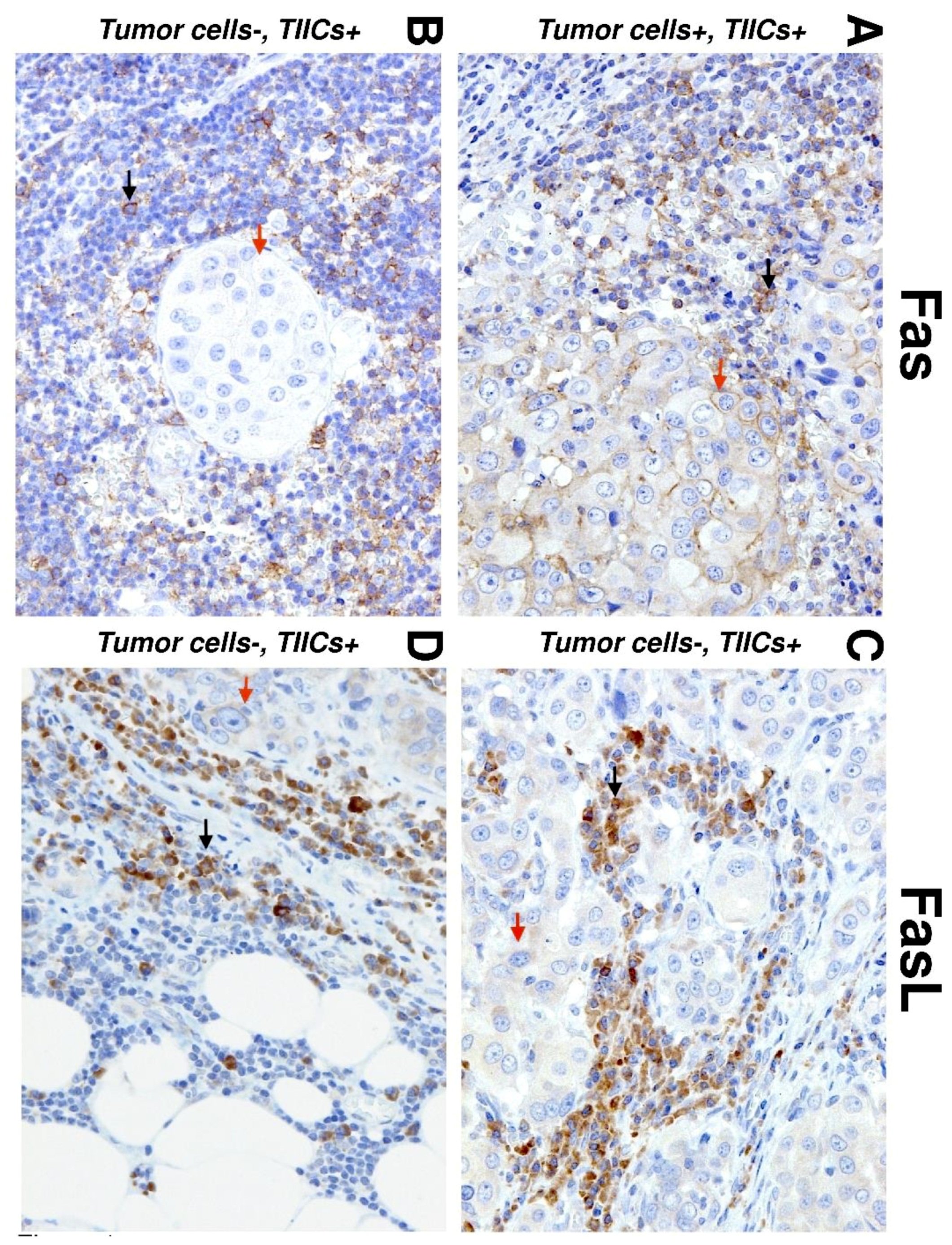
2.2. Immunohistochemistry
2.3. Statistical Analysis
3. Results
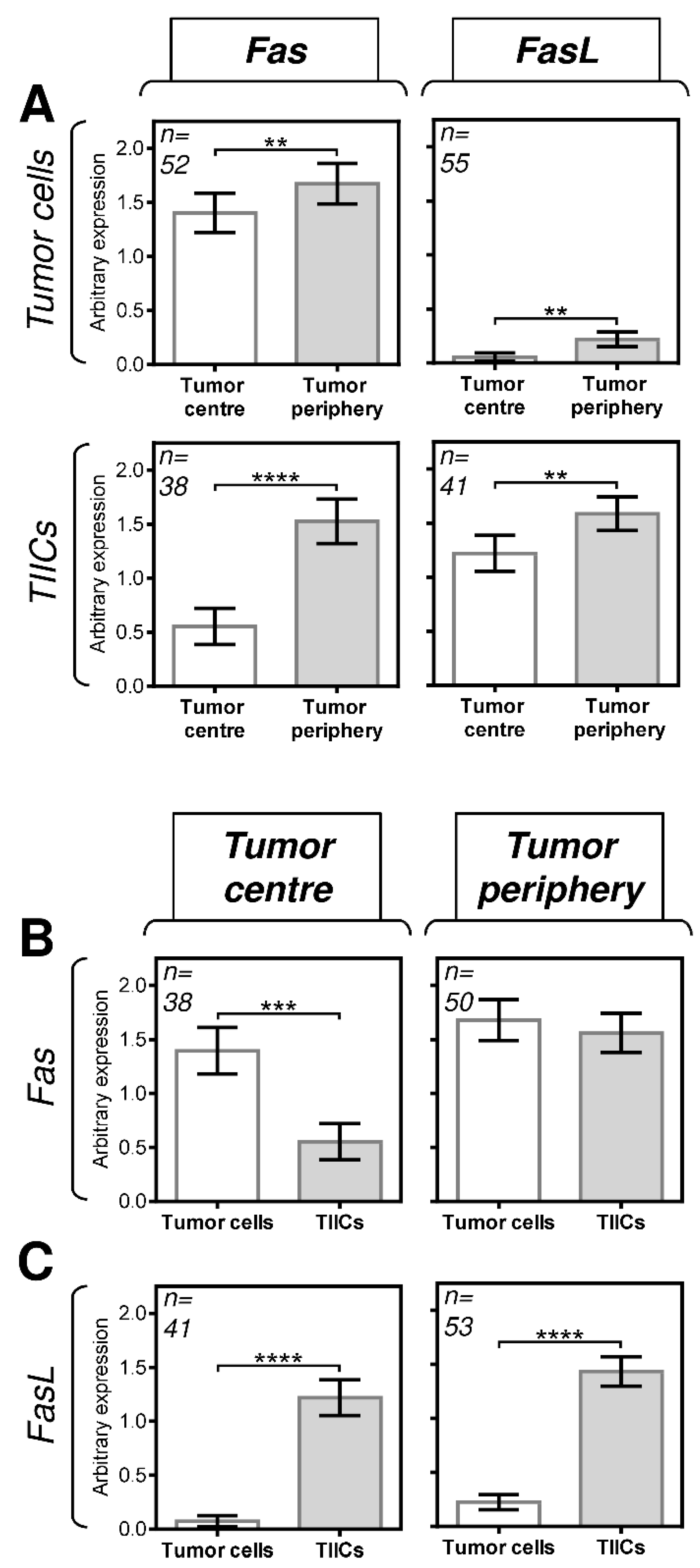
3.1. The Differences between the Expression of Fas and FasL in Tumor Cells and TIICs Are Clustered in the Tumor Center
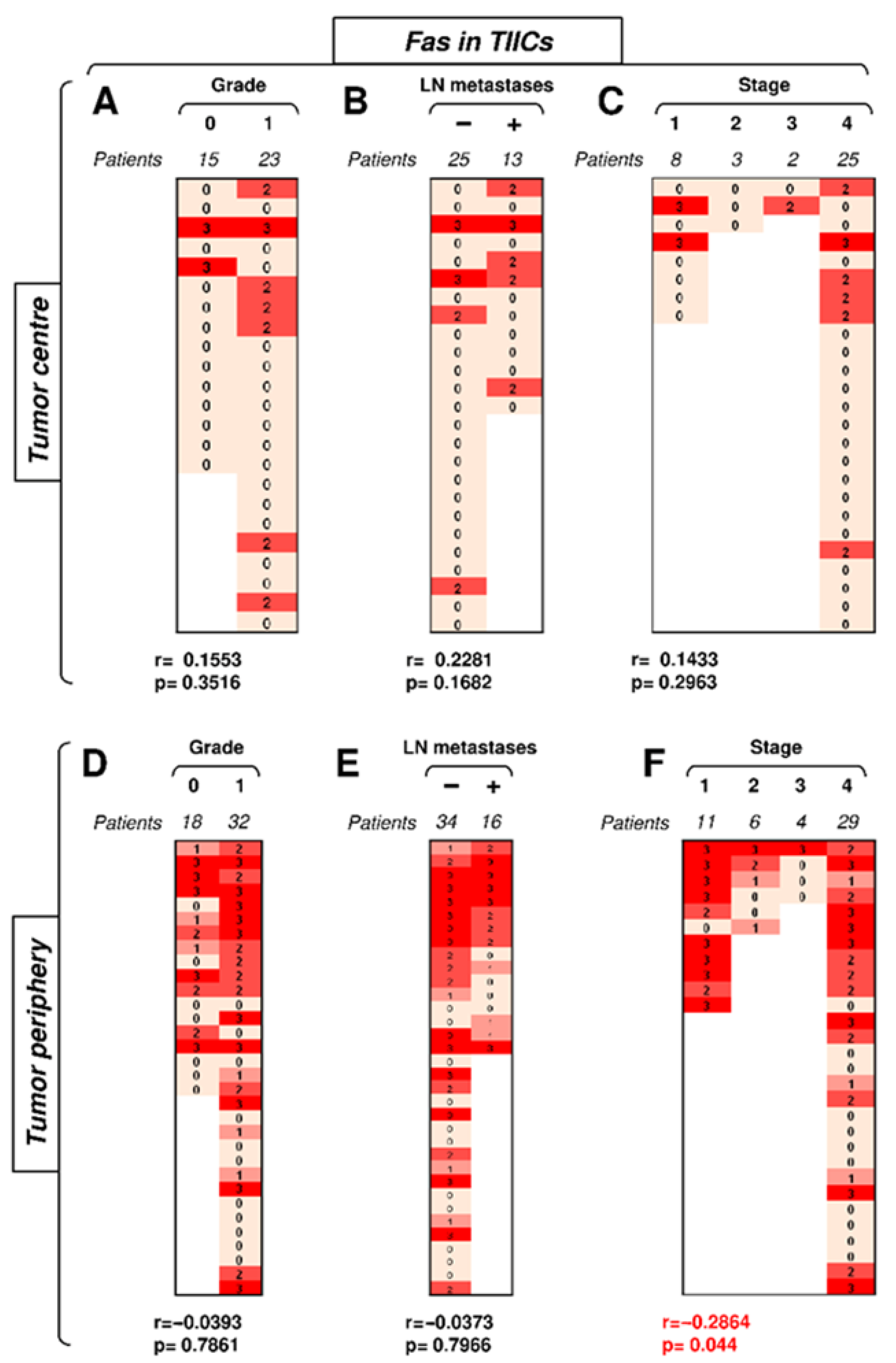
3.2. Fas Expression in TIICs Negatively Correlates with Tumor Stage in the Tumor Periphery
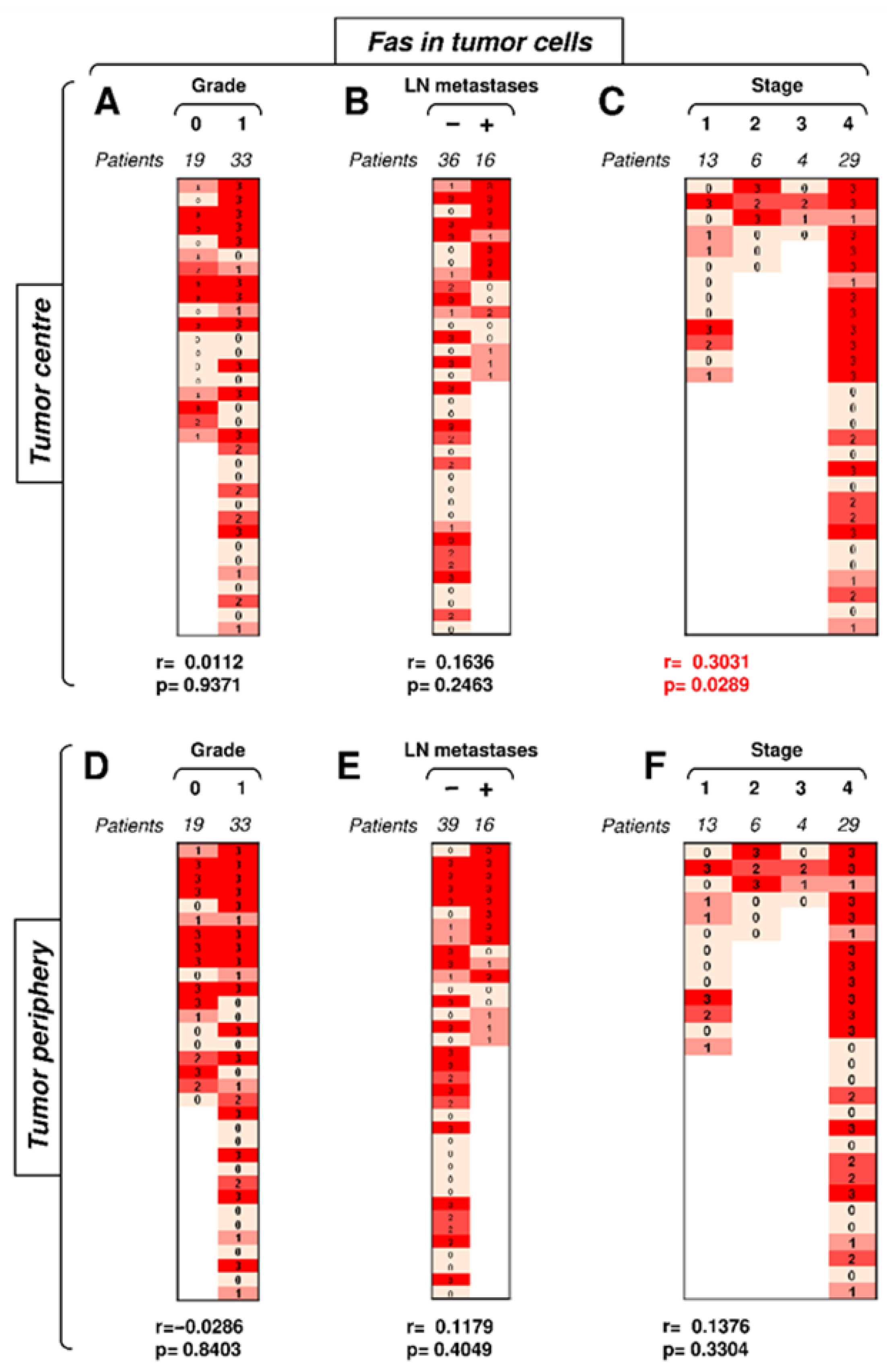
3.3. Fas Expression in Tumor Cells Positively Correlates with Tumor Stage in the Tumor Center
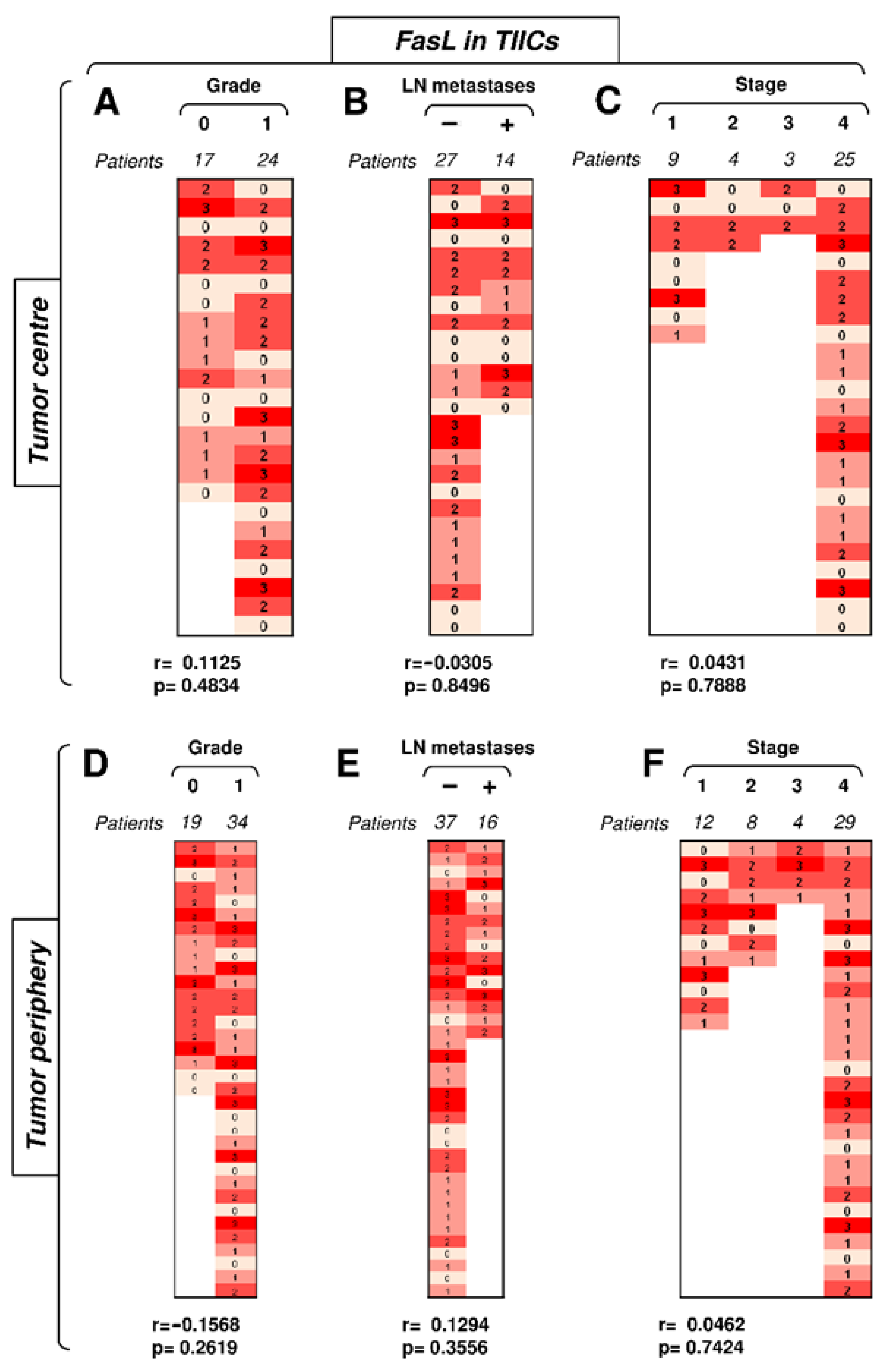
3.4. FasL Expression in TIICs Is Not Impacted by Disease Severity or Compartmental Distribution in the Tumor
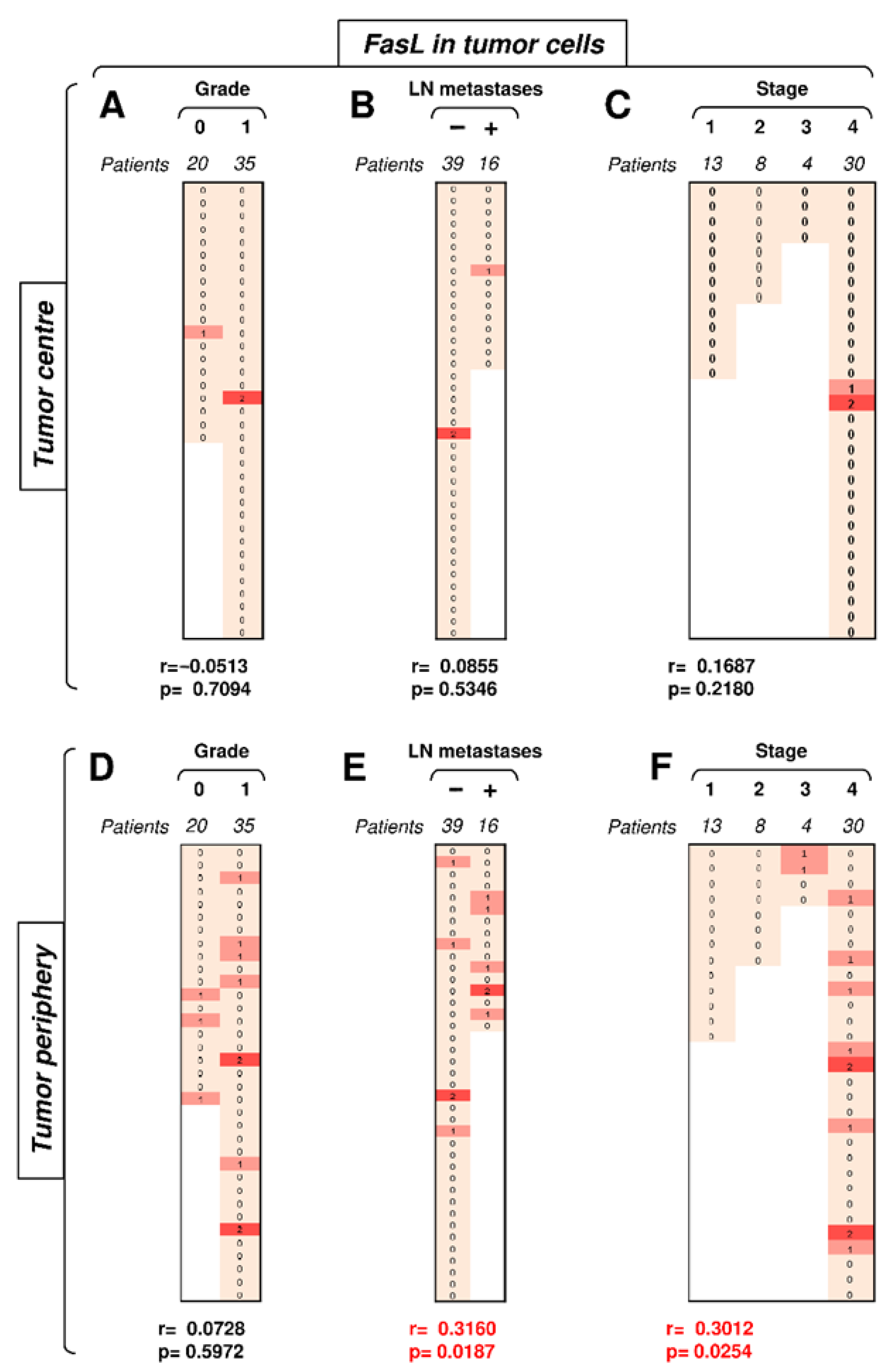
3.5. FasL Expression in Tumor Cells Positively Correlates with Tumor Stage in the Tumor Periphery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, R.J.; Tan, A.P.; Tong, E.L.; Satyadev, N.; Christensen, R.E. Epidemiology, prognostic factors, and treatment of malignant submandibular gland tumors: A population-based cohort analysis. JAMA Otolaryngol. 2015, 141, 905–912. [Google Scholar] [CrossRef] [Green Version]
- Galdirs, T.M.; Kappler, M.; Reich, W.; Eckert, A.W. Current aspects of salivary gland tumors—A systematic review of the literature. GMS Interdiscip. Plast. Reconstr. Surg. 2019, 8, 12. [Google Scholar] [CrossRef]
- Ettl, T.; Schwarz-Furlan, S.; Gosau, M.; Reichert, T.E. Salivary gland carcinomas. Oral Maxillofac. Surg. 2012, 16, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, M.B.; Albergotti, W.G.; Eisele, D.W. Recurrent salivary gland cancer. Curr. Treat. Options Oncol. 2012, 13, 58–70. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.B.; Delord, J.P.; Doi, T.; Piha-Paul, S.A.; Liu, S.V.; Gilbert, J.; Algazi, A.P.; Damian, S.; Hong, R.L.; Le Tourneau, C.; et al. Pembrolizumab for the treatment of advanced salivary gland carcinoma: Findings of the phase 1b KEYNOTE-028 study. Am. J. Clin. Oncol. 2018, 41, 1083–1088. [Google Scholar] [CrossRef]
- Voelker, R. Immunotherapy is now first-line therapy for some colorectal cancers. JAMA 2020, 324, 433. [Google Scholar] [CrossRef]
- Peters, S.; Reck, M.; Smit, E.F.; Mok, T.; Hellmann, M.D. How to make the best use of immunotherapy as first-line treatment of advanced/metastatic non-small-cell lung cancer. Ann. Oncol. 2019, 30, 884–896. [Google Scholar] [CrossRef]
- Labriola, M.K.; Batich, K.A.; Zhu, J.; McNamara, M.A.; Harrison, M.R.; Armstrong, A.J.; George, D.J.; Zhang, T. Immunotherapy is changing first-line treatment of metastatic renal-cell carcinoma. Clin. Genitourin. Cancer 2019, 17, e513–e521. [Google Scholar] [CrossRef]
- Ventola, C.L. Cancer immunotherapy, part 3: Challenges and future trends. Peer Rev. J. Formul. Manag. 2017, 42, 514–521. [Google Scholar]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, Y.; Ohta, S.; Sayem, M.A.; Tsukamoto, N.; Yaguchi, T. Immune-resistant mechanisms in cancer immunotherapy. Int. J. Clin. Oncol. 2020, 25, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Barrueto, L.; Caminero, F.; Cash, L.; Makris, C.; Lamichhane, P.; Deshmukh, R.R. Resistance to checkpoint inhibition in cancer immunotherapy. Transl. Oncol. 2020, 13, 100738. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Chen, M.; Nie, H.; Yuan, Y. PD-1 and PD-L1 in cancer immunotherapy: Clinical implications and future considerations. Hum. Vaccines Immunother. 2019, 15, 1111–1122. [Google Scholar] [CrossRef]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and Anti-CTLA-4 therapies in cancer: Mechanisms of action, efficacy, and limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Powis de Tenbossche, C.G.; Cane, S.; Colau, D.; van Baren, N.; Lurquin, C.; Schmitt-Verhulst, A.M.; Liljestrom, P.; Uyttenhove, C.; Van den Eynde, B.J. Resistance to cancer immunotherapy mediated by apoptosis of tumor-infiltrating lymphocytes. Nat. Commun. 2017, 8, 1404. [Google Scholar] [CrossRef] [Green Version]
- Gibson, J.T.; Orlandella, R.M.; Turbitt, W.J.; Behring, M.; Manne, U.; Sorge, R.E.; Norian, L.A. Obesity-associated myeloid-derived suppressor cells promote apoptosis of tumor-infiltrating CD8 T cells and immunotherapy resistance in breast cancer. Front. Immunol. 2020, 11, 590794. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, E.; Hashimoto, N.; Osuka, S.; Shimizu, T.; Ueno, S.; Okazaki, S.; Yaguchi, T.; Kawakami, Y.; Kosaki, K.; Sato, T.A.; et al. The inhibitor of apoptosis protein livin confers resistance to Fas-mediated immune cytotoxicity in refractory lymphoma. Cancer Res. 2020, 80, 4439–4450. [Google Scholar] [CrossRef]
- Peter, M.E.; Hadji, A.; Murmann, A.E.; Brockway, S.; Putzbach, W.; Pattanayak, A.; Ceppi, P. The role of CD95 and CD95 ligand in cancer. Cell Death Differ. 2015, 22, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.H.; O’Sullivan, B. Overview of the 8th edition TNM classification for head and neck cancer. Curr. Treat. Options Oncol. 2017, 18, 40. [Google Scholar] [CrossRef]
- O’Kane, G.; Lynch, M.; Hooper, S.; Aird, J.; Muldoon, C.; Mulligan, N.; Loscher, C.; Gallagher, D.J. Zonal differences in PD-1 expression in centre of tumour versus periphery in microsatellite stable and unstable colorectal cancer. J. Clin. Oncol. 2015, 33, 3574. [Google Scholar] [CrossRef]
- Ferrata, M.; Schad, A.; Zimmer, S.; Musholt, T.J.; Bahr, K.; Kuenzel, J.; Becker, S.; Springer, E.; Roth, W.; Weber, M.M.; et al. PD-L1 Expression and immune cell infiltration in Gastroenteropancreatic (GEP) and Non-GEP neuroendocrine neoplasms with high proliferative activity. Front. Oncol. 2019, 9, 343. [Google Scholar] [CrossRef] [Green Version]
- Phillips, T.; Simmons, P.; Inzunza, H.D.; Cogswell, J.; Novotny, J., Jr.; Taylor, C.; Zhang, X. Development of an automated PD-L1 immunohistochemistry (IHC) assay for non-small cell lung cancer. Appl. Immunohistochem. Mol. Morphol. 2015, 23, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Igarashi, T.; Teramoto, K.; Ishida, M.; Hanaoka, J.; Daigo, Y. Scoring of PD-L1 expression intensity on pulmonary adenocarcinomas and the correlations with clinicopathological factors. ESMO Open 2016, 1, e000083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cedres, S.; Ponce-Aix, S.; Zugazagoitia, J.; Sansano, I.; Enguita, A.; Navarro-Mendivil, A.; Martinez-Marti, A.; Martinez, P.; Felip, E. Analysis of expression of programmed cell death 1 ligand 1 (PD-L1) in malignant pleural mesothelioma (MPM). PLoS ONE 2015, 10, e0121071. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Ibrahim, M.L.; Redd, P.S.; Klement, J.D.; Lu, C.; Yang, D.; Savage, N.M.; Liu, K. Loss of Fas expression and function is coupled with colon cancer resistance to immune checkpoint inhibitor immunotherapy. Mol Cancer Res. 2019, 17, 420–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zietz, C.; Rumpler, U.; Sturzl, M.; Lohrs, U. Inverse relation of Fas-ligand and tumor-infiltrating lymphocytes in angiosarcoma: Indications of apoptotic tumor counterattack. Am. J. Pathol. 2001, 159, 963–970. [Google Scholar] [CrossRef]
- Zhu, J.; Petit, P.F.; Van den Eynde, B.J. Apoptosis of tumor-infiltrating T lymphocytes: A new immune checkpoint mechanism. Cancer Immunol. Immunother. 2019, 68, 835–847. [Google Scholar] [CrossRef]
- Blok, E.J.; van den Bulk, J.; Dekker-Ensink, N.G.; Derr, R.; Kanters, C.; Bastiaannet, E.; Kroep, J.R.; van de Velde, C.J.; Kuppen, P.J. Combined evaluation of the FAS cell surface death receptor and CD8+ tumor infiltrating lymphocytes as a prognostic biomarker in breast cancer. Oncotarget 2017, 8, 15610–15620. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.M.; Chan, F.K.; Chun, H.J.; Lenardo, M.J. The multifaceted role of Fas signaling in immune cell homeostasis and autoimmunity. Nat. Immunol. 2000, 1, 469–474. [Google Scholar] [CrossRef]
- Villa-Morales, M.; Cobos, M.A.; Gonzalez-Gugel, E.; Alvarez-Iglesias, V.; Martinez, B.; Piris, M.A.; Carracedo, A.; Benitez, J.; Fernandez-Piqueras, J. FAS system deregulation in T-cell lymphoblastic lymphoma. Cell Death Dis. 2014, 5, e1110. [Google Scholar] [CrossRef] [Green Version]
- Sordo-Bahamonde, C.; Lorenzo-Herrero, S.; Payer, A.R.; Gonzalez, S.; Lopez-Soto, A. Mechanisms of apoptosis resistance to NK cell-mediated cytotoxicity in cancer. Int. J. Mol. Sci. 2020, 21, 3726. [Google Scholar] [CrossRef] [PubMed]
- Tauzin, S.; Debure, L.; Moreau, J.F.; Legembre, P. CD95-mediated cell signaling in cancer: Mutations and post-translational modulations. Cell. Mol. Life Sci. 2012, 69, 1261–1277. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.W.; O’Connell, J.; O’Sullivan, G.C.; Brady, C.; Roche, D.; Collins, J.K.; Shanahan, F. The Fas counterattack in vivo: Apoptotic depletion of tumor-infiltrating lymphocytes associated with Fas ligand expression by human esophageal carcinoma. J. Immunol. 1998, 160, 5669–5675. [Google Scholar]
- Yamada, A.; Arakaki, R.; Saito, M.; Kudo, Y.; Ishimaru, N. Dual role of Fas/FasL-mediated signal in peripheral immune tolerance. Front. Immunol. 2017, 8, 403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waring, P.; Mullbacher, A. Cell death induced by the Fas/Fas ligand pathway and its role in pathology. Immunol. Cell Biol. 1999, 77, 312–317. [Google Scholar] [CrossRef]
- Nagata, S. Fas-induced apoptosis, and diseases caused by its abnormality. Genes Cells 1996, 1, 873–879. [Google Scholar] [CrossRef]
- Linxweiler, M.; Kuo, F.; Katabi, N.; Lee, M.; Nadeem, Z.; Dalin, M.G.; Makarov, V.; Chowell, D.; Dogan, S.; Ganly, I.; et al. The immune microenvironment and neoantigen landscape of aggressive salivary gland carcinomas differ by subtype. Clin. Cancer Res. 2020, 26, 2859–2870. [Google Scholar] [CrossRef] [Green Version]
- Tschumi, B.O.; Dumauthioz, N.; Marti, B.; Zhang, L.; Lanitis, E.; Irving, M.; Schneider, P.; Mach, J.P.; Coukos, G.; Romero, P.; et al. CART cells are prone to Fas- and DR5-mediated cell death. J. Immunother. Cancer 2018, 6, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuenzi, P.; Schneider, P.; Dobbelaere, D.A. Theileria parva-transformed T cells show enhanced resistance to Fas/Fas ligand-induced apoptosis. J. Immunol. 2003, 171, 1224–1231. [Google Scholar] [CrossRef] [Green Version]
- Yasukawa, M.; Ohminami, H.; Arai, J.; Kasahara, Y.; Ishida, Y.; Fujita, S. Granule exocytosis, and not the Fas/Fas ligand system, is the main pathway of cytotoxicity mediated by alloantigen-specific CD4(+) as well as CD8(+) cytotoxic T lymphocytes in humans. Blood 2000, 95, 2352–2355. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mucoepidermoid Carcinoma | 20.98% |
| Adenoid cystic carcinoma | 17.74% |
| Acinic cell carcinoma | 12.90% |
| Adenocarcinoma, not otherwise specified (NOS) | 9.68% |
| Salivary duct carcinoma | 9.68% |
| Undifferentiated carcinoma | 6.45% |
| Carcinoma ex pleiomorphic adenoma | 4.84% |
| Mammary analogue secretory carcinoma (MASC) | 4.84% |
| Myoepithelial carcinoma | 4.84% |
| Squamous cell carcinoma | 3.23% |
| Adenosquamous carcinoma | 1.61% |
| Carcinosarcoma | 1.61% |
| Cribriform cystadenocarcinoma | 1.61% |
 | |
| SEX | AGE | GRADE | STAGE * | METASTASES | |||||
|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 50 year ≥ x | 50 year ≤ x | Low (0) | High (1) | Stage (1 + 2) | Stage (3 + 4) | Yes (1) | No (0) |
| 58.06% | 42.94% | 43.55% | 56.45% | 35.48% | 64.52% | 38.74% | 59.68% | 30.65% | 69.35% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strizova, Z.; Kuchar, M.; Capkova, L.; Komarc, M.; Skrivan, J.; Bartunkova, J.; Plzak, J.; Smrz, D. Fas-Fas Ligand Interplay in the Periphery of Salivary Gland Carcinomas as a New Checkpoint Predictor for Disease Severity and Immunotherapy Response. Biomedicines 2021, 9, 402. https://doi.org/10.3390/biomedicines9040402
Strizova Z, Kuchar M, Capkova L, Komarc M, Skrivan J, Bartunkova J, Plzak J, Smrz D. Fas-Fas Ligand Interplay in the Periphery of Salivary Gland Carcinomas as a New Checkpoint Predictor for Disease Severity and Immunotherapy Response. Biomedicines. 2021; 9(4):402. https://doi.org/10.3390/biomedicines9040402
Chicago/Turabian StyleStrizova, Zuzana, Martin Kuchar, Linda Capkova, Martin Komarc, Jiri Skrivan, Jirina Bartunkova, Jan Plzak, and Daniel Smrz. 2021. "Fas-Fas Ligand Interplay in the Periphery of Salivary Gland Carcinomas as a New Checkpoint Predictor for Disease Severity and Immunotherapy Response" Biomedicines 9, no. 4: 402. https://doi.org/10.3390/biomedicines9040402
APA StyleStrizova, Z., Kuchar, M., Capkova, L., Komarc, M., Skrivan, J., Bartunkova, J., Plzak, J., & Smrz, D. (2021). Fas-Fas Ligand Interplay in the Periphery of Salivary Gland Carcinomas as a New Checkpoint Predictor for Disease Severity and Immunotherapy Response. Biomedicines, 9(4), 402. https://doi.org/10.3390/biomedicines9040402