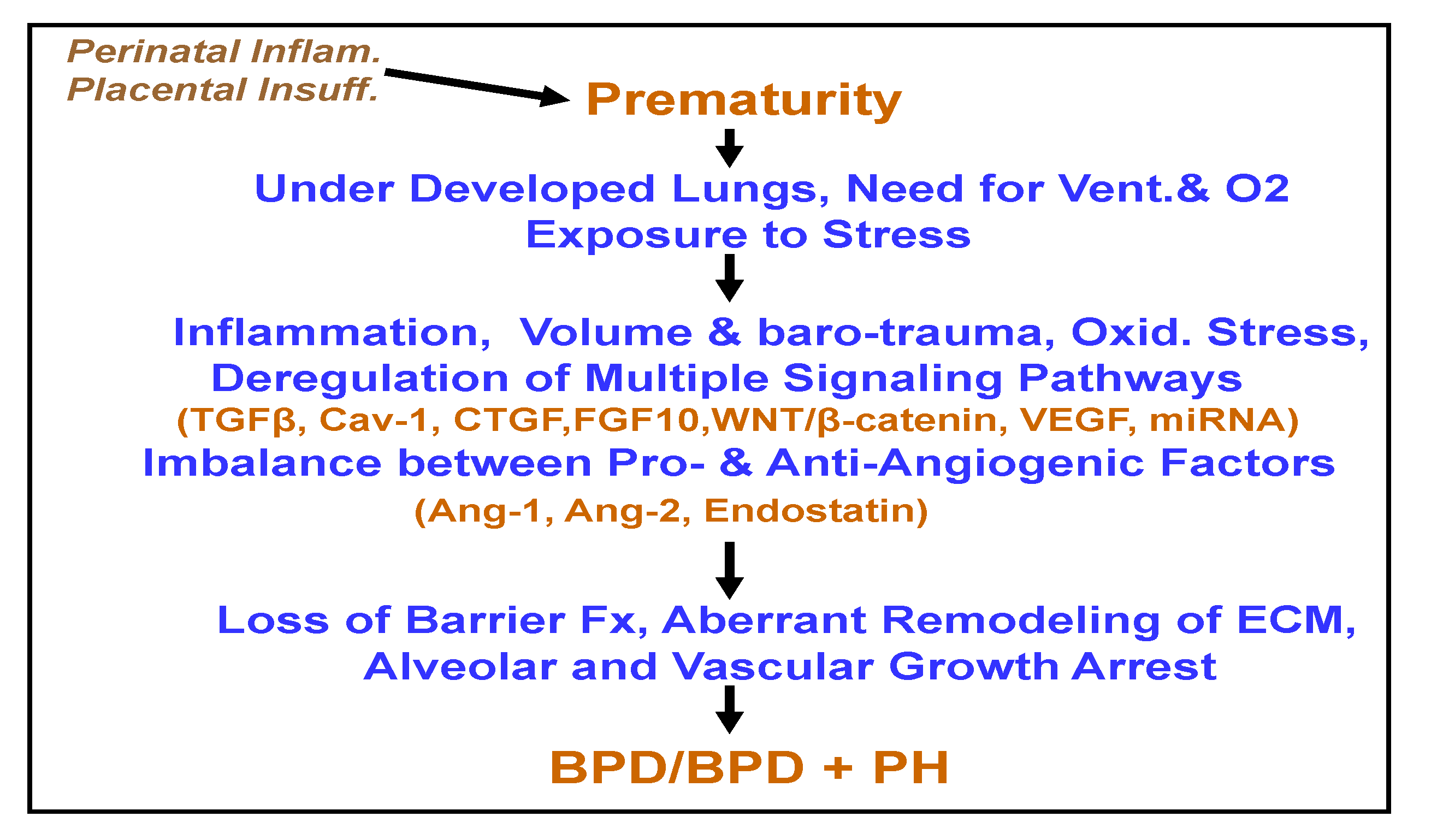
Signaling Pathways Involved in the Development of Bronchopulmonary Dysplasia and Pulmonary Hypertension

{kind=link}
Abstract
:1. Introduction
2. Inflammation, Oxidant Injury
3. Deregulated Signaling Pathways
3.1. Angiopoitins, Endostatin
3.2. Transforming Growth Factor (TGF)-β
3.3. Caveolin-1
3.4. Connective Tissue Growth Factor (CTGF)
3.5. Fibroblast Growth Factor 10 (FGF10)
3.6. WNT/β-Catenin
3.7. Vascular Endothelial Growth Factor (VEGF)
3.8. MicroRNAs
4. Loss of Barrier Function
5. Aberrant Remodeling of Extracellular Matrix (ECM)
6. Therapeutic Implications
Funding
Conflicts of Interest
References
- Ehrenkranz, R.A.; Walsh, M.C.; Vohr, B.R.; Jobe, A.H.; Wright, L.L.; Fanaroff, A.A.; Wrage, L.A.; Poole, K.; National Institutes of Child Health and Human Development Neonatal Research Network. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics 2005, 116, 1353–1360. [Google Scholar] [CrossRef] [Green Version]
- Burri, P.H. Fetal and postnatal development of the lung. Annu. Rev. Physiol. 1984, 46, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Jobe, A.H. Mechanisms of lung injury and bronchopulmonary dysplasia. Am. J. Perinatol. 2016, 33, 1076–1078. [Google Scholar] [CrossRef]
- Binet, M.-E.; Bujold, E.; Lefebvre, F.; Tremblay, Y.; Piedboeuf, B.; Canadian Neonatal Network™. Role of Gender in Morbidity and Mortality of Extremely Premature Neonates. Am. J. Perinatol. 2012, 29, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Carey, M.A.; Card, J.W.; Voltz, J.W.; Arbes, S.J., Jr.; Germolec, D.R.; Korach, K.S.; Zeldin, D.C. It’s all about sex: Male-female differences in lung development and disease. Trends Endocrinol. Metab. 2007, 18, 308–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lingappan, K.; Jiang, W.; Wang, L.; Moorthy, B. Sex-specific differences in neonatal hyperoxic lung injury. Am. J. Physiol. Lung Cell Mol. Physiol. 2016, 311, L481–L493. [Google Scholar] [CrossRef]
- Zhang, Y.; Dong, X.; Shirazi, J.; Gleghorn, J.P.; Lingappan1, K. Pulmonary endothelial cells exhibit sexual dimorphism in their response to hyperoxia. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H1287–H1292. [Google Scholar] [CrossRef] [Green Version]
- Farstad, T.; Bratlid, D.; Medbø, S.; Markestad, T.; Norwegian Extreme Prematurity Study Group. Bronchopulmonary Dysplasia–Prevalence, Severity and Predictive Factors in a National Cohort of Extremely Premature Infants. Acta Paediatr. 2011, 100, 53–58. [Google Scholar] [CrossRef]
- Fulton, C.T.; Cui, T.X.; Goldsmith, A.M.; Bermick, J.; Popova, A.P. Gene expression signatures point to a male sex-specific lung mesenchymal cell PDGF receptor signaling defect in infants developing bronchopulmonary dysplasia. Sci. Rep. 2018, 8, 17070. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, H.S.; Choi, C.W.; Kim, E.K.; Kim, B.I.; Choi, J.H. Risk factors for pulmonary artery hypertension in preterm infants with moderate or severe bronchopulmonary dysplasia. Neonatology 2012, 101, 40–46. [Google Scholar] [CrossRef]
- Underwood, M.A.; Wedgwood, S.; Lakshminrusimha, S.; Steinhorn, R.H. Somatic Growth and the Risks of Bronchopulmonary Dysplasia and Pulmonary Hypertension: Connecting Epidemiology and Physiology. Can. J. Physiol. Pharmacol. 2019, 97, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Bhat, R.; Salas, A.A.; Foster, C.; Carlo, W.A.; Ambalavanan, N. Prospective analysis of pulmonary hypertension in extremely low birth weight infants. Pediatrics 2012, 129, e682–e689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berenz, A.; Vergales, J.E.; Swanson, J.R.; Sinkin, R.A. Evidence of early pulmonary hypertension is associated with increased mortality in very low birth weight infants. Am. J. Perinatol. 2017, 34, 801–907. [Google Scholar] [CrossRef] [PubMed]
- Khemani, E.; McElhinney, D.B.; Rhein, L.; Andrade, O.; Lacro, R.V.; Thomas, K.C.; Mullen, M.P. Pulmonary artery hypertension in formerly premature infants with bronchopulmonary dysplasia: Clinical features and outcomes in the surfactant era. Pediatrics 2007, 120, 1260–1269. [Google Scholar] [CrossRef] [PubMed]
- Schachtner, S.K.; Wang, Y.; Baldwin, H.S. Qualitative and Quantitative Analysis of Embryonic Pulmonary Vessel Formation. Am. J. Respir. Cell Mol. Biol. 2000, 22, 157–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, Y.S.; Rohan, R.; Sunday, M.E.; Demello, D.E.; D’Amore, P.A. Differential expression of VEGF isoforms in mouse during development and in the adult. Dev. Dyn. 2001, 220, 112–121. [Google Scholar] [CrossRef]
- Bhatt, A.J.; Pryhubber, G.S.; Huyck, H.; Watkins, R.H.; Metlay, L.A.; Mniscalco, W.M. Disrupted Pulmonary Vasculature and Decreased Vascular Endothelial Growth Factor, Flt-1, and TIE-2 in Human Infants Dying with Bronchopulmonary Dysplasia. Am. J. Respir. Crit. Care Med. 2001, 164, 1971–1980. [Google Scholar] [CrossRef]
- Gebb, S.A.; Shannon, J.M. Tissue interactions mediate early events in pulmonary vasculogenesis. Dev. Dyn. 2000, 217, 159–169. [Google Scholar] [CrossRef]
- Stenmark, K.T.; Abman, S.H. Lung vascular development: Implications for the pathogenesis of bronchopulmonary dysplasia. Annu. Rev. Physiol. 2005, 67, 623–661. [Google Scholar] [CrossRef] [Green Version]
- Speer, C.P. Chorioamnionitis, postnatal factors and proinflammatory response in the pathogenetic sequence of bronchopulmonary dysplasia. Neonatology 2009, 95, 353–361. [Google Scholar] [CrossRef]
- Kramer, B.W.; Kallapur, S.; Newnham, J.; Jobe, A.H. Prenatal inflammation and lung development. Semin. Fetal Neonatal Med. 2009, 14, 2–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, B.H.; Romero, R.; Jun, J.K.; Park, K.H.; Park, J.D.; Ghezzi, F.; Kim, B.I. Amniotic fluid cytokines (interleukin-6, tumor necrosis factor-alpha, interleukin-1 beta, and interleukin-8) and the risk for the development of bronchopulmonary dysplasia. Am. J. Obstet. Gynecol. 1997, 177, 825–830. [Google Scholar] [CrossRef]
- Genschmer, K.R.; Russell, D.W.; Lal, C.; Szul, T.; Bratcher, P.E.; Noerager, B.D.; Roda, M.A.; Xu, X.; Rezonzew, G.; Viera, L.; et al. Activated PMN Exosomes: Pathogenic Entities Causing Matrix Destruction and Disease in the Lung. Cell 2019, 176, 113–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, D.M.G.; Nardiello, C.; Pozarska, A.; Morty, R.E. Recent advances in the mechanisms of lung alveolarization and the pathogenesis of bronchopulmonary dysplasia. Am. J. Physiol. Lung Cell Mol. Physiol. 2015, 309, L1239–L1272. [Google Scholar] [CrossRef]
- Baker, C.D.; Ryan, S.L.; Ingram, D.A.; Seedorf, G.J.; Abman, S.H.; Balasubramaniam, V. Endothelial colony-forming cells from preterm infants are increased and more susceptible to hyperoxia. Am. J. Respir. Crit. Care Med. 2009, 180, 454–461. [Google Scholar] [CrossRef] [Green Version]
- Makinde, T.; Agrawal, D.K. Intra and extra-vascular trans-membrane signaling of angiopoietin-1-Tie2 receptor in health and disease. J. Cell Mol. Med. 2008, 12, 810–828. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.P.; Marron, M.B.; Brindle, N.P. The antiinflammatory endothelial tyrosine kinase Tie2 interacts with a novel nuclear factor-kappaB inhibitor. ABIN-Circ. Res. 2003, 92, 630–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, W.; Seidenspinner, S.; Kramer, B.W.; Ska-Leda, N.K.; Chmielnicka-Kopaczyk, M.; Marx, A.; Wirbelauer, J.; Szymankiewicz, M.; Speer, C.P. Airway concentrations of angiopoietin-1 and endostatin in ventilated extremely premature infants are decreased sfter funisitis and unbalanced with bronchopulmonary dysplasia/death. Pediatr. Res. 2009, 65, 468–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janer, J.; Andersson, S.; Kajantie, E.; Lassus, P. Endostatin concentration in cord plasma predicts the development of bronchopulmonary dysplasia in very low birth weight infants. Pediatrics 2009, 123, 1142–1146. [Google Scholar] [CrossRef]
- Thomas, W.; Seidenspinner, S.; Kramer, B.W.; Wirbelauer, J.; Kawczńska-Leda, N.; Szymankiewicz, M.; Speer, C.P. Airway angiopoietin-2 in ventilated very preterm infants: Association with prenatal factors and neonatal outcome. Pediatr. Pulmonol. 2011, 46, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.; Desai, T.J.; Qian, J.; Niederreither, K.; Lü, J.; Cardoso, W.V. Inhibition of Tgf-β signaling by endogenous retinoic acid is essential for primary lung bud induction. Development 2007, 134, 2969–2979. [Google Scholar] [CrossRef] [Green Version]
- Gauldie, J.; Galt, T.; Bonniaud, P.; Robbins, C.; Kelly, M.; Warburton, D. Transfer of the active form of transforming growth factor-β1 gene to newborn rat lung induces changes consistent with BPD. Am. J. Pathol. 2003, 163, 2575–2584. [Google Scholar] [CrossRef]
- Miyawaki-Shimizu, K.; Predescu, D.; Shimizu, J.; Broman, M.; Predescu, S.; Malik, A.B. siRNA-induced caveolin-1 knockdown in mice increases lung vascular permeability via the junctional pathway. Am. J. Physiol. Lung Cell Mol. Physiol. 2006, 290, L405–L413. [Google Scholar] [CrossRef] [PubMed]
- Alejandre-Alcάzar, M.A.; Kwapiszewska, G.; Reiss, I.; Amarie, O.V.; Marsh, L.M.; Sevilla-Pe´rez, J.; Wygrecka, M.; Eul, B.; Köbrich, S.; Hesse, M.; et al. Hyperoxia modulates TGF-β/BMP signaling in a mouse model of bronchopulmonary dysplasia. Am. J. Physiol. Lung Cell Mol. Physiol. 2007, 292, L537–L549. [Google Scholar] [CrossRef] [PubMed]
- Couet, J.; Li, S.; Okamoto, T.; Ikezu, T.; Lisanti, M.P. Dentification of peptide and protein ligands for the caveolin-scaffolding domain. Implications for the interaction of caveolin with caveolae-associated proteins. Biol. Chem. 1997, 272, 6525–6533. [Google Scholar] [CrossRef] [Green Version]
- Mathew, R. Pathogenesis of pulmonary hypertension: A case for caveolin-1 and cell membrane integrity. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H15–H25. [Google Scholar] [CrossRef] [Green Version]
- Kunzmann, S.; Collins, J.J.P.; Yang, Y.; Uhlig, S.; Kallapur, S.G.; Speer, C.P.; Jobe, A.H.; Kramer, B.W. Antenatal Inflammation Reduces Expression of Caveolin-1 and Influences Multiple Signaling Pathways in Preterm Fetal Lungs. Am. J. Respir. Cell Mol. Biol. 2011, 45, 969–976. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, M.I.; Pollack, L.; Millien, G.; Cao, Y.X.; Hinds, A.; Williams, M.C. The α-isoform of caveolin-1 is a marker of vasculogenesis in early lung development. J. Histochem. Cytochem. 2002, 50, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Barar, J.; Lee Campbell, L.; Hollins, A.J.; Thomas, N.P.B.; Smith, M.W.; Morris, C.J.; Gumbleton, M. Cell Selective Glucocorticoid Induction of caveolin-1 and Caveolae in Differentiating Pulmonary Alveolar Epithelial Cell Cultures. Biochem. Biophys. Res. Commun. 2007, 359, 360–366. [Google Scholar] [CrossRef]
- Gosens, R.; Stelmack, G.L.; Bos, S.T.; Dueck, G.; Mutawe, M.M.; Schaafsma, D.; Unruh, H.; Gerthoffer, W.T.; Zaagesma, J.; Meurs, H.; et al. Caveolin-1 is required for contractile phenotype expression by airway smooth muscle cells. J. Cell. Mol. Med. 2011, 15, 2430–2442. [Google Scholar] [CrossRef] [Green Version]
- Le Saux, O.; Teeters, K.; Miyasato, S.; Choi, J.; Nakamatsu, G.; Richardson, J.A.; Starcher, B.; Davis, E.C.; Tam, E.K.; Saux, C.J.-L. The role of caveolin-1 in pulmonary matrix remodeling and mechanical properties. Am. J. Physiol. Lung Cell Mol. Physiol. 2008, 295, L1007–L1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, J.J.P.; Kunzmann, S.; Kuypers, E.; Kemp, M.W.; Speer, C.P.; Newnham, J.P.; Kallapur, S.G.; Jobe, A.H.; Kramer, B.W. Antenatal glucocorticoids counteract LPS changes in TGF-β pathway and caveolin-1 in ovine fetal lung. Am. J. Physiol. Lung Cell Mol. Physiol. 2013, 304, L438–L444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Wermuth, P.J.; Benn, B.S.; Lisanti, M.P.; Jimenez, S.A. Caveolin-1 Deficiency Induces Spontaneous Endothelial-to-Mesenchymal Transition in Murine Pulmonary Endothelial Cells in Vitro. Am. J. Pathol. 2013, 182, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Maciejewski, B.S.; Drouillard, D.; Santos, M.; Hokenson, M.A.; Hawwa, R.L.; Huang, Z.; Sanchez-Esteban, J. A role for caveolin-1 in mechanotransduction of fetal type II epithelial cells. Am. J. Physiol. Lung Cell Mol. Physiol. 2010, 298, L775–L783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dereddy, N.; Huang, J.; Erb, M.; Guzel, S.; Wolk, J.H.; Sett, S.S.; Gewitz, M.H.; Mathew, R. Associated inflammation or increased flow-mediated shear stress, but not pressure alone, disrupts endothelial caveolin-1 in infants with pulmonary hypertension. Pulm. Circ. 2012, 2, 492–500. [Google Scholar] [CrossRef] [Green Version]
- Mathew, R. Cell-Specific Dual Role of Caveolin-1 in Pulmonary Hypertension. Pulm. Med. 2011, 2011, 573432. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Frid, M.; Gewitz, M.H.; Fallon, J.T.; Brown, D.; Krafsur, G.; Stenmark, K.R.; Mathew, R. Hypoxia-induced pulmonary hypertension and chronic lung disease: Caveolin-1 dysfunction an important underlying feature. Pulm. Circ. 2019, 9, 2045894019837876. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Mathew, R. Loss of cavin1 and expression of p-Caveolin-1 in pulmonary hypertension: Possible role in neointima formation. World J. Hypertens. 2019, 9, 17–29. [Google Scholar] [CrossRef]
- Sowa, G.; Pypaert, M.; Sessa, W.C. Distinction between signaling mechanisms in lipid rafts vs. caveolae. Proc. Natl. Acad. Sci. USA 2001, 98, 14072–14077. [Google Scholar] [CrossRef] [Green Version]
- Kunzmann, S.; Speer, C.P.; Jobe, A.H.; Kramer, B.W. Antenatal inflammation induced TGF-β1 but suppressed CTGF in preterm lungs. Am. J. Physiol. Lung Cell Mol. Physiol. 2007, 292, L223–L231. [Google Scholar] [CrossRef] [Green Version]
- Brigstock, D.R. Regulation of angiogenesis and endothelial cell function by connective tissue growth factor (CTGF) and cysteine-rich 61 (CYR61). Angiogenesis 2002, 5, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cui, H.; Wu, S. CTGF: A potential therapeutic target for bronchopulmonary dysplasia. Eur. J. Pharmacol. 2019, 860, 172588. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Rong, M.; Platteau, A.; Hehre, D.; Smith, H.; Ruiz, P.; Whitsett, J.; Bancalari, E.; Wu, S. CTGF disrupts alveolarization and induces pulmonary hypertension in neonatal mice: Implication in the pathogenesis of severe bronchopulmonary dysplasia. Am. J. Physiol. Lung Cell Mol. Physiol. 2011, 300, L330–L340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alapati, D.; Rong, M.; Chen, S.; Hehre, D.; Rodriguez, M.M.; Lipson, K.E.; Wu, S. Connective tissue growth factor antibody therapy attenuates hyperoxia-induced lung injury in neonatal rats. Am. J. Respir. Cell Mol. Biol. 2011, 45, 1169–1177. [Google Scholar] [CrossRef]
- Fan, W.H.; Pech, M.; Karnovsky, M.J. Connective tissue growth factor (CTGF) stimulates vascular smooth muscle cell growth and migration in vitro. Eur. J. Cell Biol. 2000, 79, 915–923. [Google Scholar] [CrossRef]
- Volckaert, T.; De Langhe, S.P. Wnt and FGF mediated epithelial-mesenchymal crosstalk during lung development. Dev. Dyn. 2015, 244, 342–366. [Google Scholar] [CrossRef] [Green Version]
- Weaver, M.; Dunn, N.R.; Hogan, B.L. Bmp4 and Fgf10 play opposing roles during lung bud morphogenesis. Development 2000, 127, 2695–2704. [Google Scholar]
- Mailleux, A.A.; Kelly, R.; Veltmaat, J.M.; De Langhe, S.P.; Zaffran, S.; Thiery, J.P.; Bellusci, S. Fgf10 expression identifies parabronchial smooth muscle cell progenitors and is required for their entry into the smooth muscle cell lineage. Development 2005, 132, 2157–2166. [Google Scholar] [CrossRef] [Green Version]
- Yuan, T.; Volckaert, T.; Chanda, D.; Thannickal, V.J.; De Langhe, S.P. Fgf10 signaling in lung development, homeostasis, disease, and repair after injury. Front. Genet. 2018, 9, 418. [Google Scholar] [CrossRef]
- Chao, C.-M.; Moiseenko, A.; Kosanovic, D.; Rivetti, S.; El Agha, E.; Wilhelm, J.; Kampschulte, M.; Yahya, F.; Ehrhardt, H.; Zimmer, K.-P.; et al. Impact of Fgf10 deficiency on pulmonary vasculature formation in a mouse model of bronchopulmonary dysplasia. Hum. Mol. Genet. 2019, 28, 1429–1444. [Google Scholar] [CrossRef]
- Ramasamy, S.K.; Mailleux, A.A.; Gupte, V.V.; Mata, F.; Sala, F.G.; Veltmaat, J.M.; Del Moral, P.M.; De Langhe, S.; Parse, S.; Kelly, L.K.; et al. Fgf10 dosage is critical for the amplification of epithelial cell progenitors and for the formation of multiple mesenchymal lineages during lung development. Dev. Biol. 2007, 307, 237–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellusci, S.; Grindley, J.; Emoto, H.; Itoh, N.; Hogan, B.L. Fibroblast growth factor 10 (FGF10) and branching morphogenesis in the embryonic mouse lung. Development 1997, 124, 4867–4878. [Google Scholar] [PubMed]
- Benjamin, J.T.; Smith, R.J.; Halloran, B.A.; Day, T.J.; Kelly, D.R.; Prince, L.S. FGF-10 is decreased in bronchopulmonary dysplasia and suppressed by Toll-like receptor activation. Am. J. Physiol. Lung Cell Mol. Physiol. 2007, 292, L550–L558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, T.; Chi, M.; Wang, Y.; Mei, Y.; Li, Q.; Yu, M.; Ma, Q.; Chen, Y.; Feng, Z. Therapeutic effects of fibroblast growth factor-10 on hyperoxia-induced bronchopulmonary dysplasia in neonatal mice. Am. J. Transl. Res. 2017, 9, 3528–3540. [Google Scholar]
- Zhang, M.; Shi, J.; Huang, Y.; Lai, L. Expression of canonical WNT/β-CATENIN signaling components in the developing human lung. BMC Dev. Biol. 2012, 30, 12–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mucenski, M.L.; Wert, S.E.; Nation, J.M.; Loudy, D.M.; Huelsken, J.; Birchmeier, W.; Morrisey, E.E.; Whitsett, J.A. β-Catenin is required for specification of proximal/distal cell fate during lung morphogenesis. J. Biol. Chem. 2005, 378, 40231–40238. [Google Scholar] [CrossRef] [Green Version]
- Aapati, A.; Rong, M.; Chen, S.; Hehre, D.; Hummler, S.C.; Wu, S. Inhibition of β-catenin signaling improves alveolarization and reduces pulmonary hypertension in experimental bronchopulmonary dysplasia. Am. J. Respir. Cell Mol. Biol. 2014, 51, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Popova, A.P.; Bentley, J.K.; Anyanwu, A.C.; Richardson, M.N.; Linn, M.J.; Lei, J.; Wong, E.J.; Goldsmith, A.M.; Pryhuber, G.S.; Hershenson, M.B. Glycogen synthase kinase-3β/β-catenin signaling regulates neonatal lung mesenchymal stromal cell myofibroblastic differentiation. Am. J. Physiol. Lung Cell Mol. Physiol. 2012, 303, L439–L448. [Google Scholar] [CrossRef]
- Lecarpentier, Y.; Gourrier, E.; Gobert, V.; Vallée, A. Bronchopulmonary dysplasia: Crosstalk between PPARγ, WNT/β-Catenin and TGF-β pathways; the potential therapeutic role of PPARγ agonists. Front. Pediatr. 2019, 7, 176. [Google Scholar] [CrossRef]
- Dasgupta, C.; Sakurai, R.; Wang, Y.; Guo, P.; Ambalavanan, N.; Torday, J.S.; Rehan, V.K. Hyperoxia-induced neonatal rat lung injury involves activation of TGF-β and Wnt signaling and is protected by rosiglitazone. Am. J. Physiol. Lung Cell Mol. Physiol. 2009, 296, L1031–L1041. [Google Scholar] [CrossRef]
- Sucre, J.M.; Vickers, K.C.; Benjamin, J.T.; Plosa, E.J.; Jetter, C.S.; Cutrone, A.; Ransom, M.; Anderson, Z.; Sheng, Q.; Fensterheim, B.A.; et al. Hyperoxia injury in the developing lung is mediated by mesenchymal expression of Wnt5A. Am. J. Respir. Crit. Care Med. 2020, 201, 1249–1262. [Google Scholar] [CrossRef] [PubMed]
- Jakkula, M.; Le Cras, T.D.; Gebb, S.; Hirth, K.P.; Tuder, R.M.; Voelkel, N.F.; Abman, S.H. Inhibition of angiogenesis decreases alveolarization in the developing rat lung. Am. J. Physiol. Lung Cell Mol. Physiol. 2000, 279, L600–L607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Compernolle, V.; Brusselmans, K.; Acker, T.; Hoet, P.; Tjwa, M.; Beck, H.; Plaisance, S.; Dor, Y.; Keshet, E.; Lupu, F.; et al. Loss of HIF-2alpha and inhibition of VEGF impair fetal lung maturation, whereas treatment with VEGF prevents fatal respiratory distress in premature mice. Nat. Med. 2002, 8, 702–710. [Google Scholar] [CrossRef]
- Randell, S.H.; Mercer, R.R.; Young, S.L. Neonatal hyperoxia alters the pulmonary alveolar and capillary structure of 40-day-old rats. Am. J. Pathol. 1990, 136, 1259–1266. [Google Scholar]
- Le Cras, T.D.; Markham, N.E.; Tuder, R.M.; Abman, S.H. Treatment of newborn rats with a VEGF receptor inhibitor causes pulmonary hypertension and abnormal lung structure. Am. J. Physiol. Lung Cell Mol. Physiol. 2002, 283, L555–L562. [Google Scholar] [CrossRef] [Green Version]
- Lahm, T.; Crisostomo, P.R.; Markel, T.A.; Wang, M.; Lillemoe, K.D.; Meldrum, D.R. The critical role of vascular endothelial growth factor in pulmonary vascular remodeling after lung injury. Shock 2007, 28, 4–14. [Google Scholar] [CrossRef]
- Kunig, A.M.; Balasubramaniam, V.; Markham, N.E.; Morgan, D.; Montgomery, G.; Grover, T.R.; Abman, S.H. Recombinant human VEGF treatment enhances alveolarization after hyperoxic lung injury in neonatal rats. Am. J. Physiol. Lung Cell Mol. Physiol. 2005, 289, L529–L535. [Google Scholar] [CrossRef] [PubMed]
- Mokres, L.M.; Parai, K.; Hilgendorff, A.; Ertsey, R.; Alvira, C.M.; Rabinovitch, M.; Bland, R.D. Prolonged mechanical ventilation with air induces apoptosis and causes failure of alveolar septation and angiogenesis in lungs of newborn mice. Am. J. Physiol. Lung Cell Mol. Physiol. 2010, 298, L23–L35. [Google Scholar] [CrossRef] [Green Version]
- Ellis, L.V.; Cain, M.P.; Hutchison, V.; Flodby, P.; Crandall, E.D.; Borok, Z.; Zhou, B.; Ostrin, E.J.; Wythe, J.D.; Chen, J. Epithelial Vegfa specifies a distinct endothelial population in the mouse lung. Dev. Cell 2020, 52, 617–630.e6. [Google Scholar] [CrossRef]
- Syed, M.A.; Choo-Wing, R.; Homer, R.J.; Bhandari, V. Role of nitric oxide isoforms in vascular and alveolar development and lung injury in vascular endothelial growth factor overexpressing neonatal mice lungs. PLoS ONE 2016, 11, e0147588. [Google Scholar] [CrossRef]
- Xing, Y.; Fu, J.; Yang, H.; Yao, L.; Qiao, L.; Du, Y.; Xue, X. MicroRNA expression profiles and target prediction in neonatal Wistar rat lungs during the development of bronchopulmonary dysplasia. Int. J. Mol. Med. 2015, 36, 1253–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sessa, R.; Hata, A. Role of microRNAs in lung development and pulmonary diseases. Pulm. Circ. Pulm. Circ. 2013, 3, 315–328. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Dong, X.; Lingappan, K. Role of HIF-1α-miR30a-Snai1 axis in neonatal hyperoxic lung injury. Oxid. Med. Cell Longv. 2019, 2019, 8327486. [Google Scholar] [CrossRef] [Green Version]
- Alam, M.A.; Betal, S.G.N.; Aghai, Z.H.; Bhandari, V. Hyperoxia Causes miR199a-5p-mediated Injury in the Developing Lung. Pediatr. Res. 2019, 86, 579–588. [Google Scholar] [CrossRef]
- Syed, M.; Das, P.; Pawar, A.; Aghai, Z.H.; Kaskinen, A.; Zhuang, Z.W.; Ambalavanan, N.; Pryhuber, G.; Andersson, S.; Vhandari, V. Hyperoxia causes miR-34a-mediated injury via angiopoietin-1 in neonatal lungs. Nat. Commun. 2017, 8, 1173. [Google Scholar] [CrossRef]
- Chao, C.-M.; Carraro, G.A.; Rako, Z.A.; Kolck, J.; Sedighi, J.; Zimmermann, V.; Moiseenko, A.; Wilhelm, J.; Young, B.M.; Chong, L.; et al. Failure to down-regulate miR-154 expression in early postnatal mouse lung epithelium suppresses alveologenesis, with changes in Tgf-β signaling similar to those induced by exposure to hyperoxia. Cells 2020, 9, 859. [Google Scholar] [CrossRef] [Green Version]
- Olave, N.; Lal, C.V.; Halloran, B.; Pandit, K.; Cuna, A.C.; Faye-Petersen, O.M.; Kelly, D.R.; Nicola, T.; Benos, P.V.; Kaminski, N.; et al. Regulation of alveolar septation by microRNA-489. Am. J. Physiol. Lung Cell Mol. Physiol. 2016, 310, L476–L487. [Google Scholar] [CrossRef] [Green Version]
- Bhaskaran, M.; Wang, Y.; Zhang, H.; Weng, T.; Baviskar, P.; Guo, Y.; Gou, D.; Liu, L. MicroRNA-127 modulates fetal lung development. Physiol. Genom. 2009, 37, 268–278. [Google Scholar] [CrossRef] [Green Version]
- Lal, C.V.; Olave, N.; Travers, C.; Rezonzew, G.K.; Simpson, A.; Halloran, B.; Aghai, Z.; Das, P.; Sharma, N. Exosomal microRNA predicts and protects against severe bronchopulmonary dysplasia in extremely premature infants. JCI Insight 2018, 3, e93994. [Google Scholar] [CrossRef]
- Vyas-Read, S.; Vance, R.J.; Wang, W.; Colvocoresses-Dodds, J.; Brown, L.N.S.; Koval, M. Hyperoxia induces paracellular leak and alters claudin expression by neonatal alveolar epithelial cells. Pediatr. Pulmonol. 2018, 53, 17–27. [Google Scholar] [CrossRef] [Green Version]
- Mizobuchi, M.; Iwatani, S.; Sakai, H.; Yoshimoto, S.; Nakao, H. Effect of Hydrocortisone Therapy on severe leaky lung syndrome in ventilated preterm Infants. Pediatr. Int. 2012, 54, 639–645. [Google Scholar] [CrossRef]
- LaFemina, M.J.; Sutherland1, K.M.; Bentley, T.; Gonzales, L.W.; Allen, L.; Chapin, C.J.; Rokkam, D.; Sweerus, K.A.; Dobbs, L.G.; Ballard, P.L.; et al. Claudin-18 deficiency results in alveolar barrier dysfunction and impaired alveologenesis in mice. Am. J. Respir. Cell Mol. Biol. 2014, 51, 550–558. [Google Scholar] [CrossRef] [Green Version]
- You, K.; Xu, X.; Fu, J.; Xu, S.; Yue, X.; Yu, Z.; Xue, X. Hyperoxia disrupts pulmonary epithelial barrier in newborn rats via the deterioration of occluding and ZO-Respiratory. Research 2012, 13, 36. [Google Scholar]
- Overgaard, C.E.; Daugherty, B.L.; Mitchell, L.A.; Koval, M. Claudins: Control of barrier function and regulation in response to oxidant stress. Antioxid. Redox Signal. 2011, 15, 1179–1193. [Google Scholar] [CrossRef] [Green Version]
- Nusrat, A.; Parkos, C.A.; Verkade, P.; Foley, C.S.; Liang, T.W.; Innis-Whitehouse, W.K.; Eastburn, K.K.; Madara, J.L. Tight junctions are membrane microdomains. J. Cell Sci. 2000, 113, 1771–1781. [Google Scholar]
- Xu, S.; Xue, X.; You, K.; Fu, J. Caveolin-1 regulates the expression of tight junction proteins during hyperoxia-induced pulmonary epithelial barrier breakdown. Respir. Res. 2016, 17, 50. [Google Scholar] [CrossRef] [Green Version]
- Koval, M.; Billaud, M.; Straub, A.C.; Johnstone, S.R.; Zarbock, A.; Duling, B.R.; Isakson, B.E. Spontaneous lung dysfunction and fibrosis in mice lacking connexin 40 and endothelial cell connexin. Am. J. Pathol. 2011, 178, 2536–2546. [Google Scholar] [CrossRef] [Green Version]
- Mecham, R.P. Elastin in lung development and disease pathogenesis. Matrix Biol. 2018, 73, 6–20. [Google Scholar] [CrossRef]
- Thibeault, D.W.; Mabry, S.M.; Ekekezie, I.I.; Truog, W.E. Lung elastic tissue maturation and perturbations during the evolution of chronic lung disease. Pediatrics 2000, 106, 1452–1459. [Google Scholar] [CrossRef]
- Luo, Y.; Li, N.; Chen, H.; Fernandez, G.E.; Warburton, D.; Moats, R.; Mecham, R.P.; Krenitsky, D.; Pryhuber, G.S.; Shi, W. Spatial and temporal changes in extracellular elastin and laminin distribution during lung alveolar development. Sci. Rep. 2018, 8, 8334. [Google Scholar] [CrossRef]
- Mižíková1, I.; Morty, R.E. The extracellular Matrix in Bronchopulmonary Dysplasia: Target and Source. Front. Med. 2015, 2, 91. [Google Scholar] [CrossRef] [Green Version]
- Mižíková, I.; Ruiz-Camp, J.; Steenbock, H.; Madurga, A.; Vadász, Y.; Herold, S.; Mayer, K.; Seeger, W.; Brinckmann, J.; Morty, R.E. Collagen and elastin cross-linking is altered during aberrant late lung development associated with hyperoxia. Am. J. Physiol. Lung Cell Mol. Physiol. 2015, 308, L1145–L1158. [Google Scholar] [CrossRef] [Green Version]
- Witsch, T.J.; Turowski, P.; Sakkas, E.; Niess, G.; Becker, S.; Herold, S.; Mayer, K.; Vadász, I.; Roberts, J.D., Jr.; Seeger, W.; et al. Deregulation of the lysyl hydroxylase matrix cross-linking system in experimental and clinical bronchopulmonary dysplasia. Am. J. Physiol. Lung Cell Mol. Physiol. 2014, 306, L246–L259. [Google Scholar] [CrossRef]
- Nave, A.H.; Mižíková, I.; Niess, G.; Steenbock, H.; Reichenberger, F.; Talavera, M.L.; Veit, F.; Herold, S.; Mayer, K.; Vadász, I.; et al. Lysyl oxidases pPlay a causal role in vascular remodeling in clinical and experimental pulmonary arterial hypertension. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1446–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumarasamy, A.; Schmitt, I.; Nave, A.H.; Reiss, I.; van der Horst, I.; Eva Dony, E.; Roberts, J.D., Jr.; de Krijger, R.R.; Tibboel, D.; Seeger, W.; et al. Lysyl oxidase activity is dysregulated during impaired alveolarization of mouse and human lungs. Am. J. Respir. Crit. Care Med. 2009, 180, 1239–1252. [Google Scholar] [CrossRef] [Green Version]
- Mariani, T.J.; Sandefur, S.; Pierce, R.A. Elastin in lung development. Exp. Lung Res. 1997, 23, 131–145. [Google Scholar] [CrossRef]
- Li, D.Y.; Brooke, B.; Davis, E.C.; Mecham, R.P.; Sorensen, L.K.; Boak, B.B.; Eichwald, E.; Keating, M.T. Elastin Is an Essential Determinant of Arterial Morphogenesis. Nature 1998, 393, 276–280. [Google Scholar] [CrossRef]
- Bland, R.D.; Ertsey, R.; Mokres, L.M.; Xu, L.; Jacobson, B.E.; Jiang, S.; Alvira, C.M.; Rabinovitch, M.; Shinwell, E.S.; Dixit, A. Mechanical ventilation uncouples synthesis and assembly of elastin and increases apoptosis in lungs of newborn mice. Am. J. Physiol. Lung Cell Mol. Physiol. 2008, 294, L3–L14. [Google Scholar] [CrossRef] [Green Version]
- Hilgendorff, A.; Parai, K.; Ertsey, R.; Rey-Parra, G.J.; Thébaud, B.; Tamosiuniene, R.; Jain, N.; Navarro, E.F.; Starcher, B.C.; Nicolls, M.R.; et al. Neonatal mice genetically modified to express the elastase inhibitor elafin are protected against the adverse effects of mechanical ventilation on lung growth. Am. J. Physiol. Lung Cell Mol. Physiol. 2012, 303, L215–L227. [Google Scholar] [CrossRef]
- Alcazar, M.A.; Kaschwich, M.; Ertsey, R.; Preuss, S.; Milla, C.; Mujahid, S.; Msaumi, J.; Khan, S.; Mokres, L.M. Elafin Treatment Rescues EGFR-Klf4 Signaling and Lung Cell Survival in Ventilated Newborn Mice. Am. J. Respir. Cell Mol. Biol. 2018, 59, 623–634. [Google Scholar] [CrossRef]
- Mund, S.I.; Schittny, J.C. Tenascin-C deficiency impairs alveolarization and microvascular maturation during postnatal lung development. J. Appl. Physiol. 2020, 128, 1287–1298. [Google Scholar] [CrossRef] [PubMed]
- Gremlich, S.; Roth-Kleiner, M.; Equey, L.; Fytianos, K.; Schittny, J.C.; Cremona, T.P. Tenascin-C inactivation impacts lung structure and function beyond lung development. Sci. Rep. 2020, 10, 5118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaarteenaho-Wiik, R.; Kinnula, V.L.; Herva, R.; Soini, Y.; Pöllänen, R.; Pääkkö, P. Tenascin-C is highly expressed in respiratory distress syndrome and bronchopulmonary dysplasia. J. Histochem. Cytpchem. 2002, 50, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R. Pulmonary hypertension management challenges in pediatric age group. Ann. Vasc. Med. Res. 2017, 4, 1057. [Google Scholar]
- Mathew, R.; Dorai, T. Microvesicles and exosomes in pulmonary hypertension. Vessel. Plus 2020, 4, 12. [Google Scholar] [CrossRef]
- Kourembanas, S. Exosomes: Vehicles of Intercellular Signaling, Biomarkers, and Vectors of Cell Therapy. Annu. Rev. Physiol. 2015, 77, 13–27. [Google Scholar] [CrossRef] [Green Version]
- Pittenger, M.F.; Discher, D.E.; Péault, B.M.; Phinney, D.G.; Hare, J.M.; Caplan, A.J. Mesenchymal stem cell perspective: Cell biology to clinical progress. NPJ Regen. Med. 2019, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Grisafi, D.; Pozzobon, M.; Dedja, A.; Vanzo, V.; Tomanin, R.; Porzionato, A.; Macchi, V.; Salmaso, F.; Scarpa, M.; Cozzi, E.; et al. Human amniotic fluid stem cells protect rat lungs exposed to moderate hyperoxia. Pediatr. Pulmonol. 2013, 48, 1070–1080. [Google Scholar] [CrossRef]
- Jiménez, J.; Lesage, F.; Richter, J.; Nagatomo, T.; Salaets, T.; Zia, S.; Mori, D.C.M.G.; Vanoirbeek, J.; Deprest, J.A.; Toelen, J. Upregulation of vascular endothelial growth factor in amniotic fluid stem cells enhances their potential to attenuate lung injury in a preterm rabbit model of bronchopulmonary dysplasia. Neonatology 2018, 113, 275–285. [Google Scholar] [CrossRef]
- Sammour, I.; Somashekar, S.; Huang, J.; Batlahally, S.; Breton, M.; Valasaki, K.; Khan, A.; Wu, S.; Young, K.C. The effect of gender on mesenchymal stem cell (MSC) efficacy in neonatal hyperoxia-induced lung injury. PLoS ONE 2016, 11, e0164269. [Google Scholar] [CrossRef] [Green Version]
- Crisostomo, P.R.; Markel, T.A.; Wang, M.; Lahm, T.; Lillemoe, K.D.; Meldrum, D.R. In the adult mesenchymal stem cell population, source gender is a biologically relevant aspect of protective power. Surgery 2007, 142, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.S.; Ahn, S.Y.; Yoo, H.S.; Sung, S.I.; Choi, S.J.; Oh, W., II; Park, W.S. Mesenchymal stem cells for bronchopulmonary dysplasia: Phase 1 dose-escalation clinical trial. J. Pediatr. 2014, 164, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.Y.; Park, W.S.; Kim, Y.E.; Sung, D.K.; Sung, S.I.; Ahn, J.Y.; Chang, Y.S. Vascular endothelial growth factor mediates the therapeutic efficacy of mesenchymal stem cell-derived extracellular vesicles against Neonatal hyperoxic lung lnjury. Exp. Mol. Med. 2018, 13, 50. [Google Scholar]
- Qiu, G.; Zheng, G.; Ge, M.; Wang, J.; Huang, R.; Shu, Q.; Xu, J. Mesenchymal stem cell-derived extracellular vesicles affect disease outcomes via transfer of microRNAs. Stem. Cell Res. Ther. 2018, 9, 320. [Google Scholar] [CrossRef]
- Willis, G.R.; Fernandez-Gonzalez, A.; Anastas, J.; Vitali, S.H.; Liu, X.; Maria Ericsson, M.; Kwong, A.; Mitsialis, S.A.; Kourembanas, S. Mesenchymal stromal cell exosomes ameliorate experimental bronchopulmonary dysplasia and restore lung function through macrophage immunomodulation. Am. J. Respir. Crit. Care Med. 2018, 197, 104–116. [Google Scholar] [CrossRef]
- Naumburg, E.; Söderström, L.; Huber, D.; Axelsson, I. Risk factors for pulmonary arterial hypertension in children and young adults. Pediatr. Pulmonol. 2017, 52, 636–641. [Google Scholar] [CrossRef]

© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathew, R. Signaling Pathways Involved in the Development of Bronchopulmonary Dysplasia and Pulmonary Hypertension. Children 2020, 7, 100. https://doi.org/10.3390/children7080100
Mathew R. Signaling Pathways Involved in the Development of Bronchopulmonary Dysplasia and Pulmonary Hypertension. Children. 2020; 7(8):100. https://doi.org/10.3390/children7080100
Chicago/Turabian StyleMathew, Rajamma. 2020. "Signaling Pathways Involved in the Development of Bronchopulmonary Dysplasia and Pulmonary Hypertension" Children 7, no. 8: 100. https://doi.org/10.3390/children7080100
APA StyleMathew, R. (2020). Signaling Pathways Involved in the Development of Bronchopulmonary Dysplasia and Pulmonary Hypertension. Children, 7(8), 100. https://doi.org/10.3390/children7080100