Predicting Injury Status in Adolescent Dancers Involved in Different Dance Styles: A Prospective Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Design
2.2. Variables
2.2.1. Sociodemographic and Dance Factors
2.2.2. Anthropometric and Body-Built Indices
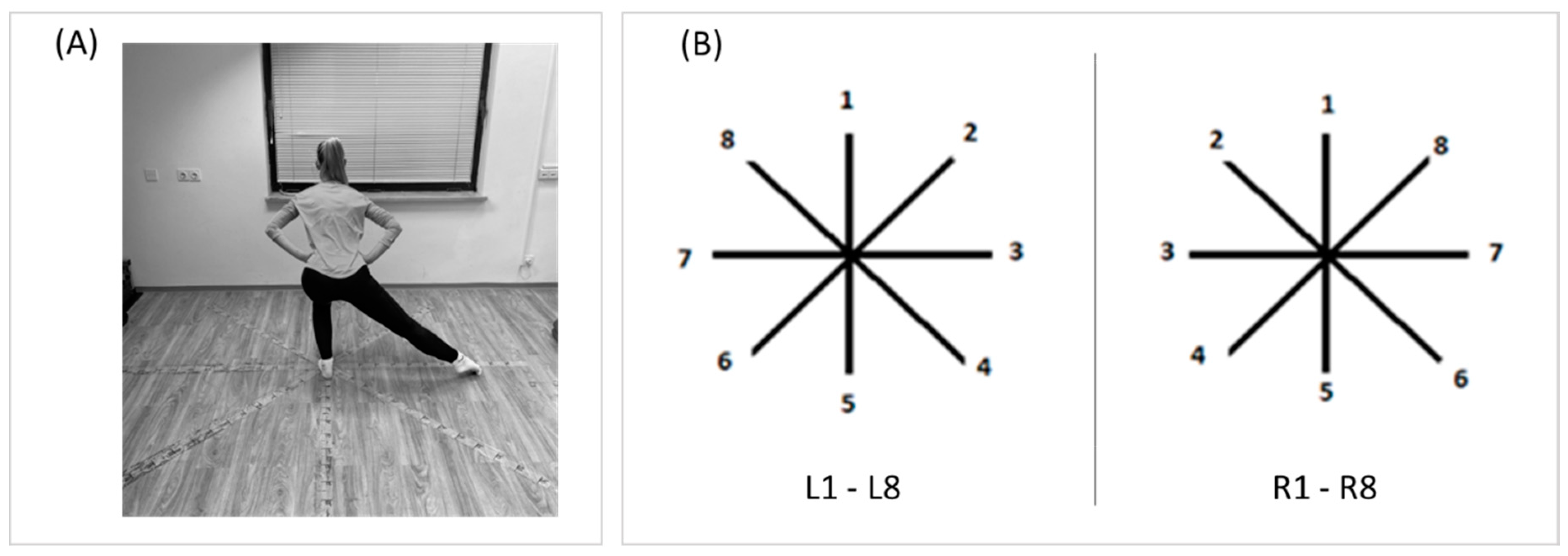
2.2.3. Dynamic Balance
2.2.4. Injury Status
2.3. Data Analysis
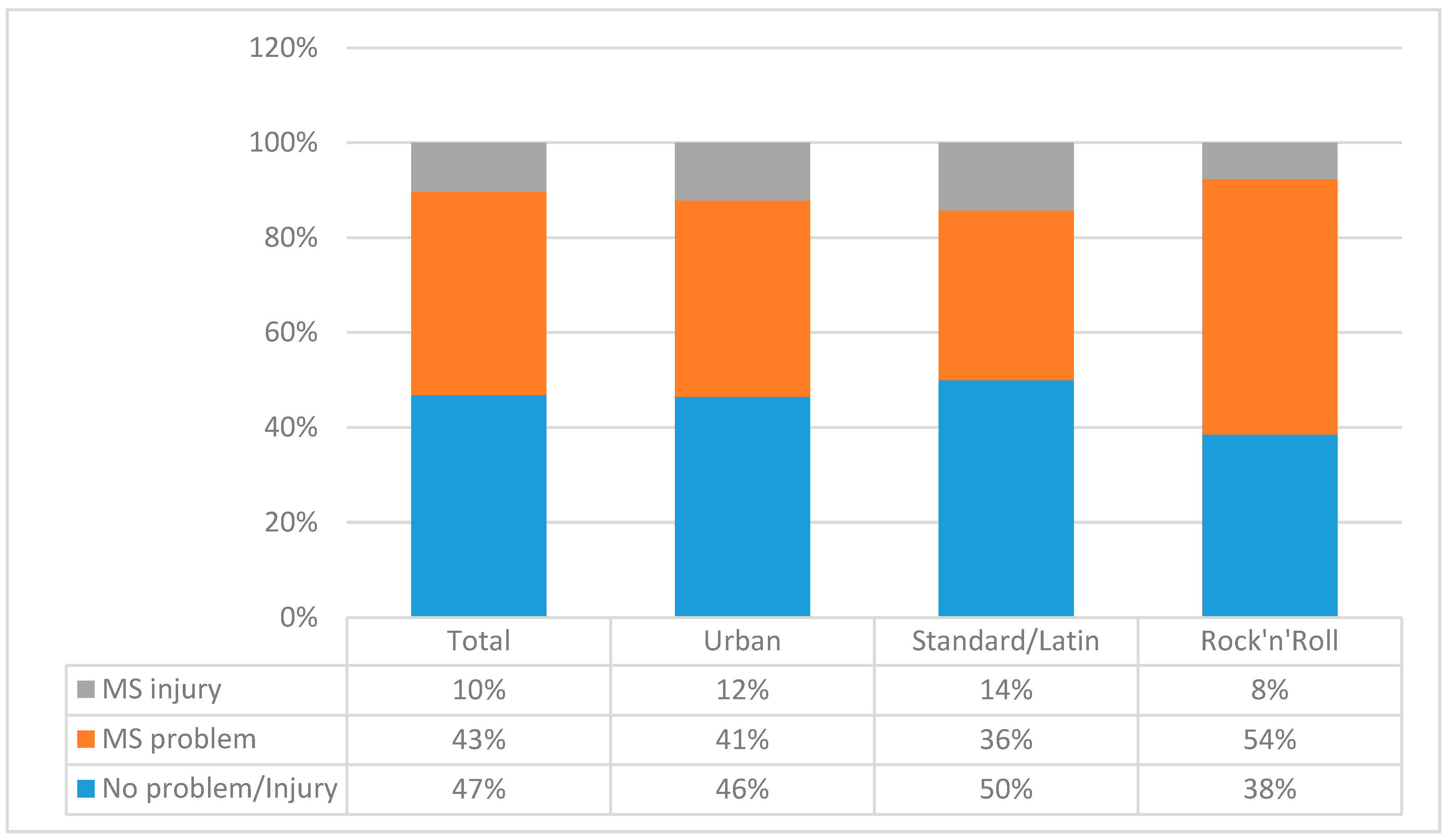
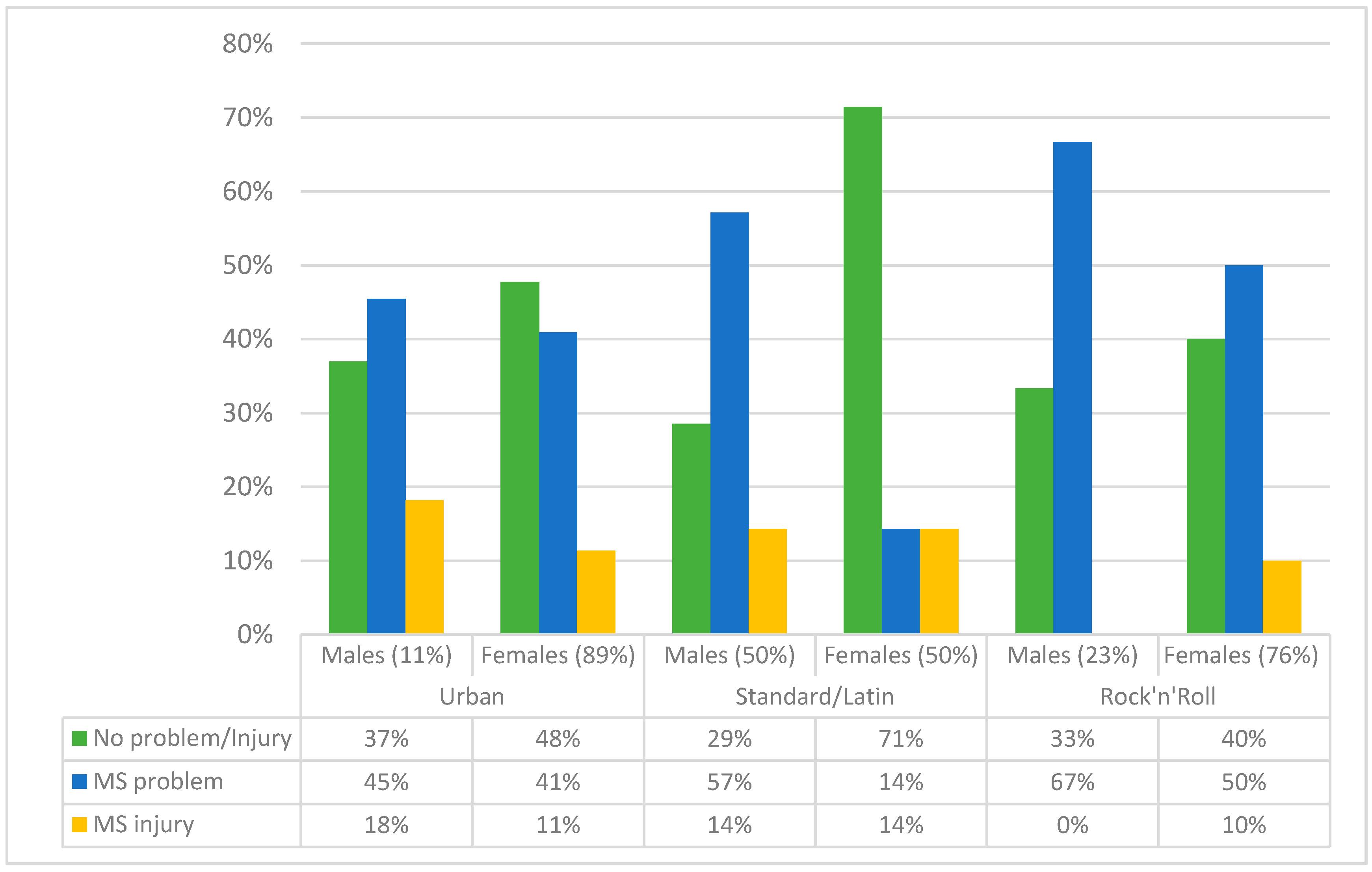
3. Results
4. Discussion
4.1. Gender and Injury Occurrence
4.2. Age and Dance Factors as Predictors of Injury
4.3. Balance and Injury Occurrence
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Xiang, M.; Gu, X.; Zhang, X.; Moss, S.; Huang, C.; Nelson, L.P.; Zhang, T. Psychosocial mechanism of adolescents’ depression: A dose-response relation with physical activity. Children 2020, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Goh, T.L.; Leong, C.H.; Brusseau, T.A.; Hannon, J. Children’s physical activity levels following participation in a classroom-based physical activity curriculum. Children 2019, 6, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granger, E.; Di Nardo, F.; Harrison, A.; Patterson, L.; Holmes, R.; Verma, A. A systematic review of the relationship of physical activity and health status in adolescents. Eur. J. Public Health 2017, 27, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Zhang, T.; Chu, T.L.A.; Gu, X. Effects of a need-supportive motor skill intervention on children’s motor skill competence and physical activity. Children 2020, 7, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moral-Garcia, J.E.; Agraso-Lopez, A.D.; Ramos-Morcillo, A.J.; Jimenez, A.; Jimenez-Eguizabal, A. The influence of physical activity, diet, weight status and substance abuse on students’ self-perceived health. Int. J. Environ. Res. Public Health 2020, 17, 1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Llewellyn, A.; Simmonds, M.; Owen, C.G.; Woolacott, N. Childhood obesity as a predictor of morbidity in adulthood: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 56–67. [Google Scholar] [CrossRef]
- Moral-Garcia, J.E.; Urchaga-Litago, J.D.; Ramos-Morcillo, A.J.; Maneiro, R. Relationship of parental support on healthy habits, school motivations and academic performance in adolescents. Int. J. Environ. Res. Public Health 2020, 17, 882. [Google Scholar] [CrossRef] [Green Version]
- Sember, V.; Morrison, S.A.; Jurak, G.; Kovac, M.; Golobic, M.; Pavletic Samardzija, P.; Gabrijelcic, M.; Primozic, M.; Kotar, T.; Djomba, J.K.; et al. Results from Slovenia’s 2018 report card on physical activity for children and youth. J. Phys. Act. Health 2018, 15, S404–S405. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Lee, J.; Gu, X.; Zhang, X.; Zhang, T. Physical fitness promotion among adolescents: Effects of a jump rope-based physical activity afterschool program. Children 2020, 7, 95. [Google Scholar] [CrossRef]
- Taylor, S.L.; Noonan, R.J.; Knowles, Z.R.; McGrane, B.; Curry, W.B.; Fairclough, S.J. Acceptability and feasibility of single-component primary school physical activity interventions to inform the AS:Sk project. Children 2018, 5, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duberg, A.; Moller, M.; Sunvisson, H. “I feel free”: Experiences of a dance intervention for adolescent girls with internalizing problems. Int. J. Qual. Stud. Health Well Being 2016, 11, 31946. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, A.; Broughton, M.C. Promoting wellbeing and health through active participation in music and dance: A systematic review. Int. J. Qual. Stud. Health Well Being 2020, 15, 1732526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.K.; McGill-Meeks, K.; Beller, J.P.; Burt Solorzano, C.M. Go girls!-Dance-based fitness to increase enjoyment of exercise in girls at risk for PCOS. Children 2019, 6, 99. [Google Scholar] [CrossRef] [Green Version]
- Vassallo, A.J.; Hiller, C.; Stamatakis, E.; Pappas, E. Epidemiology of dance-related injuries presenting to emergency departments in the United States, 2000–2013. Med. Probl. Perform. Art. 2017, 32, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Ursej, E.; Zaletel, P. Injury occurrence in modern and hip-hop dancers: A systematic literature review. Zdr. Varst. 2020, 59, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Ursej, E.; Sekulic, D.; Prus, D.; Gabrilo, G.; Zaletel, P. Investigating the prevalence and predictors of injury occurrence in competitive hip hop dancers: Prospective analysis. Int. J. Environ. Res. Public Health 2019, 16, 3214. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, C.L.; Hincapie, C.A.; Cassidy, J.D. Musculoskeletal injuries and pain in dancers: A systematic review update. J. Danc. Med. Sci. 2012, 16, 74–84. [Google Scholar]
- Hincapie, C.A.; Morton, E.J.; Cassidy, J.D. Musculoskeletal injuries and pain in dancers: A systematic review. Arch. Phys. Med. Rehabil. 2008, 89, 1819–1829. [Google Scholar] [CrossRef]
- Kenny, S.J.; Palacios-Derflingher, L.; Shi, Q.; Whittaker, J.L.; Emery, C.A. Association between previous injury and risk factors for future injury in preprofessional ballet and contemporary dancers. Clin. J. Sport Med. 2019, 29, 209–217. [Google Scholar] [CrossRef]
- van Winden, D.; Van Rijn, R.M.; Richardson, A.; Savelsbergh, G.J.P.; Oudejans, R.R.D.; Stubbe, J.H. Detailed injury epidemiology in contemporary dance: A 1-year prospective study of 134 students. BMJ Open Sport Exerc. Med. 2019, 5, e000453. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Reid, D.; Cadwell, J.; Palmer, P. Injury incidence, dance exposure and the use of the movement competency screen (Mcs) to identify variables associated with injury in full-time pre-professional dancers. Int. J. Sports Phys. Ther. 2017, 12, 352–370. [Google Scholar] [PubMed]
- Ojofeitimi, S.; Bronner, S.; Woo, H. Injury incidence in hip hop dance. Scand. J. Med. Sci. Sports 2012, 22, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Luke, A.C.; Kinney, S.A.; D. Hemecourt, P.A.; Baum, J.; Owen, M.; Micheli, L.J. Determinants of injuries in young dancers. Med. Probl. Perform. Artist. 2002, 17, 105–112. [Google Scholar]
- Zaletel, P.; Sekulic, D.; Zenic, N.; Esco, M.R.; Sajber, D.; Kondric, M. The association between body-built and injury occurrence in pre-professional ballet dancers—Separated analysis for the injured body-locations. Int. J. Occup. Med. Environ. Health 2017, 30, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Jubb, C.; Bell, L.; Cimelli, S.; Wolman, R. Injury patterns in hip hop dancers. J. Dance Med. Sci. 2019, 23, 145–149. [Google Scholar] [CrossRef]
- Premelč, J.; Vučković, G.; James, N.; Dimitriou, L. A Retrospective investigation on age and gender differences of injuries in dance sport. Int. J. Environ. Res. Public Health 2019, 16, 4164. [Google Scholar] [CrossRef] [Green Version]
- Hrysomallis, C. Relationship between balance ability, training and sports injury risk. Sports Med. 2007, 37, 547–556. [Google Scholar] [CrossRef]
- Steinberg, N.; Siev-Ner, I.; Peleg, S.; Dar, G.; Masharawi, Y.; Zeev, A.; Hershkovitz, I. Injury patterns in young, non-professional dancers. J. Sports Sci. 2011, 29, 47–54. [Google Scholar] [CrossRef]
- Aandstad, A.; Holtberget, K.; Hageberg, R.; Holme, I.; Anderssen, S.A. Validity and reliability of bioelectrical impedance analysis and skinfold thickness in predicting body fat in military personnel. Mil. Med. 2014, 179, 208–217. [Google Scholar] [CrossRef] [Green Version]
- McLester, C.N.; Nickerson, B.S.; Kliszczewicz, B.M.; McLester, J.R. Reliability and agreement of various inbody body composition analyzers as compared to dual-energy X-ray absorptiometry in healthy men and women. J. Clin. Densitom. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Ambegaonkar, J.P.; Cortes, N.; Caswell, S.V.; Ambegaonkar, G.P.; Wyon, M. Lower extremity hypermobility, but not core muscle endurance influences balance in female collegiate dancers. Int. J. Sports Phys. Ther. 2016, 11, 220–229. [Google Scholar]
- Gribble, P.A.; Hertel, J.; Plisky, P. Using the star excursion balance test to assess dynamic postural-control deficits and outcomes in lower extremity injury: A literature and systematic review. J. Athl. Train. 2012, 47, 339–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powden, C.J.; Dodds, T.K.; Gabriel, E.H. The reliability of the star excursion balance test and lower quarter Y-balance test in healthy adults: A systematic review. Int. J. Sports Phys. Ther. 2019, 14, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Clarsen, B.; Ronsen, O.; Myklebust, G.; Florenes, T.W.; Bahr, R. The Oslo sports trauma research center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. Br. J. Sports Med. 2014, 48, 754–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Rezende, A.; Sampaio II, L.H.F.; Bittar, A.J.; da Silva Hamu, T.C.D.; Wyon, M.A.; Formiga, C. The relationship between vitamin D levels, injury and muscle function in adolescent dancers. Int. J. Sports Med. 2020, 41, 360–364. [Google Scholar] [CrossRef]
- Bronner, S.; McBride, C.; Gill, A. Musculoskeletal injuries in professional modern dancers: A prospective cohort study of 15 years. J. Sports Sci. 2018, 36, 1880–1888. [Google Scholar] [CrossRef]
- Campoy, F.A.; Coelho, L.R.; Bastos, F.N.; Netto Júnior, J.; Vanderlei, L.C.; Monteiro, H.L.; Padovani, C.R.; Pastre, C.M. Investigation of risk factors and characteristics of dance injuries. Clin. J. Sport Med. 2011, 21, 493–498. [Google Scholar] [CrossRef]
- Post, E.G.; Trigsted, S.M.; Riekena, J.W.; Hetzel, S.; McGuine, T.A.; Brooks, M.A.; Bell, D.R. The association of sport specialization and training volume with injury history in youth athletes. Am. J. Sports Med. 2017, 45, 1405–1412. [Google Scholar] [CrossRef]
- Jacobs, C.L.; Cassidy, J.D.; Côté, P.; Boyle, E.; Ramel, E.; Ammendolia, C.; Hartvigsen, J.; Schwartz, I. Musculoskeletal injury in professional dancers: Prevalence and associated factors: An international cross-sectional study. Clin. J. Sport Med. 2017, 27, 153–160. [Google Scholar] [CrossRef]
- Cho, C.H.; Song, K.S.; Min, B.W.; Lee, S.M.; Chang, H.W.; Eum, D.S. Musculoskeletal injuries in break-dancers. Injury 2009, 40, 1207–1211. [Google Scholar] [CrossRef] [PubMed]
- Kauther, M.D.; Wedemeyer, C.; Wegner, A.; Kauther, K.M.; von Knoch, M. Breakdance injuries and overuse syndromes in amateurs and professionals. Am. J. Sports Med. 2009, 37, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Simmel, L. Dance Medicine in Practice: Anatomy, Injury Prevention, Training; Taylor and Francis: London, UK, 2013. [Google Scholar]
- Han, J.; Anson, J.; Waddington, G.; Adams, R.; Liu, Y. The Role of ankle proprioception for balance control in relation to sports performance and injury. Biomed. Res. Int 2015, 2015, 842804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, W.C.; Wang, D.; Chen, J.B.; Vail, J.; Rugg, C.M.; Hame, S.L. Lower quarter Y-balance test scores and lower extremity injury in NCAA division I athletes. Orthop. J. Sports Med. 2017, 5, 2325967117723666. [Google Scholar] [CrossRef] [Green Version]
- Plisky, P.J.; Rauh, M.J.; Kaminski, T.W.; Underwood, F.B. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. J. Orthop. Sports Phys. Ther. 2006, 36, 911–919. [Google Scholar] [CrossRef]
- Smith, C.A.; Chimera, N.J.; Warren, M. Association of y balance test reach asymmetry and injury in division I athletes. Med. Sci. Sports Exerc. 2015, 47, 136–141. [Google Scholar] [CrossRef]
- Brachman, A.; Kamieniarz, A.; Michalska, J.; Pawlowski, M.; Slomka, K.J.; Juras, G. Balance training programs in athletes—A systematic review. J. Hum. Kinet. 2017, 58, 45–64. [Google Scholar] [CrossRef] [Green Version]
- Valovich McLeod, T.C. The effectiveness of balance training programs on reducing the incidence of ankle sprains in adolescent athletes. J. Sport Rehabil. 2008, 17, 316–323. [Google Scholar] [CrossRef] [Green Version]
- Muehlbauer, T.; Wagner, V.; Brueckner, D.; Schedler, S.; Schwiertz, G.; Kiss, R.; Hagen, M. Effects of a blocked versus an alternated sequence of balance and plyometric training on physical performance in youth soccer players. BMC Sports Sci. Med. Rehabil. 2019, 11, 18. [Google Scholar] [CrossRef] [Green Version]
- Gebel, A.; Lesinski, M.; Behm, D.G.; Granacher, U. Effects and dose-response relationship of balance training on balance performance in youth: A systematic review and meta-analysis. Sports Med. 2018, 48, 2067–2089. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Urban Dances | Standard/Latin Dances | Rock and Roll | ANOVA | Welch’s p | ||
|---|---|---|---|---|---|---|
| (n = 99) | (n = 14) | (n = 13) | F Test | p | ||
| Age (years) | 15.8 ± 1.4 | 15.25 ± 1.96 | 15.57 ± 1.66 | 1.42 | 0.241 | 0.031 |
| Started with dance (years) | 7.77 ± 2.8 | 9.3 ± 2.7 | 7.52 ± 3.25 | 3.08 | 0.052 | 0.294 |
| Involvement in dance (years) | 8.11 ± 2.65 | 6 ± 2.65 | 8.29 ± 2.72 | 6.47 | 0.001 | 0.001 |
| Trainings per week (f) | 3.42 ± 0.87 | 5.57 ± 1.53 | 5.1 ± 0.89 | 63.09 | 0.001 | 0.001 |
| Hours of training per week (h) | 5.41 ± 1.77 | 17.91 ± 6.13 | 11.14 ± 2.39 | 205.47 | 0.001 | 0.001 |
| Body height (cm) | 165.85 ± 6.33 | 167.23 ± 9.97 | 166.91 ± 10.93 | 0.44 | 0.651 | 0.832 |
| Body mass (kg) | 58.92 ± 7.01 | 55 ± 11.38 | 58.68 ± 13.33 | 2.01 | 0.143 | 0.082 |
| Body fat (%) | 21.89 ± 6.51 | 12.09 ± 5.26 | 15.51 ± 5.63 | 29.52 | 0.001 | 0.001 |
| Lean body mass (%) | 25.34 ± 3.39 | 26.91 ± 6.65 | 27.54 ± 6.95 | 2.97 | 0.052 | 0.567 |
| Body mass index (kg/m2) | 21.43 ± 2.44 | 19.45 ± 2.1 | 20.83 ± 2.58 | 6.71 | 0.001 | 0.001 |
| R1 (SEBT result/leg length) | 83.86 ± 9.61 | 85.35 ± 5.88 | 83.29 ± 6.6 | 0.32 | 0.721 | 0.022 |
| R2 (SEBT result/leg length) | 89.25 ± 12.36 | 95.8 ± 12.79 | 92.21 ± 6.38 | 3.00 | 0.052 | 0.031 |
| R3 (SEBT result/leg length) | 100.23 ± 14.08 | 124.77 ± 23.14 | 111.32 ± 12.83 | 24.83 | 0.001 | 0.001 |
| R4 (SEBT result/leg length) | 105.72 ± 16.31 | 128.73 ± 20.3 | 130.17 ± 14.08 | 31.70 | 0.001 | 0.001 |
| R5 (SEBT result/leg length) | 106.1 ± 16.82 | 132.11 ± 19.63 | 134.72 ± 20.57 | 37.03 | 0.001 | 0.001 |
| R6 (SEBT result/leg length) | 100.07 ± 16.68 | 125.27 ± 22.6 | 127.35 ± 23.22 | 31.42 | 0.001 | 0.001 |
| R7 (SEBT result/leg length) | 89.04 ± 15.75 | 114.04 ± 22.76 | 106.71 ± 16.45 | 25.78 | 0.001 | 0.001 |
| R8 (SEBT result/leg length) | 74.84 ± 10.02 | 75.6 ± 11.36 | 75.23 ± 5.37 | 0.06 | 0.94 | 0.323 |
| L1 (SEBT result/leg length) | 83.52 ± 9.96 | 81.72 ± 5.42 | 81.25 ± 7.67 | 0.75 | 0.471 | 0.541 |
| L2 (SEBT result/leg length) | 89.82 ± 10.04 | 90.99 ± 8.3 | 90.85 ± 7.55 | 0.20 | 0.823 | 0.289 |
| L3 (SEBT result/leg length) | 99.2 ± 14.65 | 116.9 ± 20.78 | 116.79 ± 13.3 | 19.97 | 0.001 | 0.001 |
| L4 (SEBT result/leg length) | 107.38 ± 16.26 | 129.77 ± 20.22 | 130.52 ± 14.23 | 28.69 | 0.001 | 0.001 |
| L5 (SEBT result/leg length) | 106.71 ± 17.92 | 132.19 ± 21.65 | 135.68 ± 17.47 | 33.52 | 0.001 | 0.001 |
| L6 (SEBT result/leg length) | 100.57 ± 17.57 | 127.77 ± 23.2 | 125.65 ± 19.59 | 30.13 | 0.001 | 0.001 |
| L7 (SEBT result/leg length) | 90.12 ± 14.92 | 110.84 ± 23.65 | 107.39 ± 17.89 | 20.16 | 0.001 | 0.001 |
| L8 (SEBT result/leg length) | 74.48 ± 11.99 | 77.95 ± 10.23 | 77.13 ± 13.53 | 1.02 | 0.364 | 0.046 |
| Model 0 (Nonadjusted) | Model 1 (Adjusted for Dance Style, Age, and Gender) | |||
|---|---|---|---|---|
| MS Problem | MS Injury | MS Problem | MS Injury | |
| Male gender | 1.57 (0.58–4.21) | 1.05 (0.39–2.76) | ||
| Age (years) | 1.09 (0.89–1.33) | 1.51 (1.11–2.04) | ||
| Involvement in dance (years) | 1.05 (0.91–1.20) | 1.31 (1.04–1.66) | 1.01 (0.88–1.23) | 1.11 (0.91–1.51) |
| Training per week (hours) | 1.05 (0.93–1.25) | 1.00 (0.87–1.17) | 1.03 (0.91–1.27) | 1.01 (0.85–1.20) |
| Body height (cm) | 1.00 (0.97–1.05) | 0.99 (0.94–1.05) | 1.00 (0.96–1.07) | 1.00 (0.93–1.06) |
| Body mass (kg) | 1.02 (0.98–1.06) | 1.02 (0.97–1.07) | 1.01 (0.96–1.08) | 1.01 (0.96–1.08) |
| Body fat (%) | 1.00 (0.97–1.06) | 1.05 (0.97–1.15) | 1.01 (0.98–1.08) | 1.06 (0.98–1.17) |
| Lean body mass (kg) | 1.01 (0.95–1.08) | 0.99 (0.92–1.08) | 1.02 (0.94–1.09) | 0.99 (0.91–1.10) |
| Body mass index (kg/m2) | 0.97 (0.83–1.14) | 0.98 (0.81–1.21) | 0.95 (0.81–1.15) | 0.95 (0.80–1.23) |
| R1 (SEBT result/leg length) | 0.97 (0.92–1.03) | 0.93 (0.86–1.00) | 0.98 (0.90–1.05) | 0.93 (0.86–1.00) |
| R2 (SEBT result/leg length) | 0.99 (0.95–1.03) | 0.94 (0.89–1.01) | 1.00 (0.92–1.05) | 0.96 (0.87–1.04) |
| R3 (SEBT result/leg length) | 0.99 (0.97–1.01) | 0.95 (0.91–0.99) | 0.98 (0.94–1.01) | 0.96 (0.92–0.99) |
| R4 (SEBT result/leg length) | 0.98 (0.96–0.99) | 0.97 (0.95–0.99) | 0.99 (0.94–1.03) | 0.98 (0.92–1.03) |
| R5 (SEBT result/leg length) | 0.98 (0.96–0.99) | 0.97 (0.95–0.99) | 0.99 (0.94–1.02) | 0.98 (0.93–1.03) |
| R6 (SEBT result/leg length) | 0.98 (0.97–0.99) | 0.98 (0.96–1.01) | 0.99 (0.95–1.04) | 0.98 (0.94–1.02) |
| R7 (SEBT result/leg length) | 0.98 (0.96–0.99) | 0.99 (0.96–1.01) | 0.97 (0.94–1.01) | 0.98 (0.95–1.02) |
| R8 (SEBT result/leg length) | 0.96 (0.93–1.01) | 1.01 (0.96–1.06) | 0.98 (0.92–1.04) | 1.00 (0.95–1.06) |
| L1 (SEBT result/leg length) | 0.98 (0.93–1.02) | 0.98 (0.93–1.03) | 0.99 (0.94–1.05) | 1.00 (0.94–1.04) |
| L2 (SEBT result/leg length) | 0.99 (0.95–1.03) | 0.99 (0.94–1.04) | 0.99 (0.95–1.04) | 0.99 (0.94–1.05) |
| L3 (SEBT result/leg length) | 0.98 (0.96–0.99) | 0.98 (0.96–1.01) | 0.98 (0.95–0.99) | 0.98 (0.95–1.02) |
| L4 (SEBT result/leg length) | 0.98 (0.97–1.01) | 0.98 (0.96–1.01) | 0.99 (0.97–1.02) | 1.00 (0.97–1.03) |
| L5 (SEBT result/leg length) | 0.98 (0.97–0.99) | 0.98 (0.95–0.99) | 0.99 (0.97–1.02) | 1.00 (0.95–1.05) |
| L6 (SEBT result/leg length) | 0.98 (0.96–0.99) | 0.97 (0.95–0.99) | 0.98 (0.96–0.99) | 0.97 (0.95–0.99) |
| L7 (SEBT result/leg length) | 0.97 (0.95–0.99) | 0.98 (0.95–1.01) | 0.98 (0.95–1.01) | 0.99 (0.95–1.03) |
| L8 (SEBT result/leg length) | 0.96 (0.92–0.99) | 0.97 (0.93–1.01) | 0.97 (0.93–0.99) | 0.98 (0.92–1.03) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sekulic, D.; Prus, D.; Zevrnja, A.; Peric, M.; Zaletel, P. Predicting Injury Status in Adolescent Dancers Involved in Different Dance Styles: A Prospective Study. Children 2020, 7, 297. https://doi.org/10.3390/children7120297
Sekulic D, Prus D, Zevrnja A, Peric M, Zaletel P. Predicting Injury Status in Adolescent Dancers Involved in Different Dance Styles: A Prospective Study. Children. 2020; 7(12):297. https://doi.org/10.3390/children7120297
Chicago/Turabian StyleSekulic, Damir, Dasa Prus, Ante Zevrnja, Mia Peric, and Petra Zaletel. 2020. "Predicting Injury Status in Adolescent Dancers Involved in Different Dance Styles: A Prospective Study" Children 7, no. 12: 297. https://doi.org/10.3390/children7120297
APA StyleSekulic, D., Prus, D., Zevrnja, A., Peric, M., & Zaletel, P. (2020). Predicting Injury Status in Adolescent Dancers Involved in Different Dance Styles: A Prospective Study. Children, 7(12), 297. https://doi.org/10.3390/children7120297