
Anti-Phospholipid Antibodies and COVID-19 Thrombosis: A Co-Star, Not a Supporting Actor

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Reference Population
2.4. Study Definitions
2.5. Samples
2.6. Criteria aPL Determination
2.7. Extra-Criteria aPL Determination
2.8. Anti-SARS-CoV-2 Antibodies Determination
2.9. Data Collection
2.10. Statistical Analysis
2.11. Ethical Issues
3. Results
3.1. aPL Prevalence in COVID-19 Patients
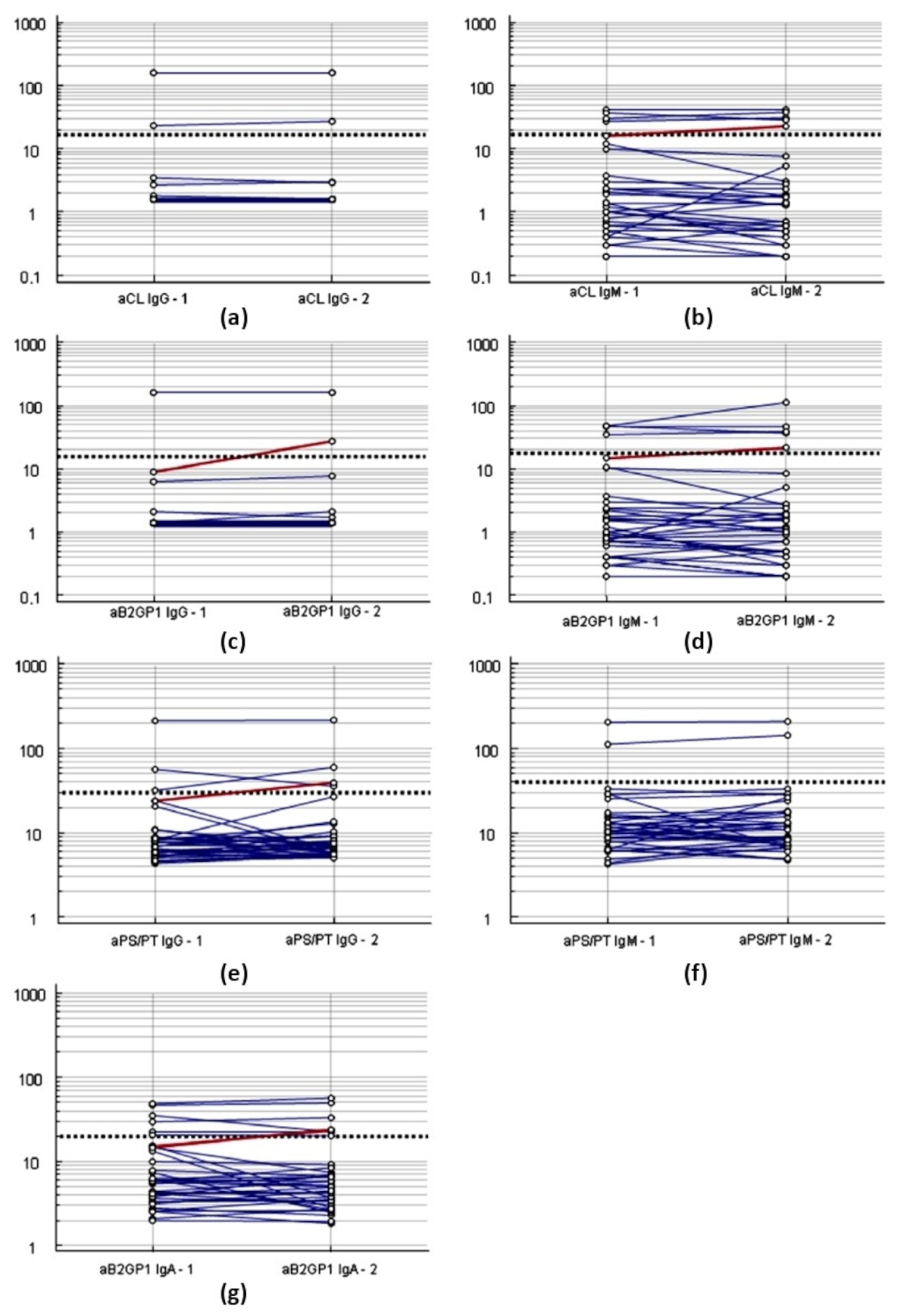
3.2. Variability of Antibodies over the Time in COVID-19 Patients
3.3. Clinical Evolution of COVID-19 Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients with Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal Transduct. Target. Ther. 2020, 5, 33. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934. [Google Scholar] [CrossRef] [Green Version]
- Marchandot, B.; Sattler, L.; Jesel, L.; Matsushita, K.; Schini-Kerth, V.; Grunebaum, L.; Morel, O. COVID-19 Related Coagulopathy: A Distinct Entity? J. Clin. Med. 2020, 9, 1651. [Google Scholar] [CrossRef]
- Helms, J.; CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis); Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Levi, M.; Iba, T. COVID-19 coagulopathy: Is it disseminated intravascular coagulation? Intern. Emerg. Med. 2020, 16, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Paz, L.; Capodanno, D.; Montalescot, G.; Angiolillo, D.J. Coronavirus Disease 2019–Associated Thrombosis and Coagulopathy: Review of the Pathophysiological Characteristics and Implications for Antithrombotic Management. J. Am. Heart Assoc. 2021, 10, e019650. [Google Scholar] [CrossRef]
- Merrill, J.T.; Erkan, D.; Winakur, J.; James, J.A. Emerging evidence of a COVID-19 thrombotic syndrome has treatment implications. Nat. Rev. Rheumatol. 2020, 16, 581–589. [Google Scholar] [CrossRef]
- Mendoza-Pinto, C.; Escárcega, R.O.; García-Carrasco, M.; Bailey, D.J.; Gálvez-Romero, J.L.; Cervera, R. Viral infections and their relationship with catastrophic antiphospholipid syndrome: A possible pathogenic mechanism of severe COVID-19 thrombotic complications. J. Intern. Med. 2020, 288, 737–739. [Google Scholar] [CrossRef] [PubMed]
- Hossri, S.; Shadi, M.; Hamarsha, Z.; Schneider, R.; El-Sayegh, D. Clinically significant anticardiolipin antibodies associated with COVID-19. J. Crit. Care 2020, 59, 32–34. [Google Scholar] [CrossRef]
- de Chambrun, M.P.; Frere, C.; Miyara, M.; Amoura, Z.; Martin-Toutain, I.; Mathian, A.; Hekimian, G.; Combes, A. High frequency of antiphospholipid antibodies in critically ill COVID-19 patients: A link with hypercoagulability? J. Intern. Med. 2020, 289, 422–424. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Puerta, J.A.; Cervera, R. Diagnosis and classification of the antiphospholipid syndrome. J. Autoimmun. 2014, 48–49, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Pérez, D.; Tincani, A.; Serrano, M.; Shoenfeld, Y.; Serrano, A. Antiphospholipid syndrome and IgA anti-beta2-glycoprotein I antibodies: When Cinderella becomes a princess. Lupus 2017, 27, 177–178. [Google Scholar] [CrossRef]
- Lakos, G.; Favaloro, E.J.; Harris, E.N.; Meroni, P.L.; Tincani, A.; Wong, R.C.; Pierangeli, S.S. International consensus guidelines on anticardiolipin and anti-β2-glycoprotein I testing: Report from the 13th International Congress on Antiphospholipid Antibodies. Arthritis Rheum. 2011, 64, 1–10. [Google Scholar] [CrossRef]
- Delgado, J.F.; Serrano, M.; Morán, L.; Enguita, A.B.; Martínez-Flores, J.A.; Ortiz-Bautista, C.; Rodríguez-Chaverri, A.; de Antonio, I.P.; Cosio, M.D.G.; Panete, M.J.C.; et al. Early mortality after heart transplantation related to IgA anti–β2-glycoprotein I antibodies. J. Heart Lung Transplant. 2017, 36, 1258–1265. [Google Scholar] [CrossRef]
- Giordano, P.; Tesse, R. Clinical and laboratory characteristics of children positive for antiphospholipid antibodies. Blood Transfus. 2012, 10, 296–301. [Google Scholar] [CrossRef]
- Sciascia, S.; Amigo, M.-C.; Roccatello, D.; Khamashta, M. Diagnosing antiphospholipid syndrome: ‘extra-criteria’ manifestations and technical advances. Nat. Rev. Rheumatol. 2017, 13, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Estes, S.K.; Ali, R.A.; Gandhi, A.A.; Yalavarthi, S.; Shi, H.; Sule, G.; Gockman, K.; Madison, J.A.; Zuo, M.; et al. Prothrombotic autoantibodies in serum from patients hospitalized with COVID-19. Sci. Transl. Med. 2020, 12, eabd3876. [Google Scholar] [CrossRef]
- Xiao, M.; Zhang, Y.; Zhang, S.; Qin, X.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; et al. Antiphospholipid Antibodies in Critically Ill Patients with COVID-19. Arthritis Rheumatol. 2020, 72, 1998–2004. [Google Scholar] [CrossRef]
- Serrano, M.; Espinosa, G.; Lalueza, A.; Bravo-Gallego, L.Y.; Diaz-Simón, R.; Bs, S.G.; Bs, J.G.; Moises, J.; Bs, L.N.; Prieto-González, S.; et al. Beta-2-Glycoprotein-I Deficiency Could Precipitate an Antiphospholipid Syndrome-like Prothrombotic Situation in Patients With Coronavirus Disease 2019. ACR Open Rheumatol. 2021, 3, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Taha, M.; Samavati, L. Antiphospholipid antibodies in COVID-19: A meta-analysis and systematic review. RMD Open 2021, 7, e001580. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Krilis, S.A.; Chong, B.H.; Gordon, S.; Chesterman, C.N. Prevalence of lupus anticoagulant and anticardiolipin antibodies in a healthy population. Aust. N. Z. J. Med. 1990, 20, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Naranjo, L.; Ostos, F.; Gil-Etayo, F.J.; Hernández-Gallego, J.; Cabrera-Marante, Ó.; Pleguezuelo, D.E.; Díaz-Simón, R.; Cerro, M.; Lora, D.; Martínez-Salio, A.; et al. Presence of Extra-Criteria Antiphospholipid Antibodies Is an Independent Risk Factor for Ischemic Stroke. Front. Cardiovasc. Med. 2021, 8, 360. [Google Scholar] [CrossRef]
- Vollmer, O.; Tacquard, C.; Dieudonné, Y.; Nespola, B.; Sattler, L.; Grunebaum, L.; Gies, V.; Radosavljevic, M.; Kaeuffer, C.; Hansmann, Y.; et al. Follow-up of COVID-19 patients: LA is transient but other aPLs are persistent. Autoimmun. Rev. 2021, 20, 102822. [Google Scholar] [CrossRef] [PubMed]
- Siguret, V.; Voicu, S.; Neuwirth, M.; Delrue, M.; Gayat, E.; Stépanian, A.; Mégarbane, B. Are antiphospholipid antibodies associated with thrombotic complications in critically ill COVID-19 patients? Thromb. Res. 2020, 195, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Hanly, J.G. Antiphospholipid syndrome: An overview. Can. Med. Assoc. J. 2003, 168, 1675–1682. [Google Scholar]
- Mendoza-Pinto, C.; García-Carrasco, M.; Cervera, R. Role of Infectious Diseases in the Antiphospholipid Syndrome (Including Its Catastrophic Variant). Curr. Rheumatol. Rep. 2018, 20, 62. [Google Scholar] [CrossRef] [PubMed]
- Harel, M.; Aron-Maor, A.; Sherer, Y.; Blank, M.; Shoenfeld, Y. The infectious etiology of the antiphospholipid syndrome: Links between infection and autoimmunity. Immunobiology 2005, 210, 743–747. [Google Scholar] [CrossRef]
- Million, M.; Bardin, N.; Bessis, S.; Nouiakh, N.; Douliery, C.; Edouard, S.; Angelakis, E.; Bosseray, A.; Epaulard, O.; Branger, S.; et al. Thrombosis and antiphospholipid antibody syndrome during acute Q fever. Medicine 2017, 96, e7578. [Google Scholar] [CrossRef]
- Asherson, R.A. Antiphospholipid antibodies and infections. Ann. Rheum. Dis. 2003, 62, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Harzallah, I.; Debliquis, A.; Drénou, B. Lupus anticoagulant is frequent in patients with COVID-19. J. Thromb. Haemost. 2020, 18, 2064–2065. [Google Scholar] [CrossRef]
- Devreese, K.M.J.; Linskens, E.A.; Benoit, D.; Peperstraete, H. Antiphospholipid antibodies in patients with COVID-19: A relevant observation? J. Thromb. Haemost. 2020, 18, 2191–2201. [Google Scholar] [CrossRef]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.W.M.; De Groot, P.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Pérez, D.; Martínez-Flores, J.A.; Serrano, A.; Lora, D.; Paz-Artal, E.; Morales, J.M. Evaluation of three fully automated immunoassay systems for detection of IgA anti-beta 2-glycoprotein I antibodies. Int. J. Lab. Hematol. 2016, 38, 560–568. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 276–282. [Google Scholar] [CrossRef]
- Li, J.; Kim, K.; Barazia, A.; Tseng, A.; Cho, J. Platelet–neutrophil interactions under thromboinflammatory conditions. Cell. Mol. Life Sci. 2015, 72, 2627–2643. [Google Scholar] [CrossRef]
- Keller, A.K.; Jorgensen, T.M.; Jespersen, B. Identification of Risk Factors for Vascular Thrombosis May Reduce Early Renal Graft Loss: A Review of Recent Literature. J. Transplant. 2012, 2012, 793461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meroni, P.L.; Borghi, M.O.; Raschi, E.; Tedesco, F. Pathogenesis of antiphospholipid syndrome: Understanding the antibodies. Nat. Rev. Rheumatol. 2011, 7, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Stark, K.; Massberg, S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat. Rev. Cardiol. 2021, 1–17. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef]
- Wu, H.; Li, R.; Pei, L.-G.; Wei, Z.-H.; Kang, L.-N.; Wang, L.; Xie, J.; Xu, B. Emerging Role of High Mobility Group Box-1 in Thrombosis-Related Diseases. Cell. Physiol. Biochem. 2018, 47, 1319–1337. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-W.; Lee, J.-K. Role of HMGB1 in the Interplay between NETosis and Thrombosis in Ischemic Stroke: A Review. Cells 2020, 9, 1794. [Google Scholar] [CrossRef]
- Chiappalupi, S.; Salvadori, L.; Donato, R.; Riuzzi, F.; Sorci, G. Hyperactivated RAGE in Comorbidities as a Risk Factor for Severe COVID-19—The Role of RAGE-RAS Crosstalk. Biomolecules 2021, 11, 876. [Google Scholar] [CrossRef]
- Fields, R.A.; Toubbeh, H.; Searles, R.P.; Bankhurst, A.D. The prevalence of anticardiolipin antibodies in a healthy elderly population and its association with antinuclear antibodies. J. Rheumatol. 1989, 16, 623–625. [Google Scholar] [PubMed]
- Manoussakis, M.N.; Tzioufas, A.G.; Silis, M.P.; Pange, P.J.; Goudevenos, J.; Moutsopoulos, H.M. High prevalence of anti-cardiolipin and other autoantibodies in a healthy elderly population. Clin. Exp. Immunol. 1987, 69, 557–565. [Google Scholar]
- Vadasz, Z.; Haj, T.; Kessel, A.; Toubi, E. Age-related autoimmunity. BMC Med. 2013, 11, 94. [Google Scholar] [CrossRef] [PubMed]
- Amezcua-Guerra, L.M.; Rojas-Velasco, G.; Brianza-Padilla, M.; Vázquez-Rangel, A.; Márquez-Velasco, R.; Baranda-Tovar, F.; Springall, R.; Gonzalez-Pacheco, H.; Juárez-Vicuña, Y.; Tavera-Alonso, C.; et al. Presence of antiphospholipid antibodies in COVID-19: A case series study. Ann. Rheum. Dis. 2020, 80, e73. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.M.; Serrano, M.; Martínez-Flores, J.A.; Pérez, D.; Castro, M.J.; Sánchez, E.; García, F.; Rodríguez-Antolín, A.; Alonso, M.; Gutierrez, E.; et al. The Presence of Pretransplant Antiphospholipid Antibodies IgA Anti-β-2-Glycoprotein I as a Predictor of Graft Thrombosis After Renal Transplantation. Transplant. 2017, 101, 597–607. [Google Scholar] [CrossRef]
- Cabrera-Marante, O.; De Frías, E.R.; Serrano, M.; Morillo, F.L.; Naranjo, L.; Gil-Etayo, F.; Paz-Artal, E.; Pleguezuelo, D.; Serrano, A. The Weight of IgA Anti-β2glycoprotein I in the Antiphospholipid Syndrome Pathogenesis: Closing the Gap of Seronegative Antiphospholipid Syndrome. Int. J. Mol. Sci. 2020, 21, 8972. [Google Scholar] [CrossRef] [PubMed]
- Ali, O.H.; Bomze, D.; Risch, L.; Brugger, S.D.; Paprotny, M.; Weber, M.; Thiel, S.; Kern, L.; Albrich, W.C.; Kohler, P.; et al. Severe Coronavirus Disease 2019 (COVID-19) is Associated with Elevated Serum Immunoglobulin (Ig) A and Antiphospholipid IgA Antibodies. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Castillo-Martínez, D.; Torres, Z.; Amezcua-Guerra, L.M.; Pineda, C. Are antiphospholipid antibodies just a common epiphenomenon or are they causative of immune-mediated coagulopathy in COVID-19? Clin. Rheumatol. 2021, 40, 3015–3019. [Google Scholar] [CrossRef]
- Cavalli, E.; Bramanti, A.; Ciurleo, R.; Tchorbanov, A.I.; Giordano, A.; Fagone, P.; Belizna, C.; Bramanti, P.; Shoenfeld, Y.; Nicoletti, F. Entangling COVID-19 associated thrombosis into a secondary antiphospholipid antibody syndrome: Diagnostic and therapeutic perspectives (Review). Int. J. Mol. Med. 2020, 46, 903–912. [Google Scholar] [CrossRef]
- Nakano, H.; Shiina, K.; Tomiyama, H. Cardiovascular Outcomes in the Acute Phase of COVID-19. Int. J. Mol. Sci. 2021, 22, 4071. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Calcaterra, I.; Ambrosino, P.; Vitelli, N.; Lupoli, R.; Orsini, R.; Chiurazzi, M.; Maniscalco, M.; Di Minno, M. Risk Assessment and Antithrombotic Strategies in Antiphospholipid Antibody Carriers. Biomedicines 2021, 9, 122. [Google Scholar] [CrossRef]
- Molinari, A.C.; Banov, L.; Bertamino, M.; Barabino, P.; Lassandro, G.; Giordano, P. A Practical Approach to the Use of Low Molecular Weight Heparins in VTE Treatment and Prophylaxis in Children and Newborns. Pediatr. Hematol. Oncol. 2014, 32, 1–10. [Google Scholar] [CrossRef]
- Bowles, L.; Platton, S.; Yartey, N.; Dave, M.; Lee, K.; Hart, D.P.; Macdonald, V.; Green, L.; Sivapalaratnam, S.; Pasi, K.J.; et al. Lupus Anticoagulant and Abnormal Coagulation Tests in Patients with COVID-19. N. Engl. J. Med. 2020, 383, 288–290. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, E.; Sartre, B.; Squara, F.; Contenti, J.; Occelli, C.; Lemoel, F.; Levraut, J.; Doyen, D.; Dellamonica, J.; Mondain, V.; et al. High Prevalence of Acquired Thrombophilia without Prognosis Value in Patients with Coronavirus Disease 2019. J. Am. Hear. Assoc. 2020, 9, e017773. [Google Scholar] [CrossRef] [PubMed]
- Schouwers, S.M.; Delanghe, J.R.; Devreese, K.M. Lupus Anticoagulant (LAC) testing in patients with inflammatory status: Does C-reactive protein interfere with LAC test results? Thromb. Res. 2010, 125, 102–104. [Google Scholar] [CrossRef]
- De Ocáriz, X.G.L.; Quismondo, N.C.; Guerrero, E.V.; Rodríguez, M.R.; Díaz, R.A.; López, J.M. Thrombosis and antiphospholipid antibodies in patients with SARS-CoV-2 infection (COVID-19). Int. J. Lab. Hematol. 2020, 42, e280–e282. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Antibodies | Reference Population n = 143 | COVID-19 Patients (n = 360) | |||
|---|---|---|---|---|---|
| First Sample | p-Value | Second Sample | p-Value | ||
| 1 Any aPL | 20 (14%) | 63 (17.5%) | 0.338 | 63 (17.5%) | 0.338 |
| 1 Classic aPL | 4 (2.8%) | 16 (4.4%) | 0.460 | 15 (4.2%) | 0.608 |
| 2 Anti-B2GPI IgG | 1 (0.7%) | 4 (1.1%) | 1.0 | 5 (1.4%) | 1.0 |
| 2 Anti-B2GPI IgM | 4 (2.8%) | 10 (2.8%) | 1.0 | 11 (3.1%) | 1.0 |
| 3 Anti-CL IgG | 2 (1.4%) | 8 (2.2%) | 0.732 | 12 (3.3%) | 0.368 |
| 3 Anti-CL IgM | 4 (2.8%) | 10 (2.8%) | 1.0 | 16 (4.4%) | 0.460 |
| 2 Anti-B2GPI IgA | 9 (6.3%) | 40 (11.1%) | 0.100 | 42 (11.7%) | 0.072 |
| 4 Anti-PS/PT | 7 (4.9%) | 15 (4.2%) | 0.719 | 16 (4.4%) | 0.827 |
| 4 Anti-PS/PT IgG | 4 (2.8%) | 7 (1.9%) | 0.517 | 8 (2.2%) | 0.748 |
| 4 Anti-PS/PT IgM | 3 (2.1%) | 9 (2.5%) | 1.0 | 9 (2.5%) | 1.0 |
| First Sample | Second Sample | Wicolxon Test | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antibodies | Mean | SEM | Median | IQR | Mean | SEM | Median | IQR | Hodges–Lehmann Median Difference | p–Value | Median Difference Index |
| 1 Anti-B2GPI IgG | 3.1 | 14.7 | 1.4 | (1.4–1.4) | 3.1 | 14.6 | 1.4 | (1.4–1.4) | 0 | 0.396 | 0 |
| 1 Anti-B2GPI IgM | 2.9 | 5.9 | 1.1 | (0.4–2.6) | 2.9 | 7.8 | 1 | (0.4–2.3) | −0.1 | 0.153 | −0.09 |
| 2 Anti-CL IgG | 3.9 | 16.9 | 1.6 | (1.6–1.6) | 3.8 | 16.8 | 1.6 | (1.6–1.6) | 0 | 0.275 | 0 |
| 2 Anti-CL IgM | 3.1 | 5.7 | 1.2 | (0.5–2.7) | 2.7 | 5.9 | 0.9 | (0.3–2.3) | −0.1 | 0.019 | −0.08 |
| 1 Anti-B2GPI IgA | 10.5 | 20.4 | 4.4 | (2.9–7.2) | 10.6 | 21.1 | 4.4 | (3.2–6.9) | 0.13 | 0.440 | 0.03 |
| 3 Anti-PS/PT IgG | 8 | 12.2 | 6 | (5.2–7.4) | 9 | 12.7 | 6.7 | (5.8–8.1) | 0.67 | <0.001 | 0.11 |
| 3 Anti-PS/PT IgM | 13.3 | 18.4 | 9.3 | (6.5–14.3) | 13.9 | 16.9 | 9.5 | (7–14.9) | 0.54 | 0.141 | 0.06 |
| 4 Anti-NCap-SARS-CoV2 | 34.2 | 38.6 | 14 | (1–65.3) | 70.4 | 37.3 | 95 | (31.8–101) | 39.5 | <0.001 | 2.82 |
| 5 Anti-RBD-SARS-CoV2 | 37.2 | 41.1 | 15.5 | (1–86) | 91.8 | 26.7 | 101 | (101–101) | 50.3 | <0.001 | 3.25 |
| 6 Anti-S1-SARS-CoV2 | 30.7 | 39.2 | 7.5 | (0.6–70) | 89.2 | 29.7 | 101 | (101–101) | 55 | <0.001 | 7.33 |
| 7 Anti-S2-SARS-CoV2 | 13.3 | 22.7 | 4 | (0.6–15) | 30.8 | 26.5 | 23 | (12–40) | 15.2 | <0.001 | 3.8 |
| Antibodies | Positive Patients First Sample | Positive Patients Second Sample | Weighted Kappa | 95% CI | Strength Agreement |
|---|---|---|---|---|---|
| 1 Any aPL | 63 (17.5%) | 63 (17.5%) | 0.75 | (0.66–0.84) | Moderate |
| 1 Any classic aPL | 16 (4.4%) | 15 (4.2%) | 0.90 | (0.79–1) | Strong |
| 2 Anti-B2GPI IgG | 4 (1.1%) | 5 (1.4%) | 0.89 | (0.67–1) | Strong |
| 2 Anti-B2GPI IgM | 10 (2.8%) | 11 (3.1%) | 0.85 | (0.69–1) | Strong |
| 3 Anti-CL IgG | 8 (2.2%) | 12 (3.3%) | 0.93 | (0.80–1) | Almost Perfect |
| 3 Anti-CL IgM | 10 (2.8%) | 16 (4.4%) | 0.91 | (0.78–1) | Almost Perfect |
| 2 Anti-B2GPI IgA | 40 (11.1%) | 42 (11.7%) | 0.92 | (0.85–0.98) | Almost Perfect |
| 4 Any anti-PS/PT | 15 (4.2%) | 16 (4.4%) | 0.43 | (0.20–0.65) | Weak |
| 4 Anti-PS/PT IgG | 7 (1.9%) | 8 (2.2%) | 0.52 | (0.21–0.83) | Weak |
| 4 Anti-PS/PT IgM | 9 (2.5%) | 9 (2.5%) | 0.43 | (0.14–0.72) | Weak |
| Variables | Thrombosis (n = 37) | No Thrombosis (n = 323) | p-Value | Relative Risk | 95% CI |
|---|---|---|---|---|---|
| A. Thrombosis Associated Factors. | |||||
| Sex (men) | 24 (64.9%) | 189 (58.5%) | 0.457 | ||
| Age years (median and IQR) | 54 (45.5–61.3) | 60 (47.3–70.0) | 0.050 | ||
| Diabetes | 6 (16.2%) | 31 (9.6%) | 0.209 | ||
| Smoker | 4 (10.8%) | 69 (21.4%) | 0.193 | ||
| Hypertension | 7 (18.9%) | 108 (33.4%) | 0.073 | ||
| Obesity | 13 (35.1.9%) | 87 (27.9%) | 0.292 | ||
| Treated at ICU | 5 (13.5%) | 32 (9.9%) | 0.494 | ||
| Antibodies First sample | |||||
| 1 Any aPL positive | 10 (27%) | 53 (16.4%) | 0.107 | ||
| 1 Classic aPL | 5 (13.5%) | 11 (3.4%) | 0.005 | 3.36 | 1.51–7.46 |
| 2 Anti-B2GPI IgA | 6 (16.2%) | 34 (10.5%) | 0.297 | ||
| 3 Any anti-PS/PT | 4 (10.8%) | 11 (3.4%) | 0.056 | ||
| Lupus anticoagulant (n = 67) | 5 (16.7%) | 8 (21.6%) | 0.750 | ||
| Anti-SARS-CoV2 (n = 128) | |||||
| 4 Anti-Ncap | 7 (63.6%) | 62 (53.9%) | 0.536 | ||
| 5 Anti-RBD | 8 (72.7%) | 62 (53.9%) | 0.230 | ||
| 6 Anti-S1 | 6 (54.5%) | 53 (46.1%) | 0.591 | ||
| 7 Anti-S2 | 4 (36.4%) | 40 (34.8%) | 0.916 | ||
| Antibodies Second sample | |||||
| 1 Any aPL positive | 13 (35.1%) | 50 (15.5%) | 0.003 | 2.55 | 1.38–4.74 |
| 1 Classic aPL | 5 (13.5%) | 10 (3.1%) | 0.003 | 3.59 | 1.61–7.9 |
| 2 Anti-B2GPI IgA | 8 (21.6%) | 34 (10.5%) | 0.047 | 2.09 | 1.02–4.26 |
| 3 Any anti-PS/PT | 5 (13.5%) | 11 (3.4%) | 0.005 | 3.36 | 1.51–7.46 |
| Anti-SARS-CoV2 (n = 128) | |||||
| 4 Anti-Ncap | 7 (63.6%) | 62 (53.9%) | 0.536 | ||
| 5 Anti-RBD | 8 (72.7%) | 62 (53.9%) | 0.230 | ||
| 6 Anti-S1 | 6 (54.5%) | 53 (46.1%) | 0.591 | ||
| 7 Anti-S2 | 4 (36.4%) | 40 (34.8%) | 0.916 | ||
| B. Logistic Regression Multivariate Analysis. | |||||
| Variable | Odds Ratio | 95%CI | p-Value | ||
| First serum sample | |||||
| 1 Any aPL positive | 2.33 | 1.03–5.29 | 0.043 | ||
| Hypertension | 0.49 | 0.21–1.17 | 0.107 | ||
| Age years | 0.98 | 0.96–1 | 0.067 | ||
| Second serum sample | |||||
| 1 Any aPL positive | 3.71 | 1.71–8.05 | 0.001 | ||
| Hypertension | 0.45 | 0.19–1.08 | 0.075 | ||
| Age years | 0.98 | 0.95–1 | 0.053 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil-Etayo, F.J.; Garcinuño, S.; Lalueza, A.; Díaz-Simón, R.; García-Reyne, A.; Pleguezuelo, D.E.; Cabrera-Marante, O.; Rodriguez-Frias, E.A.; Perez-Rivilla, A.; Serrano, M.; et al. Anti-Phospholipid Antibodies and COVID-19 Thrombosis: A Co-Star, Not a Supporting Actor. Biomedicines 2021, 9, 899. https://doi.org/10.3390/biomedicines9080899
Gil-Etayo FJ, Garcinuño S, Lalueza A, Díaz-Simón R, García-Reyne A, Pleguezuelo DE, Cabrera-Marante O, Rodriguez-Frias EA, Perez-Rivilla A, Serrano M, et al. Anti-Phospholipid Antibodies and COVID-19 Thrombosis: A Co-Star, Not a Supporting Actor. Biomedicines. 2021; 9(8):899. https://doi.org/10.3390/biomedicines9080899
Chicago/Turabian StyleGil-Etayo, Francisco Javier, Sara Garcinuño, Antonio Lalueza, Raquel Díaz-Simón, Ana García-Reyne, Daniel Enrique Pleguezuelo, Oscar Cabrera-Marante, Edgard Alfonso Rodriguez-Frias, Alfredo Perez-Rivilla, Manuel Serrano, and et al. 2021. "Anti-Phospholipid Antibodies and COVID-19 Thrombosis: A Co-Star, Not a Supporting Actor" Biomedicines 9, no. 8: 899. https://doi.org/10.3390/biomedicines9080899
APA StyleGil-Etayo, F. J., Garcinuño, S., Lalueza, A., Díaz-Simón, R., García-Reyne, A., Pleguezuelo, D. E., Cabrera-Marante, O., Rodriguez-Frias, E. A., Perez-Rivilla, A., Serrano, M., & Serrano, A. (2021). Anti-Phospholipid Antibodies and COVID-19 Thrombosis: A Co-Star, Not a Supporting Actor. Biomedicines, 9(8), 899. https://doi.org/10.3390/biomedicines9080899