

Allografts for Medial Patellofemoral Ligament (MPFL) Reconstruction in Adolescent Patients with Recurrent Patellofemoral Instability: A Systematic Review

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
- Problem: recurrent patellofemoral instability;
- Population: skeletally immature patients;
- Intervention: allografts MPFL reconstruction;
- Outcomes: PROMs, return to sport, rate of complications;
- Follow-up: minimum 24 months follow-up.
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
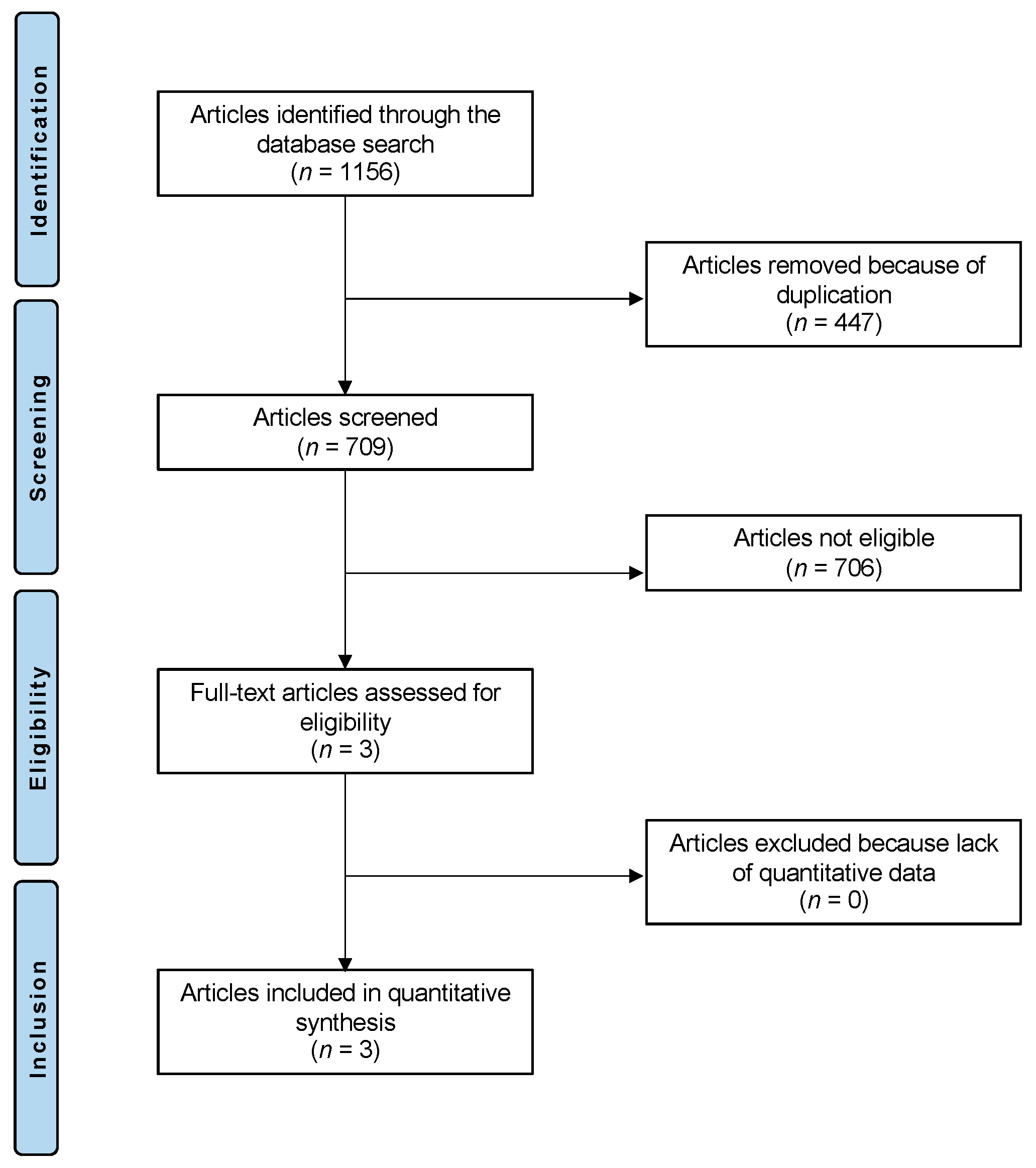
3.1. Search Result
3.2. Demographic Data and Surgical Procedures
3.3. Clinical Outcomes
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L.M. Epidemiology and natural history of acute patellar dislocation. Am. J. Sport. Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Nietosvaara, Y.; Aalto, K.; Kallio, P.E. Acute patellar dislocation in children: Incidence and associated osteochondral fractures. J. Pediatr. Orthop. 1994, 14, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Dewan, V.; Webb, M.S.L.; Prakash, D.; Malik, A.; Gella, S.; Kipps, C. When does the patella dislocate? A systematic review of biomechanical & kinematic studies. J. Orthop. 2020, 20, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Pettinari, F.; Secci, G.; Civinini, R.; Matassi, F. A rare case of osteochondral fracture of posterior aspect of lateral femoral condyle after patellar dislocation. J. Orthop. Rep. 2023, 2, 100151. [Google Scholar] [CrossRef]
- Krebs, C.; Tranovich, M.J.; Ebraheim, N. The medial patellofemoral ligament: Review of the literature. J. Orthop. 2018, 15, 596–599. [Google Scholar] [CrossRef]
- Jaquith, B.P.; Parikh, S.N. Predictors of Recurrent Patellar Instability in Children and Adolescents After First-time Dislocation. J. Pediatr. Orthop. 2017, 37, 484–490. [Google Scholar] [CrossRef]
- Desio, S.M.; Burks, R.T.; Bachus, K.N. Soft tissue restraints to lateral patellar translation in the human knee. Am. J. Sport. Med. 1998, 26, 59–65. [Google Scholar] [CrossRef]
- Migliorini, F.; Pilone, M.; Eschweiler, J.; Marsilio, E.; Hildebrand, F.; Maffulli, N. High Rates of Damage to the Medial Patellofemoral Ligament, Lateral Trochlea and Patellar Crest after Acute Patellar Dislocation: MRI Analysis. Arthroscopy 2022, 38, 2472–2479. [Google Scholar] [CrossRef]
- Beasley, L.S.; Vidal, A.F. Traumatic patellar dislocation in children and adolescents: Treatment update and literature review. Curr. Opin. Pediatr. 2004, 16, 29–36. [Google Scholar] [CrossRef]
- Boden, B.P.; Pearsall, A.W.; Garrett, W.E., Jr.; Feagin, J.A., Jr. Patellofemoral Instability: Evaluation and Management. J. Am. Acad. Orthop. Surg. 1997, 5, 47–57. [Google Scholar] [CrossRef]
- Redler, L.H.; Wright, M.L. Surgical Management of Patellofemoral Instability in the Skeletally Immature Patient. J. Am. Acad. Orthop. Surg. 2018, 26, e405–e415. [Google Scholar] [CrossRef] [PubMed]
- Kamalapathy, P.; Rush, J.K.; Montgomery, S.R., Jr.; Diduch, D.R.; Werner, B.C. A National Perspective of Patellar Instability in Children and Adolescents in the United States: MPFL Reconstruction Is Three Times Higher Than the Incidence of Isolated Lateral Release. Arthroscopy 2022, 38, 466–473.e461. [Google Scholar] [CrossRef] [PubMed]
- Giordano, M.; Falciglia, F.; Aulisa, A.G.; Guzzanti, V. Patellar dislocation in skeletally immature patients: Semitendinosous and gracilis augmentation for combined medial patellofemoral and medial patellotibial ligament reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2012, 20, 1594–1598. [Google Scholar] [CrossRef]
- Kumahashi, N.; Kuwata, S.; Tadenuma, T.; Kadowaki, M.; Uchio, Y. A “sandwich” method of reconstruction of the medial patellofemoral ligament using a titanium interference screw for patellar instability in skeletally immature patients. Arch. Orthop. Trauma Surg. 2012, 132, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Lind, M.; Enderlein, D.; Nielsen, T.; Christiansen, S.E.; Fauno, P. Clinical outcome after reconstruction of the medial patellofemoral ligament in paediatric patients with recurrent patella instability. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 666–671. [Google Scholar] [CrossRef]
- Nelitz, M.; Dreyhaupt, J.; Reichel, H.; Woelfle, J.; Lippacher, S. Anatomic reconstruction of the medial patellofemoral ligament in children and adolescents with open growth plates: Surgical technique and clinical outcome. Am. J. Sport. Med. 2013, 41, 58–63. [Google Scholar] [CrossRef]
- Nelitz, M.; Dreyhaupt, J.; Williams, S.R.M. Anatomic reconstruction of the medial patellofemoral ligament in children and adolescents using a pedicled quadriceps tendon graft shows favourable results at a minimum of 2-year follow-up. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 1210–1215. [Google Scholar] [CrossRef]
- Migliorini, F.; Driessen, A.; Quack, V.; Schenker, H.; Tingart, M.; Eschweiler, J. Correction to: Patellar fixation graft via suture anchors versus tunnel techniques during isolated MPFL reconstruction for recurrent patellofemoral instability: A systematic review of the literature. Arch. Orthop. Trauma Surg. 2021, 141, 1625–1626. [Google Scholar] [CrossRef]
- Migliorini, F.; Trivellas, A.; Driessen, A.; Quack, V.; Tingart, M.; Eschweiler, J. Correction to: Graft choice for isolated MPFL reconstruction: Gracilis versus semitendinosus. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 1255. [Google Scholar] [CrossRef]
- Migliorini, F.; Trivellas, A.; Colarossi, G.; Eschweiler, J.; Tingart, M.; Rath, B. Correction to: Single versus doublebundle patellar graft insertion for isolated MPFL reconstruction in patients with patellofemoral instability: A systematic review of the literature. Arch. Orthop. Trauma Surg. 2021, 141, 1627. [Google Scholar] [CrossRef]
- Vetrano, M.; Oliva, F.; Bisicchia, S.; Bossa, M.; De Carli, A.; Di Lorenzo, L.; Erroi, D.; Forte, A.; Foti, C.; Frizziero, A.; et al. IS Mu. LT first-time patellar dislocation guidelines. Muscles Ligaments Tendons J. 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Marcheggiani Muccioli, G.M.; Lullini, G.; Grassi, A.; Macchiarola, L.; Cammisa, E.; Maccaferri, B.; Rinaldi, V.G.; Di Paolo, S.; Zaffagnini, S. Good results are reported at 60-month follow-up after medial patello-femoral ligament reconstruction with fascia lata allograft for recurrent patellar dislocation. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Carl Heneghan Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H.; Goddard, O.; Hodgkinson, M. The 2011 Oxford CEBM Levels of Evidence. Oxf. Cent. Evid.-Based Med. Available online: https://www.cebm.net/index.aspx?o=5653 (accessed on 20 January 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Collins, N.J.; Misra, D.; Felson, D.T.; Crossley, K.M.; Roos, E.M. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res. 2011, 63 (Suppl. S11), S208–S228. [Google Scholar] [CrossRef]
- Kujala, U.M.; Jaakkola, L.H.; Koskinen, S.K.; Taimela, S.; Hurme, M.; Nelimarkka, O. Scoring of patellofemoral disorders. Arthroscopy 1993, 9, 159–163. [Google Scholar] [CrossRef]
- Matuszewski, L.; Trams, M.; Ciszewski, A.; Wilczynski, M.; Trams, E.; Jakubowski, P.; Matuszewska, A.; John, K. Medial patellofemoral ligament reconstruction in children: A comparative randomized short-term study of fascia lata allograft and gracilis tendon autograft reconstruction. Medicine 2018, 97, e13605. [Google Scholar] [CrossRef]
- Quinlan, N.J.; Tomasevich, K.M.; Mortensen, A.J.; Hobson, T.E.; Adeyemi, T.; Metz, A.K.; Aoki, S.K. Medial Patellofemoral Ligament Reconstruction in the Pediatric Population: Skeletal Immaturity Does Not Affect Functional Outcomes but Demonstrates Increased Rate of Subsequent Knee Injury. Arthrosc. Sport. Med. Rehabil. 2022, 4, e1589–e1599. [Google Scholar] [CrossRef]
- Spang, R.C.; Tepolt, F.A.; Paschos, N.K.; Redler, L.H.; Davis, E.A.; Kocher, M.S. Combined Reconstruction of the Medial Patellofemoral Ligament (MPFL) and Medial Quadriceps Tendon-Femoral Ligament (MQTFL) for Patellar Instability in Children and Adolescents: Surgical Technique and Outcomes. J. Pediatr. Orthop. 2019, 39, e54–e61. [Google Scholar] [CrossRef]
- Kaeding, C.C.; Aros, B.; Pedroza, A.; Pifel, E.; Amendola, A.; Andrish, J.T.; Dunn, W.R.; Marx, R.G.; McCarty, E.C.; Parker, R.D.; et al. Allograft Versus Autograft Anterior Cruciate Ligament Reconstruction: Predictors of Failure From a MOON Prospective Longitudinal Cohort. Sport. Health 2011, 3, 73–81. [Google Scholar] [CrossRef]
- Rhatomy, S.; Abadi, M.B.T.; Setyawan, R.; Asikin, A.I.Z.; Soekarno, N.R.; Imelda, L.G.; Budhiparama, N.C. Posterior cruciate ligament reconstruction with peroneus longus tendon versus hamstring tendon: A comparison of functional outcome and donor site morbidity. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Ellera Gomes, J.L. Medial patellofemoral ligament reconstruction for recurrent dislocation of the patella: A preliminary report. Arthroscopy 1992, 8, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Stupay, K.L.; Swart, E.; Shubin Stein, B.E. Widespread Implementation of Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Instability Maintains Functional Outcomes at Midterm to Long-Term Follow-up While Decreasing Complication Rates: A Systematic Review. Arthroscopy 2015, 31, 1372–1380. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Maffulli, N.; Vaishya, R. Patellofemoral instability: Current status and future perspectives. J. Orthop. 2023, 36, 49–50. [Google Scholar] [CrossRef]
- Nelitz, M.; Theile, M.; Dornacher, D.; Wolfle, J.; Reichel, H.; Lippacher, S. Analysis of failed surgery for patellar instability in children with open growth plates. Knee Surg. Sport. Traumatol. Arthrosc. 2012, 20, 822–828. [Google Scholar] [CrossRef]
- D’Ambrosi, R.; Corona, K.; Capitani, P.; Coccioli, G.; Ursino, N.; Peretti, G.M. Complications and Recurrence of Patellar Instability after Medial Patellofemoral Ligament Reconstruction in Children and Adolescents: A Systematic Review. Children 2021, 8, 434. [Google Scholar] [CrossRef]
- Shamrock, A.G.; Day, M.A.; Duchman, K.R.; Glass, N.; Westermann, R.W. Medial Patellofemoral Ligament Reconstruction in Skeletally Immature Patients: A Systematic Review and Meta-analysis. Orthop. J. Sport. Med. 2019, 7, 2325967119855023. [Google Scholar] [CrossRef]
- Flanigan, D.C.; Shemory, S.; Lundy, N.; Stitgen, M.; Long, J.M.; Magnussen, R.A. Medial patellofemoral ligament reconstruction with allograft versus autograft tissue results in similar recurrent dislocation risk and patient-reported outcomes. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 2099–2104. [Google Scholar] [CrossRef]
- Sharma, A.; Flanigan, D.C.; Randall, K.; Magnussen, R.A. Does Gracilis Preservation Matter in Anterior Cruciate Ligament Reconstruction? A Systematic Review. Arthroscopy 2016, 32, 1165–1173. [Google Scholar] [CrossRef]
- Berruto, M.; Ferrua, P.; Uboldi, F.; Usellini, E.; Gala, L.; Tassi, A.; Marelli, B. Medial patellofemoral ligament reconstruction with bioactive synthetic ligament is an option. A 3-year follow-up study. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 2419–2425. [Google Scholar] [CrossRef]
- Khemka, A.; Lord, S.J.; Doyle, Z.; Bosley, B.; Al Muderis, M. Minimally invasive medial patellofemoral ligament reconstruction for patellar instability using an artificial ligament: A two year follow-up. Knee 2016, 23, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.Y.F.; Golding, D.; Rozewicz, S.; Chandratreya, A. Modern synthetic material is a safe and effective alternative for medial patellofemoral ligament reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 2716–2721. [Google Scholar] [CrossRef] [PubMed]
- Nomura, E.; Horiuchi, Y.; Kihara, M. A mid-term follow-up of medial patellofemoral ligament reconstruction using an artificial ligament for recurrent patellar dislocation. Knee 2000, 7, 211–215. [Google Scholar] [CrossRef]
- Nomura, E.; Inoue, M.; Kobayashi, S. Long-term follow-up and knee osteoarthritis change after medial patellofemoral ligament reconstruction for recurrent patellar dislocation. Am. J. Sport. Med. 2007, 35, 1851–1858. [Google Scholar] [CrossRef] [PubMed]
- Suganuma, J.; Mochizuki, R.; Sugiki, T.; Inoue, Y.; Kitamura, K.; Akutsu, S.; Ono, H. Reconstruction of the Medial Patellofemoral Ligament Using a Synthetic Graft With Arthroscopic Control of Patellofemoral Congruence. Arthroscopy 2016, 32, 2259–2268. [Google Scholar] [CrossRef]
- Migliorini, F.; Eschweiler, J.; Spiezia, F.; Knobe, M.; Hildebrand, F.; Maffulli, N. Synthetic graft for medial patellofemoral ligament reconstruction: A systematic review. J. Orthop. Traumatol. 2022, 23, 41. [Google Scholar] [CrossRef]
- Nha, K.W.; Bae, J.H.; Hwang, S.C.; Nam, Y.J.; Shin, M.J.; Bhandare, N.N.; Kumar, A.; Kang, D.G.; Lee, D.Y. Medial patellofemoral ligament reconstruction using an autograft or allograft for patellar dislocation: A systematic review. Knee Surg. Relat. Res. 2019, 31, 8. [Google Scholar] [CrossRef]
- Mackay, N.D.; Smith, N.A.; Parsons, N.; Spalding, T.; Thompson, P.; Sprowson, A.P. Medial Patellofemoral Ligament Reconstruction for Patellar Dislocation: A Systematic Review. Orthop. J. Sport. Med. 2014, 2, 2325967114544021. [Google Scholar] [CrossRef]
- Schiphouwer, L.; Rood, A.; Tigchelaar, S.; Koeter, S. Complications of medial patellofemoral ligament reconstruction using two transverse patellar tunnels. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 245–250. [Google Scholar] [CrossRef]
- Dragoo, J.L.; Nguyen, M.; Gatewood, C.T.; Taunton, J.D.; Young, S. Medial Patellofemoral Ligament Repair Versus Reconstruction for Recurrent Patellar Instability: Two-Year Results of an Algorithm-Based Approach. Orthop. J. Sport. Med. 2017, 5, 2325967116689465. [Google Scholar] [CrossRef]
- Hendawi, T.; Godshaw, B.; Flowers, C.; Stephens, I.; Haber, L.; Waldron, S. Autograft vs. Allograft Comparison in Pediatric Medial Patellofemoral Ligament Reconstruction. Ochsner J. 2019, 19, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Hohn, E.; Pandya, N.K. Does the Utilization of Allograft Tissue in Medial Patellofemoral Ligament Reconstruction in Pediatric and Adolescent Patients Restore Patellar Stability? Clin. Orthop. Relat. Res. 2017, 475, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Bastrom, T.P.; Dennis, M.M.; Pennock, A.T.; Edmonds, E.W. Adolescent Medial Patellofemoral Ligament Reconstruction: A Comparison of the Use of Autograft Versus Allograft Hamstring. Orthop. J. Sport. Med. 2018, 6, 2325967118774272. [Google Scholar] [CrossRef] [PubMed]
- Matuszewski, L.; Ciszewski, A.; Wilczyński, M.; Ceynowa, M. Surgery technique of an anatomical MPFL reconstruction using allograft in children with recurrent patellar dislocation. Chir. Narz. Ruchu Ortop. Pol. 2017, 82, 78–81. [Google Scholar]
- Migliorini, F.; Trivellas, A.; Eschweiler, J.; Knobe, M.; Tingart, M.; Maffulli, N. Comparable outcome for autografts and allografts in primary medial patellofemoral ligament reconstruction for patellofemoral instability: Systematic review and meta-analysis. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 30, 1282–1291. [Google Scholar] [CrossRef]
- Calvo Rodriguez, R.; Figueroa Poblete, D.; Anastasiadis Le Roy, Z.; Etchegaray Bascur, F.; Vaisman Burucker, A.; Calvo Mena, R. Reconstruction of the medial patellofemoral ligament: Evaluation of the clinical results of autografts versus allografts. Rev. Española De Cirugía Ortopédica Y Traumatol. 2015, 59, 348–353. [Google Scholar] [CrossRef]
- Weinberger, J.M.; Fabricant, P.D.; Taylor, S.A.; Mei, J.Y.; Jones, K.J. Influence of graft source and configuration on revision rate and patient-reported outcomes after MPFL reconstruction: A systematic review and meta-analysis. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 2511–2519. [Google Scholar] [CrossRef]
- Migliorini, F.; Maffulli, N.; Bell, A.; Betsch, M. Outcomes, Return to Sport, and Failures of MPFL Reconstruction Using Autografts in Children and Adolescents with Recurrent Patellofemoral Instability: A Systematic Review. Children 2022, 9, 1892. [Google Scholar] [CrossRef]
- Slenker, N.R.; Tucker, B.S.; Pepe, M.D.; Marchetto, P.A.; Cohen, S.B. Short-/intermediate-term outcomes after medial patellofemoral ligament reconstruction in the treatment of chronic lateral patellofemoral instability. Physician Sportsmed. 2013, 41, 26–33. [Google Scholar] [CrossRef]
- Ha, J.H.; Jang, J.; Chung, S.I.; Yoon, Y. AMPK and SREBP-1c mediate the anti-adipogenic effect of beta-hydroxyisovalerylshikonin. Int. J. Mol. Med. 2016, 37, 816–824. [Google Scholar] [CrossRef]
- Shea, K.G.; Grimm, N.L.; Belzer, J.; Burks, R.T.; Pfeiffer, R. The relation of the femoral physis and the medial patellofemoral ligament. Arthroscopy 2010, 26, 1083–1087. [Google Scholar] [CrossRef] [PubMed]
- Farrow, L.D.; Alentado, V.J.; Abdulnabi, Z.; Gilmore, A.; Liu, R.W. The relationship of the medial patellofemoral ligament attachment to the distal femoral physis. Am. J. Sport. Med. 2014, 42, 2214–2218. [Google Scholar] [CrossRef] [PubMed]
- Kepler, C.K.; Bogner, E.A.; Hammoud, S.; Malcolmson, G.; Potter, H.G.; Green, D.W. Zone of injury of the medial patellofemoral ligament after acute patellar dislocation in children and adolescents. Am. J. Sport. Med. 2011, 39, 1444–1449. [Google Scholar] [CrossRef] [PubMed]
- Abouelsoud, M.M.; Abdelhady, A.; Elshazly, O. Anatomic physeal-sparing technique for medial patellofemoral ligament reconstruction in skeletally immature patients with ligamentous laxity. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Lind, M.; Nielsen, T.; Miller, L.; Sorensen, O.G.; Mygind-Klavsen, B.; Fauno, P. No Difference in Outcome Between Femoral Soft-Tissue and Screw Graft Fixation for Reconstruction of the Medial Patellofemoral Ligament: A Randomized Controlled Trial. Arthroscopy 2019, 35, 1130–1137. [Google Scholar] [CrossRef]
- Maffulli, N.; Aicale, R.; D’Addona, A.; Young, D.A.; Kader, D.F.; Oliva, F. Combined medial patellofemoral and patellotibial reconstruction with soft tissue fixation in recurrent patellar dislocation. Injury 2020, 51, 1867–1873. [Google Scholar] [CrossRef]
- Malecki, K.; Fabis, J.; Flont, P.; Niedzielski, K.R. The results of adductor magnus tenodesis in adolescents with recurrent patellar dislocation. BioMed Res. Int. 2015, 2015, 456858. [Google Scholar] [CrossRef]
- Marot, V.; Sanchis-Alfonso, V.; Perelli, S.; Gelber, P.E.; Sanchez Rabago, C.J.; Ginovart, G.; Monllau, J.C. Isolated reconstruction of medial patellofemoral ligament with an elastic femoral fixation leads to excellent clinical results. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 800–805. [Google Scholar] [CrossRef]
- Monllau, J.C.; Masferrer-Pino, A.; Ginovart, G.; Perez-Prieto, D.; Gelber, P.E.; Sanchis-Alfonso, V. Clinical and radiological outcomes after a quasi-anatomical reconstruction of medial patellofemoral ligament with gracilis tendon autograft. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 2453–2459. [Google Scholar] [CrossRef]
- Shimizu, R.; Sumen, Y.; Sakaridani, K.; Matsuura, M.; Adachi, N. Middle-to long-term outcome after medial patellofemoral ligament reconstruction with Insall’s proximal realignment for patellar instability. Asia-Pac. J. Sport. Med. Arthrosc. Rehabil. Technol. 2019, 17, 5–9. [Google Scholar] [CrossRef]
- Sobhy, M.H.; Mahran, M.A.; Kamel, E.M. Midterm results of combined patellofemoral and patellotibial ligaments reconstruction in recurrent patellar dislocation. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Marin Fermin, T.; Migliorini, F.; Kalifis, G.; Zikria, B.A.; D’Hooghe, P.; Al-Khelaifi, K.; Papakostas, E.T.; Maffulli, N. Hardware-free MPFL reconstruction in patients with recurrent patellofemoral instability is safe and effective. J. Orthop. Surg. Res. 2022, 17, 121. [Google Scholar] [CrossRef] [PubMed]
- Monk, A.P.; Doll, H.A.; Gibbons, C.L.; Ostlere, S.; Beard, D.J.; Gill, H.S.; Murray, D.W. The patho-anatomy of patellofemoral subluxation. J. Bone Jt. Surg. 2011, 93, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Boero, S.; Michelis, M.B.; Riganti, S. Use of the eight-Plate for angular correction of knee deformities due to idiopathic and pathologic physis: Initiating treatment according to etiology. J. Child. Orthop. 2011, 5, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Fabry, G.; MacEwen, G.D.; Shands, A.R., Jr. Torsion of the femur. A follow-up study in normal and abnormal conditions. J. Bone Jt. Surg. 1973, 55, 1726–1738. [Google Scholar] [CrossRef]
- Kearney, S.P.; Mosca, V.S. Selective hemiepiphyseodesis for patellar instability with associated genu valgum. J. Orthop. 2015, 12, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Mistry, H.; Metcalfe, A.; Colquitt, J.; Loveman, E.; Smith, N.A.; Royle, P.; Waugh, N. Autograft or allograft for reconstruction of anterior cruciate ligament: A health economics perspective. Knee Surg. Sport. Traumatol. Arthrosc. 2019, 27, 1782–1790. [Google Scholar] [CrossRef]
- Greis, P.E.; Koch, B.S.; Adams, B. Tibialis anterior or posterior allograft anterior cruciate ligament reconstruction versus hamstring autograft reconstruction: An economic analysis in a hospital-based outpatient setting. Arthroscopy 2012, 28, 1695–1701. [Google Scholar] [CrossRef]
- Stephen, J.M.; Kittl, C.; Williams, A.; Zaffagnini, S.; Marcheggiani Muccioli, G.M.; Fink, C.; Amis, A.A. Effect of Medial Patellofemoral Ligament Reconstruction Method on Patellofemoral Contact Pressures and Kinematics. Am. J. Sport. Med. 2016, 44, 1186–1194. [Google Scholar] [CrossRef]
- Christiansen, S.E.; Jacobsen, B.W.; Lund, B.; Lind, M. Reconstruction of the medial patellofemoral ligament with gracilis tendon autograft in transverse patellar drill holes. Arthroscopy 2008, 24, 82–87. [Google Scholar] [CrossRef]
- Fink, C.; Veselko, M.; Herbort, M.; Hoser, C. Minimally invasive reconstruction of the medial patellofemoral ligament using quadriceps tendon. Arthrosc. Tech. 2014, 3, e325–e329. [Google Scholar] [CrossRef] [PubMed]
- Saadat, A.A.; Lall, A.C.; Battaglia, M.R.; Mohr, M.R.; Maldonado, D.R.; Domb, B.G. Prevalence of Generalized Ligamentous Laxity in Patients Undergoing Hip Arthroscopy: A Prospective Study of Patients’ Clinical Presentation, Physical Examination, Intraoperative Findings, and Surgical Procedures. Am. J. Sport. Med. 2019, 47, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, T.R.; Kanakamedala, A.C.; Herbst, E.; Nagai, K.; Murphy, C.; Burnham, J.M.; Popchak, A.; Debski, R.E.; Musahl, V. Female sex is associated with greater rotatory knee laxity in collegiate athletes. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 1319–1325. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author and Year | Journal | LoE | Mean Age | Follow-Up (Months) | Girls (n) | Patients (n) | Procedures (n) |
|---|---|---|---|---|---|---|---|
| Matuszewski, et al., 2018 [27] | Arthroscopy | III | 15.00 | 24.00 | 10.00 | 22.00 | 22.00 |
| Quinlan, et al., 2022 [28] | Arthroscopy, Sports Med, Rehab | III | 15.40 | 55.20 | 19.00 | 58.00 | 67.00 |
| 13.50 | 49.20 | 9.00 | 16.00 | 17.00 | |||
| Spang, et al., 2019 [29] | J Ped Orthop | IV | 15.00 | 24.00 | 10.00 | 25.00 | 27.00 |
| Author and Year | Type of Allograft (n) | Associated Procedures (n) |
|---|---|---|
| Matuszewski, et al., 2018 [27] | fascia lata (22) | none |
| Quinlan, et al., 2022 [28] | Semitendinosus (35), gracilis (25), peroneus longus (1), tibialis anterior (1), unspecified (5) | Loose body removal (21), chondral debridement (4), OCD drilling (1) |
| Semitendinosus (11), gracilis (3), peroneus longus (1), unspecified (2) | Loose body removal (3), chondral debridement (1), partial lateral meniscectomy (1) | |
| Spang, et al., 2019 [29] | Gracilis (27) | MQTFL reconstruction (25), hemiepiphysiodesis (5) |
| PROM | At Baseline | At Last FU | MD | SE | 95% CI | T | p |
|---|---|---|---|---|---|---|---|
| Kujala Score | 75.5 ± 2.2 | 90.2 ± 6.1 | 14.7 | 0.648 | 13.4 to 15.9 | 22.7 | <0.0001 |
| IKDC | 38.9 ± 0.4 | 77.6 ± 0.4 | 38.7 | 0.1 | 38.5 to 38.8 | 684.1 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliorini, F.; Maffulli, N.; Söllner, S.; Pasurka, M.; Kubach, J.; Bell, A.; Betsch, M. Allografts for Medial Patellofemoral Ligament (MPFL) Reconstruction in Adolescent Patients with Recurrent Patellofemoral Instability: A Systematic Review. Children 2023, 10, 840. https://doi.org/10.3390/children10050840
Migliorini F, Maffulli N, Söllner S, Pasurka M, Kubach J, Bell A, Betsch M. Allografts for Medial Patellofemoral Ligament (MPFL) Reconstruction in Adolescent Patients with Recurrent Patellofemoral Instability: A Systematic Review. Children. 2023; 10(5):840. https://doi.org/10.3390/children10050840
Chicago/Turabian StyleMigliorini, Filippo, Nicola Maffulli, Stefan Söllner, Mario Pasurka, Joshua Kubach, Andreas Bell, and Marcel Betsch. 2023. "Allografts for Medial Patellofemoral Ligament (MPFL) Reconstruction in Adolescent Patients with Recurrent Patellofemoral Instability: A Systematic Review" Children 10, no. 5: 840. https://doi.org/10.3390/children10050840
APA StyleMigliorini, F., Maffulli, N., Söllner, S., Pasurka, M., Kubach, J., Bell, A., & Betsch, M. (2023). Allografts for Medial Patellofemoral Ligament (MPFL) Reconstruction in Adolescent Patients with Recurrent Patellofemoral Instability: A Systematic Review. Children, 10(5), 840. https://doi.org/10.3390/children10050840