
What Are the Implications of COVID-19 on Breastfeeding? A Synthesis of Qualitative Evidence Studies

 , ,
, ,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Exposure/Outcomes
2.3. Inclusion and Exclusion Criteria
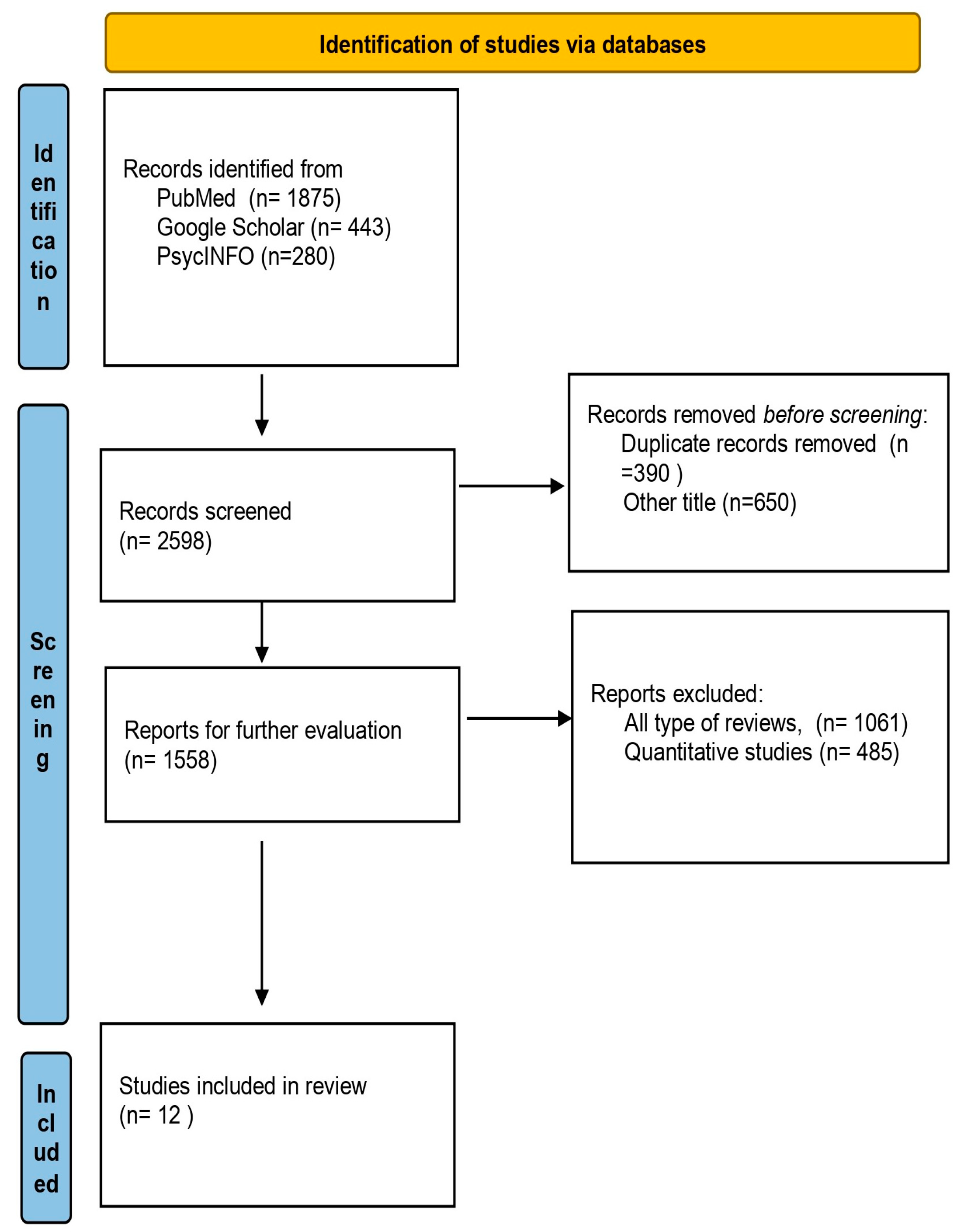
2.4. Study Selection
2.5. Study Selection
2.6. Methodological Quality of the Included Articles
3. Results
3.1. Sample Characteristics
3.2. Theme 1: Breastfeeding Support during the Pandemic
3.3. Theme 2: Effects of Social Containment Measures on Breastfeeding
3.4. Theme 3: Additional Outcomes Regarding Breastfeeding
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. WHO|Breastfeeding. Available online: http://www.who.int/nutrition/topics/exclusive_breastfeeding/en/ (accessed on 20 December 2022).
- Global Citizen. Increased Breastfeeding Could Save 800,000 Children around the World, UNICEF Says. Available online: https://www.globalcitizen.org/es/content/breastfeeding-saves-children-unicef/ (accessed on 20 December 2022).
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- The International Confederation of Midwives. Official Statements on Novel Coronavirus (COVID-19) and Pregnancy. Available online: https://internationalmidwives.org/icm-news/unfpa-statement-on-novel-coronavirus-(covid-19)-and-pregnancy.html (accessed on 2 January 2023).
- Thomas, B.; Pallivalapila, A.; El Kassem, W.; Tarannum, A.; Al Hail, F.; Rijims, M.; Parappil, H.; Bayo, A.I.; Ahmad, S.; Nazar, Z.; et al. Maternal and Perinatal Outcomes and Pharmacological Management of Covid-19 Infection in Pregnancy: A Systematic Review Protocol. Syst. Rev. 2020, 9, 161. [Google Scholar] [CrossRef] [PubMed]
- Maintaining Essential Health Services: Operational Guidance for the COVID-19 Context: Interim Guidance. 1 June 2020. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-essential_health_services-2020.2 (accessed on 3 February 2023).
- Semaan, A.; Audet, C.; Huysmans, E.; Afolabi, B.; Assarag, B.; Banke-Thomas, A.; Blencowe, H.; Caluwaerts, S.; Campbell, O.M.R.; Cavallaro, F.L.; et al. Voices from the Frontline: Findings from a Thematic Analysis of a Rapid Online Global Survey of Maternal and Newborn Health Professionals Facing the COVID-19 Pandemic. BMJ Glob. Health 2020, 5, e002967. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Disease (COVID-19): Variants of SARS-COV-2. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-variants-of-sars-cov-2 (accessed on 22 January 2023).
- Centeno-Tablante, E.; Medina-Rivera, M.; Finkelstein, J.L.; Rayco-Solon, P.; Garcia-Casal, M.N.; Rogers, L.; Ghezzi-Kopel, K.; Ridwan, P.; Peña-Rosas, J.P.; Mehta, S. Transmission of SARS-CoV-2 through Breast Milk and Breastfeeding: A Living Systematic Review. Ann. N. Y. Acad. Sci. 2021, 1484, 32–54. [Google Scholar] [CrossRef]
- Aiman, U.; Sholehah, M.; Husein, M.G. Risk Transmission through Breastfeeding and Antibody in COVID-19 Mother. Gac. Sanit. 2021, 35, S524–S529. [Google Scholar] [CrossRef]
- Breastfeeding and COVID-19. Available online: https://www.who.int/news-room/commentaries/detail/breastfeeding-and-covid-19 (accessed on 2 January 2023).
- Harriel, K.L.; Nolt, D.; Moore, S.; Kressly, S.; Bernstein, H.H. Management of Neonates after Postpartum Discharge and All Children in the Ambulatory Setting during the Coronavirus Disease 2019 (COVID-19) Pandemic. Curr. Opin. Pediatr. 2020, 32, 610–618. [Google Scholar] [CrossRef]
- Vu Hoang, D.; Cashin, J.; Gribble, K.; Marinelli, K.; Mathisen, R. Misalignment of Global COVID-19 Breastfeeding and Newborn Care Guidelines with World Health Organization Recommendations. BMJ Nutr. Prev. Health 2020, 3, 339–350. [Google Scholar] [CrossRef]
- Dona’, D.; Montagnani, C.; Di Chiara, C.; Venturini, E.; Galli, L.; Lo Vecchio, A.; Denina, M.; Olivini, N.; Bruzzese, E.; Campana, A.; et al. COVID-19 in Infants Less than 3 Months: Severe or Not Severe Disease? Viruses 2022, 14, 2256. [Google Scholar] [CrossRef]
- Latorre, G.; Martinelli, D.; Guida, P.; Masi, E.; De Benedictis, R.; Maggio, L. Impact of COVID-19 Pandemic Lockdown on Exclusive Breastfeeding in Non-Infected Mothers. Int. Breastfeed. J. 2021, 16, 36. [Google Scholar] [CrossRef]
- Lubbe, W.; Botha, E.; Niela-Vilen, H.; Reimers, P. Breastfeeding during the COVID-19 Pandemic—A Literature Review for Clinical Practice. Int. Breastfeed. J. 2020, 15, 82. [Google Scholar] [CrossRef]
- Koleilat, M.; Whaley, S.E.; Clapp, C. The Impact of COVID-19 on Breastfeeding Rates in a Low-Income Population. Breastfeed. Med. 2022, 17, 33–37. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Pandemic May Have Decreased Breastfeeding. Available online: https://www.aap.org/en/news-room/news-releases/conference-news-releases/covid-19-pandemic-may-have-decreased-breastfeeding/ (accessed on 4 February 2023).
- Matvienko-Sikar, K.; Meedya, S.; Ravaldi, C. Perinatal Mental Health during the COVID-19 Pandemic. Women Birth 2020, 33, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, N.; Mattern, E.; Cignacco, E.; Seliger, G.; König-Bachmann, M.; Striebich, S.; Ayerle, G.M. Effects of the COVID-19 Pandemic on Maternity Staff in 2020—A Scoping Review. BMC Health Serv. Res. 2021, 21, 1364. [Google Scholar] [CrossRef] [PubMed]
- Aslan, M.M.; Uslu Yuvacı, H.; Köse, O.; Toptan, H.; Akdemir, N.; Köroğlu, M.; Cevrioğlu, A.S.; Özden, S. SARS-CoV-2 Is Not Present in the Vaginal Fluid of Pregnant Women with COVID-19. J. Matern. -Fetal Neonatal Med. 2022, 35, 2876–2878. [Google Scholar] [CrossRef]
- Marín Gabriel, M.A.; Cuadrado, I.; Álvarez Fernández, B.; González Carrasco, E.; Alonso Díaz, C.; Llana Martín, I.; Sánchez, L.; Olivas, C.; de las Heras, S.; Criado, E.; et al. Multicentre Spanish Study Found No Incidences of Viral Transmission in Infants Born to Mothers with COVID-19. Acta Paediatr. 2020, 109, 2302–2308. [Google Scholar] [CrossRef] [PubMed]
- Trippella, G.; Ciarcià, M.; Ferrari, M.; Buzzatti, C.; Maccora, I.; Azzari, C.; Dani, C.; Galli, L.; Chiappini, E. COVID-19 in Pregnant Women and Neonates: A Systematic Review of the Literature with Quality Assessment of the Studies. Pathogens 2020, 9, 485. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Lockwood, C.; Porritt, K.; Munn, Z.; Rittenmeyer, L.; Salmond, S.; Bjerrum, M.; Loveday, H.; Carrier, J.; Stannard, D. Chapter 2: Systematic Reviews of Qualitative Evidence; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Turner, S.E.; Brockway, M.; Azad, M.B.; Grant, A.; Tomfohr-Madsen, L.; Brown, A. Breastfeeding in the Pandemic: A Qualitative Analysis of Breastfeeding Experiences among Mothers from Canada and the United Kingdom. Women Birth 2023, 36, e388–e396. [Google Scholar] [CrossRef]
- Vik, E.S.; Kongslien, S.; Nedberg, I.H.; Mariani, I.; Valente, E.P.; Covi, B.; Lazzerini, M. Women’s Experiences and Views on Early Breastfeeding during the COVID-19 Pandemic in Norway: Quantitative and Qualitative Findings from the IMAgiNE EURO Study. Int. Breastfeed. J. 2023, 18, 15. [Google Scholar] [CrossRef]
- Rodríguez-Gallego, I.; Strivens-Vilchez, H.; Agea-Cano, I.; Marín-Sánchez, C.; Sevillano-Giraldo, M.D.; Gamundi-Fernández, C.; Berná-Guisado, C.; Leon-Larios, F. Breastfeeding Experiences during the COVID-19 Pandemic in Spain:A Qualitative Study. Int. Breastfeed. J. 2022, 17, 11. [Google Scholar] [CrossRef]
- Aşcı, Ö.; Demirgöz Bal, M.; Ergin, A. The Breastfeeding Experiences of COVID-19-positive Women: A Qualitative Study in Turkey. Jpn. J. Nurs. Sci. 2022, 19, e12453. [Google Scholar] [CrossRef] [PubMed]
- Nuampa, S.; Ratinthorn, A.; Patil, C.L.; Kuesakul, K.; Prasong, S.; Sudphet, M. Impact of Personal and Environmental Factors Affecting Exclusive Breastfeeding Practices in the First Six Months during the COVID-19 Pandemic in Thailand: A Mixed-Methods Approach. Int. Breastfeed. J. 2022, 17, 73. [Google Scholar] [CrossRef]
- Kwan, J.; Jia, J.; Yip, K.; So, H.; Leung, S.S.F.; Ip, P.; Wong, W.H.S. A Mixed-Methods Study on the Association of Six-Month Predominant Breastfeeding with Socioecological Factors and COVID-19 among Experienced Breastfeeding Women in Hong Kong. Int. Breastfeed. J. 2022, 17, 40. [Google Scholar] [CrossRef] [PubMed]
- Agrina, A.; Afandi, D.; Suyanto, S.; Erika, E.; Dewi, Y.I.; Helina, S.; Pramita, D.; Safira, N. Analysis of Supporting Factors Associated with Exclusive Breastfeeding Practice in the Urban Setting during the COVID-19 Pandemic. Children 2022, 9, 1074. [Google Scholar] [CrossRef] [PubMed]
- Yip, K.-H.; Yip, Y.-C.; Tsui, W.-K. The Lived Experiences of Women without COVID-19 in Breastfeeding Their Infants during the Pandemic: A Descriptive Phenomenological Study. Int. J. Environ. Res. Public Health 2022, 19, 9511. [Google Scholar] [CrossRef] [PubMed]
- Igundunasse, A.; Messigah, G.O.; Odiase, N.O.; Ewelike, C. Exploring the Perceptions & Experiences of Breastfeeding Mothers During COVID 19 Lockdown. Am. J. Qual. Res. 2022, 6, 188–213. [Google Scholar] [CrossRef]
- Badr, H.; Alghamdi, S. Breastfeeding Experience among Mothers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4535. [Google Scholar] [CrossRef] [PubMed]
- Rice, K.; Williams, S. Women’s Postpartum Experiences in Canada during the COVID-19 Pandemic: A Qualitative Study. CMAJ Open 2021, 9, E556–E562. [Google Scholar] [CrossRef]
- Brown, A.; Shenker, N. Experiences of Breastfeeding during COVID-19: Lessons for Future Practical and Emotional Support. Matern. Child Nutr. 2021, 17, e13088. [Google Scholar] [CrossRef]
- Palmquist, A.E.L.; Tomori, C.; Tumlinson, K.; Fox, C.; Chung, S.; Quinn, E.A. Pandemic Policies and Breastfeeding: A Cross-Sectional Study during the Onset of COVID-19 in the United States. Front. Sociol. 2022, 7, 958108. [Google Scholar] [CrossRef]
- Shahrani, A.S.A. Does COVID-19 Policy Affect Initiation and Duration of Exclusive Breastfeeding? A Single-Center Retrospective Study. Risk Manag. Healthc. Policy 2022, 15, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Schindler-Ruwisch, J.; Phillips, K.E. Breastfeeding During a Pandemic: The Influence of COVID-19 on Lactation Services in the Northeastern United States. J. Hum. Lact. 2021, 37, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, N. Breastfeeding in India Is Disrupted as Mothers and Babies Are Separated in the Pandemic. BMJ 2020, 370, m3316. [Google Scholar] [CrossRef]
- Wolfberg, A.J.; Michels, K.B.; Shields, W.; O’Campo, P.; Bronner, Y.; Bienstock, J. Dads as Breastfeeding Advocates: Results from a Randomized Controlled Trial of an Educational Intervention. Am. J. Obstet. Gynecol. 2004, 191, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Raj, V.K.; Plichta, S.B. The Role of Social Support in Breastfeeding Promotion: A Literature Review. J. Hum. Lact. 1998, 14, 41–45. [Google Scholar] [CrossRef]
- Rempel, L.A.; Rempel, J.K.; Moore, K.C. Relationships between Types of Father Breastfeeding Support and Breastfeeding Outcomes. Matern. Child Nutr. 2017, 13, e12337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battersby, S. The role of the midwife in breastfeeding: Dichotomies and dissonance. Br. J. Midwifery 2014, 22, 551–556. Available online: https://www.britishjournalofmidwifery.com/content/clinical-practice/the-role-of-the-midwife-in-breastfeeding-dichotomies-and-dissonance/ (accessed on 8 June 2023). [CrossRef]
- Shuman, C.J.; Peahl, A.F.; Pareddy, N.; Morgan, M.E.; Chiangong, J.; Veliz, P.T.; Dalton, V.K. Postpartum Depression and Associated Risk Factors during the COVID-19 Pandemic. BMC Res. Notes 2022, 15, 102. [Google Scholar] [CrossRef]


{kind=link}
| Turner [26], 2023, Canada, UK | Vik [27], 2023, Norway | Rodríguez-Gallego [28], 2022, Spain | Aşcı [29], 2022, Turkey | Nuampa [30], 2022, Thailand | Kwan [31], 2022, Hong Kong | Agrina [32], 2022, Indonesia | Yip [33], 2022, China | Igundunasse [34], 2022, South Africa, United Kingdom, Nigeria | Badr [35], 2022, Saudi Arabia | Rice [36], 2021, Canada | Brown [37], 2021, UK | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Is there congruity between the stated philosophical perspective and the research methodology? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 2. Is there congruity between the research methodology and the research question or objectives? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 3. Is there congruity between the research methodology and the methods used to collect data? | Y | No | Y | Y | Y | U | Y | Y | Y | Y | Y | Y |
| 4. Is there congruity between the research methodology and the representation and analysis of data? | Y | U | Y | Y | Y | U | Y | Y | Y | Y | Y | Y |
| 5. Is there congruity between the research methodology and the interpretation of results? | Y | Y | Y | Y | Y | U | Y | Y | Y | Y | Y | Y |
| 6. Is there a statement locating the researcher culturally or theoretically? | U | No | No | No | U | U | Y | Y | Y | Y | Y | U |
| 7. Influence of the researcher on the research, and vice versa, is addressed | U | U | Y | U | U | U | U | Y | U | Y | No | U |
| 8. Are participants and their voices adequately represented? | Y | No | Y | Y | Y | No | No | Y | No | Y | Y | Y |
| 9. Is the research ethical according to current criteria or, for recent studies, is there evidence of ethical approval by an appropriate body? | Y | Y | Y | Y | Y | Y | Y | Y | U | Y | U | Y |
| 10. Do the conclusions drawn in the research report flow from the analysis or interpretation of the data? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Overall score | 8 | 5 | 9 | 8 | 8 | 4 | 8 | 10 | 7 | 10 | 8 | 8 |
| Author/Year | Participants | Data | Method | Data Analysis | Authors’ Conclusions |
|---|---|---|---|---|---|
| Turner [26], 2023 Canada, U.K. | 74 women from Canada 24 women from UK | 1. Pregnancy–birth cohort 2. Twitter and Instagram accounts | Semi-structured online interviews | Thematic analysis | In both Canada and the UK, new mothers need support from professionals and consistent, reliable health care and social support when breastfeeding. |
| Vik [27], 2023, Norway | 80 women | IMAgiNE EURO | Mixed method via the Internet | Systematic Text Condensation | Compared to pre-pandemic data, there is a decrease in exclusive breastfeeding at discharge during the COVID-19 pandemic in Norway. The findings should alert researchers, policy makers and clinicians in postnatal care services to improve future practices. |
| Rodríguez-Gallego [28], 2022, Spain | 30 mothers | Primary care health centers in Andalusia | Semi-structured interviews by midwives via telephone | Thematic analysis | The use of the Internet to support breastfeeding was an important factor in informing mothers during the pandemic. The role of the midwife was highlighted as quite important. The social restrictions of the pandemic had a positive effect on bundle development and breastfeeding, as a reset of their increased time spent at home. |
| Aşcı [29], 2022, Turkey | 14 mothers | Turkish Ministry of Health | Semi-structured interviews by Health care teams (midwives, nurses and family physicians) | Thematic analysis | Women diagnosed with COVID-19 believed that breast milk would protect their babies and therefore emphasized its continuation. Some mothers refused the treatment due to the fear that it penetrates breast milk. Women would like more support from midwives and psychologists. |
| Nuampa [30], 2022, Thailand | 15 mothers | Self- administered online survey | Semi-structured interviews | Thematic analysis | Informative breastfeeding support from health care providers through the participation of all family members in breastfeeding programs, especially spouses who provide essential emotional support, is a key prerequisite for breastfeeding success. |
| Kwan [31], 2022, Hong Kong | 793 mothers | Online questionnaire | Mixed methods approach | Inductive approach | Giving birth in a public hospital was associated with exclusive breastfeeding. The pandemic has also helped the continuation of breastfeeding with the support of family members and spouses. Paternity leave helped with breastfeeding. |
| Author/Year | Exposure | Breastfeeding Support | Effects of Social Containment Measures on Breastfeeding | Additional Outcomes |
|---|---|---|---|---|
| Turner [26], 2023, Canada, U.K. | Breastfeeding during the pandemic and lockdown | By midwives | Negative effect on the initiation and maintenance of breastfeeding | Increased bonding with the infant |
| Vik [27], 2023, Norway | Breastfeeding during hospitalization, during the pandemic, and lockdown | Lack of professional support Support from partner | Negative effect on the initiation and maintenance of breastfeeding | Fear of postpartum depression was reported by several women |
| Rodríguez-Gallego [28], 2022, Spain | Breastfeeding during the pandemic and lockdown | Mainly by midwives and family members | Positive effect on the initiation and maintenance of breastfeeding | Concerns about the impact of COVID-19 on their children and themselves, as well as social isolation |
| Aşcı [29], 2022, Turkey | Breastfeeding during the pandemic and lockdown | From family members and partner | Negative effect on breastfeeding | There was division among health professionals about whether they can breastfeed while on medication. There was general confusion. |
| Nuampa [30], 2022, Thailand | Breastfeeding during the pandemic and lockdown | From the staff during their hospitalization and from their partner | Positive effect on the initiation and maintenance of breastfeeding | Social isolation for nuclear families provided mothers with the opportunity to try new ways of mothering because of the reduced influence of older generations on infant feeding |
| Kwan [31], 2022, Hong Kong | Breastfeeding during the pandemic and lockdown | From family members, friends, and midwives | Positive impact on exclusive breastfeeding | Breastfeeding support organizations have been quite helpful. People working in these agencies were allowed to visit the mothers at home. |
| Agrina [32], 2022, Indonesia | Breastfeeding during the pandemic and lockdown | From family members, mainly by partners | Positive impact on exclusive breastfeeding | The work of the mother played an important role. Women who worked long hours and women with a high level of education breastfed less. |
| Yip [33], 2022, China | Breastfeeding during the pandemic and lockdown | From friends, traditional practices, online groups | Positive impact on exclusive breastfeeding | Low educational level and low socioeconomic level negatively affected breastfeeding. |
| Igundunasse [34], South Africa, United Kingdom, Nigeria | Breastfeeding during the pandemic and lockdown | From the partner | Positive impact on exclusive breastfeeding. Mothers wanted in this way to strengthen the health of their children | Most of them had a positive opinion about vaccination |
| Badr [35], 2022, Saudi Arabia | Breastfeeding during the pandemic and lockdown | From the partner and family | Positive impact on exclusive breastfeeding | Remote working has played an important role in the establishment and duration of breastfeeding |
| Rice [36], 2021, Canada | Breastfeeding during the pandemic and lockdown | From no one | Negative effect on breastfeeding | Many mothers developed symptoms of postpartum depression |
| Brown [37], 2021, UK | Breastfeeding during the pandemic and lockdown | From the partner | Negative effect on breastfeeding | Increased bonding with the infant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antoniou, E.; Tzitiridou-Chatzopoulou, M.; Voyatzaki, C.; Iliadou, M.; Eskitzis, P.; Dagla, M.; Palaska, E.; Orovou, E. What Are the Implications of COVID-19 on Breastfeeding? A Synthesis of Qualitative Evidence Studies. Children 2023, 10, 1178. https://doi.org/10.3390/children10071178
Antoniou E, Tzitiridou-Chatzopoulou M, Voyatzaki C, Iliadou M, Eskitzis P, Dagla M, Palaska E, Orovou E. What Are the Implications of COVID-19 on Breastfeeding? A Synthesis of Qualitative Evidence Studies. Children. 2023; 10(7):1178. https://doi.org/10.3390/children10071178
Chicago/Turabian StyleAntoniou, Evangelia, Maria Tzitiridou-Chatzopoulou, Chrysa Voyatzaki, Maria Iliadou, Panagiotis Eskitzis, Maria Dagla, Ermioni Palaska, and Eirini Orovou. 2023. "What Are the Implications of COVID-19 on Breastfeeding? A Synthesis of Qualitative Evidence Studies" Children 10, no. 7: 1178. https://doi.org/10.3390/children10071178
APA StyleAntoniou, E., Tzitiridou-Chatzopoulou, M., Voyatzaki, C., Iliadou, M., Eskitzis, P., Dagla, M., Palaska, E., & Orovou, E. (2023). What Are the Implications of COVID-19 on Breastfeeding? A Synthesis of Qualitative Evidence Studies. Children, 10(7), 1178. https://doi.org/10.3390/children10071178