1. Introduction
Patellofemoral instability is a frequent cause of knee injury that occurs in the pediatric population [
1,
2]. The incidence rate is 29–43 per 100,000 individuals. The incidence of chronic instability is exceptionally high among girls between 10 and 17 [
3]. The dynamics of the patellofemoral joint depends on both bony and soft tissue structures [
4]. Therefore, developmental anomalies, traumatic disruption of static restraints, and weak dynamic stabilizers can lead to symptomatic instability [
5,
6]. Osteochondral fractures are an infrequent accompanying injury which can be successfully managed with the Steadman technique [
7]. Some patients may benefit from platelet-rich plasma (PRP) injections in order to reduce the pain caused by injury to other structures of the knee such as the meniscus [
8].
Clinical diagnosis is mainly based on the medical history of patellar dislocation and the extent of the hemarthrosis that must be evacuated to reduce pain [
9]. In order to correctly assess a patellofemoral instability, clinical examination, conventional X-rays, and C.T. or MRI are needed [
10]. However, in most severe cases, computed tomography followed by 3D reconstruction and 3D printing can help the orthopedic surgeon to plan the safest and the most effective surgical approach [
11].
Conservative treatment usually consists of cast or splint immobilization, resulting in longer rehabilitation periods as well as a recurrence rate of up to 44% [
6,
8]. Surgical treatment is the next recommended step if conservative management fails to improve the symptoms significantly. Surgery is recommended in the case of recurrent dislocation [
12].
Two popular surgical treatments are lateral release with medial imbrication (LRMI) and medial patellofemoral ligament reconstruction (MPFL-R). Lateral release is sometimes also performed along with MPFL-R to reduce the pull of the lateral retinaculum in order to decrease the stress placed on the medial retinaculum, and is an especially useful technique in pediatric patients [
13]. However, there is conflicting information in the literature regarding LRMI, with several recent studies demonstrating good outcomes following application of the technique. In contrast, other studies have shown a high failure rate and a high occurrence of complications [
14,
15]. MPFL-R aims to restore the normal anatomy of the knee joint with either a autograft or a synthetic graft. Because the MPFL is the main restraint to lateral dislocation in the first 30° of flexion, proper reconstruction will prevent the recurrence of dislocation and prevent undue stress on the knee caused by an abnormal anatomy [
16].
The International Knee Documentation Committee Pediatric (IKDC-Pedi) questionnaire has been shown to be relevant is assessments of patient QoL in a variety of knee injuries, including patellar dislocation [
17].
2. Materials and Methods
The purpose of the study was to assess the QoL of patients that suffered from episodic patellar dislocation and were treated using LRMI or MPFL-R with a double bundle synthetic graft. The average patient age at diagnosis of patellar dislocation was 13.3 years ± 2 years; see
Figure 1 Most patients (96%) had at least two more luxation episodes between diagnosis and surgery.
The study was carried out on 108 pediatric patients (aged 10–18) that had undergone either LRMI or MPFL-R between 2013–2018. The diagnosis was established based on clinical findings, radiologic exams, and magnetic resonance imaging scans, using the following inclusion criteria: history of multiple locked dislocations or locked dislocation present at admission, presence of hemarthrosis, positive apprehension test, painful medial parapatellar structures, and femoral epicondyle, as well as a minimum follow-up of 24 months. Exclusion criteria were: avulsion fracture or femoral condyle osteochondral fracture, lack of preoperative and postoperative knee radiographs, or lack of informed consent. Knee radiographs performed in the anteroposterior and lateral view were used to identify complications. Magnetic resonance imaging (MRI) was used to evaluate soft tissue lesions and to determine the treatment plan by examining the growth plate and assessing whether additional procedures were needed, such as trochleoplasty or patellar tendon realignment. Both surgeries have similar indications, namely, recurrent patellar dislocation with severe trochlear dysplasia. Postop complications that would affect patient outcomes include recurrent dislocation or pain due to the altered knee anatomy; however, the latter occurs mainly in LRMI. LRMI also presents a risk of overly reducing lateral forces on the patella, thus inducing medial dislocation, worsening the patient’s QoL and requiring further corrective surgery [
18].
Patients were randomly assigned to a surgical group in the following manner: those diagnosed on an even date were assigned to LRMI while those diagnosed on an uneven date were assigned to MPFL-R. Following the randomization, 80 patients were assigned to the LRMI group and 28 to the MPFL-R group. The mean age at surgery was 14.2 years ± 2 years in the LRMI group and 14.5 years ± 2 years in the MPFL-R group. There were no statistically significant differences in age (
p = 0.091) or sex (
p = 0.07); see
Figure 1.
The postoperative rehabilitation protocol consisted of 1 week of avoiding weight-bearing movements on the operated knee, with subsequent physiotherapy with the purpose of increasing knee stability and proprioception.
Quality of life was evaluated before and after surgery using the Pediatric International Knee Documentation Committee (IKDC-Pedi) form. The postoperative evaluation of the quality of life was conducted after 24 months of follow-up. The average interval from surgery to follow-up was 30 months (25–50 months). Postoperative scarring was also assessed using The Stony Brook Scar Evaluation Scale (SBSES). Patients filled out the questionnaires under parental guidance in the presence of the attending physician.
For statistical analysis, we assumed a null hypothesis of equal efficacy of MPFL-R and LRMI. We set the significance level at 5% (0.05). We modeled the frequency by running a Shapiro-Wilk Test. As the data went through normal distribution, the independent Student-T test was used to compare IKDC-Pedi scores between patients who had undergone LRMI surgery and those who experienced MPFL-R. The response to the athletic ability-related question on the Pedi-IKDC form could not be used to express a normal distribution, so a Mann-Whitney U test was run to check for statistical significance. As the scar evaluation data was not equally distributed, a Mann-Whitney U test was also needed. Standard deviation (S.D.) was calculated, and a confidence interval (CI) of 95% was used.
The acquired and statistically analyzed data comprised the following variables: age, sex, type of surgery, date of surgery, athletic level, preoperative IKDC-Pedi score, postoperative IKDC-Pedi score, postoperative The Stony Brook Scar Evaluation Scale.
3. Results
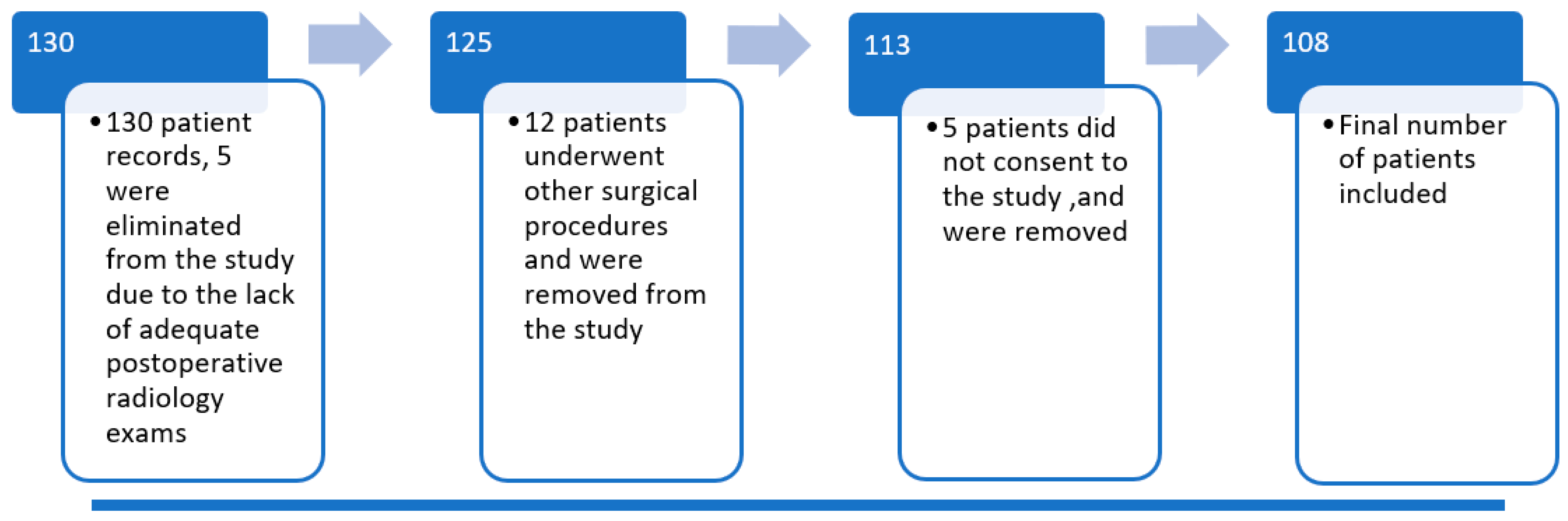
A total number of 130 patients were operated on for episodic patellar dislocation in the selected time interval. Five of them were excluded from the study due to a lack of adequate postoperative radiographs. Twelve more were excluded because they underwent other, subsequent surgical techniques. Five patients did not consent to take part in the study. One hundred and eight recreational athletes fulfilled the inclusion and exclusion criteria, completed the questionnaires, and presented at follow-up (see flow chart below-
Figure 2).
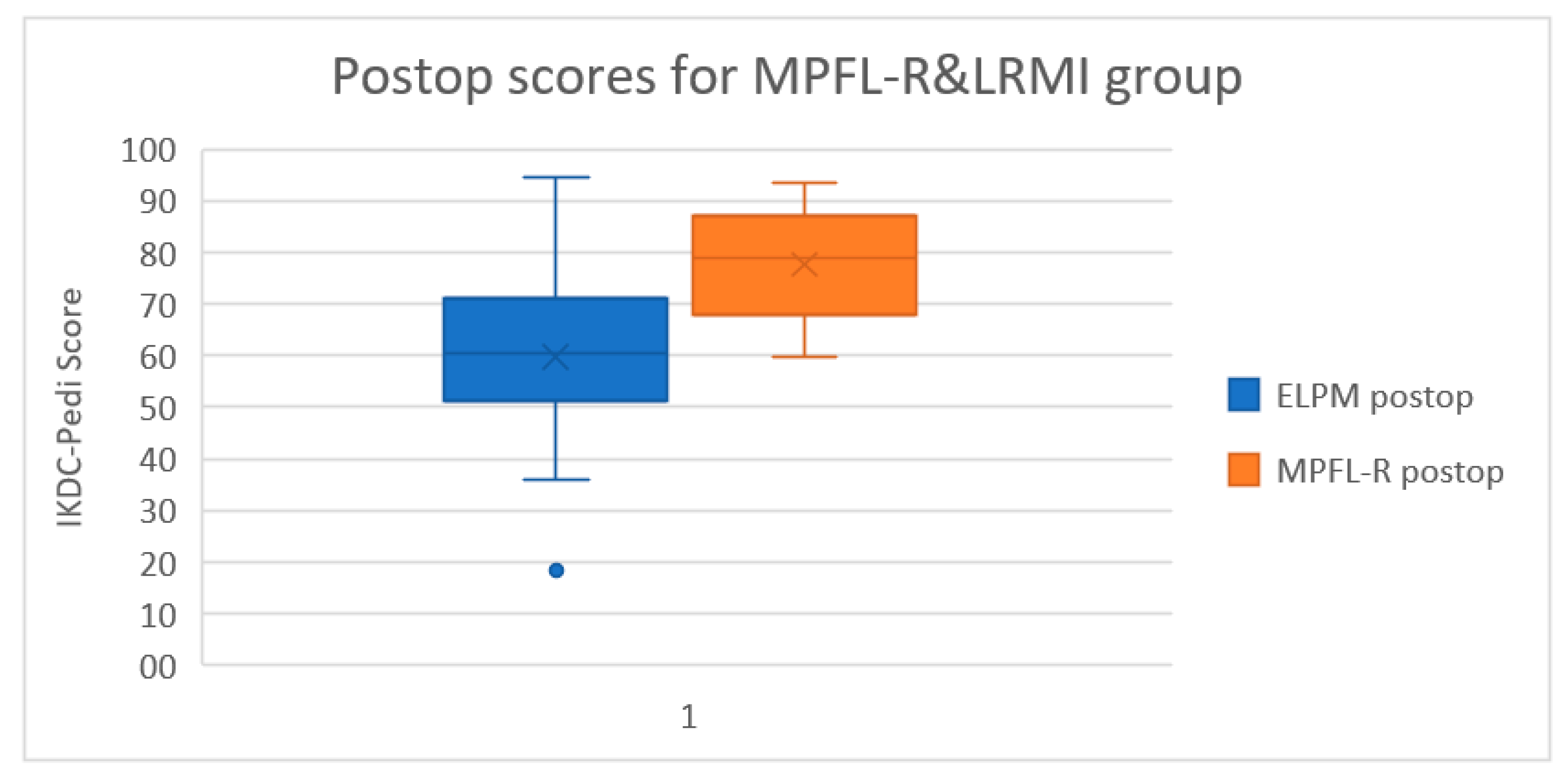
Preoperatively, the Pedi-IKDC scores were similar between the two surgical groups (MPFL-R 41.4 points vs. LRMI 39.4 points), and the difference was not statistically significant (
p = 0.314). We found significant improvement following both surgical approaches, with the MPFL-R group scoring better than LRMI in postoperative IKDC-Pedi forms compared to preoperative assessment (MPFL-R + 36.36 points-95% CI (27.76–44.97) vs. LRMI +20 points-95% CI (15.11–25.53),
p < 0.0001). A statistically significant difference in the postoperative IKDC-Pedi score between the two groups (MPFL-R 77.71 points vs. LRMI 59.74 points,
p < 0.0001-95% CI (11.22–24.72)) was observed (see
Figure 3).
There was also a statistically significant difference regarding the pain related questions of the Pedi-IKDC questionnaire, favoring MPFL-R (MPFL-R 15.8 points vs. LRMI 12.3 points p = 0.00175 95% CI (1.36–6.21).
4. Discussion
The patients from the MPFL-R group had significantly better IKDC-Pedi scores as well as significantly better scar quality. The different Pedi-IKDC scores were primarily tied to patient ability to improve or return to their previous activity level. The questions related to athletic ability showed the most significant differences in favor of MPFL-R. One possible explanation may be the faster mobilization postsurgery, which would protect against the muscular atrophy caused by immobilization [
19].
IKDC-Pedi was chosen as the QoL measurement because it had better responsiveness than KOOS-Child. In addition, as a shorter questionnaire makes, it is more likely to be fully completed in a clinical setting [
20].
The Stony Brook Scar Evaluation Scale (SBSES) was selected for the same reasons: the short time required for its completion and its good clinical relevancy [
21].
This is because MPFL-R restores the normal anatomy of the knee, thus facilitating regular joint reaction forces [
18]. However, in LRMI, the increased joint forces could cause unpleasant sensations like pressure or pain in the knee joint [
22].
The postoperative score for the MPFL-R group correlated with data from other studies found in literature, indicating good surgical technique and rehabilitation programs [
23]. The LRMI group had fewer reported redislocations than most studies using a similar surgical technique, yet the IKDC-Pedi score was lower than expected [
24,
25].
The cosmetic differences between the two procedures are also undeniable. MPFL-R is far less invasive and results in a significantly better-looking postsurgical scar. The SBSES does not consider scar length, and it should be mentioned that the MPFL-R group has two short scars while the LRMI has one long scar. As observed in our study, this is a cause of distress for patients even if the scar itself has healed without abnormal pigmentation, elevation, or depression.
One significant factor in this patient group is tibial and femoral physis [
26]. While the surgical technique used for MPFL-R in this study does not usually affect the growth plate, there is still a slight risk. In contrast, the LRMI procedure only involves the soft tissues surrounding the knee, eliminating any risk of damage to the growth plate.
Lateral release on its own has yielded unsatisfactory outcomes in the history of pa-llar dislocation treatment [
27], and release of a normal lateral retinaculum may increase lateral patellar translation and cause even more instability due to the role of the lateral retinaculum in resisting lateral patellar translation [
28]. In one study which compared MPFL-R without lateral release and MPFL-R with a lateral release, the groups had similar outcomes, thus showing that lateral release is not mandatory [
29].
The follow-up period was clinically relevant because most redislocations (70%) occur within 24 months postoperatively [
30]. However, it is insufficient to determine whether differences in joint anatomy that result after surgery remotely affect the incidence of osteoarthritis. This would require a lengthy, hard-to-manage longitudinal study. However, when considering the fact that patellar instability very often leads to unfavorable outcomes in adults, either surgery is desirable compared to nonsurgical treatment [
31].
The strengths in our study were the homogeneity of the surgical techniques that were identical for all patients and the homogeneity of the study groups concerning risk factors for patellar dislocation. The limitations were the unequal treatment groups as well as differences in follow-up period.
5. Conclusions
MPFL-R increased patient quality of life more than LRMI. MPFL-R interventions are minimally invasive, reduce postoperative recovery time and increase quality of life. This study provides further evidence for the recommendation of MPFL-R as the gold standard for patellofemoral instability. However, further studies are needed to observe the long-term stability and side effects of MPFL-R.
Author Contributions
Conceptualization, produced the results, discussion and conclusions, and assembled the paper, A.H., V.P., C.N.L., A.C. and A.U. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of “Grigore Alexandrescu” Children’s Emergency Clinical Hospital of Bucharest on the 1 March 2013. The study code is 7/01.03.2013.
Informed Consent Statement
Informed consent was obtained from the parents of all subjects involved in the study.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| LRMI | Lateral Release and Medial Imbrication approach |
| MPFL-R | Medial Patellofemoral Ligament Reconstruction |
| Pedi-IKDC | Pediatric International Knee Documentation Committee form |
| MPFL | The medial patellofemoral ligament |
| QoL | The quality of life |
| SBSES | The Stony Brook Scar Evaluation Scale |
| SD | Standard deviation |
| CI | Confidence interval |
| PRP | Platelet-Rich Plasma |
References
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L. Epidemiology and Natural History of Acute Patellar Dislocation. Am. J. Sports Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Hennrikus, W.; Pylawka, T. Patellofemoral instability in skeletally immature athletes. J. Bone Jt. Surg. Am. 2013, 95, 176–183. [Google Scholar]
- Atkin, D.; Fithian, D.; Marangi, K.; Stone, M.; Dobson, B.; Mendelsohn, C. Characteristics of patients with primary acute lateral patelar dislocation and their recovery within the first 6 months. Am. J. Sports Med. 2000, 28, 472–479. [Google Scholar] [CrossRef]
- Steense, R.N.; Bentley, J.C.; Trinh, T.O.; Backes, J.R.; Wiltfong, R.E. The prevalence and combined prevalences of an-atomic factors associated with recurrent patellar dislocaton: A magnetic resonance imaging study. Am. J. Sports Med. 2015, 43, 921–927. [Google Scholar] [CrossRef]
- Ries, Z.; Bollier, M. Patellofemoral Instability in Active Adolescents. J. Knee Surg. 2015, 28, 265–278. [Google Scholar] [CrossRef]
- Arendt, J.A.; Moore, A. First time patella dislocations: Characterizing their readiness for return to activity. Br. J. Sports Med. 2011, 45, 335–336. [Google Scholar] [CrossRef]
- Pellegrino, M.; Trinchese, E.; Bisaccia, M.; Rinonapoli, G.; Meccariello, L.; Falzarano, G.; Medici, A.; Piscitelli, L.; Ferrara, P.; Caraffa, A. Long term outcome of grade III and IV chondral injuries of the knee treat with Steadman microfracture technique. Clin. Case Miner. Bone Metab. 2016, 13, 237–240. [Google Scholar]
- Popescu, M.B.; Carp, M.; Tevanov, I.; Nahoi, C.A.; Stratila, M.A.; Haram, O.M.; Ulici, A. Isolated Meniscus Tears in Adolescent Patients Treated with Platelet-Rich Plasma Intra-articular Injections: 3-Month Clinical Outcome. BioMed Res. Int. 2020, 2020, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Sisk, D.; Fredericson, M. Update of Risk Factors, Diagnosis, and Management of Patellofemoral Pain. Curr. Rev. Musculoskelet. Med. 2019, 12, 534–541. [Google Scholar] [CrossRef]
- Clark, D.; Metcalfe, A.; Wogan, C.; Mandalia, V.; Eldridge, J. Adolescent patellar instability. Bone Jt. J. 2017, 99-B, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Tevanov, I.; Liciu, E.; Chirila, M.; Dusca, A.; Ulici, A. The use of 3D printing in impoving patient-doctor relationship and malpractice prevention. Rom. Soc. Leg. Med. 2017, 25, 279–282. [Google Scholar] [CrossRef]
- Vellios, E.E.; Trivellas, M.; Arshi, A.; Beck, J.J. Recurrent Patellofemoral Instability in the Pediatric Patient: Manage-ment and Pitfalls. Curr. Rev. Musculoskelet. Med. 2020, 13, 58–68. [Google Scholar] [CrossRef]
- Roger, J.; Viste, A.; Cievet-Bonfils, M.; Pracros, J.-P.; Raux, S.; Chotel, F. Axial patellar engagement index and patellar tilt after medial patello-femoral ligament reconstruction in children and adolescents. Orthop. Traumatol. Surg. Res. 2019, 105, 133–138. [Google Scholar] [CrossRef]
- Lee, J.-J.; Lee, S.-J.; Won, Y.-G.; Choi, C.-H. Lateral release and medial plication for recurrent patella dislocation. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2438–2444. [Google Scholar] [CrossRef] [PubMed]
- Elkousy, H. Complications in Brief: Arthroscopic Lateral Release. Clin. Orthop. Relat. Res. 2012, 470, 2949–2953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vavken, P.; Wimmer, M.D.; Camathias, C.; Quidde, J.; Valderrabano, V.; Pagenstert, G. Treating Patella Instability in Skeletally Immature Patients. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1410–1422. [Google Scholar] [CrossRef] [PubMed]
- Dietvorst, M.; Reijman, M.; Van Groningen, B.; Van Der Steen, M.C.; Janssen, R. PROMs in paediatric knee ligament injury: Use the Pedi-IKDC and avoid using adult PROMs. Knee Surg. Sports Traumatol. Arthrosc. 2017, 27, 1965–1973. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, E.W.; Glaser, D.A. Adolescent Patella Instability Extensor Mechanics. J. Pediatr. Orthop. 2016, 36, 262–267. [Google Scholar] [CrossRef]
- Appel, H. Muscular atrophy following immobilisation. Sports Med. 1990, 10, 42–58. [Google Scholar] [CrossRef]
- van der Velden, C.A.; van der Steen, M.C.; Leenders, J.; Florens, Q.; van Douveren, M.P.; Janssen, R.P.; Reijman, M. Pedi-IKDC or KOOS-child: Which questionnaire should be used in children with knee disorders? BMC Musculoskelet. Disord. 2019, 20, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Singer, A.J.; Arora, B.; Dagum, A.; Valentine, S.; Hollander, J. Development and Validation of a Novel Scar Evalua-tion Score. Plast. Reconstr. Surg. 2007, 120, 1892–1897. [Google Scholar] [CrossRef]
- Schneider, D.K.; Grawe, B.; Magnussen, R.A.; Ceasar, A.; Parikh, S.N.; Wall, E.J.; Colosimo, A.J.; Kaeding, C.C.; Myer, G.D. Outcomes after isolated medial patellofemoral ligament recon-struction for the treatment of recurrent lateral patellar dislocations: A systematic review and meta-analysis. Am. J. Sports Med. 2016, 44, 2993–3005. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; Rizzello, G.; Ciuffreda, M.; Loppini, M.; Baldari, A.; Maffulli, N.; Denaro, V. Elmslie-Trillat, Maquet, Fulkerson, Roux Goldthwait, and Other Distal Realignment Procedures for the Management of Patellar Dislocation: Systematic Review and Quantitative Synthesis of the Literature. Arthrosc J. Arthrosc. Relat. 2016, 32, 929–943. [Google Scholar] [CrossRef]
- Nwachukwu, B.U.; So, C.; Schairer, W.; Green, D.W.; Dodwell, E. Surgical versus conservative management of acute patellar dislocation in children and adolescents: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 760–767. [Google Scholar] [CrossRef]
- Ostermeier, S.; Holst, M.; Hurschler, C.; Windhagen, H.; Stukenborg-Colsman, C. Dynamic measurement of patello-femoral kinematics and contact pressure after lateral retinacular. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 547–554. [Google Scholar] [CrossRef]
- Desio, S.M.; Burks, R.T.; Bachus, K.N. Soft Tissue Restraints to Lateral Patellar Translation in the Human Knee. Am. J. Sports Med. 1998, 26, 59–65. [Google Scholar] [CrossRef]
- Malatray, M.; Magnussen, R.; Lustig, S. and Servien, E. Lateral retinacular release is not recommended in association to MPFL reconstruction in recurrent patellar dislocation. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2659–2664. [Google Scholar] [CrossRef]
- McCarthy, M.A.; Bollier, M.J. Medial Patella Subluxation: Diagnosis and Treatment. Iowa Orthop. J. 2015, 35, 26–33. [Google Scholar] [PubMed]
- Studer, K.; Vacariu, A.; Rutz, E.; Camathias, C. High failure rate 10.8 years after vastus medialis transfer and lateral release (Green’s quadricepsplasty) for recurrent dislocation of the patella. Arch. Orthop. Trauma Surg. 2020, 140, 1349–1357. [Google Scholar]
- Apostolovic, M.; Vukomanovic, B.; Slavkovic, N.; Vuckovic, V.; Djuricic, G.; Kocev, N. Acute patellar dislocation in ado-lescents: Operative versus nonoperative treatment. Int. Orthopaedics. 2011, 35, 1483–1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisaccia, M.; Caraffa, A.; Meccariello, L.; Ripani, U.; Bisaccia, O.; Gomez-Garrido, D.; Carrado-Gomez, M.; Pace, V.; Rollo, G.; Giaracuni, M.; et al. Displaced patella fractures: Percutaneous cerclage wiring and second arthroscopic look. Clin. Cases Min. Bone Metab. 2019, 16, 48–52. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}
{kind=link}
{kind=link}


