
Socioeconomic Factors and Quality of Life Perceived by Parents and Children with Complex Chronic Conditions in Spain

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
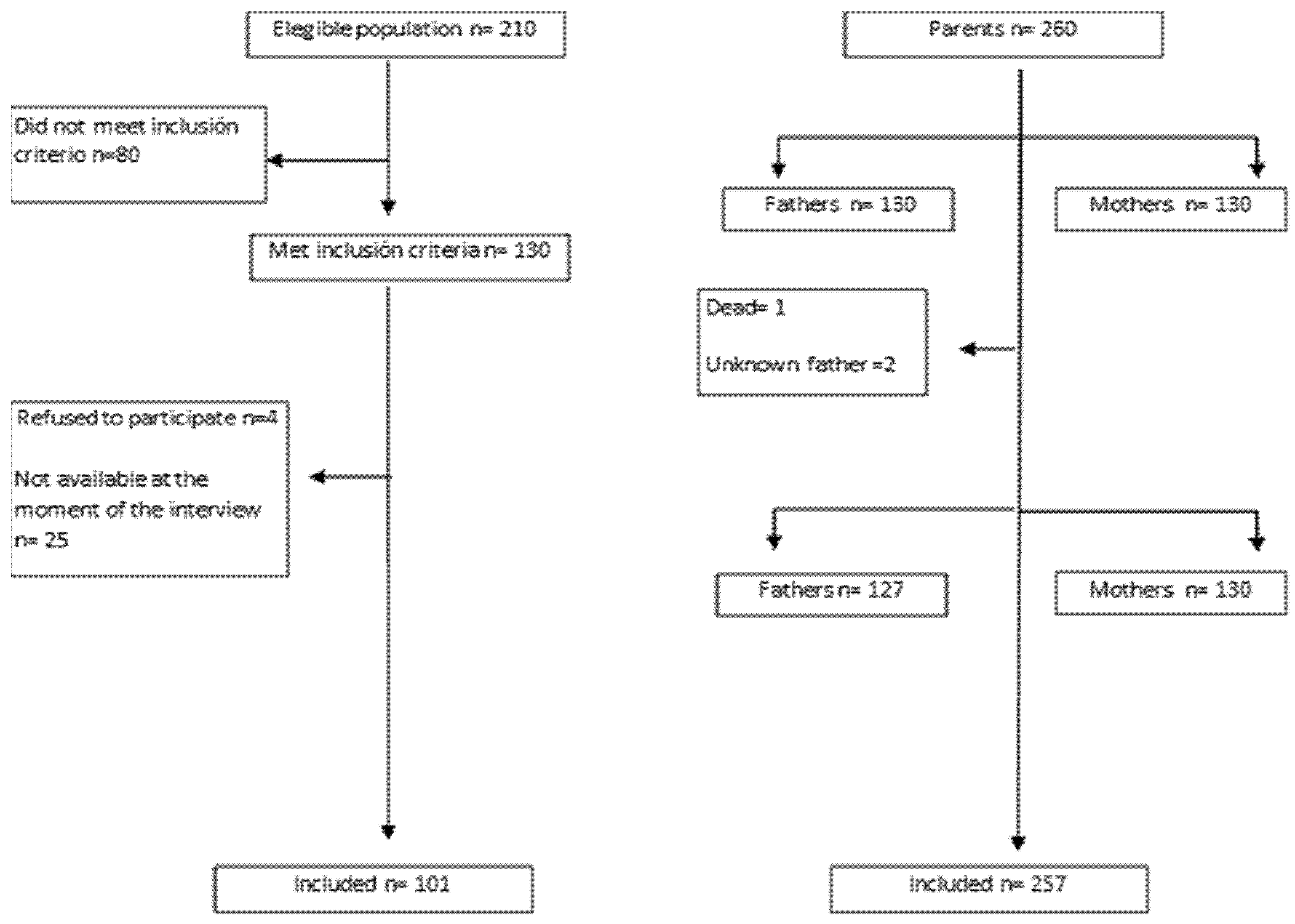
2.1. Study Design and Participants
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Demographics
3.2. Characteristics of the Participants
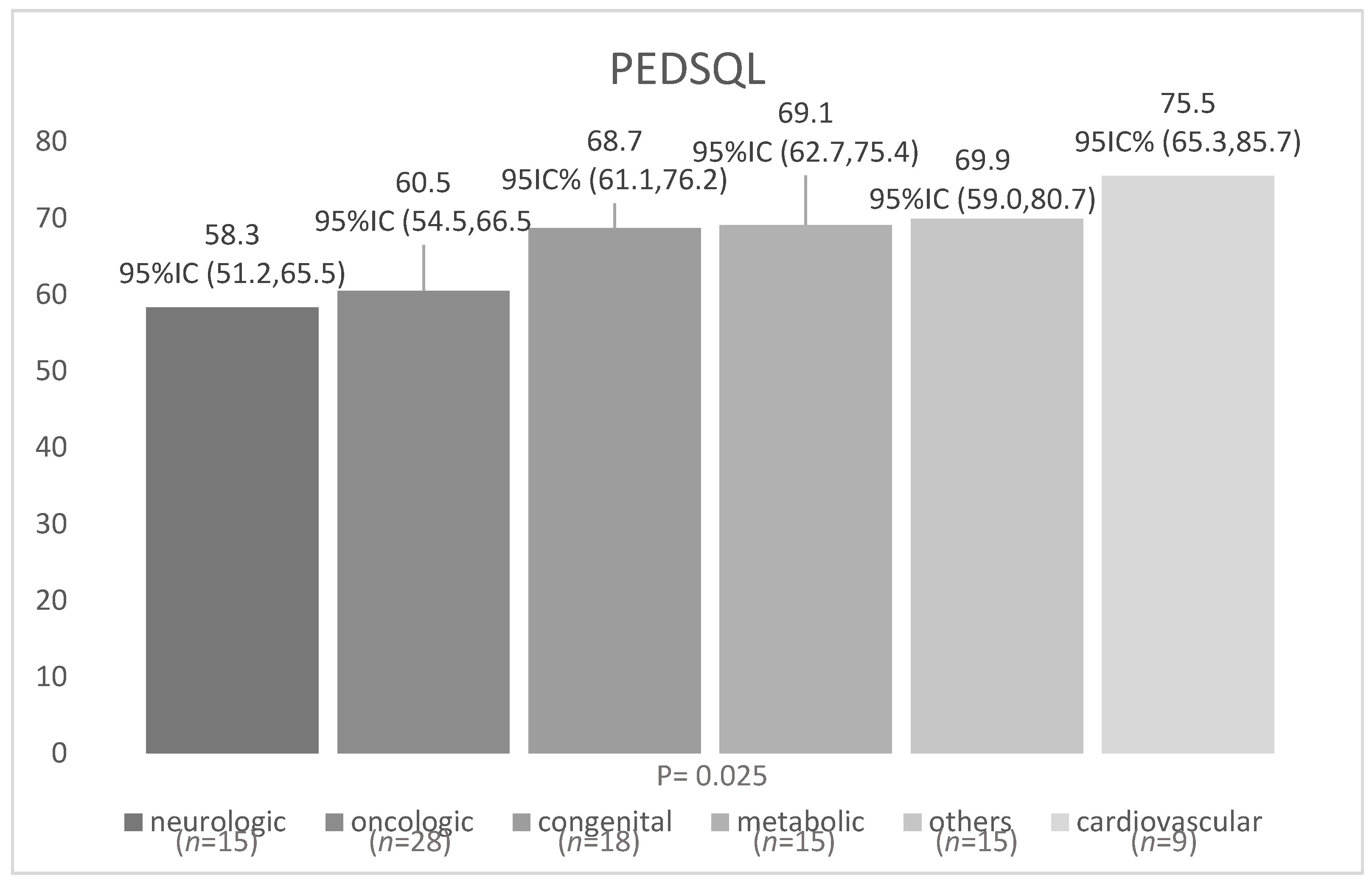
3.3. Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cohen, E.; Kuo, D.Z.; Agrawal, R.; Berry, J.G.; Bhagat, S.K.M.; Simon, T.D.; Srivastava, R. Children With Medical Complexity: An Emerging Population for Clinical and Research Initiatives. Pediatrics 2011, 127, 529–538. [Google Scholar] [CrossRef] [Green Version]
- Kuo, D.Z.; Melguizo-castro, M.; Goudie, A.; Nick, T.G.; Robbins, J.M.; Casey, P.H. Variation in Child Health Care Utilization by Medical Complexity. Matern. Child Health J. N. Y. 2015, 19, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Moore, D.; Sheetz, J. Pediatric Palliative Care Consultation. Pediatr. Clin. N. Am. 2014, 61, 735–747. [Google Scholar] [CrossRef]
- Berry, J.G.; Hall, M.; Neff, J.; Goodman, D.; Cohen, E.; Agrawal, R.; Kuo, D.; Feudtner, C. Children With Medical Complexity And Medicaid: Spending And Cost Savings. Health Aff. Chevy Chase 2014, 33, 2199–2206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, I.-C.; Shenkman, E.A.; Madden, V.L.; Vadaparampil, S.; Quinn, G.; Knapp, C.A. Measuring Quality of Life in Pediatric Palliative Care: Challenges and Potential Solutions. Palliat. Med. 2010, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varni; Limbers, C.A.; Burwinkle, T.M. Impaired Health-Related Quality of Life in Children and Adolescents with Chronic Conditions: A Comparative Analysis of 10 Disease Clusters and 33 Disease Categories/Severities Utilizing the PedsQLTM 4.0 Generic Core Scales. Health Qual. Life Outcomes 2007, 5, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellzey, A.; Valentine, K.J.; Hagedorn, C.; Murphy, N.A. Parent Perceptions of Quality of Life and Healthcare Satisfaction for Children with Medical Complexity. J. Pediatr. Rehabil. Med. 2015, 8, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Barthel, D.; Ravens-Sieberer, U.; Nolte, S.; Thyen, U.; Klein, M.; Walter, O.; Meyrose, A.-K.; Rose, M.; Otto, C. Predictors of Health-Related Quality of Life in Chronically Ill Children and Adolescents over Time. J. Psychosom. Res. 2018, 109, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Comisión Para Reducir Las Desigualdades Sociales En Salud En España. A proposal of policies and interventions to reduce social inequalities in health in Spain. Commission to Reduce Social Inequalities in Health in Spain. Gac Sanit 2012, 26, 182–189. [Google Scholar] [CrossRef] [Green Version]
- Rehm, R.S. Nursing’s Contribution to Research about Parenting Children with Complex Chronic Conditions: An Integrative Review, 2002 to 2012. Nurs. Outlook 2013, 61, 266–290. [Google Scholar] [CrossRef]
- Observatorio de la Infancia en Andalucía (OIA) Datos de Población Municipal 2015: Granada 2016. Available online: https://www.observatoriodelainfancia.es/oia/esp/index.aspx (accessed on 21 December 2016).
- Feudtner, C.; Christakis, D.A.; Connell, F.A. Pediatric Deaths Attributable to Complex Chronic Conditions: A Population-Based Study of Washington State, 1980–1997. Pediatrics 2000, 106, 205–209. [Google Scholar]
- González-Gil, T.; Mendoza-Soto, A.; Alonso-Lloret, F.; Castro-Murga, R.; Pose-Becerra, C.; Martín-Arribas, M.C. Versión Española Del Cuestionario de Calidad de Vida Para Niños y Adolescentes Con Cardiopatías (PedsQL TM). Rev. Española Cardiol. 2012, 65, 249–257. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Rode, C.A. The PedsQL: Measurement Model for the Pediatric Quality of Life Inventory. Med. Care 1999, 37, 126–139. [Google Scholar] [CrossRef]
- Domingo-Salvany, A.; Bacigalupe, A.; Carrasco, J.M.; Espelt, A.; Ferrando, J.; Borrell, C. Proposals for Social Class Classification Based on the Spanish National Classification of Occupations 2011 Using Neo-Weberian and Neo-Marxist Approaches. Gac. Sanit. 2013, 27, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Al-Gharib, R.M.; Abu-Saad Huijer, H.; Darwish, H. Quality of Care and Relationships as Reported by Children with Cancer and Their Parents. Ann. Palliat. Med. 2015, 4, 22–31. [Google Scholar]
- Jardine, J.; Glinianaia, S.V.; McConachie, H.; Embleton, N.D.; Rankin, J. Self-Reported Quality of Life of Young Children with Conditions from Early Infancy: A Systematic Review. Pediatrics 2014, 134, e1129–e1148. [Google Scholar] [CrossRef] [Green Version]
- Espartosa Larrayad, Marta; Martínez Serrano, Ana Estudio de La Calidad de Vida de Los Niños En Hemodialisis de La Comunidad de Madrid, En Comparación Con La Percibida Por Sus Padres. Cuid. Salud 2015, 12, 145–160.
- Lim, Y.; Velozo, C.; Bendixen, R.M. The Level of Agreement between Child Self-Reports and Parent Proxy-Reports of Health-Related Quality of Life in Boys with Duchenne Muscular Dystrophy. Qual. Life Res. 2014, 23, 1945–1952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Yang, H.-J.; Chen, V.C.-H.; Lee, W.-T.; Teng, M.-J.; Lin, C.-H.; Gossop, M. Meta-Analysis of Quality of Life in Children and Adolescents with ADHD: By Both Parent Proxy-Report and Child Self-Report Using PedsQLTM. Res. Dev. Disabil. 2016, 51–52, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Pardo-Guijarro, M.J.; Woll, B.; Moya-Martínez, P.; Martínez-Andrés, M.; Cortés-Ramírez, E.E.; Martínez-Vizcaíno, V. Validity and Reliability of the Spanish Sign Language Version of the KIDSCREEN-27 Health-Related Quality of Life Questionnaire for Use in Deaf Children and Adolescents. Gac. Sanit. 2013, 27, 318–324. [Google Scholar] [CrossRef] [Green Version]
- Santos, T.; de Matos, M.G.; Simões, C.; Leal, I.; do Céu Machado, M. (Health-Related) Quality of Life and Psychosocial Factors in Adolescents with Chronic Disease: A Systematic Literature Review. Int. J. Adolesc. Med. Health 2017. [Google Scholar] [CrossRef]
- Limbers, C.A.; Newman, D.A.; Varni, J.W. Factorial Invariance of Child Self-Report Across Healthy and Chronic Health Condition Groups: A Confirmatory Factor Analysis Utilizing the PedsQLTM 4.0 Generic Core Scales. J. Pediatr. Psychol. 2008, 33, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQLTM 4.0: Reliability and Validity of the Pediatric Quality of Life InventoryTM Version 4.0 Generic Core Scales in Healthy and Patient Populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef]
- Shaw, S.R.; McCabe, P.C. Hospital-to-School Transition for Children with Chronic Illness: Meeting the New Challenges of an Evolving Health Care System. Psychol. Sch. 2008, 45, 74–87. [Google Scholar] [CrossRef]
- Silva, N.; Pereira, M.; Otto, C.; Ravens-Sieberer, U.; Canavarro, M.C.; Bullinger, M. Do 8- to 18-Year-Old Children/Adolescents with Chronic Physical Health Conditions Have Worse Health-Related Quality of Life than Their Healthy Peers? A Meta-Analysis of Studies Using the KIDSCREEN Questionnaires. Qual. Life Res. 2019, 28, 1725–1750. [Google Scholar] [CrossRef]
- Pinquart, M. Health-Related Quality of Life of Young People with and Without Chronic Conditions. J. Pediatr. Psychol. 2020, 45, 780–792. [Google Scholar] [CrossRef]
- Raluy-Callado, M.; Chen, W.-H.; Whiteman, D.A.H.; Fang, J.; Wiklund, I. The Impact of Hunter Syndrome (Mucopolysaccharidosis Type II) on Health-Related Quality of Life. Orphanet J. Rare Dis. 2013, 8, 101. [Google Scholar] [CrossRef] [Green Version]
- Zan, H.; Scharff, R.L. The Heterogeneity in Financial and Time Burden of Caregiving to Children with Chronic Conditions. Matern. Child Health J. 2015, 19, 615–625. [Google Scholar] [CrossRef]
- Hope, S.; Pearce, A.; Whitehead, M.; Law, C. Effects of Child Long-Term Illness on Maternal Employment: Longitudinal Findings from the UK Millennium Cohort Study. Eur. J. Public Health 2017, 27, 48–52. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-Y.; Cisler, R. Assessing Health-Related Quality of Life Among Children With Special Health Care Needs in the United States. Child. Health Care 2011, 40, 311–325. [Google Scholar] [CrossRef]
- Mota, J.F.; Rezio, M.A.; Soares, R.C.; Pimentel, G.D.; Coelho, A.S.G.; Cunha, J. Quality of Life Is Influenced by Body Weight, Education, and Family Income in Adolescents with Chronic Diseases. Biomed. Res. Int. 2018, 2018, 8485103. [Google Scholar] [CrossRef] [Green Version]
- Didsbury, M.S.; Kim, S.; Medway, M.M.; Tong, A.; McTaggart, S.J.; Walker, A.M.; White, S.; Mackie, F.E.; Kara, T.; Craig, J.C.; et al. Socio-Economic Status and Quality of Life in Children with Chronic Disease: A Systematic Review. J. Paediatr. Child Health 2016, 52, 1062–1069. [Google Scholar] [CrossRef] [PubMed]
- Geyer, S.; Hemström, O.; Peter, R.; Vågerö, D. Education, Income, and Occupational Class Cannot Be Used Interchangeably in Social Epidemiology. Empirical Evidence against a Common Practice. J. Epidemiol. Community Health 2006, 60, 804–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, T.L.; Goodman, E.; The Committee on Pediatric Research. Race, Ethnicity, and Socioeconomic Status in Research on Child Health. Pediatrics 2015, 135, e225–e237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knapp, C.; Madden, V.; Revicki, D.; Feeny, D.; Wang, H.; Curtis, C.; Sloyer, P. Health Status and Health-Related Quality of Life in a Pediatric Palliative Care Program. J. Palliat. Med. 2012, 15, 790–797. [Google Scholar] [CrossRef]
- Shippee, N.D.; Shah, N.D.; May, C.R.; Mair, F.S.; Montori, V.M. Cumulative Complexity: A Functional, Patient-Centered Model of Patient Complexity Can Improve Research and Practice. J. Clin. Epidemiol. 2012, 65, 1041–1051. [Google Scholar] [CrossRef] [Green Version]
- Coad, J.; Kaur, J.; Ashley, N.; Owens, C.; Hunt, A.; Chambers, L.; Brown, E. Exploring the Perceived Met and Unmet Need of Life-Limited Children, Young People and Families. J. Pediatr. Nurs. 2015, 30, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Ravens-Sieberer, U.; Erhart, M.; Wille, N.; Wetzel, R.; Nickel, J.; Bullinger, M. Generic Health-Related Quality-of-Life Assessment in Children and Adolescents: Methodological Considerations. Pharmacoeconomics 2006, 24, 1199–1220. [Google Scholar] [CrossRef]
- García-Salido, A.; Santos-Herranz, P.; Puertas-Martín, V.; García-Teresa, M.Á.; Martino-Alba, R.; Serrano-González, A. Estudio retrospectivo de pacientes derivados de cuidados intensivos pediátricos a cuidados paliativos: Por qué y para qué. Pediatrics 2018, 88, 3–11. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Children | |||
|---|---|---|---|
| n = 101 | |||
| mean (SD) or n (%) | p | ||
| Age (years) mean (SD) | 10.5 (3.1) | ||
| Nationality, n (%) | |||
| Spanish | 91 (90.1) | ||
| Other | 10 (9.9) | ||
| Duration of the disease (years) mean (SD) | 6.1 (4.6) | ||
| Types of diseases, n (%) | |||
| Cardiovascular | 9 (8.9) | ||
| Respiratory | 1 (0.9) | ||
| Renal | 5 (4.9) | ||
| Gastrointestinal | 4 (3.9) | ||
| Hematologic or immunologic | 5 (4.9) | ||
| Metabolic | 15 (14.9) | ||
| Congenital or genetic | 18 (17.8) | ||
| Neurologic | 15 (14.9) | ||
| Oncologic or Malignancy | 29 (28.7) | ||
| Dispersion of health care resources, n (%) | 106 (59.6) | ||
| Referred from other provinces, n (%) | 37 (20.7) | ||
| Fathers n = 127 | Mothers n = 130 | ||
| Age (years) mean (SD) | 44.4 (6.7) | 41.5 (6.1) | |
| Education background, n (%) | |||
| No qualifications | 10 (7.7) | 7 (5.4) | (χ2 = 117.7) <0.001 |
| Primary education | 47 (36.2) | 45 (34.6) | |
| Secondary education | 43 (33.1) | 37 (28.5) | |
| University education | 27 (20.8) | 41 (31.5) | |
| Occupation, n (%) | |||
| Unemployed or retired | 23 (17.7) | 72 (55.4) | (χ2 = 72.2) <0.001 |
| Managerial | 17 (13.1) | 18 (13.8) | |
| Supervisory, intermediate level | 39 (30) | 24 (18.5) | |
| Unskilled | 46 (35.4) | 16 (12.3) | |
| Father (n = 130) | Mother (n = 130) | Children Comparison with Fathers (n = 101) † | Children Comparison with Mothers (n = 101) †† | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | 95%CI | p | Mean (SD) | 95%CI | p | Mean (SD) | 95%CI | p | Mean (SD) | 95%CI | p | |||||
| Overall PedsQL Score | Parents: 57.2 (17.5) | Children: 65.4 (15.8) | ||||||||||||||
| Educational level § | ||||||||||||||||
| No qualifications (n = 17) | 44.9 (16.9) | 32.8 | 57.0 | 0.015 | 49.7 (19.7) | 31.5 | 67.9 | 0.135 | 65.7 (12.1) | 54.4 | 76.9 | 0.466 | 67.4 (5.4) | 58.8 | 76.0 | 0.838 |
| Primary school (n = 92) | 54.7 (16.2) | 50.0 | 59.5 | 54.7 (17.0) | 49.6 | 59.7 | 62.0 (17.1) | 56.3 | 67.7 | 62.3 (18.1) | 57.0 | 69.7 | ||||
| Secondary school (n = 80) | 58.2 (19.0) | 52.3 | 64.0 | 56.2 (18.7) | 49.9 | 62.4 | 67.7 (14.6) | 62.7 | 72.9 | 66.4(14.1) | 61.2 | 71.7 | ||||
| University (n = 68) | 64.3 (15.5) | 58.1 | 70.4 | 62.1 (16.0) | 57.0 | 67.1 | 66.9 (17.6) | 58.7 | 75.2 | 66.3 (16.0) | 60.7 | 71.9 | ||||
| Occupation § | ||||||||||||||||
| Unemployed/retired (n = 95) | 47.9 (16.4) | 40.8 | 54.9 | 0.013 | 54.7 (19.1) | 50.2 | 59.2 | 0.084 | 63.4 (20.1) | 51.3 | 75.6 | 0.695 | 64.8 (17.2) | 60.1 | 69.4 | 0.940 |
| Managerial (n = 35) | 65.2 (13.2) | 58.4 | 72.0 | 66.4 (12.8) | 60.0 | 72.8 | 63.1 (16.2) | 52.2 | 74 | 67.9 (13.7) | 59.6 | 76.1 | ||||
| Intermediate (n = 63) | 59.5 (17.1) | 54.0 | 65.0 | 58.3 (15.8) | 51.6 | 65.0 | 68.1 (17.2) | 62.0 | 74.2 | 65.5 (17.2) | 58.8 | 72.2 | ||||
| Unqualified (n = 62) | 57.5 (18.7) | 52.0 | 63.0 | 55.8 (13.4) | 48.6 | 63.0 | 64.5 (14.0) | 60.0 | 69.0 | 65.2 (12.6) | 56.2 | 74.2 | ||||
| Psychosoc. PedsQL Score | Parents: 59 (16.7) | Children: 67 (15.2) | ||||||||||||||
| Educational level § | ||||||||||||||||
| No qualifications (n = 17) | 47.8 (18.0) | 34.9 | 60.7 | 0.002 | 52.4 (18.5) | 35.2 | 69.5 | 0.002 | 66.4 (11.1) | 56.2 | 76.6 | 0.442 | 69.2 (7.4) | 57.4 | 80.9 | 0.696 |
| Primary school (n = 92) | 55.8 (16.0) | 51.1 | 60.5 | 55.0 (16.2) | 50.1 | 59.9 | 63.4 (17.6) | 57.5 | 69.3 | 64.7 (17.5) | 58.5 | 70.8 | ||||
| Secondary school (n = 80) | 60.1 (17.3) | 54.8 | 65.5 | 58.3(18.7) | 52.0 | 64.5 | 68.9 (12.9) | 64.4 | 73.4 | 66.2 (14.3) | 60.9 | 71.6 | ||||
| University (n = 68) | 66.5 (14.3) | 60.8 | 72.2 | 65.1 (13.5) | 60.9 | 69.4 | 68.8 (16.8) | 61.0 | 76.7 | 69.0 (14.7) | 63.8 | 74.2 | ||||
| Occupation § | ||||||||||||||||
| Unemployed/retired (n = 95) | 46.1 (16.2) | 39.1 | 53.2 | <0.001 | 58.1 (18.2) | 53.8 | 62.4 | 0.106 | 61.8 (21.1) | 49.0 | 74.5 | 0.576 | 66.7 (16.5) | 62.2 | 71.2 | 0.756 |
| Managerial (n = 35) | 67.1 (11.7) | 61.1 | 73.2 | 66.8 (12.4) | 60.6 | 73.0 | 65.9 (15.5) | 55.5 | 76.3 | 69.7 (14.8) | 60.8 | 78.7 | ||||
| Intermediate (n = 63) | 59.6 (16.1) | 54.4 | 64.9 | 59.6 (15.0) | 53.2 | 65.9 | 69 (15.0) | 63.6 | 74.3 | 67.0 (12.0) | 61.8 | 72.2 | ||||
| Unqualified (n = 62) | 61.7 (16.8) | 56.7 | 66.7 | 53.2 (14.4) | 45.5 | 60.9 | 66.4 (14.4) | 61.7 | 71.1 | 62.7 (17.1) | 50.4 | 74.9 | ||||
| Physical PedsQL Score | Parents: 53.7 (27.6) | Children: 63.41 (23.5) | ||||||||||||||
| Educational level § | ||||||||||||||||
| No qualifications (n = 17) | 39.4 (27.8) | 19.5 | 59.2 | 0.260 | 44.6 (25.9) | 20.6 | 68.6 | 0.774 | 64.3 (26.9) | 39.4 | 89.1 | 0.621 | 64.1 (6.5) | 53.7 | 74.4 | 0.667 |
| Primary school (n = 92) | 52 (27.6) | 44 | 50 | 53.1 (28.8) | 44.5 | 61.7 | 58.2 (26) | 49.6 | 66.7 | 59.5 (28.3) | 49.8 | 69.3 | ||||
| Secondary school (n = 80) | 54.4 (29.3) | 45.4 | 63.4 | 52.2 (28.1) | 42.8 | 61.5 | 65.6 (23) | 57.6 | 73.6 | 66.7 (22.6) | 58.3 | 75.2 | ||||
| University (n = 68) | 59.5 (25.5) | 49.5 | 69.4 | 55.9 (26.9) | 47.5 | 64.3 | 63.4 (22.7) | 52.8 | 74.1 | 61.2 (21.6) | 53.5 | 68.9 | ||||
| Occupation § | ||||||||||||||||
| Unemployed/retired (n = 95) | 49.5 (29.6) | 36.9 | 62 | 0.235 | 48.4 (28.6) | 41.7 | 55.1 | 0.093 | 62.9 (29.5) | 45.9 | 80 | 0.696 | 61.2 (24.9) | 54.4 | 67.9 | 0.948 |
| Managerial (n = 35) | 60.4 (24.7) | 48.1 | 72.7 | 65.6 (22.2) | 54.6 | 76.6 | 57.9 (21.5) | 43.5 | 72.4 | 64.4 (17.5) | 53.8 | 75 | ||||
| Intermediate (n = 63) | 59.4 (26.3) | 50.8 | 67.9 | 55.4 (27.9) | 43.8 | 66.9 | 66.6 (25.4) | 57.5 | 75.6 | 62.7 (27) | 51.1 | 74.4 | ||||
| Unqualified (n = 62) | 49.5 (28.4) | 41.1 | 58 | 57.9 (25.1) | 45 | 70.8 | 61 (22.1) | 53.8 | 68.1 | 65.1 (21.8) | 50.4 | 79.7 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Ardanaz, B.; Peláez-Cantero, M.J.; Morales-Asencio, J.M.; Vellido-González, C.; Gómez-González, A.; León-Campos, Á.; Gutiérrez-Rodríguez, L. Socioeconomic Factors and Quality of Life Perceived by Parents and Children with Complex Chronic Conditions in Spain. Children 2021, 8, 931. https://doi.org/10.3390/children8100931
Pérez-Ardanaz B, Peláez-Cantero MJ, Morales-Asencio JM, Vellido-González C, Gómez-González A, León-Campos Á, Gutiérrez-Rodríguez L. Socioeconomic Factors and Quality of Life Perceived by Parents and Children with Complex Chronic Conditions in Spain. Children. 2021; 8(10):931. https://doi.org/10.3390/children8100931
Chicago/Turabian StylePérez-Ardanaz, Bibiana, María José Peláez-Cantero, José Miguel Morales-Asencio, Concepción Vellido-González, Alberto Gómez-González, Álvaro León-Campos, and Laura Gutiérrez-Rodríguez. 2021. "Socioeconomic Factors and Quality of Life Perceived by Parents and Children with Complex Chronic Conditions in Spain" Children 8, no. 10: 931. https://doi.org/10.3390/children8100931
APA StylePérez-Ardanaz, B., Peláez-Cantero, M. J., Morales-Asencio, J. M., Vellido-González, C., Gómez-González, A., León-Campos, Á., & Gutiérrez-Rodríguez, L. (2021). Socioeconomic Factors and Quality of Life Perceived by Parents and Children with Complex Chronic Conditions in Spain. Children, 8(10), 931. https://doi.org/10.3390/children8100931