

Importance of Desensitization for Autistic Children in Dental Practice

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Methods
Information Exchange
2.3. Questionnaire
2.4. Examination
- Data card recording of the dental experience portrayed in the video.
- Data card recording of the achievement of steps in the dental examination.
2.5. Statistical Analyses
3. Results
3.1. Questionnaire Results
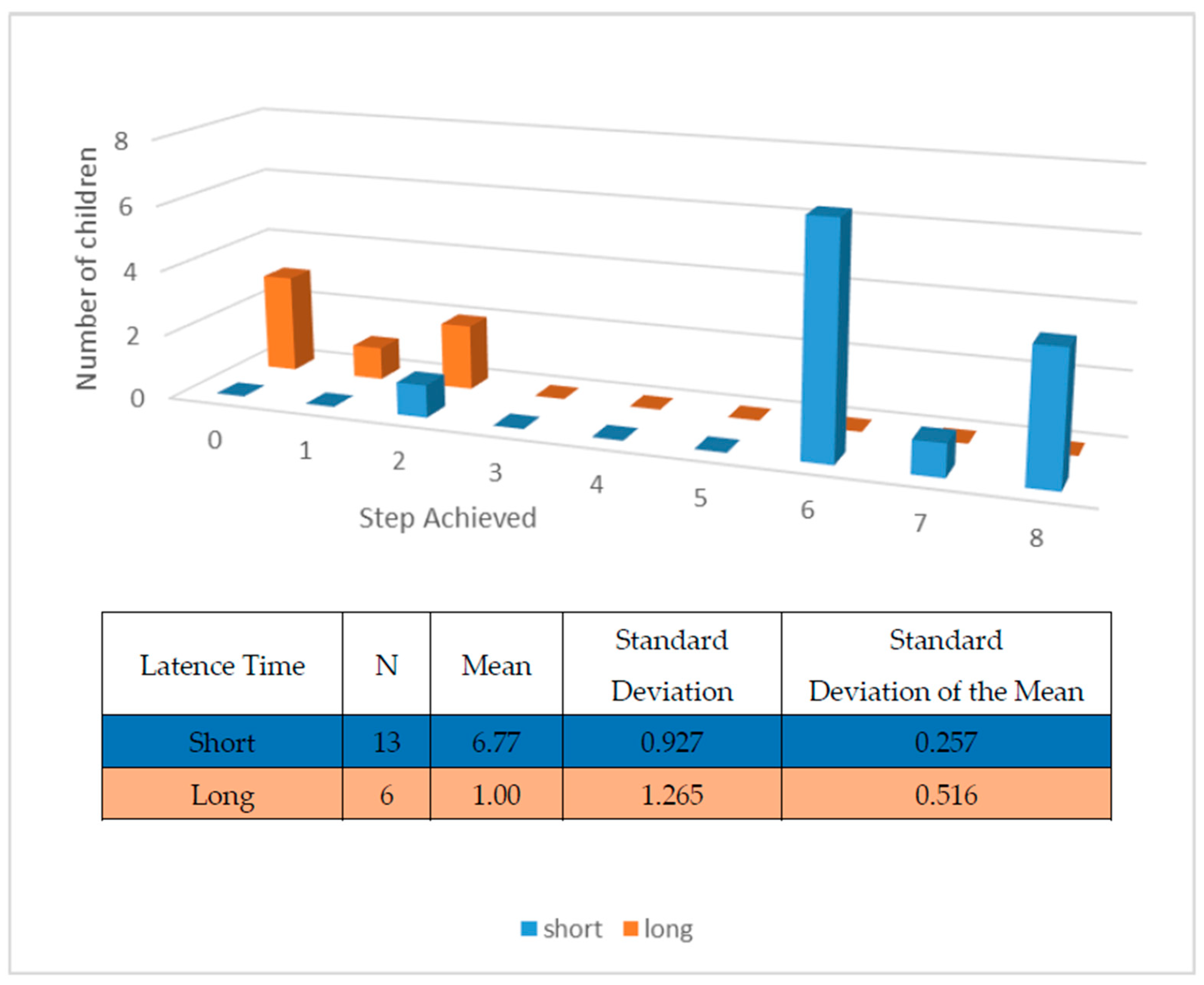
3.2. Examination Protocol Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canal, R.; Magan, M.; Bejarano, A.; De Pablos, A.; Bueno, G.; Manso, S.; Martin-Cilleros, M.V. Early detection and stability of diagnosis in autism spectrum disorders. Rev. Neurol. 2016, 62 (Suppl. S1), S15–S20. [Google Scholar]
- Miranda, A.; Baixauli, I.; Colomer, C.; Roselló, B. Autism and attention deficit hyperactivity disorder: Similarities and differences in executive functioning and theory of mind. Rev. Neurol. 2013, 57 (Suppl. S1), S177–S184. [Google Scholar]
- Barbaresi, W.J.; Katusic, S.K.; Voigt, R.G. Autism: A Review of the State of the Science for Pediatric Primary Health Care Clinicians. Arch. Pediatr. Adolesc. Med. 2006, 160, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Posserud, M.; Lundervold, A.J.; Lie, S.A.; Gillberg, C. The prevalence of autism spectrum disorders: Impact of diagnostic instrument and non-response bias. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 319–327. [Google Scholar] [CrossRef]
- Fernandes, F.D.; De La Higuera, C.A.; Cardoso, C.; Navas, A.L.; Molini-Avejonas, D.R. Reading in Autism Spectrum Disorders: A Literature Review. Folia Phoniatr. Logop. 2015, 67, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Tesini, D.A.; Fenton, S.J. Oral health needs of persons with physical or mental disabilities. Dent. Clin. N. Am. 1994, 38, 483–498. [Google Scholar] [CrossRef]
- Kopycka-Kedzierawski, D.T.; Auinger, P. Dental needs and status of autistic children: Results from the National Survey of Children’s Health. Pediatr. Dent. 2008, 30, 54–58. [Google Scholar]
- Sarnat, H.; Samuel, E.; Ashkenazi-Alfasi, N.; Peretz, B. Oral Health Characteristics of Preschool Children with Autistic Syndrome Disorder. J. Clin. Pediatr. Dent. 2016, 40, 21–25. [Google Scholar] [CrossRef]
- Luppanapornlarp, S.; Leelataweewud, P.; Putongkam, P.; Ketanont, S. Periodontal status and orthodontic treatment need of autistic children. World J. Orthod. 2010, 11, 256–261. [Google Scholar]
- Namal, N.; Vehit, H.E.; Koksal, S. Do autistic children have higher levels of caries? A cross-sectional study in Turkish children. J. Indian Soc. Pedod. Prev. Dent. 2007, 25, 97–102. [Google Scholar] [CrossRef]
- Morinushi, T.; Ueda, Y.; Tanaka, C. Autistic children: Experience and severity of dental caries between 1980 and 1995 in Kagoshima City, Japan. J. Clin. Pediatr. Dent. 2001, 25, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Shapira, J.; Mann, J.; Tamari, I.; Mester, R.; Knobler, H.; Yoeli, Y.; Newbrun, E. Oral health status and dental needs of an autistic population of children and young adults. Spec. Care Dentist. 1989, 9, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, A.; Tuchman, R.F. Antiepileptic drugs: Affective use in autism spectrum disorders. Pediatr. Neurol. 2001, 25, 199–207. [Google Scholar] [CrossRef]
- Medina, A.C.; Sogbe, R.; Gómez-Rey, A.M.; Mata, M. Factitial oral lesions in an autistic paediatric patient. Int. J. Paediatr. Dent. 2003, 13, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.C. Autoextraction of twelve permanent teeth in a child with autistic spectrum disorder. Int. J. Paediatr. Dent. 2016, 26, 157–159. [Google Scholar] [CrossRef]
- Amstrong, D.; Matt, M. Autoextraction in an autistic dental patient: A case report. Spec. Care Dent. 1999, 19, 72–74. [Google Scholar] [CrossRef]
- Klein, U.; Nowak, A.J. Characteristics of patients with autistic disorder presenting for dental treatment: A survey and chart review. Spec. Care Dentist. 1999, 19, 200–207. [Google Scholar] [CrossRef]
- Lewis, C.; Vigo, L.; Novak, L.; Klein, E.J. Listening to Parents: A Qualitative Look at the dental and oral care experiences of children with Autism Spectrum Disorder. Pediatr. Dent. 2015, 37, 98–104. [Google Scholar]
- Luscre, D.M.; Center, D.B. Procedures for reducing dental fear in children with autism. J. Autism Dev. Disord. 1996, 26, 547–556. [Google Scholar] [CrossRef]
- Loo, C.Y.; Graham, R.M.; Hughes, C.V. The caries experience and behavior of dental patients with autism spectrum disorder. J. Am. Dent. Assoc. 2008, 139, 1518–1524. [Google Scholar] [CrossRef]
- Gandhi, R.P.; Klein, U. Autism spectrum disorders: An update on oral health management. J. Evid. Based Dent. Pract. 2014, 14, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Kohlenberg, R.; Greenberg, D.; Reymore, L.; Hass, G. Behavior modification and the management of mentally retarded dental patients. J. Dent. Child. 1972, 39, 61–67. [Google Scholar]
- Marcus, A.; Wilder, D.A. A comparison of peer video modelling and self video modeling to teach textual responses in children with autism. J. Appl. Behav. Anal. 2009, 42, 335–341. [Google Scholar] [CrossRef]
- Pielbro, C.; Backman, B. Teaching oral hygiene to children with autism. Int. J. Paediatr. Dent. 2005, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bäckman, B.; Pilebro, C. Visual pedagogy in dentistry for children with autism. J. Dent. Child. 1999, 66, 325–329. [Google Scholar]
- Altabet, S.C. Decreasing dental resistance among individuals with severe and profound mental retardation. J. Dev. Phys. Disabil. 2002, 14, 297–305. [Google Scholar] [CrossRef]
- Berman, M.H. Autistic spectrum disorder: The challenge for dentists. Dent. Today 2010, 29, 96–98. [Google Scholar]
- Hernandez, P.; Ikkanda, Z. Applied behavior analysis: Behavior management of children with autism spectrum disorders in dental environments. J. Am. Dent. Assoc. 2011, 142, 281–287. [Google Scholar] [CrossRef]
- Boj, J.R.; Davila, J.M. Differences between normal and developmentally disabled children in a first dental visit. ASDC J. Dent. Child. 1995, 62, 52–56. [Google Scholar]
- Lowe, O.; Lindemann, R. Assessment of the autistic patient’s dental needs and ability to undergo dental examination. J. Dent. Child. 1985, 52, 29–34. [Google Scholar]



{kind=link}
{kind=link}
| Steps Planned in the Examination Protocol |
|---|
| 1. Sits in dental chair: seated in dental chair with legs extended but without lying back in the chair. |
| 2. Lies in dental chair: leaning with legs extended. |
| 3. Tolerates direct light on face. |
| 4. Opens mouth. |
| 5. Tolerates physical examination of the face: lets dentist manipulate the exterior of the mouth. |
| 6. Tolerates physical manipulation of the interior of the mouth. |
| 7. Opens mouth in front of a mirror. |
| 8. Tolerates examination of the interior of the mouth with the mirror, keeping the mouth wide open. |
| Steps of the Dental Examination Protocol n: 19 | Achieved without Help n (%) | Achieved with Help n (%) | Total Achieved n (%) | Not Carried out n (%) |
|---|---|---|---|---|
| 1. Sits down on dental chair | 6 (31.58%) | 10 (52.63%) | 16 (84.21%) | 3 (15.79%) |
| 2. Leans back in dental chair | 6 (31.58%) | 9 (47.37%) | 15 (78.95%) | 4 (21.05%) |
| 3. Tolerates direct light on face | 6 (31.58%) | 8 (42.11%) | 14 (73.69%) | 5 (26.31%) |
| 4. Opens mouth | 6 (31.58%) | 7 (36.84%) | 13 (68.42%) | 6 (31.58%) |
| 5. Tolerates physical examination of the face | 6 (31.58%) | 7 (36.84%) | 13 (68.42%) | 6 (31.58%) |
| 6. Tolerates physical manipulation of the mouth | 6 (31.58%) | 7 (36.4%) | 13 (68.42%) | 6 (31.58%) |
| 7. Opens mouth in front of a mirror | 3 (15.79%) | 3 (15.79%) | 6 (31.58%) | 13 (68.42%) |
| 8. Tolerates examination of the interior of mouth, keeping it wide open | 3 (15.79%) | 1 (5.26%) | 4 (21.05%) | 15 (78.95%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez Pérez, E.; Adanero Velasco, A.; Gómez Clemente, V.; Miegimolle Herrero, M.; Planells Del Pozo, P. Importance of Desensitization for Autistic Children in Dental Practice. Children 2023, 10, 796. https://doi.org/10.3390/children10050796
Martínez Pérez E, Adanero Velasco A, Gómez Clemente V, Miegimolle Herrero M, Planells Del Pozo P. Importance of Desensitization for Autistic Children in Dental Practice. Children. 2023; 10(5):796. https://doi.org/10.3390/children10050796
Chicago/Turabian StyleMartínez Pérez, Eva, Alberto Adanero Velasco, Víctor Gómez Clemente, Mónica Miegimolle Herrero, and Paloma Planells Del Pozo. 2023. "Importance of Desensitization for Autistic Children in Dental Practice" Children 10, no. 5: 796. https://doi.org/10.3390/children10050796
APA StyleMartínez Pérez, E., Adanero Velasco, A., Gómez Clemente, V., Miegimolle Herrero, M., & Planells Del Pozo, P. (2023). Importance of Desensitization for Autistic Children in Dental Practice. Children, 10(5), 796. https://doi.org/10.3390/children10050796