Congenital Syphilis: A U.S. Perspective



Abstract
:1. Introduction
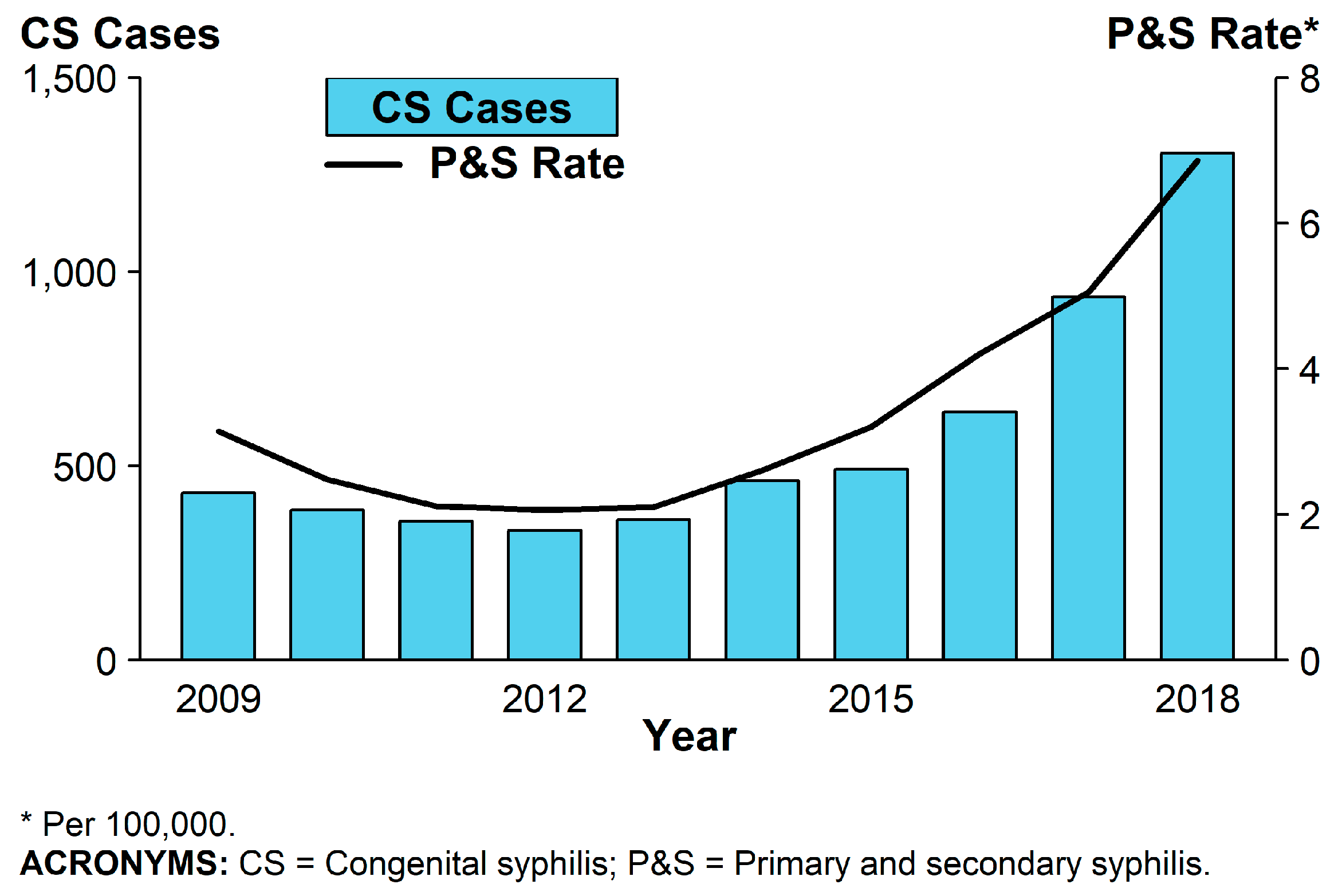
2. Epidemiology
3. Biology of Treponema Pallidum
4. Clinical Manifestations
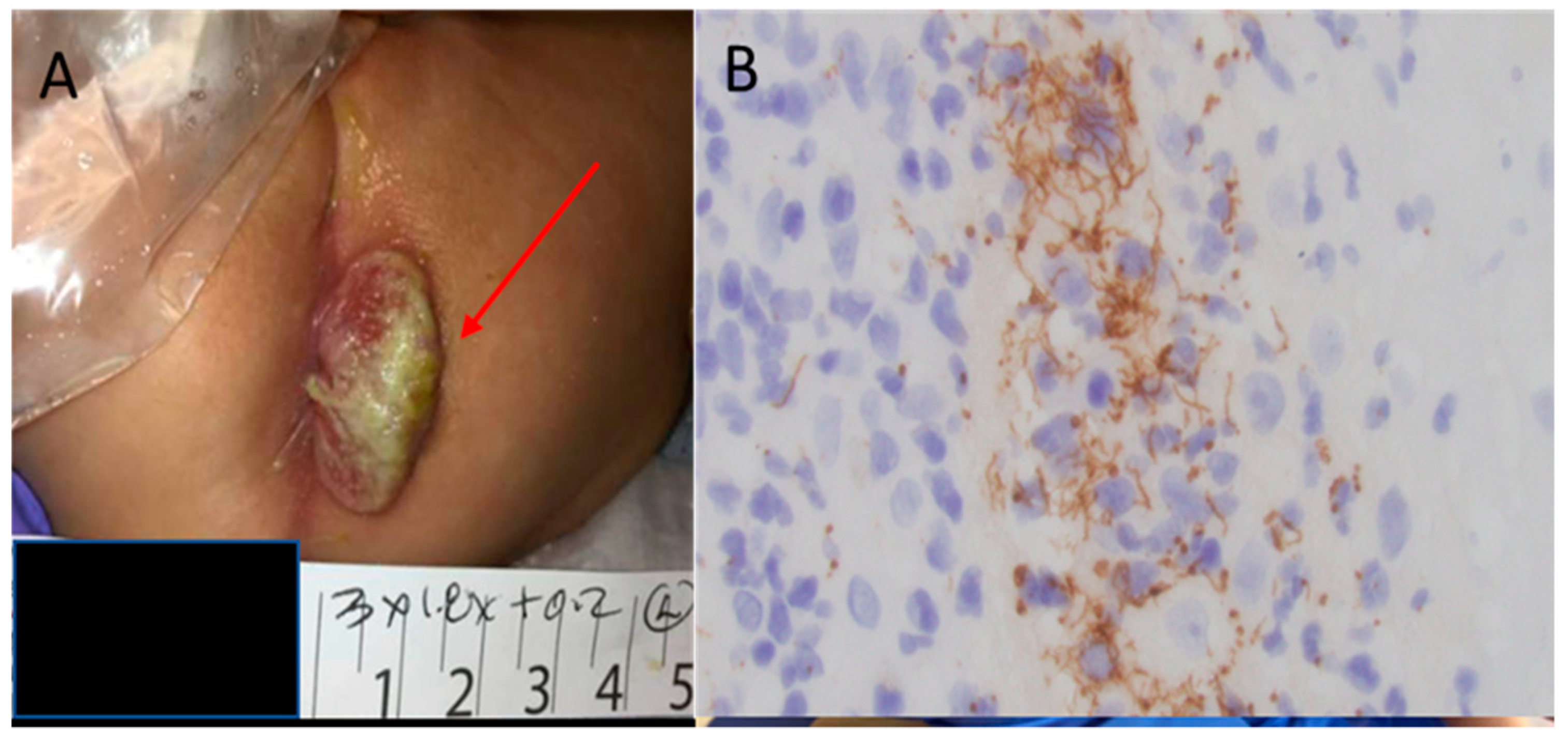
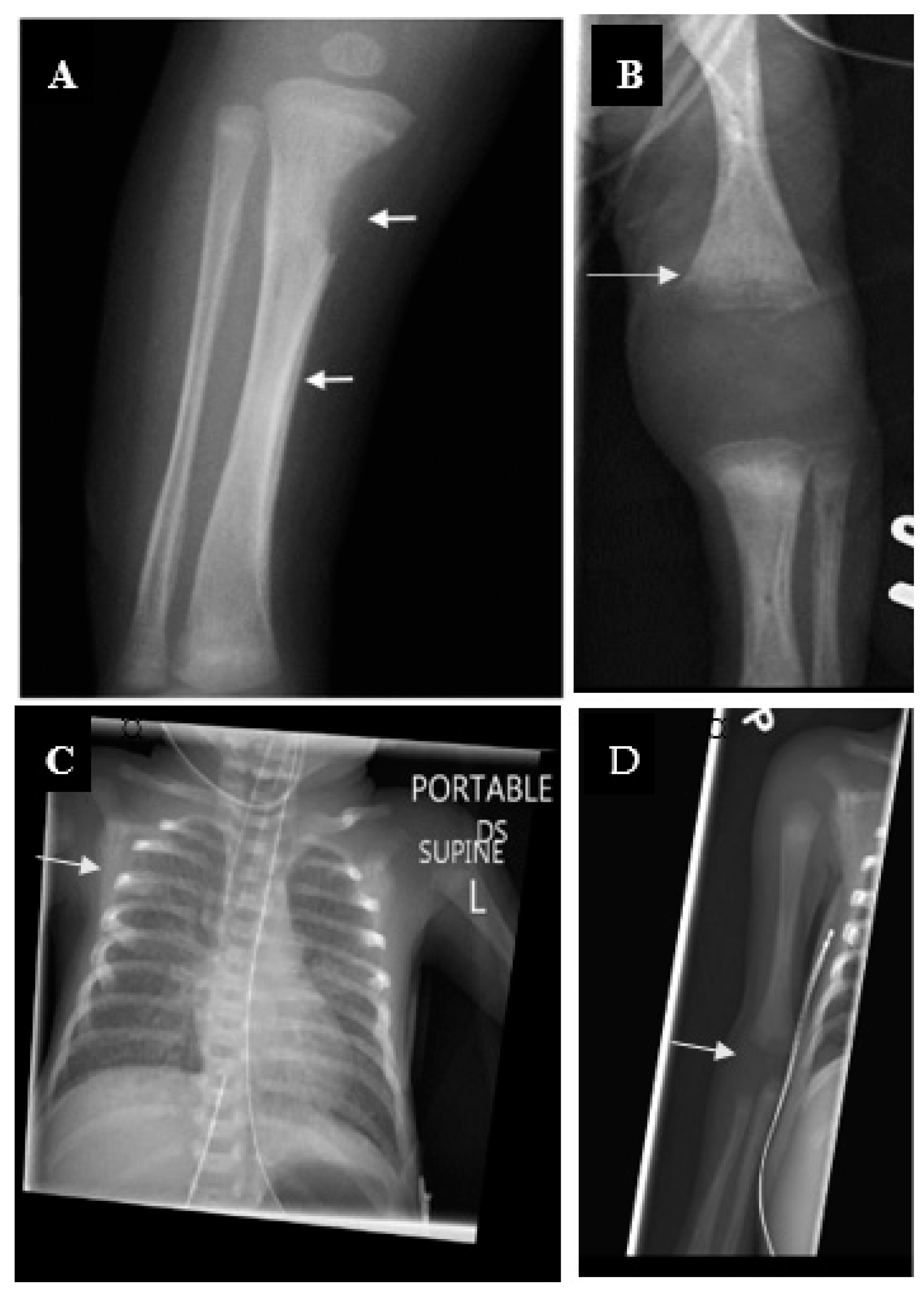
4.1. Early Congenital Syphilis
4.2. Late Congenital Syphilis
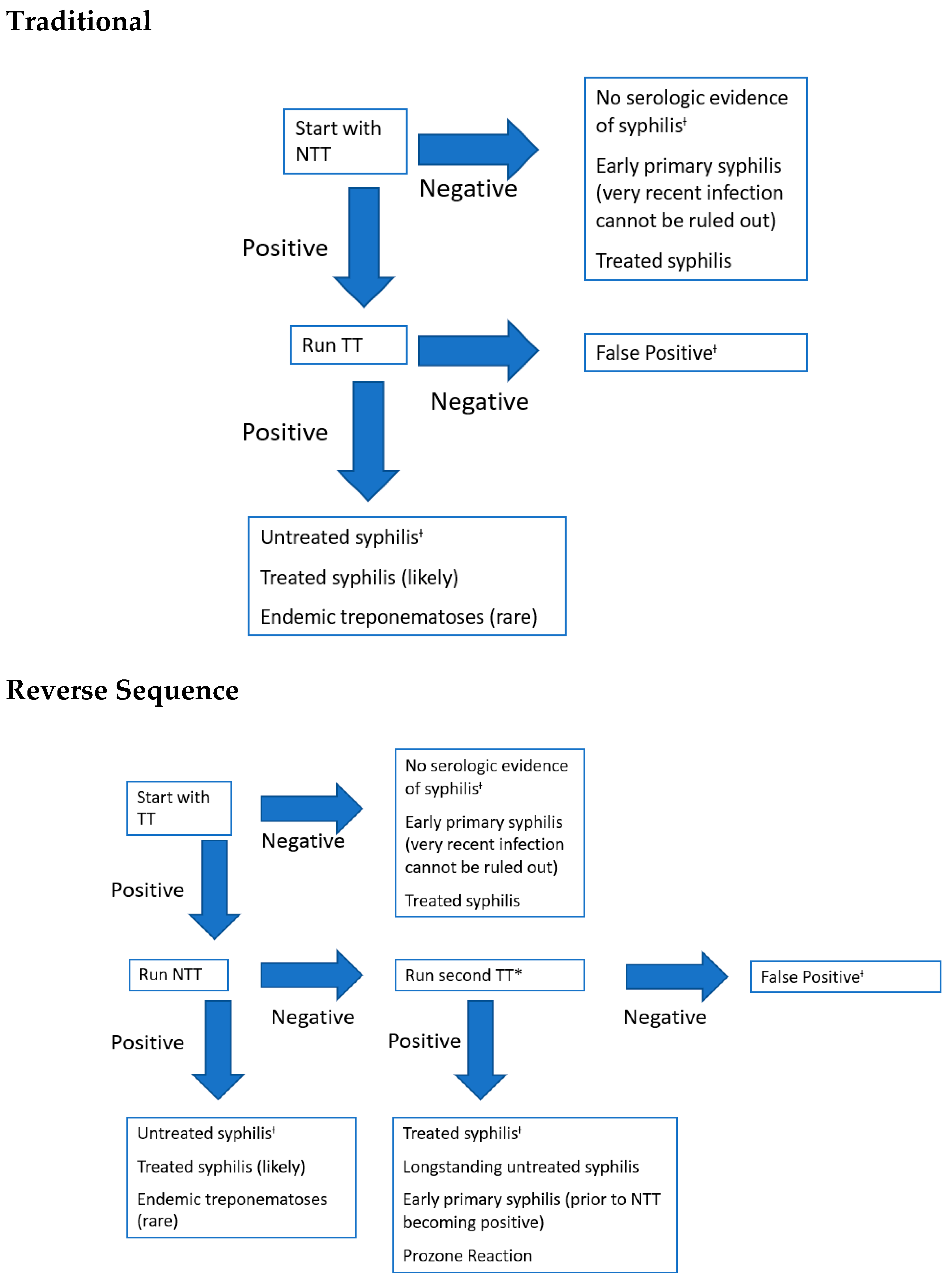
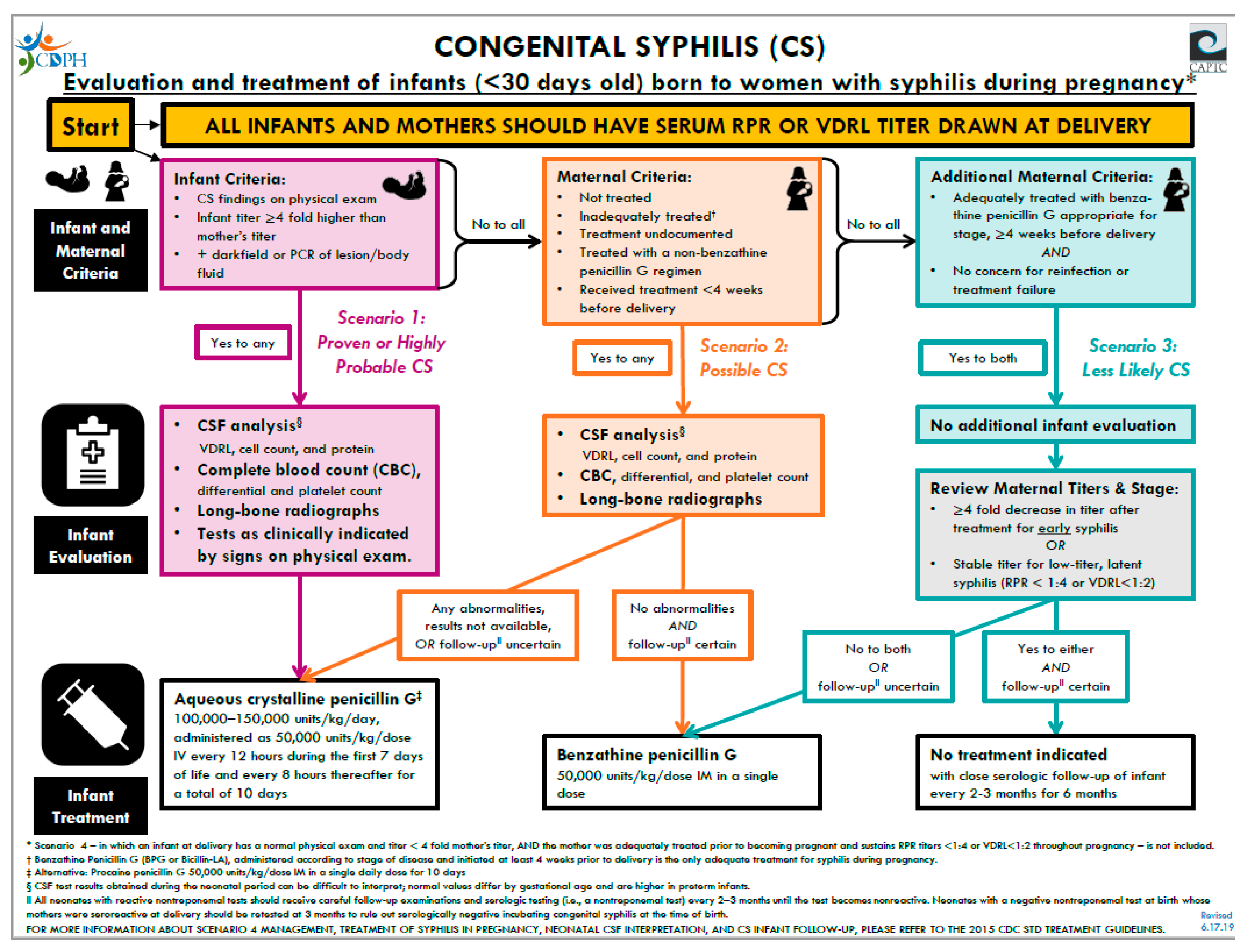
5. Diagnostic Tests and Management
6. Treatment and Follow-Up
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Congenital syphilis--New York City, 1986–1988. MMWR Morb. Mortal. Wkly. Rep. 1989, 38, 825–829.
- Lawn, J.E.; Blencowe, H.; Waiswa, P.; Amouzou, A.; Mathers, C.; Hogan, D.; Flenady, V.; Frøen, J.F.; Qureshi, Z.U.; Calderwood, C.; et al. Stillbirths: Rates, risk factors, and acceleration towards 2030. Lancet 2016, 387, 587–603. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.M.; Sánchez, P.J. Congenital syphilis. Semin. Perinatol. 2018, 42, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Kimball, A.; Miele, K.; Bachmann, L.; Thorpe, P.; Weinstock, H.; Bowen, V. Missed Opportunities for Prevention of Congenital Syphilis. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 661–665. [Google Scholar] [CrossRef]
- Korenromp, E.L.; Rowley, J.; Alonso, M.; Mello, M.B.; Wijesooriya, N.S.; Mahiané, S.G.; Ishikawa, N.; Le, L.-V.; Newman-Owiredu, M.; Nagelkerke, N.; et al. Global burden of maternal and congenital syphilis and associated adverse birth outcomes—Estimates for 2016 and progress since 2012. PLoS ONE 2019, 14, e0211720. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2018; U.S. Department of Health and Human Services: Washington, DC, USA, 2019. [CrossRef]
- Peeling, R.W.; Hook, E.W. The pathogenesis of syphilis: The Great Mimicker, revisited. J. Pathol. 2005, 208, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Šmajs, D.; Strouhal, M.; Knauf, S. Genetics of human and animal uncultivable treponemal pathogens. Infect. Genet. Evol. 2018, 61, 92–107. [Google Scholar] [CrossRef] [PubMed]
- Radolf, J.D.; Kumar, S. The Treponema pallidum Outer Membrane. Curr. Top. Microbiol. Immunol. 2017, 415, 1–38. [Google Scholar] [CrossRef]
- Radolf, J.D.; Deka, R.K.; Anand, A.; Šmajs, D.; Norgard, R.K.D.M.V.; Yang, X.F. Treponema pallidum, the syphilis spirochete: Making a living as a stealth pathogen. Nat. Rev. Genet. 2016, 14, 744–759. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Liu, Y.; Wan, D.; Fang, X.; Li, T.; Guo, Y.; Chang, D.; Su, L.; Wang, Y.; Zhao, J.; et al. Whole-Genome Sequence of Staphylococcus aureus Strain LCT-SA112. J. Bacteriol. 2012, 194, 4124. [Google Scholar] [CrossRef] [Green Version]
- Gust, D.A.; Levine, W.C.; Louis, M.E.S.; Braxton, J.; Berman, S.M. Mortality associated with congenital syphilis in the United States, 1992–1998. Pediatrics 2002, 109, e79. [Google Scholar] [CrossRef] [Green Version]
- Su, J.R.; Brooks, L.C.; Davis, D.W.; Torrone, E.A.; Weinstock, H.S.; Kamb, M.L. Congenital syphilis: Trends in mortality and morbidity in the United States, 1999 through 2013. Am. J. Obstet. Gynecol. 2016, 214, 381.e1–381.e9. [Google Scholar] [CrossRef]
- Dorfman, D.H.; Glaser, J.H. Congenital Syphilis Presenting in Infants after the Newborn Period. N. Engl. J. Med. 1990, 323, 1299–1302. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, P.S.; Cantey, J.B.; Zeray, F.; Leos, N.K.; Sheffield, J.S.; Wendel, G.D.; Sánchez, P.J. Congenital syphilis in neonates with nonreactive nontreponemal test results. J. Perinatol. 2017, 37, 1112–1116. [Google Scholar] [CrossRef]
- Force, U.P.S.T.; Curry, S.J.; Krist, A.H.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; et al. Screening for Syphilis Infection in Pregnant Women. JAMA 2018, 320, 911–917. [Google Scholar] [CrossRef] [Green Version]
- Follett, T.; Clarke, D.F. Resurgence of Congenital Syphilis: Diagnosis and Treatment. Neonatal Netw. 2011, 30, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Long, S.S.; Pickering, L.K.; Prober, C.G. Principles and Practice of Pediatric Infectious Diseases, 2nd Ed. Shock 2003, 20, 98. [Google Scholar] [CrossRef]
- Arrieta, A.C.; Singh, J. Congenital Syphilis. N. Engl. J. Med. 2019, 381, 2157. [Google Scholar] [CrossRef] [PubMed]
- Stephens, J.R.; Arenth, J. Wimberger Sign in Congenital Syphilis. J. Pediatr. 2015, 167, 1451. [Google Scholar] [CrossRef]
- Fiumara, N.; Lessell, S. Manifestations of Late Congenital Syphilis. Arch. Derm. 1970, 102, 78–84. [Google Scholar] [CrossRef]
- De Santis, M.; De Luca, C.; Mappa, I.; Spagnuolo, T.; Licameli, A.; Straface, G.; Scambia, G. Syphilis Infection during Pregnancy: Fetal Risks and Clinical Management. Infect. Dis. Obstet. Gynecol. 2012, 2012, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Khetarpal, S.; Kempf, E.; Mostow, E. Congenital Syphilis: Early- and Late-Stage Findings of Rhagades and Dental Anomalies. Pediatr. Dermatol. 2011, 28, 401–403. [Google Scholar] [CrossRef]
- Chen, M.; Akinboyo, I.C.; Sue, P.K.; Donohue, P.K.; Ghanem, K.G.; Detrick, B.; Witter, F.R.; Page, K.R.; Arav-Boger, R.; Golden, W.C. Evaluating congenital syphilis in a reverse sequence testing environment. J. Perinatol. 2019, 39, 956–963. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Committee on Infectious, D. Red Book: Report of the Committee on Infectious Diseases; American Academy of Pediatrics: Elk Grove Village, IL, USA, 2018. [Google Scholar]
- Seña, A.C.; White, B.L.; Sparling, P.F. Novel Treponema pallidum Serologic Tests: A Paradigm Shift in Syphilis Screening for the 21st Century. Clin. Infect. Dis. 2010, 51, 700–708. [Google Scholar] [CrossRef] [Green Version]
- Discordant results from reverse sequence syphilis screening--five laboratories, United States, 2006–2010. MMWR. Morb. Mortal. Wkly. Rep. 2011, 60, 133–137.
- Ghanem, K.G.; Ram, S.; Rice, P.A. The Modern Epidemic of Syphilis. N. Engl. J. Med. 2020, 382, 845–854. [Google Scholar] [CrossRef]
- Beeram, M.R.; Chopde, N.; Dawood, Y.; Siriboe, S.; Abedin, M. Lumbar puncture in the evaluation of possible asymptomatic congenital syphilis in neonates. J. Pediatr. 1996, 128, 125–129. [Google Scholar] [CrossRef]
- Gomez, G.B.; Kamb, M.L.; Newman, L.M.; Mark, J.; Broutet, N.; Hawkes, S.J. Untreated maternal syphilis and adverse outcomes of pregnancy: A systematic review and meta-analysis. Bull. World Health Organ. 2013, 91, 217–226. [Google Scholar] [CrossRef]
- CDPH. Congenital Syphilis Algorithm. California Department of Public Health. 2019. Available online: https://www.cdph.ca.gov/Programs/CID/DCDC/Pages/CongenitalSyphilis.aspx (accessed on 29 September 2020).
- Matthias, J.M.; Rahman, M.M.; Newman, D.R.; Peterman, T.A. Effectiveness of Prenatal Screening and Treatment to Prevent Congenital Syphilis, Louisiana and Florida, 2013–2014. Sex. Transm. Dis. 2017, 44, 498–502. [Google Scholar] [CrossRef]
- Stafford, I.A.; Sánchez, P.J.; Stoll, B.J. Ending Congenital Syphilis. JAMA 2019, 322, 2073. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Early Congenital Syphilis | Late Congenital Syphilis | ||
|---|---|---|---|
| Prenatal | Dentition | ||
| Nonimmune hydrops | Hutchinson’s teeth | ||
| Intrauterine growth retardation | Mulberry molars | ||
| Stillbirth | Eye | ||
| Hematological/ Reticuloendothelial | Interstitial keratitis | ||
| Hepatosplenomegaly | Ear | ||
| Lymphadenopathy | Eight nerve deafness | ||
| Thrombocytopenia | Nose/Face | ||
| Anemia | Saddle nose | ||
| Leukopenia/Leukocytosis (monocytosis) | Impaired maxillary growth | ||
| Mucocutaneous | Cutaneous | ||
| Rhinitis (sniffles) | Rhagades | ||
| Rash (papulovesicular, prominent in palms and sole; pemphigus syphiliticus) | Skeletal | ||
| Mucous patches | Frontal bossing | ||
| Skeletal | Saber shins | ||
| Long bone lesions (Wimberger sign in tibial protuberance) | Clavicle (sternal end) hypertrophy (Higoumenakis’ sign) | ||
| Periostitis (pseudoparalysis) | Clutton’s joints (knees) | ||
| Neurological | Neurological | ||
| Aseptic meningitis | Aseptic meningitis/asymptomatic neurosyphilis | ||
| Ocular | |||
| Retinitis (rare, also cataracts and keratitis) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galvis, A.E.; Arrieta, A. Congenital Syphilis: A U.S. Perspective. Children 2020, 7, 203. https://doi.org/10.3390/children7110203
Galvis AE, Arrieta A. Congenital Syphilis: A U.S. Perspective. Children. 2020; 7(11):203. https://doi.org/10.3390/children7110203
Chicago/Turabian StyleGalvis, Alvaro E., and Antonio Arrieta. 2020. "Congenital Syphilis: A U.S. Perspective" Children 7, no. 11: 203. https://doi.org/10.3390/children7110203
APA StyleGalvis, A. E., & Arrieta, A. (2020). Congenital Syphilis: A U.S. Perspective. Children, 7(11), 203. https://doi.org/10.3390/children7110203