Sleep-Disordered Breathing in Children with Recurrent Wheeze/Asthma: A Single Centre Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Anthropometry
2.3. In-Laboratory Overnight Respiratory Polygraph
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Conflicts of Interest
References
- Wilhelm, C.P.; deShazo, R.D.; Tamanna, S.; Ullah, M.I.; Skipworth, L.B. The nose, upper airway, and obstructive sleep apnea. Ann. Allergy Asthma Immunol. 2015, 115, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Zaffanello, M.; Piacentini, G.; Gasperi, E.; Maffeis, C.; Fava, C.; Bonafini, S.; Tagetti, A.; Antoniazzi, F. Snoring in a cohort of obese children: Association with palate position and nocturnal desaturations. J. Pediatr. Neonatal Individ. Med. 2016, 5. [Google Scholar] [CrossRef]
- White, D.P. The pathogenesis of obstructive sleep apnea: Advances in the past 100 years. Am. J. Respir. Cell Mol. Biol. 2006, 34, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Grime, C.; Tan, H.L. Sleep Disordered Breathing in Children. Indian J. Pediatr. 2015, 82, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, K.O.; Sedaghat, A.R.; Ishman, S.L. Trends in Inpatient Pediatric Polysomnography for Laryngomalacia and Craniofacial Anomalies. Ann. Otol. Rhinol. Laryngol. 2016, 125, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Aurora, R.N.; Lamm, C.I.; Zak, R.S.; Kristo, D.A.; Bista, S.R.; Rowley, J.A.; Casey, K.R. Practice parameters for the non-respiratory indications for polysomnography and multiple sleep latency testing for children. Sleep 2012, 35, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Brockmann, P.E.; Bertrand, P.; Castro-Rodriguez, J.A. Influence of asthma on sleep disordered breathing in children: A systematic review. Sleep Med. Rev. 2014, 18, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, T.; Castro-Rodríguez, J.A.; Brockmann, P.E. Sleep-disordered breathing in children with asthma: A systematic review on the impact of treatment. J. Asthma Allergy 2016, 9, 83–91. [Google Scholar] [PubMed]
- Guven, S.F.; Dursun, A.B.; Ciftci, B.; Erkekol, F.O.; Kurt, O.K. The prevalence of obstructive sleep apnea in patients with difficult-to-treat asthma. Asian Pac. J. Allergy Immunol. 2014, 32, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Weiss, L.N. The diagnosis of wheezing in children. Am. Fam. Physician 2008, 77, 1109–1114. [Google Scholar] [PubMed]
- Tenero, L.; Piazza, M.; Piacentini, G. Recurrent wheezing in children. Transl. Pediatr. 2016, 5, 31–36. [Google Scholar] [PubMed]
- Alkhalil, M.; Schulman, E.; Getsy, J. Obstructive sleep apnea syndrome and asthma: What are the links? J. Clin. Sleep Med. 2009, 5, 71–78. [Google Scholar] [PubMed]
- Tapia, I.E.; Marcus, C.L.; McDonough, J.M.; Kim, J.Y.; Cornaglia, M.A.; Xiao, R.; Allen, J.L. Airway Resistance in Children with Obstructive Sleep Apnea Syndrome. Sleep 2016, 39, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Schulze, J.; Biedebach, S.; Christmann, M.; Herrmann, E.; Voss, S.; Zielen, S. Impulse Oscillometry as a Predictor of Asthma Exacerbations in Young Children. Respiration 2016, 91, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Ross, K.R.; Rosen, C.L. Sleep and respiratory physiology in children. Clin. Chest Med. 2014, 35, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Felix, O.; Amaddeo, A.; Olmo Arroyo, J.; Zerah, M.; Puget, S.; Cormier-Daire, V.; Baujat, G.; Pinto, G.; Fernandez-Bolanos, M.; Fauroux, B. Central sleep apnea in children: Experience at a single center. Sleep Med. 2016, 25, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Herlenius, E. An inflammatory pathway to apnea and autonomic dysregulation. Respir. Physiol. Neurobiol. 2011, 178, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Zaffanello, M.; Piacentini, G.; Pietrobelli, A.; Fava, C.; Lippi, G.; Maffeis, C.; Gasperi, E.; Nosetti, L.; Bonafini, S.; Tagetti, A.; et al. Ambulatory clinical parameters and sleep respiratory events in a group of obese children unselected for respiratory problems. World J. Pediatr. 2017, 13, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Tagetti, A.; Bonafini, S.; Zaffanello, M.; Benetti, M.V.; Vedove, F.D.; Gasperi, E.; Cavarzere, P.; Gaudino, R.; Piacentini, G.; Minuz, P.; et al. Sleep-disordered breathing is associated with blood pressure and carotid arterial stiffness in obese children. J. Hypertens. 2017, 35, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [PubMed]
- Villa, M.P.; Pietropaoli, N.; Supino, M.C.; Vitelli, O.; Rabasco, J.; Evangelisti, M.; Del Pozzo, M.; Kaditis, A.G. Diagnosis of Pediatric Obstructive Sleep Apnea Syndrome in Settings with Limited Resources. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Scholle, S.; Wiater, A.; Scholle, H.C. Normative values of polysomnographic parameters in childhood and adolescence: Cardiorespiratory parameters. Sleep Med. 2011, 12, 988–996. [Google Scholar] [CrossRef] [PubMed]
- Delessert, A.; Espa, F.; Rossetti, A.; Lavigne, G.; Tafti, M.; Heinzer, R. Pulse wave amplitude drops during sleep are reliable surrogate markers of changes in cortical activity. Sleep 2010, 33, 1687–1692. [Google Scholar] [CrossRef] [PubMed]
- Boudewyns, A.; Abel, F.; Alexopoulos, E.; Evangelisti, M.; Kaditis, A.; Miano, S.; Villa, M.P.; Verhulst, S.L. Adenotonsillectomy to treat obstructive sleep apnea: Is it enough? Pediatr. Pulmonol. 2017, 52, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Kritzinger, F.E.; Al-Saleh, S.; Narang, I. Descriptive analysis of central sleep apnea in childhood at a single center. Pediatr. Pulmonol. 2011, 46, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Baldassari, C.M.; Kepchar, J.; Bryant, L.; Beydoun, H.; Choi, S. Changes in central apnea index following pediatric adenotonsillectomy. Otolaryngol. Head Neck Surg. 2012, 146, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Zaffanello, M.; Sala, F.; Sacchetto, L.; Gasperi, E.; Piacentini, G. Evaluation of the central sleep apnea in asymptomatic children with Chiari 1 malformation: An open question. Childs Nerv. Syst. 2017, 33, 829–832. [Google Scholar] [CrossRef] [PubMed]
- Boudewyns, A.; Van de Heyning, P.; Verhulst, S. Central apneas in children with obstructive sleep apnea syndrome: Prevalence and effect of upper airway surgery. Sleep Med. 2016, 25, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Orr, J.E.; Malhotra, A.; Sands, S.A. Pathogenesis of central and complex sleep apnea. Respirology 2017, 22, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Banno, K.; Kryger, M.H. Sleep apnea: Clinical investigations in humans. Sleep Med. 2007, 8, 400–426. [Google Scholar] [CrossRef] [PubMed]
- Shanley, L.A.; Lin, H.; Flores, G. Factors associated with length of stay for pediatric asthma hospitalizations. J. Asthma 2015, 52, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Tenero, L.; Piazza, M.; Sandri, M.; Azzali, A.; Chinellato, I.; Peroni, D.; Boner, A.; Piacentini, G. Effect of montelukast on markers of airway remodeling in children with asthma. Allergy Asthma Proc. 2016, 37, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Tenero, L.; Piazza, M.; Zanoni, L.; Bodini, A.; Peroni, D.; Piacentini, G.L. Antioxidant supplementation and exhaled nitric oxide in children with asthma. Allergy Asthma Proc. 2016, 37, e8–e13. [Google Scholar] [CrossRef] [PubMed]
- Mak, J.C.; Ho, S.P.; Ho, A.S.; Law, B.K.; Cheung, A.H.; Ho, J.C.; Ip, M.S.; Chan-Yeung, M.M. Sustained elevation of systemic oxidative stress and inflammation in exacerbation and remission of asthma. ISRN Allergy 2013, 2013, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Chien, J.W.; Lin, C.Y.; Yang, K.D.; Lin, C.H.; Kao, J.K.; Tsai, Y.G. Increased IL-17A secreting CD4+ T cells, serum IL-17 levels and exhaled nitric oxide are correlated with childhood asthma severity. Clin. Exp. Allergy 2013, 43, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Navratil, M.; Plavec, D.; Dodig, S.; Jelcic, Z.; Nogalo, B.; Erceg, D. Markers of systemic and lung inflammation in childhood asthma. J. Asthma 2009, 46, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Chrissobolis, S.; Faraci, F.M. The role of oxidative stress and NADPH oxidase in cerebrovascular disease. Trends Mol. Med. 2008, 14, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, L.; Zicari, A.M.; Occasi, F.; Perri, L.; Carnevale, R.; Angelico, F.; Del Ben, M.; Martino, F.; Nocella, C.; Savastano, V.; et al. Endothelial dysfunction and oxidative stress in children with sleep disordered breathing: Role of NADPH oxidase. Atherosclerosis 2015, 240, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Álvarez, M.L.; Terán-Santos, J.; Ordax Carbajo, E.; Cordero-Guevara, J.A.; Navazo-Egüia, A.I.; Kheirandish-Gozal, L.; Gozal, D. Reliability of home respiratory polygraphy for the diagnosis of sleep apnea in children. Chest 2015, 147, 1020–1028. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Patients | Recurrent Wheeze/Asthma | Not Asthma | Chi-Square Test | |
| N (%) | (p-Value) | |||
| Totals (% males) | 126 (56.3%) | 28 (46.4%) | 98 (59.2%) | 0.233 |
| Obesity (N (%)) | 55 (43.7%) | 6 (21.4%) | 49 (50%) | 0.007 |
| Allergy (N (%)) | 34 (27.0%) | 16 (57.1%) | 18 (18.4%) | <0.001 |
| GER (N (%)) | 3 (2.4%) | 2 (7.1%) | 1 (1%) | 0.062 |
| Physical Characteristics | Mean ± SD | Mann–Whitney Test | ||
| (p-Value) | ||||
| Age (years) | 7.8 ± 4.1 | 5.8 ± 3.4 | 8.4 ± 4.1 | 0.002 |
| Weight (kg) | 39.8 ± 28.3 | 24.5 ± 14.3 | 44.2 ± 29.8 | 0.001 |
| Weight-for-Age Percentiles | 76.3 ± 29.0 | 69.6 ± 26.9 | 78.2 ± 29.5 | 0.011 |
| Weight-for-Age Z-score | 1.13 ± 1.28 | 0.70 ± 0.98 | 1.25 ± 1.33 | 0.011 |
| Height (cm) | 127 ± 25 | 114.1 ± 20.3 | 131.3 ± 25.2 | 0.001 |
| Height-for-Age Percentiles | 65.0 ± 28.2 | 65.0 ± 29.6 | 65.0 ± 28.0 | 0.897 |
| Height-for-Age Z-score | 0.64 ± 1.2 | 0.67 ± 1.23 | 0.64 ± 1.18 | 0.963 |
| BMI (kg/m2) | 21.3 ± 7.1 | 17.6 ± 2.9 | 22.4 ± 7.6 | 0.009 |
| BMI Percentiles | 74.9 ± 29.9 | 68.0 ± 26.8 | 76.8 ± 30.7 | 0.011 |
| BMI Z-score | 1.1 ± 1.2 | 0.7 ± 1.0 | 1.2 ± 1.3 | 0.013 |
| Sleep Respiratory Results | Total (N = 126) | Recurrent Wheeze/Asthma (N = 28) | Not Asthma (N = 98) | Mann–Whitney Test |
|---|---|---|---|---|
| Mean ± SD | p-Value | |||
| eTST (h) | 8.8 ± 0.9 | 9.1 ± 1.0 | 8.7 ±0.9 | 0.020 |
| OAHI (N/h) | 2.8 ± 5.2 | 1.7 ± 1.6 | 3.1 ± 5.8 | 0.733 |
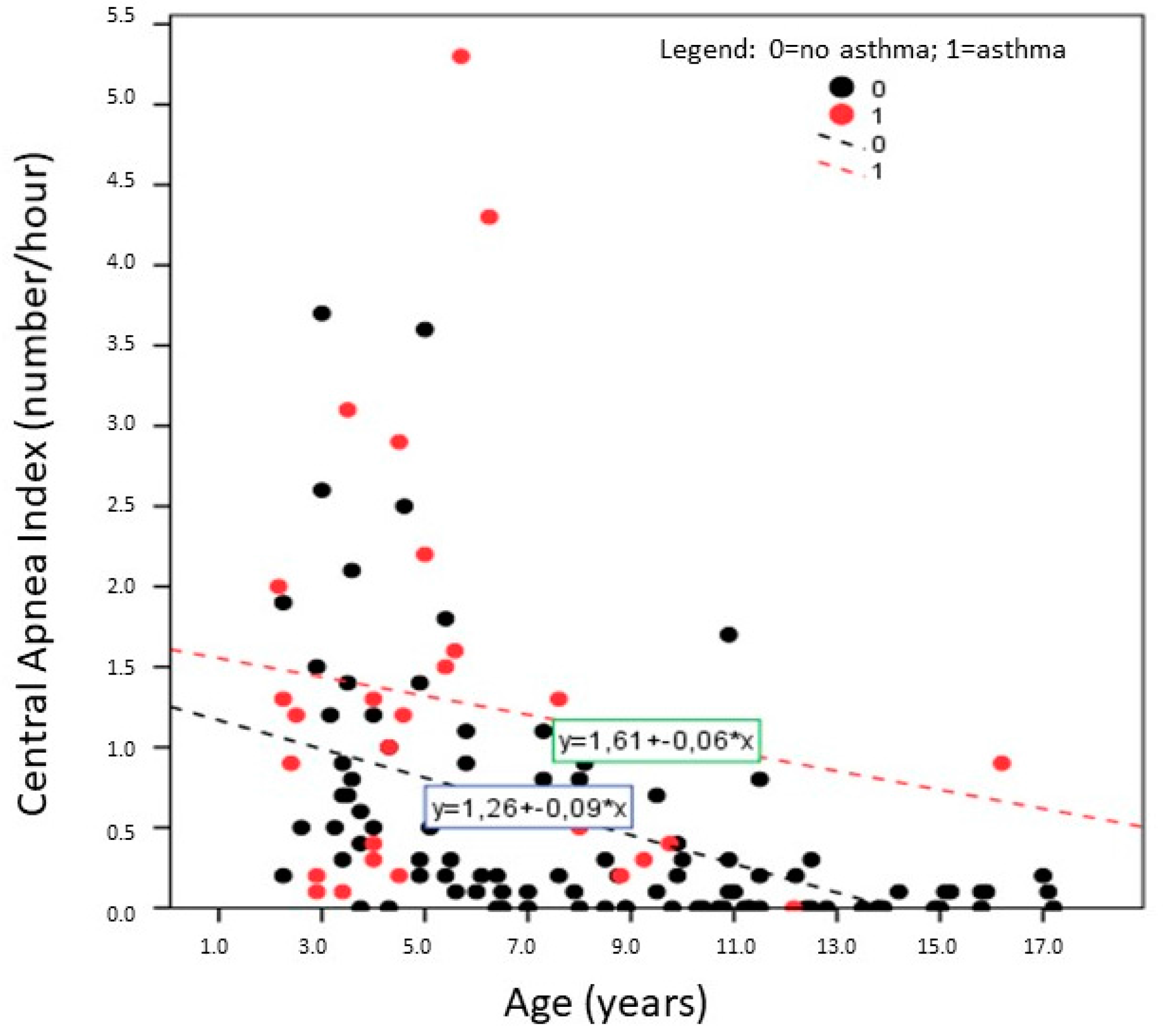
| CA (N/h) | 0.7 ± 0.9 | 1.3 ±1.3 | 0.5 ± 0.7 | <0.001 |
| ODI (N/h) | 2.1 ± 5.7 | 1.2 ± 1.4 | 2.3 ± 6.4 | 0.535 |
| Mean SpO2 (%) | 97.7 ± 0.9 | 97.6 ± 1.0 | 97.7 ± 0.9 | 0.914 |
| Min SpO2 (%) | 88.3 ± 8.3 | 87.4 ± 11.8 | 88.6 ± 7.1 | 0.580 |
| Snoring (%) | 2.2 ± 5.4 | 1.0 ± 2.4 | 2.6 ± 6.0 | 0.038 |
| Change of position (N/h) | 3.0 ± 1.8 | 3.4 ± 1.6 | 2.9 ± 1.9 | 0.173 |
| Respiratory Polygraph Variables | Total (N = 126) | Recurrent Wheeze/Asthma (N = 28) | No Asthma (N = 98) |
|---|---|---|---|
| r (p-Value) | |||
| OAHI vs. ODI | 0.807 (<0.001) | 0.407 (0.032) | 0.813 (<0.001) |
| OAHI vs. SpO2 min | −0.250 (0.005) | −0.032 (0.873) | −0.303 (<0.001) |
| OAHI vs. snoring | 0.038 (0.671) | 0.117 (0.552) | 0.022 (0.828) |
| ODI vs. SatO2 min | −0.302 (0.001) | −0.350 (0.068) | −0.378 (<0.001) |
| ODI vs. Snoring | 0.093 (0.298) | 0.480 (0.010) | 0.076 (0.459) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaffanello, M.; Gasperi, E.; Tenero, L.; Piazza, M.; Pietrobelli, A.; Sacchetto, L.; Antoniazzi, F.; Piacentini, G. Sleep-Disordered Breathing in Children with Recurrent Wheeze/Asthma: A Single Centre Study. Children 2017, 4, 97. https://doi.org/10.3390/children4110097
Zaffanello M, Gasperi E, Tenero L, Piazza M, Pietrobelli A, Sacchetto L, Antoniazzi F, Piacentini G. Sleep-Disordered Breathing in Children with Recurrent Wheeze/Asthma: A Single Centre Study. Children. 2017; 4(11):97. https://doi.org/10.3390/children4110097
Chicago/Turabian StyleZaffanello, Marco, Emma Gasperi, Laura Tenero, Michele Piazza, Angelo Pietrobelli, Luca Sacchetto, Franco Antoniazzi, and Giorgio Piacentini. 2017. "Sleep-Disordered Breathing in Children with Recurrent Wheeze/Asthma: A Single Centre Study" Children 4, no. 11: 97. https://doi.org/10.3390/children4110097
APA StyleZaffanello, M., Gasperi, E., Tenero, L., Piazza, M., Pietrobelli, A., Sacchetto, L., Antoniazzi, F., & Piacentini, G. (2017). Sleep-Disordered Breathing in Children with Recurrent Wheeze/Asthma: A Single Centre Study. Children, 4(11), 97. https://doi.org/10.3390/children4110097