
Perioperative Vascular Biomarker Profiling in Elective Surgery Patients Developing Postoperative Delirium: A Prospective Cohort Study

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Serum Sampling and Biomarker Profiling
2.3. Assessment of POD
2.4. Statistical and Bioinformatical Analysis
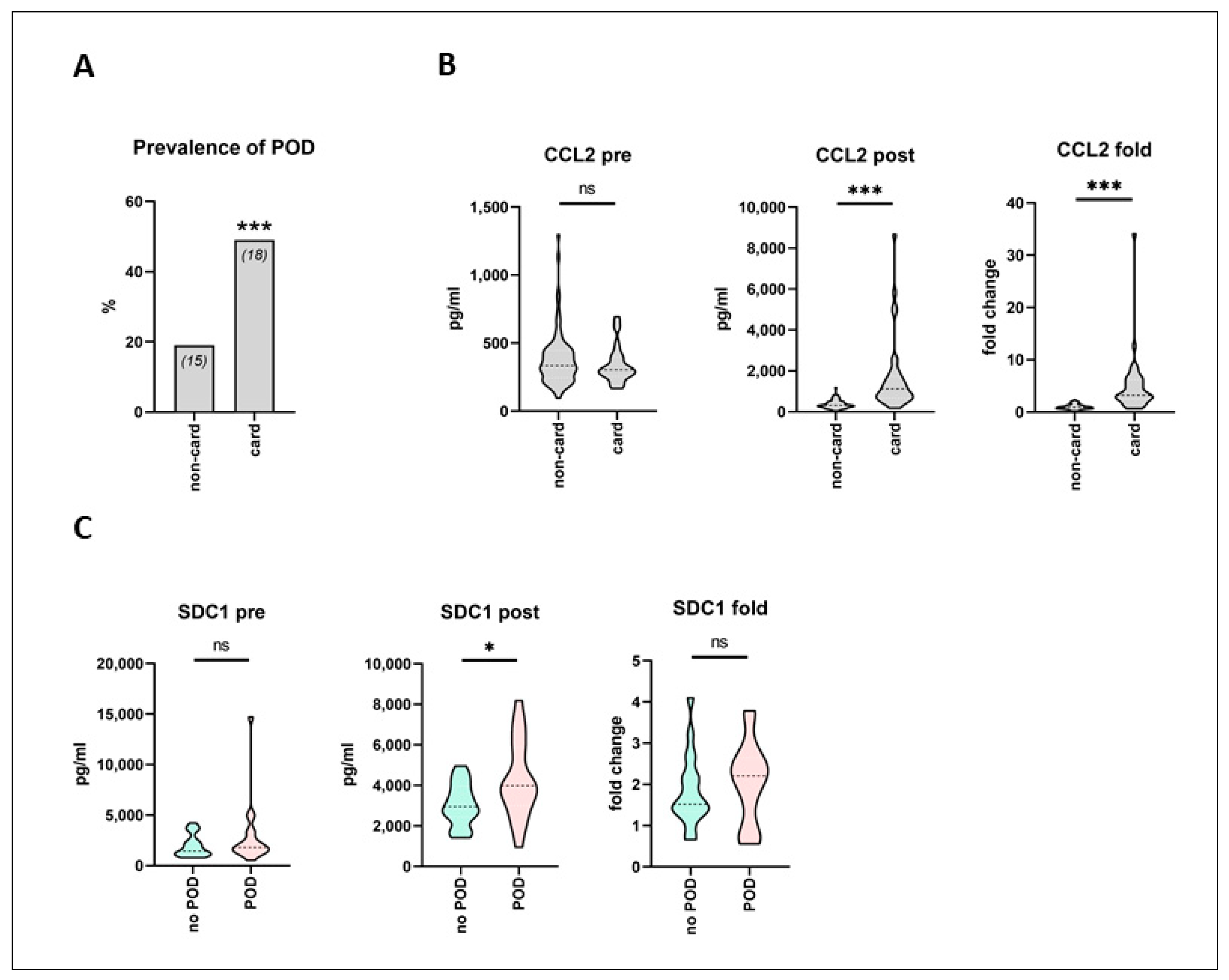
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jin, Z.; Hu, J.; Ma, D. Postoperative delirium: Perioperative assessment, risk reduction, and management. Br. J. Anaesth. 2020, 125, 492–504. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- Brown, C.H.; Laflam, A.; Max, L.; Lymar, D.; Neufeld, K.J.; Tian, J.; Shah, A.S.; Whitman, G.J.; Hogue, C.W. The Impact of Delirium After Cardiac Surgical Procedures on Postoperative Resource Use. Ann. Thorac. Surg. 2016, 101, 1663–1669. [Google Scholar] [CrossRef] [Green Version]
- Raats, J.W.; Van Eijsden, W.A.; Crolla, R.; Steyerberg, E.; Van Der Laan, L. Risk Factors and Outcomes for Postoperative Delirium after Major Surgery in Elderly Patients. PLoS ONE 2015, 10, e0136071. [Google Scholar] [CrossRef] [Green Version]
- Gleason, L.J.; Schmitt, E.M.; Kosar, C.M.; Tabloski, P.; Saczynski, J.S.; Robinson, T.N.; Cooper, Z.; Rogers, S.O.; Jones, R.N.; Marcantonio, E.R.; et al. Effect of Delirium and Other Major Complications on Outcomes After Elective Surgery in Older Adults. JAMA Surg. 2015, 150, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Van Meenen, L.C.C.; Van Meenen, D.M.P.; De Rooij, S.E.; Ter Riet, G. Risk Prediction Models for Postoperative Delirium: A Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2014, 62, 2383–2390. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yu, Y.; Zhu, S. Inflammatory markers in postoperative delirium (POD) and cognitive dysfunction (POCD): A meta-analysis of observational studies. PLoS ONE 2018, 13, e0195659. [Google Scholar] [CrossRef]
- Atterton, B.; Paulino, M.C.; Povoa, P.; Martin-Loeches, I. Sepsis Associated Delirium. Intensive Care Med. 2020, 56, 240. [Google Scholar] [CrossRef]
- Lee, W.L.; Liles, W.C. Endothelial activation, dysfunction and permeability during severe infections. Curr. Opin. Hematol. 2011, 18, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.G.; Pandharipande, P.P.; Thompson, J.L.; Chandrasekhar, R.; Ware, L.B.; Ely, E.W.; Girard, T.D. Endothelial Activation and Blood-Brain Barrier Injury as Risk Factors for Delirium in Critically Ill Patients. Crit. Care Med. 2016, 44, e809–e817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, A.V.; Liles, W.C. Biomarkers of endothelial activation/dysfunction in infectious diseases. Virulence 2013, 4, 507–516. [Google Scholar] [CrossRef] [Green Version]
- Rudolph, J.L.; Jones, R.N.; Rasmussen, L.S.; Silverstein, J.H.; Inouye, S.K.; Marcantonio, E.R. Independent Vascular and Cognitive Risk Factors for Postoperative Delirium. Am. J. Med. 2007, 120, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Thudium, M.; Ellerkmann, R.K.; Heinze, I.; Hilbert, T. Relative cerebral hyperperfusion during cardiopulmonary bypass is associated with risk for postoperative delirium: A cross-sectional cohort study. BMC Anesthesiol. 2019, 19, 35. [Google Scholar] [CrossRef] [PubMed]
- Menzenbach, J.; Guttenthaler, V.; Kirfel, A.; Ricchiuto, A.; Neumann, C.; Adler, L.; Kieback, M.; Velten, L.; Fimmers, R.; Mayr, A.; et al. Estimating patients’ risk for postoperative delirium from preoperative routine data—Trial design of the PRe-Operative prediction of postoperative DElirium by appropriate SCreening (PROPDESC) study—A monocentre prospective observational trial. Contemp. Clin. Trials Commun. 2020, 17, 100501. [Google Scholar] [CrossRef]
- Glance, L.G.; Lustik, S.J.; Hannan, E.L.; Osler, T.M.; Mukamel, D.B.; Qian, F.; Dick, A.W. The Surgical Mortality Probability Model: Derivation and Validation of a Simple Risk Prediction Rule for Noncardiac Surgery. Ann. Surg. 2012, 255, 696–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Birru, R.; Di, Y.P. Analysis of Clinical and Biological Samples Using Microsphere-Based Multiplexing Luminex System. Mol. Toxicol. Protoc. 2014, 1105, 43–57. [Google Scholar] [CrossRef]
- Guenther, U.; Popp, J.; Koecher, L.; Muders, T.; Wrigge, H.; Ely, E.W.; Putensen, C. Validity and Reliability of the CAM-ICU Flowsheet to diagnose delirium in surgical ICU patients. J. Crit. Care 2010, 25, 144–151. [Google Scholar] [CrossRef]
- Inouye, S.K.; Van Dyck, C.H.; Alessi, C.A.; Balkin, S.; Siegal, A.P.; Horwitz, R.I. Clarifying Confusion: The Confusion Assessment Method. A New Method for Detection of Delirium. Ann. Intern. Med. 1990, 113, 941–948. [Google Scholar] [CrossRef]
- Bellelli, G.; Morandi, A.; Davis, D.H.; Mazzola, P.; Turco, R.; Gentile, S.; Ryan, T.; Cash, H.; Guerini, F.; Torpilliesi, T.; et al. Validation of the 4AT, a new instrument for rapid delirium screening: A study in 234 hospitalised older people. Age Ageing 2014, 43, 496–502. [Google Scholar] [CrossRef] [Green Version]
- Schuurmans, M.J.; Shortridge-Baggett, L.M.; Duursma, S.A. The Delirium Observation Screening Scale: A Screening Instrument for Delirium. Res. Theory Nurs. Pract. 2003, 17, 31–50. [Google Scholar] [CrossRef]
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. Matching as Nonparametric Preprocessing for Reducing Model Dependence in Parametric Causal Inference. Political Anal. 2007, 15, 199–236. [Google Scholar] [CrossRef] [Green Version]
- Alam, A.; Hana, Z.; Jin, Z.; Suen, K.C.; Ma, D. Surgery, neuroinflammation and cognitive impairment. EBioMedicine 2018, 37, 547–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.; Johnson, D.K.; Carlson, S.; Hocum-Stone, L.; Kelly, R.F.; Gravely, A.A.; Mbai, M.; Green, D.L.; Santilli, S.; Garcia, S.; et al. NT-Pro BNP Predicts Myocardial Injury Post-vascular Surgery and is Reduced with CoQ10: A Randomized Double-Blind Trial. Ann. Vasc. Surg. 2020, 64, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Rodseth, R.N.; Biccard, B.M.; Chu, R.; Lurati Buse, G.A.; Thabane, L.; Bakhai, A.; Bolliger, D.; Cagini, L.; Cahill, T.J.; Cardinale, D.; et al. Postoperative B-Type Natriuretic Peptide for Prediction of Major Cardiac Events in Patients Undergoing Noncardiac Surgery: Systematic Review and Individual Patient Meta-Analysis. Anesthesiology 2013, 119, 270–283. [Google Scholar] [CrossRef] [Green Version]
- Raslau, D.; Bierle, D.M.; Stephenson, C.R.; Mikhail, M.A.; Kebede, E.B.; Mauck, K.F. Preoperative Cardiac Risk Assessment. Mayo Clin. Proc. 2020, 95, 1064–1079. [Google Scholar] [CrossRef] [Green Version]
- De Hert, S.; Staender, S.; Fritsch, G.; Hinkelbein, J.; Afshari, A.; Bettelli, G.; Bock, M.; Chew, M.S.; Coburn, M.; De Robertis, E.; et al. Pre-operative evaluation of adults undergoing elective noncardiac surgery: Updated guideline from the european society of anaesthesiology. Eur. J. Anaesthesiol. 2018, 35, 407–465. [Google Scholar] [CrossRef]
- Marković, D.Z.; Jevtović-Stoimenov, T.; Ćosić, V.; Stošić, B.; Živković, B.M.; Janković, R.J. Addition of biomarker panel improves prediction performance of American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) calculator for cardiac risk assessment of elderly patients preparing for major non-cardiac surgery: A pilot study. Aging Clin. Exp. Res. 2018, 30, 419–431. [Google Scholar] [CrossRef]
- Vasunilashorn, S.M.; Ngo, L.; Inouye, S.K.; Libermann, T.A.; Jones, R.N.; Alsop, D.C.; Guess, J.; Jastrzebski, S.; McElhaney, J.E.; Kuchel, G.; et al. Cytokines and Postoperative Delirium in Older Patients Undergoing Major Elective Surgery. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2015, 70, 1289–1295. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.-T.; Yeh, S.-L.; Wu, M.-S.; Lin, J.-T.; Lee, P.-H.; Liaw, K.-Y.; Chang, K.-J.; Chen, W.-J. Impact of surgery on local and systemic responses of cytokines and adhesion molecules. Hepatogastroenterology 2009, 56, 1341–1345. [Google Scholar] [PubMed]
- Klaschik, S.; Gehlen, J.; Neumann, C.; Keyver-Paik, M.-D.; Soehle, M.; Frede, S.; Velten, M.; Hoeft, A.; Hilbert, T. Network of Mediators for Vascular Inflammation and Leakage Is Dysbalanced during Cytoreductive Surgery for Late-Stage Ovarian Cancer. Mediat. Inflamm. 2019, 2019, 5263717. [Google Scholar] [CrossRef] [Green Version]
- Hilbert, T.; Duerr, G.D.; Hamiko, M.; Frede, S.; Rogers, L.; Baumgarten, G.; Hoeft, A.; Velten, M. Endothelial permeability following coronary artery bypass grafting: An observational study on the possible role of angiopoietin imbalance. Crit. Care Lond. Engl. 2016, 20, 51. [Google Scholar] [CrossRef] [Green Version]
- Shibasaki, H.; Furukawa, K.; Yamamori, H.; Kimura, F.; Tashiro, T.; Miyazaki, M. The Post-Operative Level of Serum Monocyte Chemoattractant Protein-1 and Its Correlation with the Severity of Surgical Stress. J. Surg. Res. 2006, 136, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Skrede, K.; Wyller, T.B.; Watne, L.O.; Seljeflot, I.; Juliebø, V. Is there a role for monocyte chemoattractant protein-1 in delirium? Novel observations in elderly hip fracture patients. BMC Res. Notes 2015, 8, 186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, J.; Vacas, S.; Terrando, N.; Yuan, M.; Sands, L.P.; Kramer, J.; Bozic, K.; Maze, M.M.; Leung, J.M. Perioperative cerebrospinal fluid and plasma inflammatory markers after orthopedic surgery. J. Neuroinflamm. 2016, 13, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, W.L.; Karpus, W.J.; Van Eldik, L.J. MCP-1-deficient mice show reduced neuroinflammatory responses and increased peripheral inflammatory responses to peripheral endotoxin insult. J. Neuroinflamm. 2008, 5, 35. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.; Oyeyemi, D.; Olurinde, M.O.; Whitson, H.E.; Weinhold, K.J.; Woldorff, M.G.; Lipsitz, L.A.; Moretti, E.; Giattino, C.M.; Roberts, K.C.; et al. The INTUIT Study: Investigating Neuroinflammation Underlying Postoperative Cognitive Dysfunction. J. Am. Geriatr. Soc. 2019, 67, 794–798. [Google Scholar] [CrossRef]
- Cereghetti, C.; Siegemund, M.; Schaedelin, S.; Fassl, J.; Seeberger, M.D.; Eckstein, F.S.; Steiner, L.A.; Goettel, N. Independent Predictors of the Duration and Overall Burden of Postoperative Delirium After Cardiac Surgery in Adults: An Observational Cohort Study. J. Cardiothorac. Vasc. Anesth. 2017, 31, 1966–1973. [Google Scholar] [CrossRef]
- Moledina, D.; Isguven, S.; McArthur, E.; Thiessen-Philbrook, H.; Garg, A.X.; Shlipak, M.; Whitlock, R.; Kavsak, P.A.; Coca, S.G.; Parikh, C.R.; et al. Plasma Monocyte Chemotactic Protein-1 Is Associated with Acute Kidney Injury and Death After Cardiac Operations. Ann. Thorac. Surg. 2017, 104, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Pesonen, E.; Passov, A.; Andersson, S.; Suojaranta, R.; Niemi, T.; Raivio, P.; Salmenperä, M.; Schramko, A. Glycocalyx Degradation and Inflammation in Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2019, 33, 341–345. [Google Scholar] [CrossRef] [Green Version]
- Bell, J.D.; Rhind, S.G.; Di Battista, A.P.; Macdonald, R.L.; Baker, A.J. Biomarkers of Glycocalyx Injury are Associated with Delayed Cerebral Ischemia Following Aneurysmal Subarachnoid Hemorrhage: A Case Series Supporting a New Hypothesis. Neurocrit. Care 2016, 26, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Kazmierski, J.; Banys, A.; Latek, J.; Bourke, J.; Jaszewski, R. Raised IL-2 and TNF-α concentrations are associated with postoperative delirium in patients undergoing coronary-artery bypass graft surgery. Int. Psychogeriatr. 2014, 26, 845–855. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Median (25th–75th Percentile) |
|---|---|
| Patient details: | |
| n | 118 |
| Age (years) | 71 (66–78) |
| Male gender (n [%]) | 70 (59) |
| Body mass index (kg/m2) | 27.3 (24.4–30.2) |
| ASA status: | |
| I (n [%]) | 3 (2.5) |
| II (n [%]) | 35 (29.7) |
| III (n [%]) | 70 (59.3) |
| IV (n [%]) | 10 (8.5) |
| Preoperative routine laboratory values: | |
| Hemoglobin (g/dL) | 13.4 (12.2–14.5) |
| HbA1C (%) | 5.6 (5.4–6.2) |
| Leukocyte count (G/L) | 6.9 (5.9–8.8) |
| Sodium (mmol/L) | 140 (138–142) |
| Potassium (mmol/L) | 4.4 (4.1–4.7) |
| Creatinine (mg/dL) | 0.9 (0.78–1.05) |
| C-reactive protein (mg/L) | 3.1 (1.1–8.8) |
| Total protein (g/L) | 69 (65–73) |
| High-sensitive cardiac troponin T (ng/L) | 12.9 (8.1–20.3) |
| NT-proBNP (pg/mL) | 235 (114–796) |
| Procedural and anesthesia details: | |
| Surgical risk: | |
| Low (n [%]) | 11 (9.3) |
| Intermediate (n [%]) | 47 (39.8) |
| High (n [%]) | 60 (50.9) |
| Surgical specialty: | |
| General (n [%]) | 18 (15) |
| Orthopedic and trauma (n [%]) | 35 (30) |
| Cardiac (n [%]) | 37 (31) |
| Thoracic (n [%]) | 2 (2) |
| Vascular (n [%]) | 4 (3) |
| Ear-nose-throat (n [%]) | 11 (9) |
| Urologic (n [%]) | 9 (8) |
| Plastic (n [%]) | 2 (2) |
| Placement of epidural catheter (n [%]) | 6 (5) |
| Duration of surgery (min) | 219 (136–298) |
| Duration of mechanical ventilation (h) | 6.0 (3.6–14.0) |
| Postoperative admission to ICU (n [%]) | 66 (55) |
| Length of hospital stay (days) | 13 (10–23) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menzenbach, J.; Frede, S.; Petras, J.; Guttenthaler, V.; Kirfel, A.; Neumann, C.; Mayr, A.; Wittmann, M.; Coburn, M.; Klaschik, S.; et al. Perioperative Vascular Biomarker Profiling in Elective Surgery Patients Developing Postoperative Delirium: A Prospective Cohort Study. Biomedicines 2021, 9, 553. https://doi.org/10.3390/biomedicines9050553
Menzenbach J, Frede S, Petras J, Guttenthaler V, Kirfel A, Neumann C, Mayr A, Wittmann M, Coburn M, Klaschik S, et al. Perioperative Vascular Biomarker Profiling in Elective Surgery Patients Developing Postoperative Delirium: A Prospective Cohort Study. Biomedicines. 2021; 9(5):553. https://doi.org/10.3390/biomedicines9050553
Chicago/Turabian StyleMenzenbach, Jan, Stilla Frede, Janine Petras, Vera Guttenthaler, Andrea Kirfel, Claudia Neumann, Andreas Mayr, Maria Wittmann, Mark Coburn, Sven Klaschik, and et al. 2021. "Perioperative Vascular Biomarker Profiling in Elective Surgery Patients Developing Postoperative Delirium: A Prospective Cohort Study" Biomedicines 9, no. 5: 553. https://doi.org/10.3390/biomedicines9050553
APA StyleMenzenbach, J., Frede, S., Petras, J., Guttenthaler, V., Kirfel, A., Neumann, C., Mayr, A., Wittmann, M., Coburn, M., Klaschik, S., & Hilbert, T. (2021). Perioperative Vascular Biomarker Profiling in Elective Surgery Patients Developing Postoperative Delirium: A Prospective Cohort Study. Biomedicines, 9(5), 553. https://doi.org/10.3390/biomedicines9050553