How Do We Monitor Oxygenation during the Management of PPHN? Alveolar, Arterial, Mixed Venous Oxygen Tension or Peripheral Saturation?


Abstract
:1. Introduction
2. Discussion
2.1. Relation of PO2 and Fetal PVR
2.2. Gestational Age, Fetal PVR, and PO2
2.3. Effect of PO2 on PVR at Birth
2.4. Oxygen and Hypoxic Pulmonary Vasoconstriction (HPV)
2.5. Supplemental Oxygen and PO2 during the Transition
2.6. Oxygen Tension in Spontaneous Air Breathing Infants
2.7. Oxygen Tension and PPHN
2.8. Alveolar PAO2 and its Effect on PPHN
2.9. Arterial Oxygen Tension and Its Effect on PPHN
3. Post-Ductal PaO2 (PDPaO2) and PPHN
3.1. Mixed Venous Oxygen Tension (PvO2) and Management of PPHN
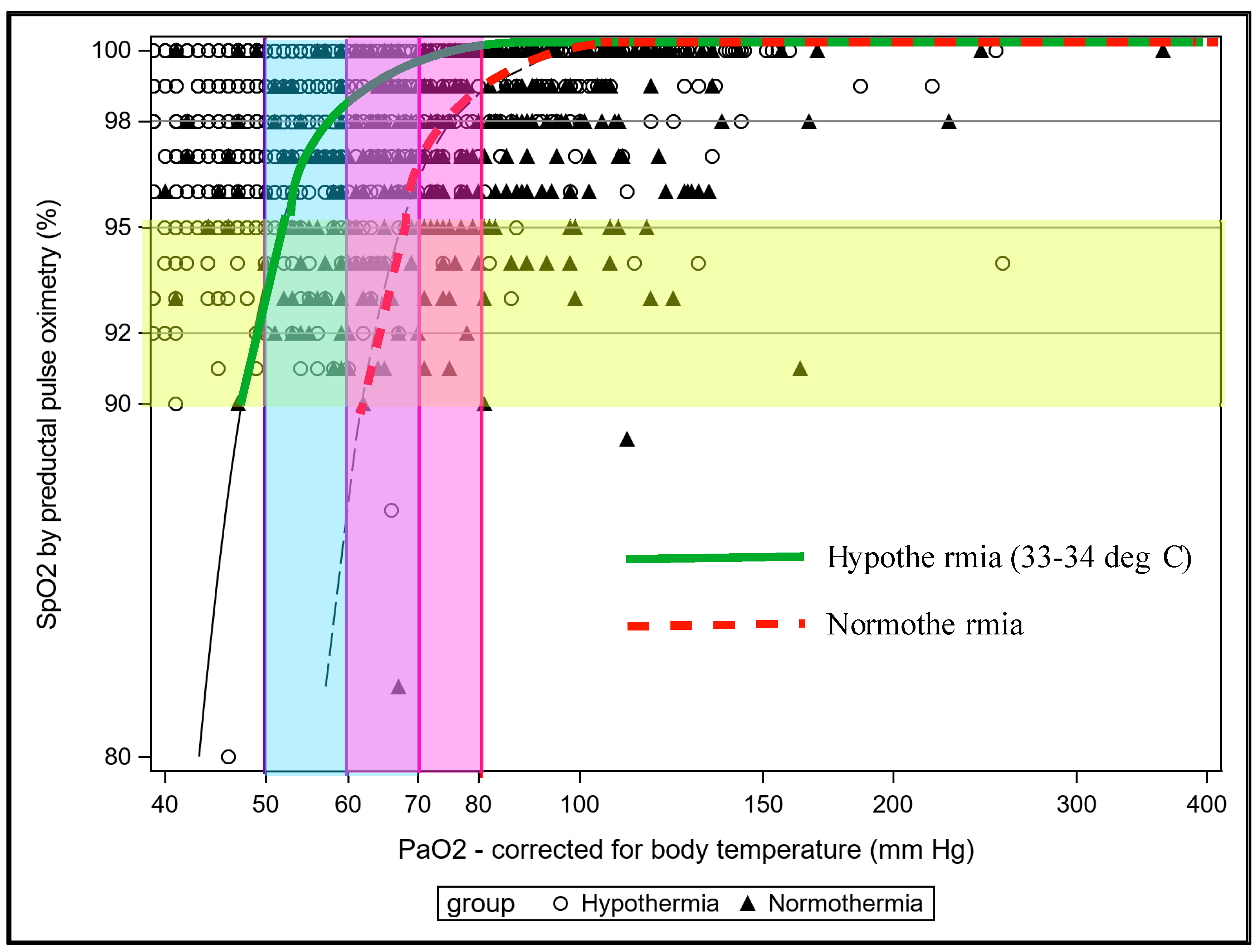
3.2. Effect of Transfusion, pH and Temperature on Relationship between SpO2 and PaO2 in PPHN
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abman, S.H.; Hansmann, G.; Archer, S.L.; Ivy, D.D.; Adatia, I.; Chung, W.K.; Hanna, B.D.; Rosenzweig, E.B.; Raj, J.U.; Cornfield, D.; et al. Pediatric Pulmonary Hypertension: Guidelines From the American Heart Association and American Thoracic Society. Circulation 2015, 132, 2037–2099. [Google Scholar] [CrossRef]
- Evans, N.J.; Archer, L.N. Doppler assessment of pulmonary artery pressure and extrapulmonary shunting in the acute phase of hyaline membrane disease. Arch. Dis. Child. 1991, 66, 6–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halliday, H.; Hirschfeld, S.; Riggs, T.; Liebman, J.; Fanaroff, A.; Bormuth, C. Respiratory distress syndrome: Echocardiographic assessment of cardiovascular function and pulmonary vascular resistance. Pediatrics 1977, 60, 444–449. [Google Scholar] [PubMed]
- Skinner, J.R.; Boys, R.J.; Hunter, S.; Hey, E.N. Pulmonary and systemic arterial pressure in hyaline membrane disease. Arch. Dis. Child. 1992, 67, 366–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walther, F.J.; Benders, M.J.; Leighton, J.O. Persistent pulmonary hypertension in premature neonates with severe respiratory distress syndrome. Pediatrics 1992, 90, 899–904. [Google Scholar]
- Mourani, P.M.; Abman, S.H. Pulmonary vascular disease in bronchopulmonary dysplasia: Pulmonary hypertension and beyond. Curr. Opin. Pediatr. 2013, 25, 329–337. [Google Scholar] [CrossRef]
- Mourani, P.M.; Abman, S.H. Pulmonary Hypertension and Vascular Abnormalities in Bronchopulmonary Dysplasia. Clin. Perinatol. 2015, 42, 839–855. [Google Scholar] [CrossRef] [Green Version]
- Mourani, P.M.; Ivy, D.D.; Gao, D.; Abman, S.H. Pulmonary vascular effects of inhaled nitric oxide and oxygen tension in bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2004, 170, 1006–1013. [Google Scholar] [CrossRef]
- Walsh-Sukys, M.C.; Tyson, J.E.; Wright, L.L.; Bauer, C.R.; Korones, S.B.; Stevenson, D.K.; Verter, J.; Stoll, B.J.; Lemons, J.A.; Papile, L.A.; et al. Persistent pulmonary hypertension of the newborn in the era before nitric oxide: Practice variation and outcomes. Pediatrics 2000, 105, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Inhaled nitric oxide in term and near-term infants: Neurodevelopmental follow-up of the neonatal inhaled nitric oxide study group (NINOS). J. Pediatr. 2000, 136, 611–617. [CrossRef]
- Konduri, G.G.; Vohr, B.; Robertson, C.; Sokol, G.M.; Solimano, A.; Singer, J.; Ehrenkranz, R.A.; Singhal, N.; Wright, L.L.; Van Meurs, K.; et al. Early inhaled nitric oxide therapy for term and near-term newborn infants with hypoxic respiratory failure: Neurodevelopmental follow-up. J. Pediatr. 2007, 150, 235–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakshminrusimha, S.; Swartz, D.D.; Gugino, S.F.; Ma, C.X.; Wynn, K.A.; Ryan, R.M.; Russell, J.A.; Steinhorn, R.H. Oxygen concentration and pulmonary hemodynamics in newborn lambs with pulmonary hypertension. Pediatr. Res. 2009, 66, 539–544. [Google Scholar] [CrossRef] [Green Version]
- Rudolph, A.M.; Heyman, M.A. Fetal and neonatal circulation and respiration. Annu. Rev. Physiol. 1974, 36, 187–207. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, A.M.; Heymann, M.A. The fetal circulation. Annu. Rev. Med. 1968, 19, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, A.M.; Yuan, S. Response of the pulmonary vasculature to hypoxia and H+ ion concentration changes. J. Clin. Investig. 1966, 45, 399–411. [Google Scholar] [CrossRef]
- Sorensen, A.; Holm, D.; Pedersen, M.; Tietze, A.; Stausbol-Gron, B.; Duus, L.; Uldbjerg, N. Left-right difference in fetal liver oxygenation during hypoxia estimated by BOLD MRI in a fetal sheep model. Ultrasound Obstet. Gynecol. 2011, 38, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekharan, P.; Lakshminrusimha, S. Oxygen therapy in preterm infants with pulmonary hypertension. Semin. Fetal Neonatal Med. 2020, 25, 101070. [Google Scholar] [CrossRef]
- Villanueva, M.E.; Zaher, F.M.; Svinarich, D.M.; Konduri, G.G. Decreased gene expression of endothelial nitric oxide synthase in newborns with persistent pulmonary hypertension. Pediatr. Res. 1998, 44, 338–343. [Google Scholar] [CrossRef] [Green Version]
- Lewis, A.B.; Heymann, M.A.; Rudolph, A.M. Gestational changes in pulmonary vascular responses in fetal lambs in utero. Circ. Res. 1976, 39, 536–541. [Google Scholar] [CrossRef] [Green Version]
- Rasanen, J.; Wood, D.C.; Debbs, R.H.; Cohen, J.; Weiner, S.; Huhta, J.C. Reactivity of the human fetal pulmonary circulation to maternal hyperoxygenation increases during the second half of pregnancy: A randomized study. Circulation 1998, 97, 257–262. [Google Scholar] [CrossRef] [Green Version]
- Teitel, D.F.; Iwamoto, H.S.; Rudolph, A.M. Changes in the pulmonary circulation during birth-related events. Pediatr. Res. 1990, 27, 372–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakshminrusimha, S. The pulmonary circulation in neonatal respiratory failure. Clin. Perinatol. 2012, 39, 655–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumb, A.B.; Slinger, P. Hypoxic pulmonary vasoconstriction: Physiology and anesthetic implications. Anesthesiology 2015, 122, 932–946. [Google Scholar] [CrossRef] [PubMed]
- Moudgil, R.; Michelakis, E.D.; Archer, S.L. Hypoxic pulmonary vasoconstriction. J. Appl. Physiol. (1985) 2005, 98, 390–403. [Google Scholar] [CrossRef]
- American Academy of Pediatrics and American Heart Association. Textbook of Neonatal Resuscitation (NRP), 7th ed.; American Academy of Pediatrics and American Heart Association: Elk Grove Village, IL, USA, 2016; p. 326. [Google Scholar]
- Lakshminrusimha, S.; Manja, V.; Mathew, B.; Suresh, G.K. Oxygen targeting in preterm infants: A physiological interpretation. J. Perinatol. 2015, 35, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Castillo, A.; Sola, A.; Baquero, H.; Neira, F.; Alvis, R.; Deulofeut, R.; Critz, A. Pulse oxygen saturation levels and arterial oxygen tension values in newborns receiving oxygen therapy in the neonatal intensive care unit: Is 85% to 93% an acceptable range? Pediatrics 2008, 121, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.J.; Okken, A.; Rubin, D. Arterial oxygen tension during active and quiet sleep in the normal neonate. J. Pediatr. 1979, 94, 271–274. [Google Scholar] [CrossRef]
- Bachman, T.E.; Iyer, N.P.; Newth, C.J.L.; Ross, P.A.; Khemani, R.G. Thresholds for oximetry alarms and target range in the NICU: An observational assessment based on likely oxygen tension and maturity. BMC Pediatr. 2020, 20, 317. [Google Scholar] [CrossRef]
- Lakshminrusimha, S.; Steinhorn, R.H.; Wedgwood, S.; Savorgnan, F.; Nair, J.; Mathew, B.; Gugino, S.F.; Russell, J.A.; Swartz, D.D. Pulmonary hemodynamics and vascular reactivity in asphyxiated term lambs resuscitated with 21 and 100% oxygen. J. Appl. Physiol. (1985) 2011, 111, 1441–1447. [Google Scholar] [CrossRef]
- Custer, J.R.; Hales, C.A. Influence of alveolar oxygen on pulmonary vasoconstriction in newborn lambs versus sheep. Am. Rev. Respir. Dis. 1985, 132, 326–331. [Google Scholar] [CrossRef]
- Lakshminrusimha, S.; Russell, J.A.; Steinhorn, R.H.; Swartz, D.D.; Ryan, R.M.; Gugino, S.F.; Wynn, K.A.; Kumar, V.H.; Mathew, B.; Kirmani, K.; et al. Pulmonary hemodynamics in neonatal lambs resuscitated with 21%, 50%, and 100% oxygen. Pediatr. Res. 2007, 62, 313–318. [Google Scholar] [CrossRef] [Green Version]
- Lakshminrusimha, S.; Kinsella, J.P.; Krishnan, U.S.; Van Meurs, K.; Edwards, E.M.; Bhatt, D.R.; Chandrasekharan, P.; Oei, J.L.; Manja, V.; Ramanathan, R.; et al. Just Say No to iNO in Preterms-Really? J. Pediatr. 2020, 218, 243–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinsella, J.P.; Ivy, D.D.; Abman, S.H. Ontogeny of NO activity and response to inhaled NO in the developing ovine pulmonary circulation. Am. J. Physiol. 1994, 267, H1955–H1961. [Google Scholar] [CrossRef] [PubMed]
- Lesneski, A.; Hardie, M.; Ferrier, W.; Lakshminrusimha, S.; Vali, P. Bidirectional Ductal Shunting and Preductal to Postductal Oxygenation Gradient in Persistent Pulmonary Hypertension of the Newborn. Children 2020, 7, 137. [Google Scholar] [CrossRef] [PubMed]
- Rawat, M.; Chandrasekharan, P.; Gugino, S.F.; Koenigsknecht, C.; Nielsen, L.; Wedgwood, S.; Mathew, B.; Nair, J.; Steinhorn, R.; Lakshminrusimha, S. Optimal Oxygen Targets in Term Lambs with Meconium Aspiration Syndrome and Pulmonary Hypertension. Am. J. Respir. Cell Mol. Biol. 2020, 63, 510–518. [Google Scholar] [CrossRef]
- Barrington, K.J. Umbilical artery catheters in the newborn: Effects of position of the catheter tip. Cochrane Database Syst. Rev. 2000, CD000505. [Google Scholar] [CrossRef]
- Plotz, F.B.; van Lingen, R.A.; Bos, A.P. Venous oxygen measurements in the inferior vena cava in neonates with respiratory failure. Crit. Care 1998, 2, 57–60. [Google Scholar] [CrossRef] [Green Version]
- Yapakci, E.; Ecevit, A.; Ince, D.A.; Gokdemir, M.; Tekindal, M.A.; Gulcan, H.; Tarcan, A. Inferior Vena Cava Oxygen Saturation during the First Three Postnatal Days in Preterm Newborns with and without Patent Ductus Arteriosus. Balk. Med. J. 2014, 31, 230–234. [Google Scholar] [CrossRef]
- Chandrasekharan, P.; Rawat, M.; Gugino, S.F.; Koenigsknecht, C.; Helman, J.; Nair, J.; Vali, P.; Lakshminrusimha, S. Effect of various inspired oxygen concentrations on pulmonary and systemic hemodynamics and oxygenation during resuscitation in a transitioning preterm model. Pediatr. Res. 2018, 84, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Rawat, M.; Chandrasekharan, P.K.; Swartz, D.D.; Mathew, B.; Nair, J.; Gugino, S.F.; Koenigsknecht, C.; Vali, P.; Lakshminrusimha, S. Neonatal resuscitation adhering to oxygen saturation guidelines in asphyxiated lambs with meconium aspiration. Pediatr. Res. 2016, 79, 583–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, J.A.; Rudenski, A.; Gibson, J.; Howard, L.; O’Driscoll, R. Relating oxygen partial pressure, saturation and content: The haemoglobin-oxygen dissociation curve. Breathe (Sheff) 2015, 11, 194–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afzal, B.; Chandrasekharan, P.; Tancredi, D.J.; Russell, J.; Steinhorn, R.H.; Lakshminrusimha, S. Monitoring Gas Exchange During Hypothermia for Hypoxic-Ischemic Encephalopathy. Pediatr. Crit. Care Med. 2019, 20, 166–171. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | O2 (%) | PaCO2 (mmHg) * | PaO2 (mm Hg) * | PVR (mmHg/mL/kg/min) * | PAO2 (mmHg) Calculated * |
|---|---|---|---|---|---|
| Control | 21 | 42 ± 2 | 57 ± 6 | 0.28 ± 0.01 | 94.5 ± 6.2 |
| PPHN | 21 | 44 ± 3 | 23 ± 2 | 1.6 ± 0.2 | 92.0 ± 5.3 |
| PPHN | 50 | 39 ± 3 | 36 ± 8 | 1.0 ± 0.1 | 301.3 ± 11.3 |
| PPHN | 100 | 47 ± 5 | 40 ± 5 | 1.0 ± 0.1 | 641.3 ± 10.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandrasekharan, P.; Rawat, M.; Lakshminrusimha, S. How Do We Monitor Oxygenation during the Management of PPHN? Alveolar, Arterial, Mixed Venous Oxygen Tension or Peripheral Saturation? Children 2020, 7, 180. https://doi.org/10.3390/children7100180
Chandrasekharan P, Rawat M, Lakshminrusimha S. How Do We Monitor Oxygenation during the Management of PPHN? Alveolar, Arterial, Mixed Venous Oxygen Tension or Peripheral Saturation? Children. 2020; 7(10):180. https://doi.org/10.3390/children7100180
Chicago/Turabian StyleChandrasekharan, Praveen, Munmun Rawat, and Satyan Lakshminrusimha. 2020. "How Do We Monitor Oxygenation during the Management of PPHN? Alveolar, Arterial, Mixed Venous Oxygen Tension or Peripheral Saturation?" Children 7, no. 10: 180. https://doi.org/10.3390/children7100180
APA StyleChandrasekharan, P., Rawat, M., & Lakshminrusimha, S. (2020). How Do We Monitor Oxygenation during the Management of PPHN? Alveolar, Arterial, Mixed Venous Oxygen Tension or Peripheral Saturation? Children, 7(10), 180. https://doi.org/10.3390/children7100180