COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep

 ,
,  , ,
, ,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. COVID-19 and Decreased Physical Activity
3. COVID-19 and Increased Sedentary Behavior
4. COVID-19 and Sleep
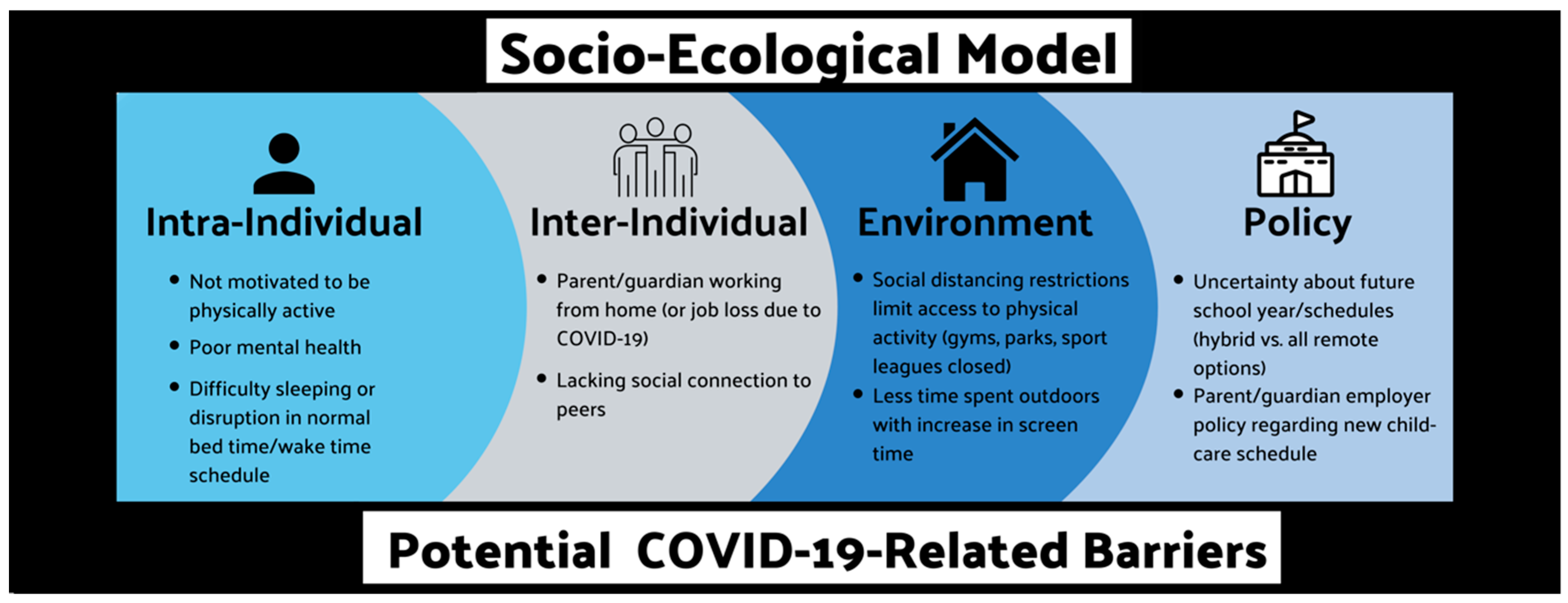
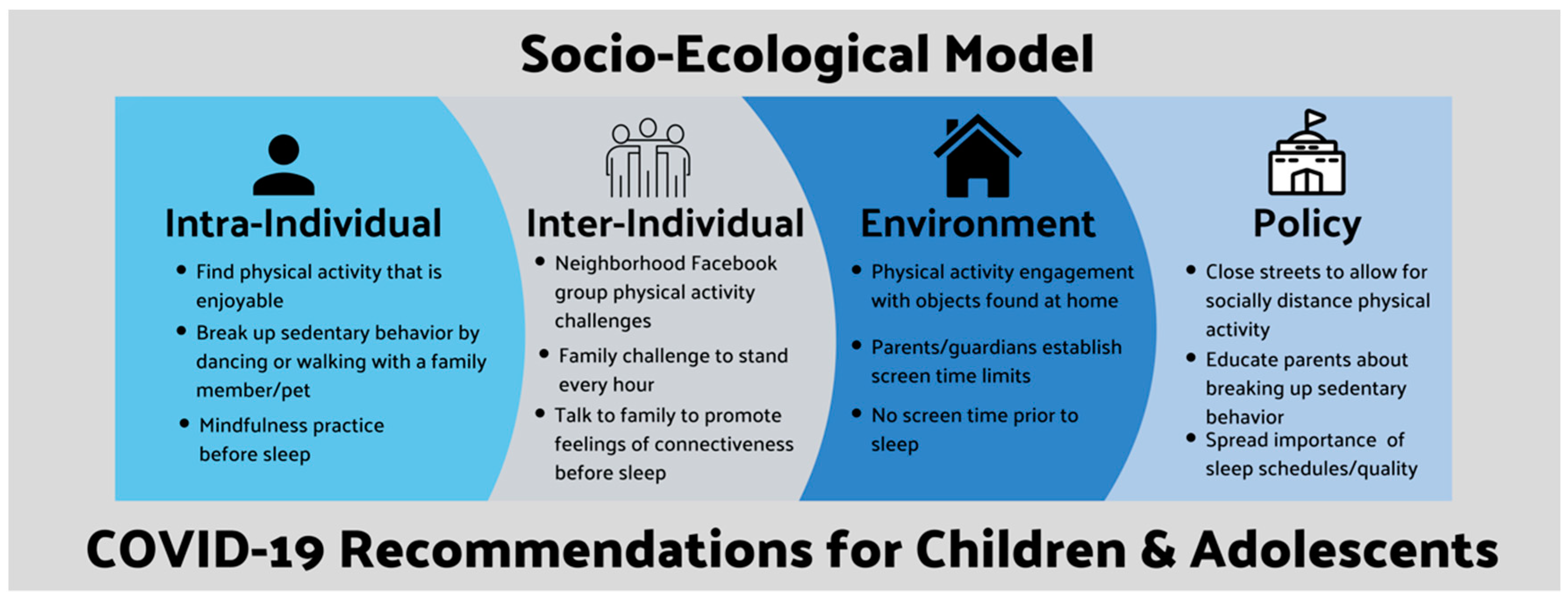
5. Intervening with a Socio-Ecological Model: Recommendations and Considerations
5.1. Physical Activity
5.2. Sedentary Behavior
5.3. Sleep
5.4. The 24-h Day Behavior Interaction—Establishing a Routine
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World HealthOrganization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Map-Johns Hopkins Coronavirus Resource Center. Available online: https://mashupmd.com/covid-19-map-johns-hopkins-coronavirus-resource-center-7/ (accessed on 20 July 2020).
- Couzin-Frankel, J.; Vogel, G.; Weiland, M. School openings across globe suggest ways to keep coronavirus at bay, despite outbreaks. Science 2020, 369, 241–245. [Google Scholar] [PubMed]
- Margaritis, I.; Houdart, S.; El Ouadrhiri, Y.; Bigard, X.; Vuillemin, A.; Duché, P. How to deal with COVID-19 epidemic-related lockdown physical inactivity and sedentary increase in youth? Adaptation of Anses’ benchmarks. Arch. Public Health 2020, 78, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Vanderloo, L.M.; Carsley, S.; Aglipay, M.; Cost, K.T.; Maguire, J.; Birken, C.S. Applying Harm Reduction Principles to Address Screen Time in Young Children Amidst the COVID-19 Pandemic. J. Dev. Behav. Pediatr. 2020, 41, 335–336. [Google Scholar] [CrossRef]
- Lee, J. Mental health effects of school closures during COVID-19. Lancet Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef]
- Becker, S.P.; Gregory, A.M. Editorial Perspective: Perils and promise for child and adolescent sleep and associated psychopathology during the COVID-19 pandemic. J. Child Psychol. Psychiatry Allied Discip. 2020, 61, 757–759. [Google Scholar] [CrossRef]
- Zenic, N.; Taiar, R.; Gilic, B.; Blazevic, M.; Maric, D.; Pojskic, H.; Sekulic, D. Levels and changes of physical activity in adolescents during the COVID-19 Pandemic: Contextualizing urban vs. Rural living environment. Appl. Sci. 2020, 10, 3997. [Google Scholar] [CrossRef]
- Moore, S.; Faulkner, G.; Rhodes, R.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.; Mitra, R.; O’Reilly, N.; Spence, J.; Vanderloo, L.; et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Submitted 2020. [Google Scholar] [CrossRef]
- Guerrero, M.D.; Vanderloo, L.M.; Rhodes, R.E.; Faulkner, G.; Moore, S.A.; Tremblay, M.S. Canadian children’s and youth’s adherence to the 24-h movement guidelines during the COVID-19 pandemic: A decision tree analysis. J. Sport Health Sci. 2020, 9, 313–321. [Google Scholar] [CrossRef]
- Grgic, J.; Dumuid, D.; Bengoechea, E.G.; Shrestha, N.; Bauman, A.; Olds, T.; Pedisic, Z. Health outcomes associated with reallocations of time between sleep, sedentary behaviour, and physical activity: A systematic scoping review of isotemporal substitution studies. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 69. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Connor Gorber, S.; et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: An update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef] [PubMed]
- Healthy Campus 2020-Ecological Model. American College Health Association. Available online: https://www.acha.org/HealthyCampus/HealthyCampus/Ecological_Model.aspx (accessed on 20 July 2020).
- Roman-Viñas, B.; Chaput, J.-P.; Katzmarzyk, P.T.; Fogelholm, M.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; Onywera, V.; Sarmiento, O.L.; et al. Proportion of children meeting recommendations for 24-h movement guidelines and associations with adiposity in a 12-country study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberger, M.E.; Fulton, J.E.; Buman, M.P.; Troiano, R.P.; Grandner, M.A.; Buchner, D.M.; Haskell, W.L. The 24-Hour Activity Cycle: A New Paradigm for Physical Activity. Med. Sci. Sports Exerc. 2019, 51, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, T.J.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Olds, T.; Connor Gorber, S.; Kho, M.E.; Sampson, M.; et al. Combinations of physical activity, sedentary behaviour and sleep: Relationships with health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S283–S293. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Carson, V.; Chaput, J.-P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Australian Government (Department of Health) Australian 24-Hour Movement Guidelines for Children and Young People (5 to 17 years). Available online: https://www1.health.gove.au/internet/main/publishing.nsf/Content/AC46EFBE3130BC97CA2583D00023E7B0/$File/Australian%2024-Hour%20Movement%20Guidelines%20for%20Children%20and%20Young%20People%205-17%20years.pdf (accessed on 20 July 2020).
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Spence, J.C.; Berry, T.; Faulkner, G.; Latimer-Cheung, A.E.; O’Reilly, N.; Tremblay, M.S.; Vanderloo, L. Parental support of the Canadian 24-h movement guidelines for children and youth: Prevalence and correlates. BMC Public Health 2019, 19, 1385. [Google Scholar] [CrossRef] [Green Version]
- Guan, H.; Okely, A.D.; Aguilar-Farias, N.; del Pozo Cruz, B.; Draper, C.E.; El Hamdouchi, A.; Florindo, A.A.; Jáuregui, A.; Katzmarzyk, P.T.; Kontsevaya, A.; et al. Promoting healthy movement behaviours among children during the COVID-19 pandemic. Lancet Child Adolesc. Health 2020, 4, 416–418. [Google Scholar] [CrossRef]
- Santos, D.A.; Silva, A.M.; Baptista, F.; Santos, R.; Vale, S.; Mota, J.; Sardinha, L.B. Sedentary behavior and physical activity are independently related to functional fitness in older adults. Exp. Gerontol. 2012, 47, 908–912. [Google Scholar] [CrossRef]
- Salmon, J.; Tremblay, M.S.; Marshall, S.J.; Hume, C. Health risks, correlates, and interventions to reduce sedentary behavior in young people. Am. J. Prev. Med. 2011, 41, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.A.; Byun, W. Sedentary behavior and health outcomes in children and adolescents. Am. J. Lifestyle Med. 2014, 8, 173–199. [Google Scholar] [CrossRef]
- Fakhouri, T.H.I.; Hughes, J.P.; Brody, D.J.; Kit, B.K.; Ogden, C.L. Physical Activity and Screen-Time Viewing Among Elementary School–Aged Children in the United States From 2009 to 2010. JAMA Pediatr. 2013, 167, 223–229. [Google Scholar] [CrossRef] [Green Version]
- Xiang, M.; Zhang, Z.; Kuwahara, K. Impact of COVID-19 Pandemic on children and adolescents’ lifestyle behavior larger than expected. Prog. Cardiovasc. Dis. 2020. [Google Scholar] [CrossRef]
- Dunton, G.; Do, B.; Wang, S. Early Effects of the COVID-19 Pandemic on Physical Activity and Sedentary Behavior in U.S. Children. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef]
- Paruthi, S.; Brooks, L.J.; Ambrosio, C.D.; Hall, W.A.; Kotagal, S.; Lloyd, R.M.; Malow, B.A.; Maski, K.; Nichols, C.; Quan, S.F.; et al. Consensus Statement of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2016, 12, 1553–1561. [Google Scholar] [CrossRef]
- Rudnicka, A.R.; Nightingale, C.M.; Donin, A.S.; Sattar, N.; Cook, D.G.; Whincup, P.H.; Owen, C.G. Sleep duration and risk of type 2 diabetes. Pediatrics 2017, 140, e20170338. [Google Scholar] [CrossRef] [Green Version]
- Jiao, W.Y.; Wang, L.N.; Liu, J.; Fang, S.F.; Jiao, F.Y.; Pettobello-Mantovani, M.; Somekh, E. Behavioral and Emotional Disorders in Children during the COVID-19 Epidemic. J. Pediatr. 2020, 21, 264. [Google Scholar] [CrossRef]
- Wang, G.; Zhang, Y.; Zhao, J.; Zhang, J.; Jiang, F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 2020, 395, 945–947. [Google Scholar] [CrossRef]
- Zhou, S.J.; Zhang, L.G.; Wang, L.L.; Guo, Z.C.; Wang, J.Q.; Chen, J.C.; Liu, M.; Chen, X.; Chen, J.X. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur. Child Adolesc. Psychiatry 2020, 29, 749–758. [Google Scholar] [CrossRef]
- Is the Pandemic Having an Impact on the Way Children Sleep? Available online: https://www.hopkinsallchildrens.org/ACH-News/General-News/Is-the-Pandemic-Having-an-Impact-on-the-Way-Childr. (accessed on 15 September 2020).
- Baranowski, T.; O’Connor, T.; Johnston, C.; Hughes, S.; Moreno, J.; Chen, T.-A.; Meltzer, L.; Baranowski, J. School year versus summer differences in child weight gain: A narrative review. Child. Obes. 2014, 10, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Brazendale, K.; Beets, M.W.; Weaver, R.G.; Pate, R.R.; Turner-McGrievy, G.M.; Kaczynski, A.T.; Chandler, J.L.; Bohnert, A.; von Hippel, P.T. Understanding differences between summer vs. school obesogenic behaviors of children: The structured days hypothesis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- Moreno, J.P.; Crowley, S.J.; Alfano, C.A.; Hannay, K.M.; Thompson, D.; Baranowski, T. Potential circadian and circannual rhythm contributions to the obesity epidemic in elementary school age children. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merikanto, I.; Kuula, L.; Lahti, J.; Räikkönen, K.; Pesonen, A.-K. Eveningness associates with lower physical activity from pre-to late adolescence. Sleep Med. 2020. [Google Scholar] [CrossRef]
- Youngstedt, S.D.; Kline, C.E.; Elliott, J.A.; Zielinski, M.R.; Devlin, T.M.; Moore, T.A. Circadian Phase-Shifting Effects of Bright Light, Exercise, and Bright Light + Exercise. J. Circadian Rhythms 2016, 14, 2. [Google Scholar]
- Hisler, G.; Twenge, J.M.; Krizan, Z. Associations between screen time and short sleep duration among adolescents varies by media type: Evidence from a cohort study. Sleep Med. 2020, 66, 92–102. [Google Scholar] [CrossRef]
- Maume, D.J. Social Ties and Adolescent Sleep Disruption. J. Health Soc. Behav. 2013, 54, 498–515. [Google Scholar] [CrossRef]
- Altena, E.; Baglioni, C.; Espie, C.A.; Ellis, J.; Gavriloff, D.; Holzinger, B.; Schlarb, A.; Frase, L.; Jernelöv, S.; Riemann, D. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: Practical recommendations from a task force of the European CBT-I Academy. J. Sleep Res. 2020. [Google Scholar] [CrossRef]
- Kuehn, B.M. Resetting the circadian clock might boost metabolic health. JAMA-J. Am. Med. Assoc. 2017, 317, 1303–1305. [Google Scholar] [CrossRef]
- Nelson, C.L. The relationship between sleep and sedentary time, and the impact of varying sleep patterns. Grad. Theses Diss. 2017, 16183. [Google Scholar] [CrossRef]
- Cho, Y.M.; Ryu, S.H.; Lee, B.R.; Kim, K.H.; Lee, E.; Choi, J. Effects of artificial light at night on human health: A literature review of observational and experimental studies applied to exposure assessment. Chronobiol. Int. 2015, 32, 1294–1310. [Google Scholar] [CrossRef] [PubMed]
- Blume, C.; Schmidt, M.H.; Cajochen, C. Effects of the COVID-19 lockdown on human sleep and rest-activity rhythms. Curr. Biol. 2020, 30, R795–R797. [Google Scholar] [CrossRef] [PubMed]
- Stoner, L.; Beets, M.W.; Brazendale, K.; Moore, J.B.; Weaver, R.G. Social Jetlag Is Associated With Adiposity in Children. Glob. Pediatr. Health 2018, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Z.-D.; Wang, Z.-Y.; Zhang, S.-F.; Li, X.; Li, L.; Li, C.; Cui, Y.; Fu, R.-B.; Dong, Y.-Z.; Chi, X.-Y. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis 2020, 26, 10–3201. [Google Scholar] [CrossRef]
- Morawska, L.; Cao, J. Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef]
- King, A.J.; Burke, L.M.; Halson, S.L.; Hawley, J.A. The Challenge of Maintaining Metabolic Health During a Global Pandemic. Sport. Med. 2020, 50, 1233–1241. [Google Scholar] [CrossRef]
- An, R. Projecting the impact of the coronavirus disease-19 pandemic on childhood obesity in the United States: A microsimulation model. J. Sport Health Sci. 2020, 9, 302–311. [Google Scholar] [CrossRef]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bates, L.C.; Zieff, G.; Stanford, K.; Moore, J.B.; Kerr, Z.Y.; Hanson, E.D.; Barone Gibbs, B.; Kline, C.E.; Stoner, L. COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep. Children 2020, 7, 138. https://doi.org/10.3390/children7090138
Bates LC, Zieff G, Stanford K, Moore JB, Kerr ZY, Hanson ED, Barone Gibbs B, Kline CE, Stoner L. COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep. Children. 2020; 7(9):138. https://doi.org/10.3390/children7090138
Chicago/Turabian StyleBates, Lauren C., Gabriel Zieff, Kathleen Stanford, Justin B. Moore, Zachary Y. Kerr, Erik D. Hanson, Bethany Barone Gibbs, Christopher E. Kline, and Lee Stoner. 2020. "COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep" Children 7, no. 9: 138. https://doi.org/10.3390/children7090138
APA StyleBates, L. C., Zieff, G., Stanford, K., Moore, J. B., Kerr, Z. Y., Hanson, E. D., Barone Gibbs, B., Kline, C. E., & Stoner, L. (2020). COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep. Children, 7(9), 138. https://doi.org/10.3390/children7090138