
Addition of V-Stage to Conventional TNM Staging to Create the TNVM Staging System for Accurate Prediction of Prognosis in Colon Cancer: A Multi-Institutional Retrospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Study Design
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Baseline Patient Characteristics According to the Study Groups
3.3. Univariate and Multivariate Analyses
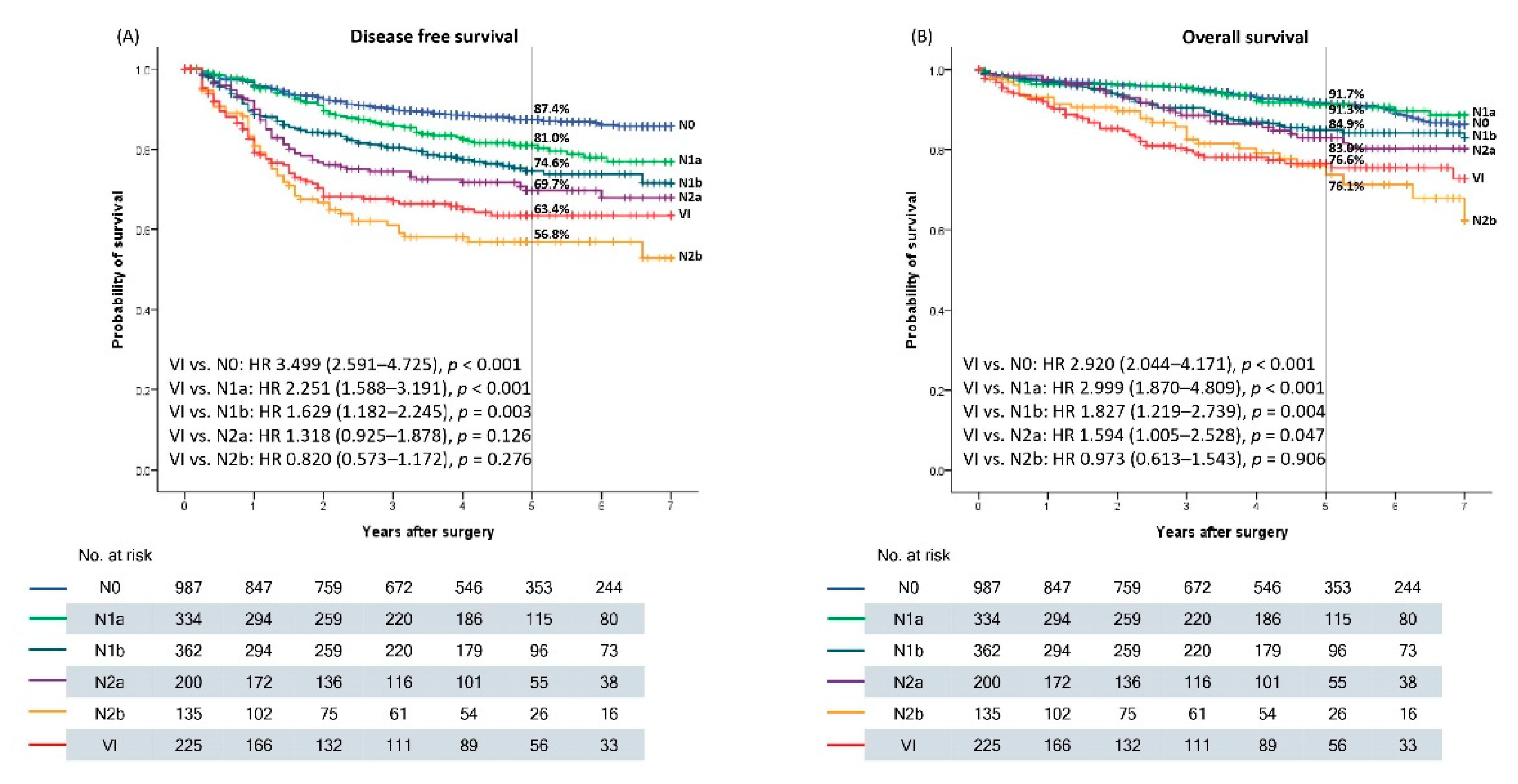
3.4. Recurrence and Survival Outcome according to the N Stage and VI
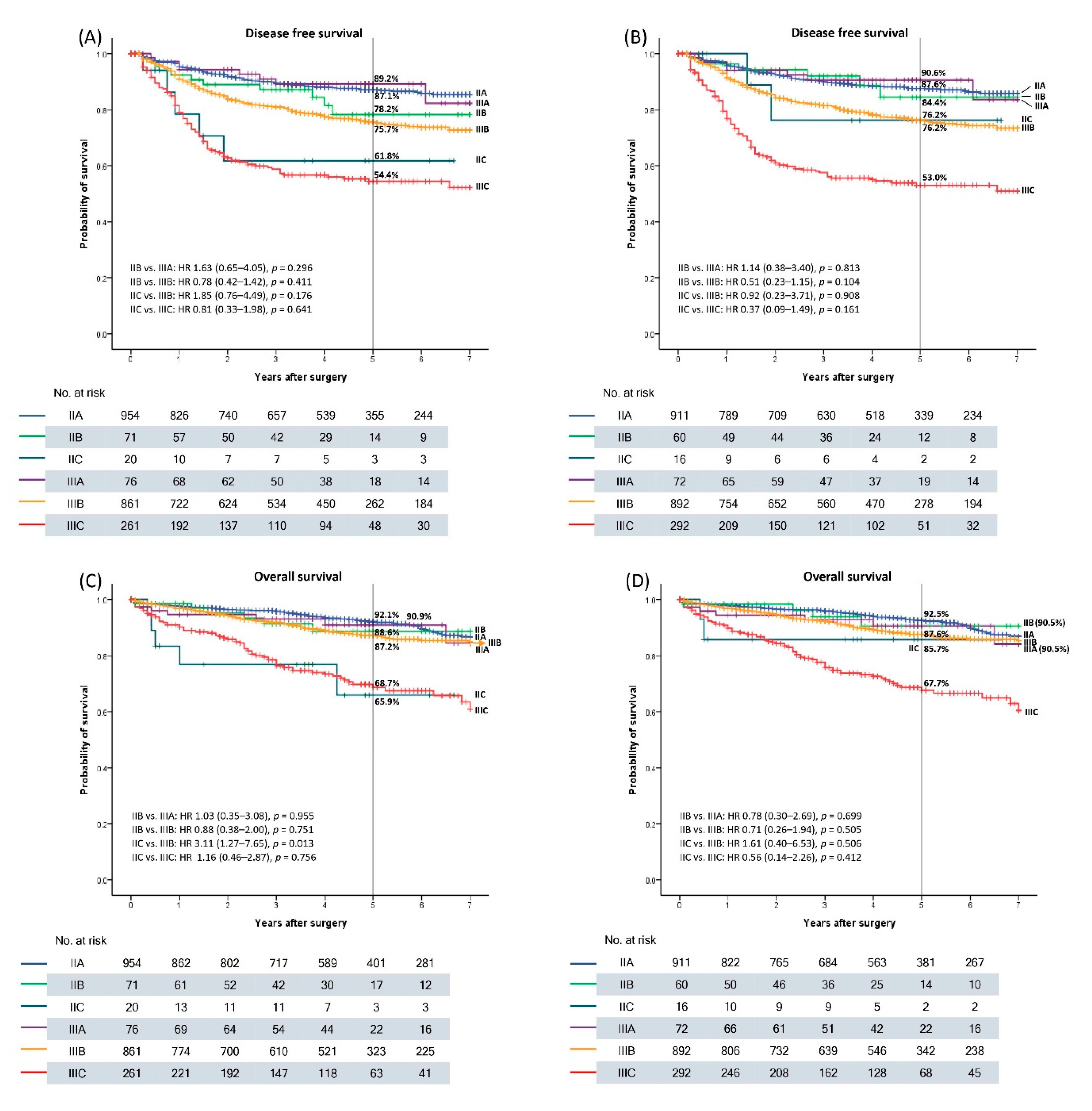
3.5. New TNV Staging System Including VI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jemal, A.; Ward, E.M.; Johnson, C.J.; Cronin, K.A.; Ma, J.; Ryerson, B.; Mariotto, A.; Lake, A.J.; Wilson, R.; Sherman, R.L.; et al. Annual Report to the Nation on the Status of Cancer, Featuring Survival. J. Natl. Cancer Inst. 2017, 109, 1975–2014. [Google Scholar] [CrossRef]
- Yin, D.; Morris, C.R.; Bates, J.H.; German, R.R. Effect of misclassified underlying cause of death on survival estimates of colon and rectal cancer. J. Natl. Cancer Inst. 2011, 103, 1130–1133. [Google Scholar] [CrossRef] [Green Version]
- Auclin, E.; Zaanan, A.; Vernerey, D.; Douard, R.; Gallois, C.; Laurent-Puig, P.; Bonnetain, F.; Taieb, J. Subgroups and prognostication in stage III colon cancer: Future perspectives for adjuvant therapy. Ann. Oncol. 2017, 28, 958–968. [Google Scholar] [CrossRef]
- Babcock, B.D.; Aljehani, M.A.; Jabo, B.; Choi, A.H.; Morgan, J.W.; Selleck, M.J.; Luca, F.; Raskin, E.; Reeves, M.E.; Garberoglio, C.A.; et al. High-Risk Stage II Colon Cancer: Not All Risks Are Created Equal. Ann. Surg. Oncol. 2018, 25, 1980–1985. [Google Scholar] [CrossRef]
- Caritg, O.; Navarro, A.; Moreno, I.; Martínez-Rodenas, F.; Cordeiro, A.; Muñoz, C.; Ruiz-Martinez, M.; Santasusagna, S.; Castellano, J.J.; Monzó, M. Identifying High-Risk Stage II Colon Cancer Patients: A Three-MicroRNA-Based Score as a Prognostic Biomarker. Clin. Colorectal Cancer 2016, 15, e175–e182. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. NCCN Guidelines Insights: Colon Cancer, Version 2.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 359–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef]
- Dienstmann, R.; Salazar, R.; Tabernero, J. Personalizing colon cancer adjuvant therapy: Selecting optimal treatments for individual patients. J. Clin. Oncol. 2015, 33, 1787–1796. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.O. Precision treatment in colorectal cancer: Now and the future. JGH Open 2019, 3, 361–369. [Google Scholar] [CrossRef]
- Li, S.; Li, Q. Cancer stem cells and tumor metastasis (Review). Int. J. Oncol. 2014, 44, 1806–1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stacker, S.A.; Williams, S.P.; Karnezis, T.; Shayan, R.; Fox, S.B.; Achen, M.G. Lymphangiogenesis and lymphatic vessel remodelling in cancer. Nat. Rev. Cancer 2014, 14, 159–172. [Google Scholar] [CrossRef]
- Holopainen, T.; Bry, M.; Alitalo, K.; Saaristo, A. Perspectives on lymphangiogenesis and angiogenesis in cancer. J. Surg. Oncol. 2011, 103, 484–488. [Google Scholar] [CrossRef] [PubMed]
- Pantel, K.; Brakenhoff, R.H. Dissecting the metastatic cascade. Nat. Rev. Cancer 2004, 4, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Hari, D.M.; Leung, A.M.; Lee, J.H.; Sim, M.S.; Vuong, B.; Chiu, C.G.; Bilchik, A.J. AJCC Cancer Staging Manual 7th edition criteria for colon cancer: Do the complex modifications improve prognostic assessment? J. Am. Coll. Surg. 2013, 217, 181–190. [Google Scholar] [CrossRef] [Green Version]
- Leijssen, L.G.J.; Dinaux, A.M.; Amri, R.; Taylor, M.S.; Deshpande, V.; Bordeianou, L.G.; Kunitake, H.; Berger, D.L. Impact of intramural and extramural vascular invasion on stage II-III colon cancer outcomes. J. Surg. Oncol. 2019, 119, 749–757. [Google Scholar] [CrossRef]
- Skancke, M.; Arnott, S.M.; Amdur, R.L.; Siegel, R.S.; Obias, V.J.; Umapathi, B.A. Lymphovascular Invasion and Perineural Invasion Negatively Impact Overall Survival for Stage II Adenocarcinoma of the Colon. Dis. Colon. Rectum. 2019, 62, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Parnaby, C.N.; Scott, N.W.; Ramsay, G.; MacKay, C.; Samuel, L.; Murray, G.I.; Loudon, M.A. Prognostic value of lymph node ratio and extramural vascular invasion on survival for patients undergoing curative colon cancer resection. Br. J. Cancer 2015, 113, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.H.; Kim, J.M.; Kang, G.H.; Chang, H.J.; Kang, D.W.; Kim, J.H.; Bae, J.M.; Seo, A.N.; Park, H.S.; Kang, Y.K.; et al. Standardized Pathology Report for Colorectal Cancer, 2nd Edition. J. Pathol. Transl. Med. 2020, 54, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Weiser, M.R.; Gönen, M.; Chou, J.F.; Kattan, M.W.; Schrag, D. Predicting survival after curative colectomy for cancer: Individualizing colon cancer staging. J. Clin. Oncol. 2011, 29, 4796–4802. [Google Scholar] [CrossRef] [Green Version]
- Gunderson, L.L.; Jessup, J.M.; Sargent, D.J.; Greene, F.L.; Stewart, A.K. Revised TN categorization for colon cancer based on national survival outcomes data. J. Clin. Oncol. 2010, 28, 264–271. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Luo, D.; Cai, S.; Li, Q.; Li, X. P-TNM staging system for colon cancer: Combination of P-stage and AJCC TNM staging system for improving prognostic prediction and clinical management. Cancer Manag. Res. 2018, 10, 2303–2314. [Google Scholar] [CrossRef] [Green Version]
- Dienstmann, R.; Mason, M.J.; Sinicrope, F.A.; Phipps, A.I.; Tejpar, S.; Nesbakken, A.; Danielsen, S.A.; Sveen, A.; Buchanan, D.D.; Clendenning, M.; et al. Prediction of overall survival in stage II and III colon cancer beyond TNM system: A retrospective, pooled biomarker study. Ann. Oncol. 2017, 28, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Petersen, V.C.; Baxter, K.J.; Love, S.B.; Shepherd, N.A. Identification of objective pathological prognostic determinants and models of prognosis in Dukes’ B colon cancer. Gut 2002, 51, 65–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amri, R.; England, J.; Bordeianou, L.G.; Berger, D.L. Risk Stratification in Patients with Stage II Colon Cancer. Ann. Surg. Oncol. 2016, 23, 3907–3914. [Google Scholar] [CrossRef]
- Betge, J.; Pollheimer, M.J.; Lindtner, R.A.; Kornprat, P.; Schlemmer, A.; Rehak, P.; Vieth, M.; Hoefler, G.; Langner, C. Intramural and extramural vascular invasion in colorectal cancer: Prognostic significance and quality of pathology reporting. Cancer 2012, 118, 628–638. [Google Scholar] [CrossRef]
- Gibson, K.M.; Chan, C.; Chapuis, P.H.; Dent, O.F.; Bokey, L. Mural and extramural venous invasion and prognosis in colorectal cancer. Dis. Colon. Rectum. 2014, 57, 916–926. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.; Lee, S.; Kim, A.; Kim, Y.G.; Ahn, S.J.; Park, D.Y. Venous Invasion in Colorectal Cancer: Impact of Morphologic Findings on Detection Rate. Cancer Res. Treat. 2016, 48, 1222–1228. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total Patients (n = 2243) | No VI (n = 2018) | VI (n = 225) | p |
|---|---|---|---|---|
| Age ≥ 65 years | 1129(50.3) | 1014(50.2) | 115(51.1) | 0.806 |
| Sex, male | 1238(55.2) | 1105(54.8) | 133(59.1) | 0.213 |
| ASA score ≥ 3 | 161(7.2) | 146(7.2) | 15(6.7) | 0.754 |
| Tumor location | 0.379 | |||
| Right colon | 848(37.8) | 769(38.1) | 79(35.1) | |
| Left colon | 1395(62.2) | 1249(61.9) | 146(64.9) | |
| Surgical approach | 0.355 | |||
| Laparoscopic | 1412(63.0) | 1264(62.6) | 148(65.8) | |
| Conventional | 831(37.0) | 754(37.4) | 77(34.2) | |
| T stage | <0.001 | |||
| 1–3 | 1951(87.0) | 1795(88.9) | 156(69.3) | |
| 4 | 292(13.0) | 223(11.1) | 69(30.7) | |
| N stage | <0.001 | |||
| 0 | 1045(46.6) | 987(48.9) | 58(25.8) | |
| 1 | 762(34.0) | 696(34.5) | 66(29.3) | |
| 2 | 436(19.4) | 335(16.6) | 101(44.9) | |
| TNM stage | <0.001 | |||
| II | 1045(46.6) | 987(48.9) | 58(25.8) | |
| III | 1198(53.4) | 1031(51.1) | 167(74.2) | |
| Number of LN harvest < 12 | 369(16.5) | 336(16.7) | 33(14.7) | 0.447 |
| Histological grade, poor | 210(9.4) | 180(8.9) | 30(13.3) | 0.031 |
| Lymphatic invasion, yes | 1067(47.6) | 909(45.0) | 158(70.2) | <0.001 |
| Perineural invasion, yes | 567(25.3) | 468(23.2) | 99(44.0) | <0.001 |
| Adjuvant chemotherapy, yes | 1772(79.0) | 1586(78.6) | 186(82.7) | 0.155 |
| Recurrence, yes | 420(18.7) | 349(17.3) | 71(31.6) | <0.001 |
| Local recurrence, yes | 51 (2.3) | 46 (2.3) | 5 (2.2) | 0.956 |
| Variables | N0 (n = 987) | N1 (n = 696) | N2 (n = 335) | VI (n = 225) | p * | p ** |
|---|---|---|---|---|---|---|
| Age ≥ 65 years | 504(51.1) | 349(50.1) | 161(48.1) | 115(51.1) | 0.809 | 0.479 |
| Sex, male | 571(57.9) | 359(51.6) | 175(52.2) | 133(59.1) | 0.028 | 0.109 |
| ASA score ≥ 3 | 70(7.1) | 59(8.5) | 17(5.1) | 15(6.7) | 0.252 | 0.426 |
| Tumor location | 0.351 | 0.964 | ||||
| Right side | 391(39.6) | 261(37.5) | 117(34.9) | 79(35.1) | ||
| Left side | 596(60.4) | 435(62.5) | 218(65.1) | 146(64.9) | ||
| Surgical approach | 0.707 | 0.303 | ||||
| Laparoscopic | 615(62.3) | 433(63.6) | 206(61.5) | 148(65.8) | ||
| Conventional | 372(37.7) | 253(36.4) | 129(38.5) | 77(34.2) | ||
| T stage | <0.001 | 0.003 | ||||
| 1–3 | 911(92.3) | 615(88.4) | 269(80.3) | 156(69.3) | ||
| 4 | 76(7.7) | 81(11.6) | 66(19.7) | 69(30.7) | ||
| N stage | <0.001 | |||||
| 0 | 987(100.0) | 58(25.8) | ||||
| 1 | 696(100.0) | 66(29.3) | ||||
| 2 | 335(100.0) | 101(44.9) | ||||
| TNM stage | <0.001 | |||||
| II | 987(100.0) | 0 | 0 | 58(25.8) | ||
| III | 0 | 696(100.0) | 335(100.0) | 167(74.2) | ||
| Number of LN harvest < 12 | 173(17.5) | 133(19.1) | 30(9.0) | 33(14.7) | <0.001 | 0.036 |
| Histological grade, poor | 59(6.0) | 67(9.6) | 54(16.1) | 30(13.3) | <0.001 | 0.365 |
| Lymphatic invasion, yes | 154(15.6) | 493(70.8) | 262(78.2) | 158(70.2) | <0.001 | 0.032 |
| Perineural invasion, yes | 165(16.7) | 167(24.0) | 136(40.6) | 99(44.0) | <0.001 | 0.424 |
| Adjuvant chemotherapy, yes | 696(70.5) | 595(85.5) | 295(88.1) | 186(82.7) | <0.001 | 0.072 |
| Recurrence, yes | 107(10.8) | 136(19.5) | 106(31.6) | 71(31.6) | <0.001 | 0.983 |
| Local recurrence, yes | 16(1.6) | 15(2.2) | 15(4.5) | 5(2.2) | 0.026 | 0.159 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p | HR (95% CI) | p |
| Age ≥ 65 years | 1.258 (1.039–1.524) | 0.019 | 1.260 (1.039–1.527) | 0.019 |
| Sex, male | 1.099 (0.906–1.333) | 0.340 | ||
| ASA score ≥ 3 | 1.323 (0.918–1.908) | 0.134 | ||
| Tumor location | ||||
| Right side | Reference | |||
| Left side | 1.198 (0.979–1.467) | 0.080 | ||
| Surgical approach | ||||
| Laparoscopic | Reference | Reference | ||
| Conventional | 1.318 (1.086–1.599) | 0.005 | 1.307 (1.073–1.593) | 0.008 |
| T stage | ||||
| 1–3 | Reference | Reference | ||
| 4 | 2.426 (1.931–3.048) | <0.001 | 1.920 (1.511–2.439) | <0.001 |
| N stage | ||||
| 0 | Reference | |||
| 1 | 1.785 (1.410–2.261) | <0.001 | ||
| 2 | 3.147 (2.472–4.006) | <0.001 | ||
| TNM stage | ||||
| II | Reference | |||
| III | 2.248 (1.822–2.772) | <0.001 | ||
| Number of LN harvest < 12 | 1.275 (1.001–1.625) | 0.049 | 1.453 (1.132–1.864) | 0.003 |
| Histological grade, poor * | 1.627 (1.220–2.171) | 0.001 | 1.315 (0.977–1.770) | 0.070 |
| VI, yes | 2.149 (1.665–2.774) | <0.001 | ||
| Lymphatic invasion, yes | 1.602 (1.320–1.944) | <0.001 | 0.882 (0.699–1.114) | 0.291 |
| Perineural invasion, yes | 1.557 (1.271–1.907) | <0.001 | 1.259 (1.015–1.561) | 0.036 |
| Adjuvant chemotherapy, no | 0.909 (0.696–1.186) | 0.480 | ||
| Group | ||||
| N0 | 0.538(0.418–0.693) | <0.001 | 0.543 (0.407–0.722) | <0.001 |
| N1 | Reference | Reference | ||
| N2 | 1.778(1.379–2.292) | <0.001 | 1.738 (1.343–2.251) | <0.001 |
| VI | 1.904(1.429–2.537) | <0.001 | 1.704 (1.267–2.291) | <0.001 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p | HR (95% CI) | p |
| Age ≥ 65 years | 1.650 (1.290–2.112) | <0.001 | 1.282 (0.990–1.661) | 0.060 |
| Sex, male | 1.349 (1.051–1.732) | 0.019 | 1.319 (1.026–1.696) | 0.031 |
| ASA score ≥ 3 | 2.921 (2.077–4.107) | <0.001 | 2.531 (1.774–3.611) | <0.001 |
| Tumor location | ||||
| Right side | Reference | |||
| Left side | 1.056 (0.821–1.359) | 0.671 | ||
| Surgical approach | ||||
| Laparoscopic | Reference | Reference | ||
| Conventional | 1.711 (1.341–2.184) | <0.001 | 1.569 (1.225–2.011) | <0.001 |
| T stage | ||||
| 1–3 | Reference | Reference | ||
| 4 | 2.726 (2.057–3.612) | <0.001 | 2.110 (1.567–2.842) | <0.001 |
| N stage | ||||
| 0 | Reference | |||
| 1 | 1.367 (1.016–1.840) | 0.039 | ||
| 2 | 2.642 (1.964–3.555) | <0.001 | ||
| TNM stage | ||||
| II | Reference | |||
| III | 1.805 (1.396–2.333) | <0.001 | ||
| Number of LN harvest < 12 | 1.507 (1.127–2.014) | 0.006 | 1.588 (1.177–2.142) | 0.002 |
| Histological grade, poor * | 1.812 (1.279–2.566) | 0.001 | 1.577 (1.095–2.271) | 0.014 |
| VI, yes | 2.260 (1.652–3.092) | <0.001 | ||
| Lymphatic invasion, yes | 1.607 (1.256–2.056) | <0.001 | 1.251 (0.919–1.704) | 0.154 |
| Perineural invasion, yes | 1.219 (0.933–1.594) | 0.147 | ||
| Adjuvant chemotherapy, no | 2.055 (1.569–2.692) | <0.001 | 2.268 (1.699–3.027) | <0.001 |
| Group | ||||
| N0 | 0.785 (0.573–1.076) | 0.132 | 0.870 (0.598–1.266) | 0.467 |
| N1 | Reference | Reference | ||
| N2 | 1.790 (1.268–2.528) | 0.001 | 1.949 (1.366–2.779) | <0.001 |
| VI | 2.295 (1.594–3.304) | <0.001 | 2.301 (1.582–3.348) | <0.001 |
| T | N | V | TN Stage | TNV Stage | Change | N (%) |
|---|---|---|---|---|---|---|
| T3 | N0 | V0 | IIA | IIA | No | 911 (40.6) |
| V1 | IIA | IIIB | Yes | 43 (1.9) | ||
| T4a | N0 | V0 | IIB | IIB | No | 60 (2.7) |
| V1 | IIB | IIIC | Yes | 11 (0.5) | ||
| T4b | N0 | V0 | IIC | IIC | No | 16 (0.7) |
| V1 | IIC | IIIC | Yes | 4 (0.2) | ||
| T1 | N1 | V0 | IIIA | IIIA | No | 22 (1.0) |
| V1 | IIIA | IIIA | No | 1 (0.0) | ||
| T2 | N1 | V0 | IIIA | IIIA | No | 47 (2.1) |
| V1 | IIIA | IIIB | Yes | 4 (0.2) | ||
| T3 | N1 | V0 | IIIB | IIIB | No | 546 (24.3) |
| V1 | IIIB | IIIB | No | 44 (2.0) | ||
| T4a | N1 | V0 | IIIB | IIIB | No | 70 (3.1) |
| V1 | IIIB | IIIC | Yes | 16 (0.7) | ||
| T4b | N1 | V0 | IIIC | IIIC | No | 11 (0.5) |
| V1 | IIIC | IIIC | No | 1 (0.0) | ||
| T1 | N2a | V0 | IIIA | IIIA | No | 2 (0.1) |
| V1 | IIIA | IIIA | No | 0 (0.0) | ||
| T2 | N2a | V0 | IIIB | IIIB | No | 5 (0.2) |
| V1 | IIIB | IIIB | No | 0 (0.0) | ||
| T3 | N2a | V0 | IIIB | IIIB | No | 154 (6.9) |
| V1 | IIIB | IIIB | No | 23 (1.0) | ||
| T4 | N2a | V0 | IIIC | IIIC | No | 39 (1.7) |
| V1 | IIIC | IIIC | No | 12 (0.5) | ||
| T1 | N2b | V0 | IIIB | IIIB | No | 0 (0.0) |
| V1 | IIIB | IIIB | No | 1 (0.0) | ||
| T2 | N2b | V0 | IIIB | IIIB | No | 0 (0.0) |
| V1 | IIIB | IIIB | No | 2 (0.1) | ||
| T3 | N2b | V0 | IIIC | IIIC | No | 106 (4.7) |
| V1 | IIIC | IIIC | No | 40 (1.8) | ||
| T4 | N2b | V0 | IIIC | IIIC | No | 27 (1.2) |
| V1 | IIIC | IIIC | No | 25 (1.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, J.H.; Kim, J.H.; Lee, J.; Kye, B.-H.; Lee, S.C.; Lee, I.K.; Kang, W.K.; Cho, H.-M.; Lee, Y.S. Addition of V-Stage to Conventional TNM Staging to Create the TNVM Staging System for Accurate Prediction of Prognosis in Colon Cancer: A Multi-Institutional Retrospective Cohort Study. Biomedicines 2021, 9, 888. https://doi.org/10.3390/biomedicines9080888
Bae JH, Kim JH, Lee J, Kye B-H, Lee SC, Lee IK, Kang WK, Cho H-M, Lee YS. Addition of V-Stage to Conventional TNM Staging to Create the TNVM Staging System for Accurate Prediction of Prognosis in Colon Cancer: A Multi-Institutional Retrospective Cohort Study. Biomedicines. 2021; 9(8):888. https://doi.org/10.3390/biomedicines9080888
Chicago/Turabian StyleBae, Jung Hoon, Ji Hoon Kim, Jaeim Lee, Bong-Hyeon Kye, Sang Chul Lee, In Kyu Lee, Won Kyung Kang, Hyeon-Min Cho, and Yoon Suk Lee. 2021. "Addition of V-Stage to Conventional TNM Staging to Create the TNVM Staging System for Accurate Prediction of Prognosis in Colon Cancer: A Multi-Institutional Retrospective Cohort Study" Biomedicines 9, no. 8: 888. https://doi.org/10.3390/biomedicines9080888
APA StyleBae, J. H., Kim, J. H., Lee, J., Kye, B. -H., Lee, S. C., Lee, I. K., Kang, W. K., Cho, H. -M., & Lee, Y. S. (2021). Addition of V-Stage to Conventional TNM Staging to Create the TNVM Staging System for Accurate Prediction of Prognosis in Colon Cancer: A Multi-Institutional Retrospective Cohort Study. Biomedicines, 9(8), 888. https://doi.org/10.3390/biomedicines9080888