Temperamental Development among Preterm Born Children. An RCT Follow-Up Study


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Intervention Program
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Child Temperament Reported by Mothers
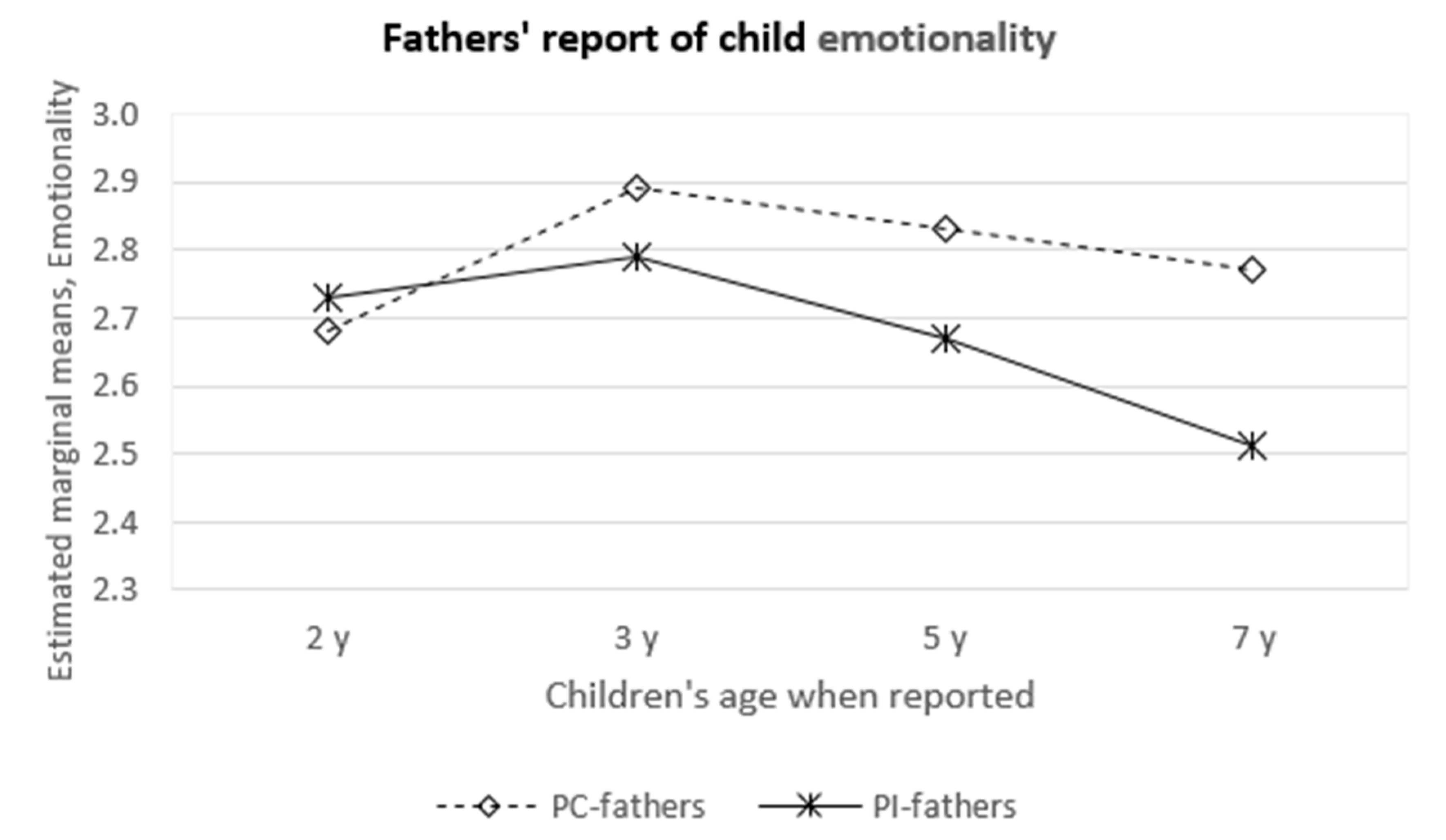
3.2. Child Temperament Reported by Fathers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations:
| CCTI | Colorado Childhood Temperament Inventory |
| EAS | Emotionality, Activity, and Sociability Questionnaire |
| MITP-m | Mother−Infant Transaction Program, modified version |
| NICU | neonatal intensive care unit |
| PC group | preterm control group |
| PI group | preterm intervention group |
References
- Aylward, G.P. Neurodevelopmental outcomes of infants born prematurely. J. Dev. Behav. Pediatr. 2005, 26, 427–441. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, A.; Cleves, M.; Casey, P.H.; Cradock, M.M.; Anand, K. Cognitive and behavioral outcomes of school-aged children who were born preterm. JAMA 2002, 288, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Anzman-Frasca, S.; Stifter, C.A.; Paul, I.M.; Birch, L.L. Negative temperament as a moderator of intervention effects in infancy: Testing a differential susceptibility model. Prev. Sci. 2014, 15, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Cassiano, R.G.M.; Gaspardo, C.M.; Linhares, M.B.M. Temperament moderated by neonatal factors predicted behavioral problems in childhood: A prospective longitudinal study. Early Hum. Dev. 2019, 135, 37–43. [Google Scholar] [CrossRef]
- Eisenberg, N. Temperamental effortful control (self-regulation). In Encyclopedia on Early Childhood Development; Tremblay, R.E., Barr, R.G., Peters, R.D.V., Eds.; Centre of Excellence for Early Childhood Development: Montreal, QB, Canada, 2005. [Google Scholar]
- Bohlin, G.; Hagekull, B. Socio-emotional development: From infancy to young adulthood. Scand. J. Psychol. 2009, 50, 592–601. [Google Scholar] [CrossRef]
- Cassiano, R.G.M.; Gaspardo, C.M.; Fiurini, G.C.B.; Martinez, F.E.; Linhares, M.B.M. Impact of neonatal risk and temperament on behavioral problems in toddlers born preterm. Early Hum. Dev. 2016, 103, 175–181. [Google Scholar] [CrossRef]
- Lee, Y.K.; Lee, J. Characteristics of temperament of preterm toddlers and their relation to early language and communication development. Commun. Sci. Dis. 2017, 22, 458–470. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Pereira, M.; Fernández, P.; Resches, M.; Gómez-Taibo, M.L. Does temperament influence language development? Evidence from preterm and full-term children. Infant Behav. Dev. 2016, 42, 11–21. [Google Scholar] [CrossRef]
- Gray, P.H.; Edwards, D.M.; O’Callaghan, M.J.; Cuskelly, M.; Gibbons, K. Parenting stress in mothers of very preterm infants - Influence of development, temperament and maternal depression. Early Hum. Dev. 2013, 89, 625–629. [Google Scholar] [CrossRef]
- Gueron-Sela, N.; Atzaba-Poria, N.; Meiri, G.; Marks, K. Temperamental susceptibility to parenting among preterm and full-term infants in early cognitive development. Infancy 2016, 21, 312–331. [Google Scholar] [CrossRef]
- Langerock, N.; van Hanswijck de Jonge, L.; Graz, M.B.; Hüppi, P.S.; Tolsa, C.B.; Barisnikov, K. Emotional reactivity at 12 months in very preterm infants born at <29 weeks of gestation. Infant Behav. Dev. 2013, 36, 289–297. [Google Scholar] [PubMed]
- Witt, A.; Theurel, A.; Tolsa, C.B.; Lejeune, F.; Fernandes, L.; de Jonge, L.H.; Monnier, M.; Bickle Graz, M.; Barisnikov, K.; Gentaz, E.; et al. Emotional and effortful control abilities in 42-month-old very preterm and full-term children. Early Hum. Dev. 2014, 90, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Belsky, J.; Bakermans-Kranenburg, M.J.; van Izendoorn, M.H. For better and for worse. Different susceptibility to environmental influences. Curr. Dir. Psychol. Sci. 2007, 16, 300–304. [Google Scholar] [CrossRef] [Green Version]
- Rothbart, M.K. Becoming Who We Are: Temperament and Personality in Development; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Fox, N.A. Temperament and regulation of emotion in the first years of life. Pediatrics 1998, 102, 1230–1235. [Google Scholar]
- Else-Quest, N.M.; Hyde, J.S.; Goldsmith, H.H.; Van Hulle, C.A. Gender differences in temperament: A meta-analysis. Psychol. Bull. 2006, 132, 33–72. [Google Scholar] [CrossRef] [Green Version]
- Klein, V.C.; Rocha, L.C.; Martinez, F.E.; Putnam, S.P.; Linhares, M.B.M. Temperament and behavior problems in toddlers born preterm and very low birth weight. Span. J. Psychol. 2013, 16, e18. [Google Scholar] [CrossRef]
- Caravale, B.; Sette, S.; Cannoni, E.; Marano, A.; Riolo, E.; Devescovi, A.; De Curtis, M.; Bruni, O. Sleep characteristics and temperament in preterm children at two years of age. J. Clin. Sleep Med. 2017, 13, 1081–1088. [Google Scholar] [CrossRef]
- Montirosso, R.; Provenzi, L.; Fumagalli, M.; Sirgiovanni, I.; Giorda, R.; Pozzoli, U.; Beri, S.; Menozzi, G.; Tronick, E.; Morandi, F.; et al. Serotonin transporter gene (SLC6A4) methylation associates with neonatal intensive care unit stay and 3- month-old temperament in preterm infants. Child Dev. 2016, 87, 38–48. [Google Scholar] [CrossRef]
- Dalimonte-Merckling, D.M.; Brophy-Herb, H.E. A person-centered approach to child temperament and parenting. Child Dev. 2018, 90, 1702–1717. [Google Scholar] [CrossRef]
- Poehlmann, J.; Schwichtenberg, A.J.M.; Shlafer, R.J.; Hahn, E.; Bianchi, J.P.; Warner, R. Emerging self-regulation in toddlers born preterm or low birth weight: Differential susceptibility to parenting? Dev. Psychopathol. 2011, 23, 177–193. [Google Scholar] [CrossRef] [Green Version]
- Blair, C. Early intervention for low birth weight, preterm infants: The role of negative emotionality in the specification of effects. Dev. Psychopathol. 2002, 14, 311–332. [Google Scholar] [CrossRef] [PubMed]
- Gatta, M.; Miscioscia, M.; Svanellini, L.; Brianda, M.E.; Guerra, G.; Battistella, P.A.; Simonelli, A. Triadic interactions in families with preterm children: A comparative study with children born at term. Neuropsychiatr. Dis. Treat. 2017, 13, 2375–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newnham, C.A.; Milgrom, J.; Skouteris, H. Effectiveness of a modified mother-infant transaction program on outcomes for preterm infants from 3 to 24 months of age. Infant Behav. Dev. 2009, 32, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.H.; Hahn, C.S.; Putnick, D.L.; Pearson, R. Stability of child temperament: Multiple moderation by child and mother characteristics. Br. J. Dev. Psychol. 2019, 37, 51–67. [Google Scholar] [CrossRef] [Green Version]
- Guerin, D.W.; Gottfried, A.W. Developmental stability and change in parent reports of temperament: A ten-year longitudinal investigation from infancy through preadolescence. Merrill-Palmer Quart. 1994, 40, 334–355. [Google Scholar]
- Sameroff, A. (Ed.) The Transactional Model of Development, How Children and Contexts Shape Each Other; American Psychological Association: Washington, DC, USA, 2009. [Google Scholar]
- Laucht, M.; Esser, G.; Schmidt, M.H. Differential development of infants at risk for psychopathology: The moderating role of early maternal responsivity. Dev. Med. Child Neurol. 2001, 43, 292–300. [Google Scholar] [CrossRef]
- Ahn, S.; Youngblut, J.M. Predictors of women’s postpartum health status in the first 3 months after childbirth. Asian Nurs. Res. 2007, 1, 136–146. [Google Scholar] [CrossRef] [Green Version]
- Maghaireh, D.F.; Abdullah, K.L.; Chan, C.M.; Piaw, C.Y.; Kawafha, M.M.A. Systematic review of qualitative studies exploring parental experiences in the Neonatal Intensive Care Unit. J. Clin. Nurs. 2016, 25, 2745–2756. [Google Scholar] [CrossRef]
- Tan, J.B.C.; Boskovic, D.S.; Angeles, D.M. The energy costs of prematurity and the Neonatal Intensive Care Unit (NICU) experience. Antioxidants 2018, 7, 37. [Google Scholar] [CrossRef] [Green Version]
- Als, H.; Butler, S.; Kosta, S.; McAnulty, G. The assessment of preterm infants’ behavior (ABIP): Furthering the understanding and measurement of neurodevelopmental competence in preterm and full-term infants. Ment. Retard. Dev. Disabil. Res. Rev. 2005, 11, 94–102. [Google Scholar] [CrossRef]
- Sansavini, A.; Zavagli, V.; Guarini, A.; Savini, S.; Alessandroni, R.; Faldella, G. Dyadic co-regulation, affective intensity and infant’s development at 12 months: A comparison among extremely preterm and full-term dyads. Infant Behav. Dev. 2015, 40, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Landsem, I.P.; Handegard, B.H.; Tunby, J.; Ulvund, S.E.; Ronning, J.A. Early intervention program reduces stress in parents of preterms during childhood, a randomized controlled trial. Trials 2014, 15, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abidin, R.R. Parenting Stress Index, Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1995. [Google Scholar]
- Gerstein, E.D.; Poehlmann-Tynan, J. Transactional processes in children born preterm: Influences of mother-child interactions and parenting stress. J. Fam. Psychol. 2015, 29, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Bilgin, A.; Wolke, D. Maternal sensitivity in parenting preterm children: A meta- analysis. Pediatrics 2015, 136, e177–e193. [Google Scholar] [CrossRef] [Green Version]
- Case-Smith, J.; Butcher, L.; Reed, D. Parents’ report of sensory responsiveness and temperament in preterm infants. Am. J. Occup. Ther. 1998, 52, 547–555. [Google Scholar] [CrossRef] [Green Version]
- Neel, M.L.M.; Stark, A.R.; Maitre, N.L. Parenting style impacts cognitive and behavioural outcomes of former preterm infants: A systematic review. Child Care Health Dev. 2018, 44, 507–515. [Google Scholar] [CrossRef]
- Kaaresen, P.I.; Rønning, J.A.; Ulvund, S.E.; Dahl, L.B. A randomized, controlled trial of the effectiveness of an early-intervention program in reducing parenting stress after preterm birth. Pediatrics 2006, 118, e9–e19. [Google Scholar] [CrossRef] [Green Version]
- Olafsen, K.S.; Kaaresen, P.I.; Handegård, B.H.; Ulvund, S.E.; Dahl, L.B.; Rønning, J.A. Maternal ratings of infant regulatory competence from 6 to 12 months: Influence of perceived stress, birth-weight, and intervention. A randomized controlled trial. Infant Behav. Dev. 2008, 31, 408–421. [Google Scholar] [CrossRef]
- Landsem, I.P.; Handegard, B.H.; Ulvund, S.E.; Tunby, J.; Kaaresen, P.I.; Ronning, J.A. Does an early intervention influence behavioral development until age 9 in children born prematurely? Child Dev. 2015, 86, 1063–1079. [Google Scholar] [CrossRef]
- Rauh, V.A.; Nurcombe, B.; Achenbach, T.; Howell, C. The Mother-Infant Transaction program. The content and implications of an intervention for the mothers of low- birthweight infants. Clin. Perinatol. 1990, 17, 31–45. [Google Scholar] [CrossRef]
- Buss, A.H.; Plomin, R. Temperament. Early Developing Personality Traits; Lawrence Erlbaum: Hillsdale, NJ, USA, 1984. [Google Scholar]
- Rowe, D.C.; Plomin, R. Temperament in early childhood. J. Pers. Assess. 1977, 41, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Sidor, A.; Fischer, C.; Cierpka, M. The link between infant regulatory problems, temperament traits, maternal depressive symptoms and children’s psychopathological symptoms at age three: A longitudinal study in a German at-risk sample. Child Adolesc. Psychiatry Ment. Health 2017, 11, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, F.; Giallo, R.; Hiscock, H.; Mensah, F.; Sanchez, K.; Reilly, S. Infant regulation and child mental health concerns: A longitudinal study. Pediatrics 2019, 143, e20180977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKay, E.R.; Rosinski, L.; Mayes, L.C.; Rutherford, H.J.V.; Bridgett, D.J. Maternal positive responses to a distressed infant simulator predict subsequent negative affect in infants. Infant Behav. Dev. 2019, 56, 101299. [Google Scholar] [CrossRef]
- Rajhans, P.; Goin-Kochel, R.P.; Strathearn, L.; Kim, S. It takes two! Exploring sex differences in parenting neurobiology and behaviour. J. Neuroendocrinol. 2019, 31, e12721. [Google Scholar] [CrossRef]
- Dayton, C.J.; Walsh, T.B.; Oh, W.; Volling, B. Hush now baby: Mothers’ and fathers’ strategies for soothing their infants and associated parenting outcomes. J. Pediatr. Health Care 2015, 29, 145–155. [Google Scholar] [CrossRef] [Green Version]
- Ghera, M.M.; Hane, A.A.; Malesa, E.E.; Fox, N.A. The role of infant soothability in the relation between infant negativity and maternal sensitivity. Infant Behav. Dev. 2006, 29, 289–293. [Google Scholar] [CrossRef]
- Burney, R.V.; Leerkes, E.M. Links between mothers’ and fathers’ perceptions of infant temperament and coparenting. Infant Behav. Dev. 2010, 33, 125–135. [Google Scholar] [CrossRef] [Green Version]
- Scheper, F.Y.; Majdandzic, M.; van de Ven, P.M.; Jansen, L.M.C.; Doreleijers, T.A.H.; Schuengel, C.; de Vries, A.L.C. Temperament traits and psychopathology in young clinically referred children compared to a general population sample. Child Psychiatry Hum. Dev. 2017, 48, 841–850. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| PI Group n = 72 | PC Group n = 74 | |
|---|---|---|
| Infant characteristics | ||
| BW, mean ± SD, g | 1396 ± 429 | 1381 ± 436 |
| 400–1000 g, n (%) | 20 (28) | 20 (27) |
| 1001–1500 g, n (%) | 15 (21) | 20 (27) |
| 1501–2000 g, n (%) | 37 (51) | 34 (46) |
| GA, mean ± SD, weeks | 30.2 ± 3.1 | 29.9 ± 3.5 |
| <28 weeks, n (%) | 17 (24) | 19 (27) |
| 28–32 weeks, n (%) | 36 (50) | 37 (50) |
| >33 weeks, n (%) | 19 (26) | 18 (24) |
| Boy, n (%) | 38 (53) | 39 (53) |
| Twin, n (%) | 16 (22) | 16 (21) |
| Received ventilation, n (%) | 29 (40) | 37 (50) |
| Duration of ventilation, n (%) | 7.0 ± 18.6 | 7.1 ± 17.3 |
| Postnatal steroid use, n (%) | 9 (13) | 10 (14) |
| Oxygen therapy at 38 weeks GA, n (%) | 11 (15) | 14 (19) |
| Abnormal cerebral ultrasound, n (%) | ||
| IVH grade 1 or 2 | 7 (10) | 8 (11) |
| IVH grade 3 or 4 | 3 (4) | 5 (7) |
| Periventricular leukomalacia | 4 (6) | 8 (11) |
| Maternal and social characteristics | ||
| Mother’s age a, mean ± SD, | 30.8 ± 6.1 | 29.1 ± 6.4 |
| First-born child, n (%) | 40 (56) | 37 (54) |
| Mother’s education a, mean ± SD, n = 131 | 14.6 ± 2.8 | 13.5 ± 3.2 |
| Father’s education a, mean ± SD, n = 131 | 13.8 ± 3.1 | 13.5 ± 3.2 |
| Mother’s monthly income b, | 15.8 ± 7.7 | 14.6 ± 6.7 |
| mean ± SD, n = 131 | ||
| Father’s monthly income b, | 21.1 ± 8.7 | 19.9 ± 8.1 |
| mean ± SD, n = 131 |
| No. of Items | Maternal Reports Cronbach’s Alpha | Paternal Reports Cronbach’s Alpha | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T4 | T1 | T2 | T3 | T4 | ||
| Shyness | 4 | 0.71 | 0.65 | 0.71 | 0.71 | 0.67 | 0.63 | 0.77 | 0.69 |
| Emotionality | 5 | 0.67 | 0.66 | 0.64 | 0.66 | 0.63 | 0.62 | 0.69 | 0.73 |
| Sociality | 5 | 0.62 | 0.71 | 0.67 | 0.76 | 0.56 | 0.56 | 0.57 | 0.61 |
| Activity | 5 | 0.67 | 0.67 | 0.67 | 0.66 | 0.66 | 0.64 | 0.66 | 0.63 |
| Soothability | 5 | 0.67 | 0.72 | 0.67 | 0.70 | 0.71 | 0.67 | 0.65 | 0.69 |
| PI Group | PC Group | Effects Related to Group and Time | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | T1 Mean (SE) | T2 Mean (SE) | T3 Mean (SE) | T4 Mean (SE) | T1 Mean (SE) | T2 Mean (SE) | T3 Mean (SE) | T4 Mean (SE) | Time × Group 3 | Group 4 | Time 5 |
| Shyness-m 1 | 2.21 (0.09) | 2.18 (0.09) | 2.23 (0.09) | 2.21 (0.09) | 2.28 (0.09) | 2.20 (0.09) | 2.33 (0.09) | 2.20 (0.09) | −0.02 ns. | 0.02 ns. | <0.01 ns. |
| Shyness-f 2 | 2.20 (0.08) | 2.37 (0.08) | 2.28 (0.08) | 2.16 (0.09) | 2.17 (0.9) | 2.20 (0.09) | 2.43 (0.09) | 2.19 (0.09) | 0.02 ns. | 0.05 ns. | <0.01 ns. |
| Emotionality-m 1 | 2.73 (0.08) | 2.87 (0.08) | 2.67 (0.08) | 2.72 (0.08) | 2.98 (0.08) | 3.02 (0.08) | 2.96 (0.08) | 2.80 (0.08) | −0.03 ns. | 0.33 ** | <0.01 ns. |
| Emotionality-f 2 | 2.73 (0.08) | 2.79 (0.08) | 2.68 (0.08) | 2.50 (0.08) | 2.68 (0.08) | 2.89 (0.08) | 2.83 (0.08) | 2.77 (0.08) | 0.06 * | 0.05 ns. | −0.04 * |
| Sociality-m 1 | 3.87 (0.08) | 3.99 (0.08) | 3.84 (0.07) | 3.85 (0.08) | 3.77 (0.08) | 3.95 (0.08) | 3.69 (0.08) | 3.75 (0.08) | <0.01 ns. | 0.08 ns. | −0.02 ns. |
| Sociality-f 2 | 3.80 (0.07) | 3.81 (0.07) | 3.70 (0.07) | 3.83 (0.07) | 3.77 (0.08) | 3.66 (0.08) | 3.58 (0.08) | 3.76 (0.08) | <0.01 ns. | 0.07 ns. | <0.01 ns. |
| Activity-m 1 | 4.07 (0.07) | 4.02 (0.07) | 3.50 (0.07) | 3.60 (0.07) | 3.93 (0.07) | 3.83 (0.07) | 3.44 (0.07) | 3.54 (0.07) | 0.02 ns. | 0.16 ns. | −0.11 *** |
| Activity-f 2 | 3.97 (0.07) | 3.86 (0.07) | 3.54 (0.07) | 3.43 (0.07) | 3.99 (0.07) | 3.84 (0.07) | 3.70 (0.07) | 3.57 (0.07) | 0.01 ns. | 0.08 ns. | −0.11 *** |
| Soothability-m 1 | 3.40 (0.07) | 3.42 (0.07) | 3.39 (0.07) | 3.36 (0.07) | 3.30 (0.07) | 3.13 (0.07) | 3.03 (0.07) | 3.12 (0.07) | −0.02 ns. | 0.17 ns. | −0.01 ns. |
| Soothability-f 2 | 3.46 (0.07) | 3.38 (0.07) | 3.36 (0.07) | 3.34 (0.07) | 3.17 (0.07) | 3.02 (0.07) | 3.11 (0.07) | 3.16 (0.07) | 0.03 ns. | 0.37 *** | −0.02 ns. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Landsem, I.P.; Handegård, B.H.; Ulvund, S.E. Temperamental Development among Preterm Born Children. An RCT Follow-Up Study. Children 2020, 7, 36. https://doi.org/10.3390/children7040036
Landsem IP, Handegård BH, Ulvund SE. Temperamental Development among Preterm Born Children. An RCT Follow-Up Study. Children. 2020; 7(4):36. https://doi.org/10.3390/children7040036
Chicago/Turabian StyleLandsem, Inger Pauline, Bjørn Helge Handegård, and Stein Erik Ulvund. 2020. "Temperamental Development among Preterm Born Children. An RCT Follow-Up Study" Children 7, no. 4: 36. https://doi.org/10.3390/children7040036
APA StyleLandsem, I. P., Handegård, B. H., & Ulvund, S. E. (2020). Temperamental Development among Preterm Born Children. An RCT Follow-Up Study. Children, 7(4), 36. https://doi.org/10.3390/children7040036