
Parathyroid Disease in Pregnancy and Lactation: A Narrative Review of the Literature



Abstract
:1. Introduction and Methodology
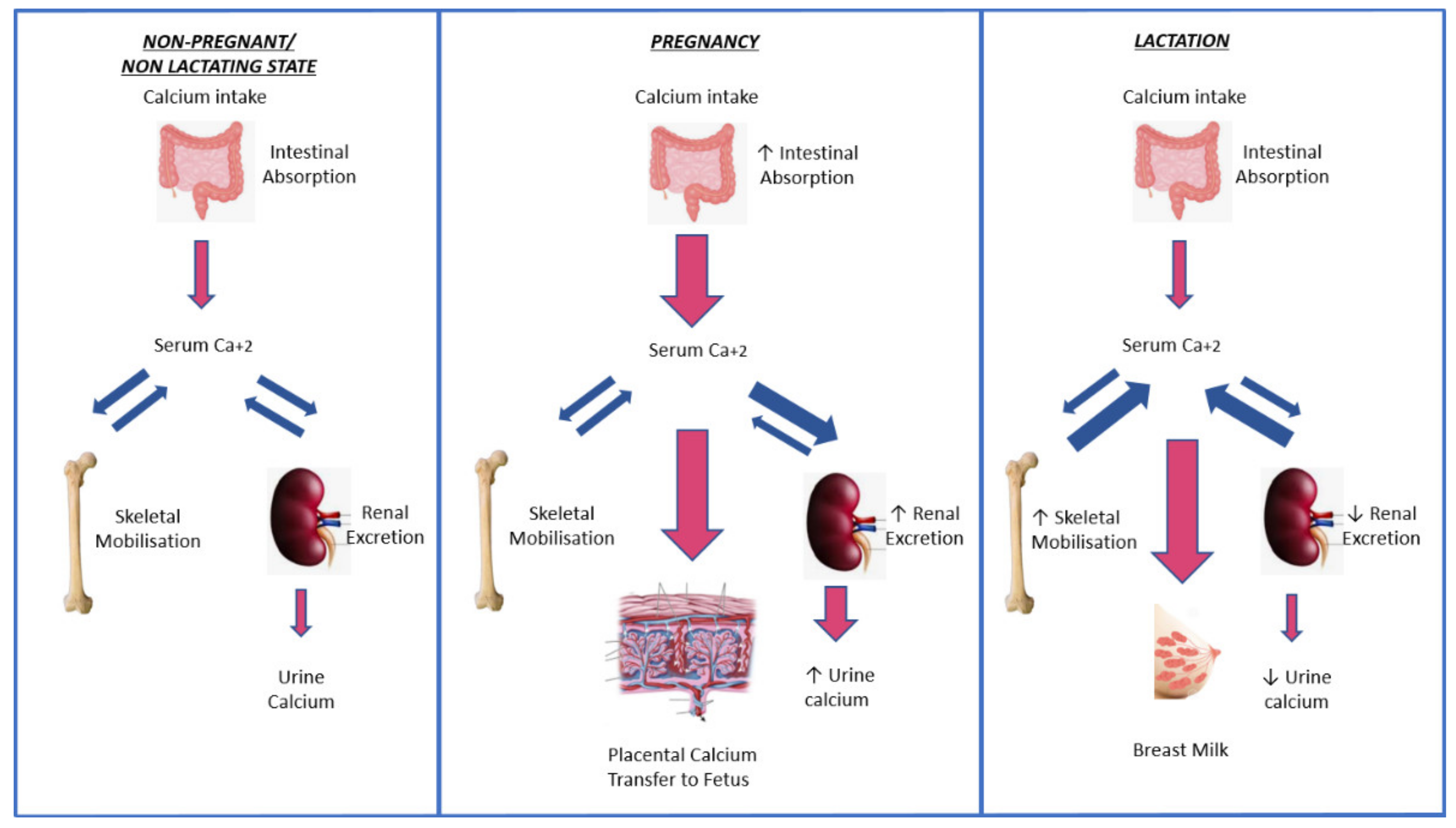
2. Calcium Physiology during Pregnancy and Lactation
3. Disorders of Calcium and Parathyroid Physiology during Pregnancy and Lactation
3.1. Primary Hyperparathyroidism
3.2. Pregnancy Outcomes in Primary Hyperparathyroidism
3.3. Maternal Complications of Primary Hyperparathyroidism
3.4. Fetal Complications of Primary Hyperparathyroidism
3.5. Management of Primary Hyperparathyroidism during Pregnancy

{kind=link}
{kind=link}
| Study | Study Design | No of Women/Pregnancies | Intervention | Trimester | Outcome | Comments |
|---|---|---|---|---|---|---|
| Gelister et al., 1989 [70] | Retrospective case series | 4 | Sx: 2 non-Sx: 2 | 1st and NR | Sx: uncomplicated non-Sx: 1 uncomplicated; 1 3rd trimester hypertension-CS-healthy infant | |
| Hsieh et al., 1998 [53] | Retrospective case series | 3 | Sx: 2 Non-Sx: 1 | 3rd | Sx: no maternal, fetal, or neonatal complications non-Sx: neonatal hypocalcemia | |
| Gidiri et al., 2004 [54] | Case series | 2 | Sx: 2 | 3rd | healthy infants | |
| Schnatz & Thaxton 2005 [52] | Review | 16 | Sx: 16 | 3rd | Complications 5.9% for fetuses and 0% for mothers | -lower than previously described complications if Sx at 3rd trimester |
| Truong et al., 2008 [49] | Retrospective case series | 3 | Sx: 3 | 2nd and 3rd | No maternal, fetal, or neonatal complications | |
| Norman et al., 2009 [26] | Retrospective case series | 32/77 | Sx: 15 non-Sx: 62 | 2nd | Sx: 15/15 healthy infants non-Sx: 30/62 pregnancy loss | -Pregnancy loss x 3.5 higher -Pregnancy loss at late 1st or early 2nd trimester -Fetal loss associated with maternal Ca levels |
| DiMarco et al., 2019 [55] | Case series | 17 | Sx: 15 non-Sx: 2 | 2nd (n = 14) 3rd (n = 1) | Sx: 1 CS – 15/15 healthy infants non-Sx: 1 miscarriage – 1 IUGR/CS | |
| McMullen et al., 2010 [46] | Retrospective case series | 7 | Sx: 3 non-Sx: 4 | 2nd | Sx: 3/3 healthy infantnon-Sx: 1/4 pregnancy loss 3/4 preterm delivery | |
| Abood & Vestergaard, 2014 [27] | Register-based retrospective cohort study | 1057/NR | Sx: 576 Non-Sx: 481 | 2nd and 3rd | no difference in pregnancy outcomes between Sx and non-Sx | -no difference in pregnancy outcomes between women with PHPT and not -more SC in PHPT vs no-PHPT |
| Hirsch et al., 2015 [22] | Retrospective case series | 74/124 | Sx: 5 | NR | Pregnancy loss 12/124(9.7%) Preterm delivery 2/124(1.6%) Other complications 17/124(13.7%) Sx: 5/5 no maternal or infant complications | -no difference in complications between Sx and non-Sx women -no correlation between maternal Ca and pregnancy outcome |
| Gokkaya et al., 2016 [71] | Case series | 4 | Sx: 1 non-Sx: 3 | Sx: uncomplicated non-Sx: 1 uncomplicated 1 mother nephrolithiasis/SC 1 preterm SC/infant death | ||
| McCarthy et al., 2019 [50] | Case series | 3 | Sx: 3 | 2nd | 2 SC – all infants healthy | |
| Latif et al., 2020 [47] | Case series | 2 | Sx: 1 non-Sx: 1 | 3rd | Sx: uncomplicated non-Sx: preterm CS | |
| Sandler et al., 2021 [43] | Systematic review | 382 | Sx: 108 non-Sx: 274 | Mostly 2nd | Sx: 9/108 infant complications or death—0/108 surgical complications -infant complication rate lower in Sx vs. non-Sx (9.1 vs. 38.9%) | -complications less likely if Sx on the 2nd vs. 3rd trimester |
3.6. Management of Primary Hyperparathyroidism during Lactation
3.7. Hereditary Syndromes and Other Causes of Hypercalcemia
3.8. Hypoparathyroidism
3.9. Maternal and Fetal Complications of Hypoparathyroidism
3.10. Management of Hypoparathyroidism during Pregnancy
3.11. Management of Hypoparathyroidism during Lactation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooper, M.S. Disorders of calcium metabolism and parathyroid disease. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, C.S. Maternal mineral and bone metabolism during pregnancy, lactation, and post-weaning recovery. Physiol. Rev. 2016, 96, 449–547. [Google Scholar] [CrossRef] [Green Version]
- Leere, J.S.; Vestergaard, P. Calcium metabolic disorders in pregnancy: Primary hyperparathyroidism, pregnancy-induced osteoporosis, and vitamin D deficiency in pregnancy. Endocrinol. Metab. Clin. N. Am. 2019, 48, 643–655. [Google Scholar] [CrossRef]
- Diaz-Soto, G.; Linglart, A.; Sénat, M.V.; Kamenicky, P.; Chanson, P. Primary hyperparathyroidism in pregnancy. Endocrine 2013, 44, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Philbrick, W.M.; Wysolmerski, J.J.; Galbraith, S.; Holt, E.; Orloff, J.J.; Yang, K.H.; Vasavada, R.C.; Weir, E.C.; Broadus, A.E.; Stewart, A.F. Defining the roles of parathyroid hormone-related protein in normal physiology. Physiol. Rev. 1996, 76, 127–173. [Google Scholar] [CrossRef] [PubMed]
- Curtis, N.E.; Thomas, R.J.; Gillespie, M.T.; King, R.G.; Rice, G.E.; Wlodek, M.E. Parathyroid hormone-related protein (PTHrP) mRNA splicing and parathyroid hormone/PTHrP receptor mRNA expression in human placenta and fetal membranes. J. Mol. Endocrinol. 1998, 21, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, J.E., 2nd; Gorman, J.V.; Bruns, D.E.; Weir, E.C.; Burtis, W.J.; Martin, T.J.; Bruns, M.E. Abundant expression of parathyroid hormone-related protein in human amnion and its association with labor. Proc. Natl. Acad. Sci. USA 1992, 89, 8384–8388. [Google Scholar] [CrossRef] [Green Version]
- Karaplis, A.C.; Luz, A.; Glowacki, J.; Bronson, R.T.; Tybulewicz, V.L.; Kronenberg, H.M.; Mulligan, R.C. Lethal sleketal dysplasia from targeted disruption of the parathyroid hormone-related peptide gene. Genes Dev. 1994, 8, 277–289. [Google Scholar] [CrossRef] [Green Version]
- Miao, D.; Su, H.; He, B.; Gao, J.; Xia, Q.; Zhu, M.; Gu, Z.; Goltzman, D.; Karaplis, A.C. Severe growth retardation and early lethality in mice lacking the nuclear localization and C-terminus of PTH-related protein. Proc. Natl. Acad. Sci. USA 2008, 105, 20309–20314. [Google Scholar] [CrossRef] [Green Version]
- Horwitz, M.J.; Tedesco, M.B.; Sereika, S.M.; Hollis, B.W.; Garcia-Ocaña, A.; Stewart, A.F. Direct comparison of sustained infusion of human parathyroid hormone-related protein-(1-36) [hPTHTrP-(1-36)] versus hPTH- (1-34) on serum calcium, plasma 1,25-dihydroxyvitamin D concentrations, and fractional calcium excretion in healthy human volunteers. J. Clin. Endocrinol. Metab. 2003, 88, 1603–1609. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, C.S. The role of PTHrP in regulating mineral metabolism during pregnancy, lactation, and fetal/neonatal development. Clin. Rev. Bone Miner. Metab. 2014, 12, 142–164. [Google Scholar] [CrossRef]
- VanHouten, J.N.; Dann, P.; Stewart, A.F.; Watson, C.J.; Pollak, M.; Karaplis, A.C.; Wysolmerski, J.J. Mammary-specific deletion of parathyroid hormone-related protein preserves bone mass during lactation. J. Clin. Investig. 2003, 112, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Brembeck, P.; Lorentzon, M.; Ohlsson, C.; Winkvist, A.; Augustin, H. Changes in cortical volumetric bone mineral density and thickness, and trabecular thickness in lactating women postpartum. J. Clin. Endocrinol. Metab. 2015, 100, 535–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjjørnerem, Å.; Ghasem-Zadeh, A.; Wang, X.; Bui, M.; Walker, S.P.; Zebaze, R.; Seeman, E. Irreversible deterioration of cortical and trabecular microstructure associated with breastfeeding. J. Bone Miner. Res. 2017, 32, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Winter, E.M.; Ireland, A.; Butterfield, N.C.; Haffner-Luntzer, M.; Horcajada, M.N.; Veldhuis-Vlug, A.G.; Oei, L.; Colaianni, G.; Bonnet, N. Pregnancy and lactation, a challenge for the skeleton. Endocr. Connect. 2020, 9, R143–R157. [Google Scholar] [CrossRef] [PubMed]
- Hardcastle, S.A.; Yahya, F.; Bhalla, A.K. Pregnancy-associated osteoporosis: A UK case series and literature review. Osteoporos. Int. 2019, 30, 939–948. [Google Scholar] [CrossRef]
- Langdahl, B.L. Osteoporosis in premenopausal women. Curr. Opin. Rheumatol. 2017, 29, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.C.; Cusano, N.E.; Bilezikian, J.P. Primary hyperparathyroidism. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 593–607. [Google Scholar] [CrossRef] [Green Version]
- Kort, K.C.; Schiller, H.J.; Numann, P.J. Hyperparathyroidism and pregnancy. Am. J. Surg. 1999, 177, 66–68. [Google Scholar] [CrossRef]
- Richert, L.; Trombetti, A.; Herrmann, F.R.; Triponez, F.; Meier, C.; Robert, J.H.; Rizzoli, R. Age and gender distribution of primary hyperparathyroidism and incidence of surgical treatment in a European country with a particularly high life expectancy. Swiss Med. Wkly. 2009, 139, 400–404. [Google Scholar]
- DiMarco, A.; Christakis, I.; Constantinides, V.; Regan, L.; Palazzo, F.F. Undiagnosed primary hyperparathyroidism and recurrent miscarriage: The first prospective pilot study. World J. Surg. 2018, 42, 639–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, D.; Kopel, V.; Nadler, V.; Levy, S.; Toledano, Y.; Tsvetov, G. Pregnancy outcomes in women with primary hyperparathyroidism. J. Clin. Endocrinol. Metab. 2015, 100, 2115–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, T.R. Primary hyperparathyroidism during pregnancy. Surgery 1991, 110, 1028–1033. [Google Scholar] [PubMed]
- Shangold, M.M.; Dor, N.; Welt, S.I.; Fleischman, A.R.; Crenshaw, M.C., Jr. Hyperparathyroidism and pregnancy: A review. Obstet. Gynecol. Surv. 1982, 37, 217–228. [Google Scholar] [CrossRef]
- Ludwig, G.D. Hyperparathyroidism in relation to pregnancy. N. Engl. J. Med. 1962, 267, 637–642. [Google Scholar] [CrossRef]
- Norman, J.; Politz, D.; Politz, L. Hyperparathyroidism during pregnancy and the effect of rising calcium on pregnancy loss: A call for earlier intervention. Clin. Endocrinol. 2009, 71, 104–109. [Google Scholar] [CrossRef]
- Abood, A.; Vestergaard, P. Pregnancy outcomes in women with primary hyperparathyroidism. Eur. J. Endocrinol. 2014, 171, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Rigg, J.; Gilbertson, E.; Barrett, H.L.; Britten, F.L.; Lust, K. Primary hyperparathyroidism in pregnancy: Maternofetal outcomes at a quaternary referral obstetric hospital, 2000 through 2015. J. Clin. Endocrinol. Metab. 2019, 104, 721–729. [Google Scholar] [CrossRef] [Green Version]
- Carella, M.J.; Gossain, V.V. Hyperparathyroidism and pregnancy: Case report and review. J. Gen. Intern. Med. 1992, 7, 448–453. [Google Scholar] [CrossRef]
- Krysiak, R.; Wilk, M.; Okopien, B. Recurrent pancreatitis induced by hyperparathyroidism in pregnancy. Arch. Gynecol. Obstet. 2011, 284, 531–544. [Google Scholar] [CrossRef] [Green Version]
- Hong, M.K.; Hsieh, C.T.C.; Chen, B.H.; Tu, S.T.; Chou, P.H. Primary hyperparathyroidism and acute pancreatitis during the third trimester of pregnancy. J. Matern. Fetal. Med. 2001, 10, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Nagai, H.; Kasahara, K.; Kanazawa, K. Primary hyperparathyroidism and acute pancreatitis during pregnancy. Report of a case and a review of the English and Japanese literature. Int. J. Pancreatol. 1998, 24, 43–47. [Google Scholar] [PubMed]
- Hultin, H.; Hellman, P.; Lundgren, E.; Olovsson, M.; Ekbom, A.; Rastad, J.; Montgomery, S.M. Association of parathyroid adenoma and pregnancy with preeclampsia. J. Clin. Endocrinol. Metab. 2009, 94, 3394–3399. [Google Scholar] [CrossRef] [PubMed]
- Schnatz, P.F.; Curry, S.L. Primary hyperparathyroidism in pregnancy: Evidence-based management. Obstet. Gynecol. Surv. 2002, 57, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Nash, E.; Ranka, P.; Tarigopula, G.; Rashid, T. Primary hyperparathyroidism in pregnancy leading to hypercalcaemic crisis and uraemic encephalopathy. BMJ Case Rep. 2015, 2015, bcr2014208829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scholl, T.O.; Chen, X.; Stein, T.P. Maternal calcium metabolic stress and fetal growth. Am. J. Clin. Nutr. 2014, 99, 918–925. [Google Scholar] [CrossRef] [Green Version]
- Malekar-Raikar, S.; Sinnott, B.P. Primary hyperparathyroidism in pregnancy-a rare cause of life-threatening hypercalcemia: Case report and literature review. Case Rep. Endocrinol. 2011, 520516. [Google Scholar] [CrossRef]
- Korkmaz, H.A.; Ozkan, B.; Terek, D.; Dizdarer, C.; Arslanoğlu, S. Neonatal seizure as a manifestation of unrecognised maternal hyperparathyroidism. J. Clin. Res. Pediatr. Endocrinol. 2013, 5, 206–208. [Google Scholar]
- Cemeroglu, A.P.; Böber, E.; Büyükgebiz, A. Prolonged hypocalcemia in a 2 month-old boy unmasking maternal diagnosis of primary hyperparathyroidism. J. Pediatr. Endocrinol Metab. 2001, 14, 785–787. [Google Scholar] [CrossRef]
- Wagner, G.; Transbøl, I.; Melchior, J.C. Hyperparathyroidism and pregnancy. Acta Endocrinol. 1964, 47, 549–564. [Google Scholar] [CrossRef]
- Çakir, U.; Alan, S.; Erdeve, Ö.; Atasay, B.; Şıklar, Z.; Berberoğlu, M.; Arslan, S. Late neonatal hypocalcemic tetany as a manifestation of unrecognised maternal primary hyperparathyroidism. Turk. J. Pediatr. 2013, 55, 438–440. [Google Scholar] [PubMed]
- Pieringer, H.; Hatzl-Griesenhofer, M.; Shebl, O.; Wiesinger-Eidenberger, G.; Maschek, W.; Biesenbach, G. Hypocalcemic tetany in the newborn as a manifestation of unrecognized maternal primary hyperparathyroidism. Wien. Klin. Wochenschr. 2007, 119, 129–131. [Google Scholar] [CrossRef]
- Sandler, M.L.; Ho, R.; Xing, M.H.; Gidumal, S.; Spitzer, H.; Levy, J.C.; Chai, R.L. Primary hyperparathyroidism during pregnancy treated with parathyroidectomy: A systematic review. Laryngoscope 2021. [Google Scholar] [CrossRef]
- Kristoffersson, A.; Dahlgren, S.; Lithner, F.; Järhult, J. Primary hyperparathyroidism in pregnancy. Surgery 1985, 97, 326–330. [Google Scholar] [CrossRef]
- Owen, R.P.; Chou, K.J.; Silver, C.E.; Beilin, Y.; Tang, J.J.; Yanagisawa, R.T.; Rinaldo, A.; Shaha, A.R.; Ferlito, A. Thyroid and parathyroid surgery in pregnancy. Eur. Arch. Otorhinolaryngol. 2010, 267, 1825–1835. [Google Scholar] [CrossRef]
- McMullen, T.P.W.; Learoyd, D.L.; Williams, D.C.; Sywak, M.S.; Sidhu, S.B.; Delbridge, L.W. Hyperparathyroidism in pregnancy: Options for localization and surgical therapy. World J. Surg. 2010, 34, 1811–1816. [Google Scholar] [CrossRef] [PubMed]
- Latif, A.; Gastelum, A.A.; Farhan, K.; Jagadesh, S.; Mutnuri, S. Treatment approach for primary hyperparathyroidism in pregnancy. Bayl. Univ. Med. Cent. Proc. 2020, 34, 191–193. [Google Scholar] [CrossRef]
- Som, M.; Stroup, J.S. Primary hyperparathyroidism and pregnancy. Bayl. Univ. Med. Cent. Proc. 2016, 29, 214–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Truong, M.T.; Lalakea, M.L.; Robbins, P.; Friduss, M. Primary hyperparathyroidism in pregnancy: A case series and review. Laryngoscope 2008, 118, 1966–1969. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, A.; Howarth, S.; Khoo, S.; Hale, J.; Oddy, S.; Halsall, D.; Fish, B.; Mariathasan, S.; Andrews, K.; Oyibo, S.O.; et al. Management of primary hyperparathyroidism in pregnancy: A case series. Endocrinol. Diabetes Metab. Case Rep. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedbäck, G.M.; Odén, A.S. Cardiovascular disease, hypertension and renal function in primary hyperparathyroidism. J. Intern. Med. 2002, 251, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Schnatz, P.F.; Thaxton, S. Parathyroidectomy in the third trimester of pregnancy. Obstet. Gynecol. Surv. 2005, 60, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.Y.; Chang, C.C.; Tsai, H.D.; Yang, T.C.; Chiu, T.H.; Tsai, C.H. Primary hyperparathyroidism in pregnancy—Report of 3 cases. Arch. Gynecol. Obstet. 1998, 261, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Gidiri, M.; Lindow, S.W.; Masso, E.A.; Philips, K. Parathyroidectomy in pregnancy for primary hyperparathyroidism with successful pregnancy outcome: A report of two pregnancies. J. Obstet. Gynaecol. 2004, 24, 318–319. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, A.N.; Meeran, K.; Christakis, I.; Sodhi, V.; Nelson-Piercy, C.; Tolley, N.S.; Palazzo, F.F. Seventeen cases of primary hyperparathyroidism in pregnancy: A call for management guidelines. J. Endocr. Soc. 2019, 3, 1009–1021. [Google Scholar] [CrossRef] [Green Version]
- Pothiwala, P.; Levine, S.L. Parathyroid surgery in pregnancy: Review of the literature and localization by aspiration for parathyroid hormone levels. J. Perinatol. 2009, 29, 779–784. [Google Scholar] [CrossRef] [Green Version]
- Udelsman, R.; Lin, Z.; Donovan, P. The superiority of minimally invasive parathyroidectomy based on 1650 consecutive patients with primary hyperparathyroidism. Ann. Surg. 2011, 253, 585–591. [Google Scholar] [CrossRef]
- Stringer, K.M.; Gough, J.; Gough, I.R. Primary hyperparathyroidism during pregnancy: Management by minimally invasive surgery based on ultrasound localization. ANZ J. Surg. 2017, 87, E134–E137. [Google Scholar] [CrossRef] [PubMed]
- Bendinelli, C.; Nebauer, S.; Quach, T.; Mcgrath, S.; Acharya, S. Is minimally invasive parathyroid surgery an option for patients with gestational primary hyperparathyroidism? BMC Pregnancy Childbirth 2013, 13, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitetta, G.M.; Neri, P.; Chiecchio, A.; Carriero, A.; Cirillo, S.; Mussetto, A.B.; Codegone, A. Role of ultrasonography in the management of patients with primary hyperparathyroidism: Retrospective comparison with technetium-99m sestamibi scintigraphy. J. Ultrasound 2014, 17, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.Y.; Lang, B.H.; Chan, W.F.; Kung, A.W.; Lam, K.S. A prospective evaluation of preoperative localization by technetium-99m sestamibi scintigraphy and ultrasonography in primary hyperparathyroidism. Am. J. Surg. 2007, 193, 155–159. [Google Scholar] [CrossRef]
- Abraham, D.; Sharma, P.K.; Bentz, J.; Gault, P.M.; Neumayer, L.; McClain, D.A. Utility of ultrasound-guided fine-needle aspiration of parathyroid adenomas for localization before minimally invasive parathyroidectomy. Endocr. Pract. 2007, 13, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Erbil, Y.; Salmaslioğlu, A.; Kabul, E.; Işsever, H.; Tunaci, M.; Adalet, I.; Bozbora, A.; Ozarmağan, S. Use of preoperative parathyroid fine-needle aspiration and parathormone assay in the primary hyperparathyroidism with concomitant thyroid nodules. Am. J. Surg. 2007, 193, 665–671. [Google Scholar] [CrossRef]
- Zhang, X.; Xu, N.; Wu, Y.; Huang, B.; Liu, X.; Yuan, F. Novel approaches for the management of primary hyperparathyroidism during pregnancy. Clin. Endocrinol. 2018, 89, 526–527. [Google Scholar] [CrossRef] [PubMed]
- Norton, K.S.; Johnson, L.W.; Griffen, F.D.; Burke, J.; Kennedy, S.; Aultman, D.; Li, B.D.; Zibari, G. The sestamibi scan as a preoperative screening tool. Am. Surg. 2002, 68, 812–815. [Google Scholar] [PubMed]
- Gilbert, W.M.; Newman, P.S.; Eby-Wilkens, E.; Brace, R.A. Technetium Tc 99m rapidly crosses the ovine placenta and intramembranous pathway. Am. J. Obstet. Gynecol. 1996, 175, 1557–1562. [Google Scholar] [CrossRef]
- Michaud, L.; Balogova, S.; Burgess, A.; Ohnona, J.; Huchet, V.; Kerrou, K.; Lefèvre, M.; Tassart, M.; Montravers, F.; Périé, S.; et al. A pilot comparison of 18F-fluorocholine PET/CT, ultrasonography and 123I/99mTc-sestaMIBI dual-phase dual-isotope scintigraphy in the preoperative localization of hyperfunctioning parathyroid glands in primary or secondary hyperparathyroidism: Influence of thyroid anomalies. Medicine 2015, 94, e1701. [Google Scholar]
- Hu, Y.; Cui, M.; Sun, Z.; Su, Z.; Gao, X.; Liao, Q.; Zhao, Y. Clinical presentation, management, and outcomes of primary hyperparathyroidism during pregnancy. Int. J. Endocrinol. 2017, 2017, 3947423. [Google Scholar] [CrossRef] [Green Version]
- Vignali, E.; Picone, A.; Materazzi, G.; Steffe, S.; Berti, P.; Cianferotti, L.; Cetani, F.; Ambrogini, E.; Miccoli, P.; Pinchera, A.; et al. A quick intraoperative parathyroid hormone assay in the surgical management of patients with primary hyperparathyroidism: A study of 206 consecutive cases. Eur. J. Endocrinol. 2002, 146, 783–788. [Google Scholar] [CrossRef] [Green Version]
- Gelister, J.S.; Sanderson, J.D.; Chapple, C.R.; O’Riordan, J.L.; Cowie, A.G.; Milroy, E.J. Management of hyperparathyroidism in pregnancy. Br. J. Surg. 1989, 76, 1207–1208. [Google Scholar] [CrossRef]
- Gokkaya, N.; Gungor, A.; Bilen, A.; Bilen, H.; Gviniashvili, D.; Karadeniz, Y. Primary hyperparathyroidism in pregnancy: A case series and literature review. Gynecol. Endocrinol. 2016, 32, 783–786. [Google Scholar] [CrossRef]
- Dochez, V.; Ducarme, G. Primary hyperparathyroidism during pregnancy. Arch. Gynecol. Obstet. 2015, 291, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Djokanovic, N.; Klieger-Grossmann, C.; Koren, G. Does treatment with bisphosphonates endanger the human pregnancy? J. Obstet. Gynaecol. Can. 2008, 30, 505–507. [Google Scholar] [CrossRef]
- Patlas, N.; Golomb, G.; Yaffe, P.; Pinto, T.; Breuer, E.; Ornoy, A. Transplacental effects of bisphosphonates on fetal skeletal ossification and mineralization in rats. Teratology 1999, 60, 68–73. [Google Scholar] [CrossRef]
- Levy, S.; Fayez, I.; Taguchi, N.; Han, J.Y.; Aiello, J.; Matsui, D.; Moretti, M.; Koren, G.; Ito, S. Pregnancy outcome following in utero exposure to bisphosphonates. Bone 2009, 44, 428–430. [Google Scholar] [CrossRef] [PubMed]
- Vera, L.; Oddo, S.; Di Iorgi, N.; Bentivoglio, G.; Giusti, M. Primary hyperparathyroidism in pregnancy treated with cinacalcet: A case report and review of the literature. J. Med. Case Rep. 2016, 10, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marotta, V.; Di Somma, C.; Rubino, M.; Sciammarella, C.; Del Prete, M.; Marciello, F.; Ramundo, V.; Circelli, L.; Buonomano, P.; Modica, R.; et al. Potential role of cinacalcet hydrochloride in sporadic primary hyperparathyroidism without surgery indication. Endocrine 2015, 49, 274–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovacs, C.S.; Ho-Pao, C.L.; Hunzelman, J.L.; Lanske, B.; Fox, J.; Seidman, J.G.; Seidman, C.E.; Kronenberg, H.M. Regulation of murine fetal-placental calcium metabolism by the calcium-sensing receptor. J. Clin. Investig. 1998, 101, 2812–2820. [Google Scholar] [CrossRef] [PubMed]
- Boyce, R.W.; Varela, A.; Chouinard, L.; Bussiere, J.L.; Chellman, G.J.; Ominsky, M.S.; Pyrah, I.T. Infant cynomolgus monkeys exposed to denosumab in utero exhibit an osteoclast-poor osteopetrotic-like skeletal phenotype at birth and in the early postnatal period. Bone 2014, 64, 314–325. [Google Scholar] [CrossRef]
- Okamatsu, N.; Sakai, N.; Karakawa, A.; Kouyama, N.; Sato, Y.; Inagaki, K.; Kiuchi, Y.; Oguchi, K.; Negishi-Koga, T.; Takami, M. Biological effects of anti-RANKL antibody administration in pregnant mice and their newborns. Biochem. Biophys. Res. Commun. 2017, 491, 614–621. [Google Scholar] [CrossRef]
- Winter, E.M.; Appelman-Dijkstra, N.M. Parathyroid hormone-related protein-induced hypercalcemia of pregnancy successfully reversed by a dopamine agonist. J. Clin. Endocrinol. Metab. 2017, 102, 4417–4420. [Google Scholar] [CrossRef]
- Khosla, S.; van Heerden, J.A.; Gharib, H.; Jackson, I.T.; Danks, J.; Hayman, J.A.; Martin, T.J. Parathyroid hormone-related protein and hypercalcemia secondary to massive mammary hyperplasia. N. Engl. J. Med. 1990, 322, 1157. [Google Scholar]
- Jackson, I.T.; Saleh, J.; van Heerden, J.A. Gigantic mammary hyperplasia in pregnancy associated with pseudohyperparathyroidism. Plast. Reconstr. Surg. 1989, 84, 806–810. [Google Scholar] [CrossRef]
- Appelman-Dijkstra, N.M.; Ertl, D.A.; Zillikens, M.C.; Rjenmark, L.; Winter, E.M. Hypercalcemia during pregnancy: Management and outcomes for mother and child. Endocrine 2021, 71, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Hanley, D.A.; Rizzoli, R.; Bollerslev, J.; Young, J.E.; Rejnmark, L.; Thakker, R.; D’Amour, P.; Paul, T.; Van Uum, S.; et al. Primary hyperparathyroidism: Review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos. Int. 2017, 28, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marini, F.; Cianferotti, L.; Giusti, F.; Brandi, M.L. Molecular genetics in primary hyperparathyroidism: The role of genetic tests in differential diagnosis, disease prevention strategy, and therapeutic planning. A 2017 update. Clin. Cases Miner. Bone Metab. 2017, 14, 60–70. [Google Scholar] [CrossRef]
- Hannan, F.M.; Thakker, R.V. Calcium-sensing receptor (CaSR) mutations and disorders of calcium, electrolyte and water metabolism. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.R.; Hare, M.J.; Brown, J.; Yang, J.; Meyer, C.; Milat, F.; Allan, C.A. Familial hypocalciuric hypercalcemia in pregnancy: Diagnostic pitfalls. JBMR Plus 2020, 4, e10362. [Google Scholar] [CrossRef] [PubMed]
- Ghaznavi, S.A.; Saad, N.M.; Donovan, L.E. The biochemical profile of familial hypocalciuric hypercalcemia and primary hyperparathyroidism during pregnancy and lactation: Two case reports and review of the literature. Case Rep. Endocrinol. 2016, 2725486. [Google Scholar] [CrossRef] [Green Version]
- Maltese, G.; Izatt, L.; McGowan, B.M.; Hafeez, K.; Hubbard, J.G.; Carroll, P.V. Making (mis) sense of asymptomatic marked hypercalcemia in pregnancy. Clin. Case Rep. 2017, 5, 1587–1590. [Google Scholar] [CrossRef] [Green Version]
- Walker, A.; Fraile, J.J.; Hubbard, J.G. “Parathyroidectomy in pregnancy”-a single centre experience with review of evidence and proposal for treatment algorithm. Gland Surg. 2014, 3, 158–164. [Google Scholar] [PubMed]
- Powell, B.R.; Buist, N.R. Late presenting, prolonged hypocalcemia in an infant of a woman with hypocalciuric hypercalcemia. Clin. Pediatr. 1990, 29, 241–243. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.R.; Bennett, J.D. Symptomatic hypocalcemia and hypoparathyroidism in two infants of mothers with hyperparathyroidism and familial benign hypercalcemia. J. Perinatol. 1995, 15, 23–26. [Google Scholar] [PubMed]
- Hundahl, S.A.; Fleming, I.D.; Fremgen, A.M.; Menck, H.R. Two hundred eighty-six cases of parathyroid carcinoma treated in the U.S. between 1985–1995: A national cancer data base report. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer 1999, 86, 538–544. [Google Scholar] [CrossRef]
- Christmas, T.J.; Chapple, C.R.; Noble, J.G.; Milroy, E.J.; Cowie, A.G. Hyperparathyroidism after neck irradiation. Br. J. Surg. 1988, 75, 873–874. [Google Scholar] [CrossRef]
- Boyle, N.H.; Ogg, C.S.; Hartley, R.B.; Owen, W.J. Parathyroid carcinoma secondary to prolonged hyperplasia in chronic renal failure and in coeliac disease. Eur. J. Surg. Oncol. 1999, 25, 100–103. [Google Scholar]
- Howell, V.M.; Haven, C.J.; Kahnoski, K.; Khoo, S.K.; Petillo, D.; Chen, J.; Fleuren, G.J.; Robinson, B.G.; Delbridge, L.W.; Philips, J.; et al. HRPT2 mutations are associated with malignancy in sporadic parathyroid tumours. J. Med. Genet. 2003, 40, 657–663. [Google Scholar] [CrossRef] [Green Version]
- Paul, R.G.; Elston, M.S.; Gill, A.J.; Marsh, D.; Beer, I.; Wolmarans, L.; Conaglen, J.V.; Meyer-Rochow, G.Y. Hypercalcaemia due to parathyroid carcinoma presenting in the third trimester of pregnancy. Aust. N. Z. J. Obstet. Gynaecol. 2012, 52, 204–207. [Google Scholar] [CrossRef]
- Montoro, M.N.; Paler, R.J.; Goodwin, T.M.; Mestman, J.H. Parathyroid carcinoma during pregnancy. Obstet. Gynecol. 2000, 96, 841. [Google Scholar] [PubMed]
- Parham, G.P.; Orr, J.W. Hyperparathyroidism secondary to parathyroid carcinoma in pregnancy. A case report. J. Reprod. Med. 1987, 32, 123–125. [Google Scholar]
- Hess, H.M.; Dickson, J.; Fox, H.E. Hyperfunctioning parathyroid carcinoma presenting as acute pancreatitis in pregnancy. J. Reprod. Med. 1980, 25, 83–87. [Google Scholar]
- Panchani, R.; Varma, T.; Goyal, A.; Tripathi, S. Parathyroid carcinoma masquerading as morning sickness in pregnancy. Indian J. Endocrinol. Metab. 2013, 17, S198–S200. [Google Scholar] [CrossRef]
- Baretić, M.; Tomić Brzac, H.; Dobrenić, M.; Jakovčević, A. Parathyroid carcinoma in pregnancy. World J. Clin. Cases 2014, 16, 151–156. [Google Scholar] [CrossRef]
- Nadarasa, K.; Bailey, M.; Chahal, H.; Raja, O.; Bhat, R.; Gayle, C.; Grossman, A.B.; Druce, M.R. The use of cinacalcet in pregnancy to treat a complex case of parathyroid carcinoma. Endocrinol. Diabetes Metab. Case Rep. 2014, 2014, 140056. [Google Scholar] [CrossRef]
- Sato, K. Hypercalcemia during pregnancy, puerperium, and lactation: Review and a case report of hypercalcemic crisis after delivery due to excessive production of PTH-related protein (PTHrP) without malignancy (humoral hypercalcemia of pregnancy). Endocr. J. 2008, 55, 959–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eller-Vainicher, C.; Ossola, M.W.; Beck-Peccoz, P.; Chiodini, I. PTHrP-associated hypercalcemia of pregnancy resolved after delivery: A case report. Eur. J. Endocrinol. 2012, 166, 753–756. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, T.O. CYP24A1 loss of function: Clinical phenotype of monoallelic and biallelic mutations. J. Steroid Biochem. Mol. Biol. 2017, 173, 337–340. [Google Scholar] [CrossRef]
- McBride, L.; Houlihan, C.; Quinlan, C.; Messazos, B.; Stark, Z.; Crosthwaite, A. Outcomes following treatment of maternal hypercalcemia due to CYP24A1 pathogenic variants. Kidney Int. Rep. 2019, 4, 888–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, G.N.; Saitman, A.; Gao, H.; Clarke, N.J.; Fitzgerald, R.L.; Chi, N.W. A young woman with recurrent gestational hypercalcemia and acute pancreatitis caused by CYP24A1 deficiency. J. Bone Miner. Res. 2016, 31, 1841–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwong, W.T.; Fehmi, S.M. Hypercalcemic pancreatitis triggered by pregnancy with a CYP24A1 mutation. Pancreas 2016, 45, e31–e32. [Google Scholar] [CrossRef]
- Arnold, N.; O’Toole, V.; Huynh, T.; Smith, H.C.; Luxford, C.; Clifton-Bligh, R.; Eastman, C.J. Intractable hypercalcaemia during pregnancy and the postpartum secondary to pathogenic variants in CYP24A1. Endocrinol. Diabetes Metab. Case Rep. 2019, 2019, 19-0114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedberg, F.; Pilo, C.; Wikner, J.; Törring, O.; Calissendorff, J. Three sisters with heterozygous gene variants of CYP24A1: Maternal hypercalcemia, new-Onset hypertension, and neonatal hypoglycemia. J. Endocr. Soc. 2018, 3, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Almaghamsi, A.; Almalki, M.H.; Buhary, B.M. Hypocalcemia in pregnancy: A clinical review update. Oman Med. J. 2018, 33, 453–462. [Google Scholar] [CrossRef]
- Glass, E.J.; Barr, D.G. Transient neonatal hyperparathyroidism secondary to maternal pseudohypoparathyroidism. Arch. Dis. Child 1981, 56, 565–568. [Google Scholar] [CrossRef]
- Mannstadt, M.; Bilezikian, J.P.; Thakker, R.V.; Hannan, F.M.; Clarke, B.L.; Rejnmark, L.; Mitchell, D.M.; Vokes, T.J.; Winer, K.K.; Shoback, D.M. Hypoparathyroidism. Nat. Rev. Dis. Primers 2017, 3, 17055. [Google Scholar] [CrossRef] [PubMed]
- Bilezikian, J.P.; Khan, A.; Potts, J.T., Jr.; Brandi, M.L.; Clarke, B.L.; Shoback, D.; Jüppner, H.; D’Amour, P.; Fox, J.; Rejnmark, L.; et al. Hypoparathyroidism in the adult: Epidemiology, diagnosis, pathophysiology, target-organ involvement, treatment, and challenges for future research. J. Bone Miner. Res. 2011, 26, 2317–2337. [Google Scholar] [CrossRef] [PubMed]
- Gimm, O. Thyroid cancer. Cancer Lett. 2001, 163, 143–156. [Google Scholar] [CrossRef]
- Tunbridge, W.M.; Evered, D.C.; Hall, R.; Appleton, D.; Brewis, M.; Clark, F.; Evans, J.G.; Young, E.; Bird, T.; Smith, P.A. The spectrum of thyroid disease in a community: The Whickham survey. Clin. Endocrinol. 1977, 7, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Eastell, R.; Edmonds, C.J.; de Chayal, R.C.; McFadyen, I.R. Prolonged hypoparathyroidism presenting eventually as second trimester abortion. Br. Med. J. (Clin. Res. Ed.) 1985, 291, 955–956. [Google Scholar] [CrossRef] [Green Version]
- Trotter, M.; Hixon, B.B. Sequential changes in weight, density, and percentage ash weight of human skeletons from an early fetal period through old age. Anat. Rec. 1974, 179, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Schauberger, C.W.; Pitkin, R.M. Maternal-perinatal calcium relationships. Obstet. Gynecol. 1979, 53, 74–76. [Google Scholar]
- David, L.; Anast, C.S. Calcium metabolism in newborn infants. The interrelationship of parathyroid function and calcium, magnesium, and phosphorus metabolism in normal, “sick”, and hypocalcemic newborns. J. Clin. Investig. 1974, 54, 287–296. [Google Scholar] [CrossRef]
- Saggese, G.; Baroncelli, G.I.; Bertelloni, S.; Cipolloni, C. Intact parathyroid hormone levels during pregnancy, in healthy term neonates and in hypocalcemic preterm infants. Acta Paediatr. 1991, 80, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Aceto, T., Jr.; Batt, R.E.; Bruck, E.; Schultz, R.B.; Perz, Y.R. Intrauterine hyperparathyroidism: A complication of untreated maternal hypoparathyroidism. J. Clin. Endocrinol. Metab. 1966, 26, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Bronsky, D.; Kiamko, R.T.; Moncada, R.; Rosenthal, I.M. Intra-uterine hyperparathyroidism secondary to maternal hypoparathyroidism. Pediatrics 1968, 42, 606–613. [Google Scholar]
- Alikasifoglu, A.; Gonc, E.N.; Yalcin, E.; Dogru, D.; Yordam, N. Neonatal hyperparathyroidism due to maternal hypoparathyroidism and vitamin D deficiency: A cause of multiple bone fractures. Clin. Pediatr. 2005, 44, 267–269. [Google Scholar] [CrossRef]
- Callies, F.; Arlt, W.; Scholz, H.J.; Reincke, M.; Allolio, B. Management of hypoparathyroidism during pregnancy—Report of twelve cases. Eur. J. Endocrinol. 1998, 139, 284–289. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, J.A.; Klainer, L.M.; Neuwirth, R.S. The management of hypoparathyroidism in pregnancy. Am. J. Obstet. Gynecol. 1966, 94, 1103–1107. [Google Scholar] [CrossRef]
- Salle, B.L.; Berthezene, F.; Glorieux, F.H.; Delvin, E.E.; Berland, M.; David, L.; Varenne, J.P.; Putet, G. Hypoparathyroidism during pregnancy: Treatment with calcitriol. J. Clin. Endocrinol. Metab. 1981, 52, 810–813. [Google Scholar] [CrossRef]
- Sadeghi-Nejad, A.; Wolfsdorf, J.I.; Senior, B. Hypoparathyroidism and pregnancy. Treatment with calcitriol. JAMA 1980, 243, 254–255. [Google Scholar] [CrossRef]
- Sweeney, L.L.; Malabanan, A.O.; Rosen, H. Decreased calcitriol requirement during pregnancy and lactation with a window of increased requirement immediately post partum. Endocr. Pract. 2010, 16, 459–462. [Google Scholar] [CrossRef]
- Caplan, R.H.; Wickus, G.G. Reduced calcitriol requirements for treating hypoparathyroidism during lactation. A case report. J. Reprod. Med. 1993, 38, 914–918. [Google Scholar] [PubMed]
- Hatswell, B.L.; Allan, C.A.; Teng, J.; Wong, P.; Ebeling, P.R.; Wallace, E.M.; Fuller, P.J.; Milat, F. Management of hypoparathyroidism in pregnancy and lactation—A report of 10 cases. Bone Rep. 2015, 3, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartogsohn, E.A.R.; Khan, A.A.; Kjaersulf, L.U.; Sikjaer, T.; Hussain, S.; Rejnmark, L. Changes in treatment needs of hypoparathyroidism during pregnancy and lactation: A case series. Clin. Endocrinol. 2020, 93, 261–268. [Google Scholar] [CrossRef]
- Khan, A.A.; Clarke, B.; Rejnmark, L.; Brandi, M.L. MANAGEMENT OF ENDOCRINE DISEASE: Hypoparathyroidism in pregnancy: Review and evidence-based recommendations for management. Eur. J. Endocrinol. 2019, 180, R37–R44. [Google Scholar] [CrossRef] [Green Version]
- Krysiak, R.; Kobielusz-Gembala, I.; Okopien, B. Hypoparathyroidism in pregnancy. Gynecol. Endocrinol. 2011, 27, 529–532. [Google Scholar] [CrossRef] [PubMed]
- Mather, K.J.; Chik, C.L.; Corenblum, B. Maintenance of serum calcium by parathyroid hormone-related peptide during lactation in a hypoparathyroid patient. J. Clin. Endocrinol. Metab. 1999, 84, 424–427. [Google Scholar] [CrossRef]
- Wright, A.D.; Joplin, G.F.; Dixon, H.G. Post-partum hypercalcaemia in treated hypoparathyroidism. Br. Med. J. 1969, 1, 23–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilany, J.; Vered, I.; Cohen, O. The effect of continuous subcutaneous recombinant PTH (1-34) infusion during pregnancy on calcium homeostasis—A case report. Gynecol. Endocrinol. 2013, 29, 807–810. [Google Scholar] [CrossRef]
- Kiattisunthorn, K.; Wutyam, K.; Indranoi, A.; Vasuvattakul, S. Randomized trial comparing pulse calcitriol and alfacalcidol for the treatment of secondary hyperparathyroidism in haemodialysis patients. Nephrology 2011, 16, 277–284. [Google Scholar] [CrossRef]
- Caplan, R.H.; Beguin, E.A. Hypercalcemia in a calcitriol-treated hypoparathyroid woman during lactation. Obstet. Gynecol. 1990, 76, 485–489. [Google Scholar] [PubMed]
- Rude, R.K.; Haussler, M.R.; Singer, F.R. Postpartum resolution of hypocalcemia in a lactating hypoparathyroid patient. Endocrinol. Jpn. 1984, 31, 227–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsourdi, E.; Anastasilakis, A.D. Parathyroid Disease in Pregnancy and Lactation: A Narrative Review of the Literature. Biomedicines 2021, 9, 475. https://doi.org/10.3390/biomedicines9050475
Tsourdi E, Anastasilakis AD. Parathyroid Disease in Pregnancy and Lactation: A Narrative Review of the Literature. Biomedicines. 2021; 9(5):475. https://doi.org/10.3390/biomedicines9050475
Chicago/Turabian StyleTsourdi, Elena, and Athanasios D. Anastasilakis. 2021. "Parathyroid Disease in Pregnancy and Lactation: A Narrative Review of the Literature" Biomedicines 9, no. 5: 475. https://doi.org/10.3390/biomedicines9050475
APA StyleTsourdi, E., & Anastasilakis, A. D. (2021). Parathyroid Disease in Pregnancy and Lactation: A Narrative Review of the Literature. Biomedicines, 9(5), 475. https://doi.org/10.3390/biomedicines9050475