
Association of Birth Weight with Central and Peripheral Corneal Thickness in Adulthood—Results from the Population-Based German Gutenberg Health Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Birth Weight
2.3. Ophthalmologic Examination
2.4. Scheimpflug Imaging
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
Non-Responder Analysis
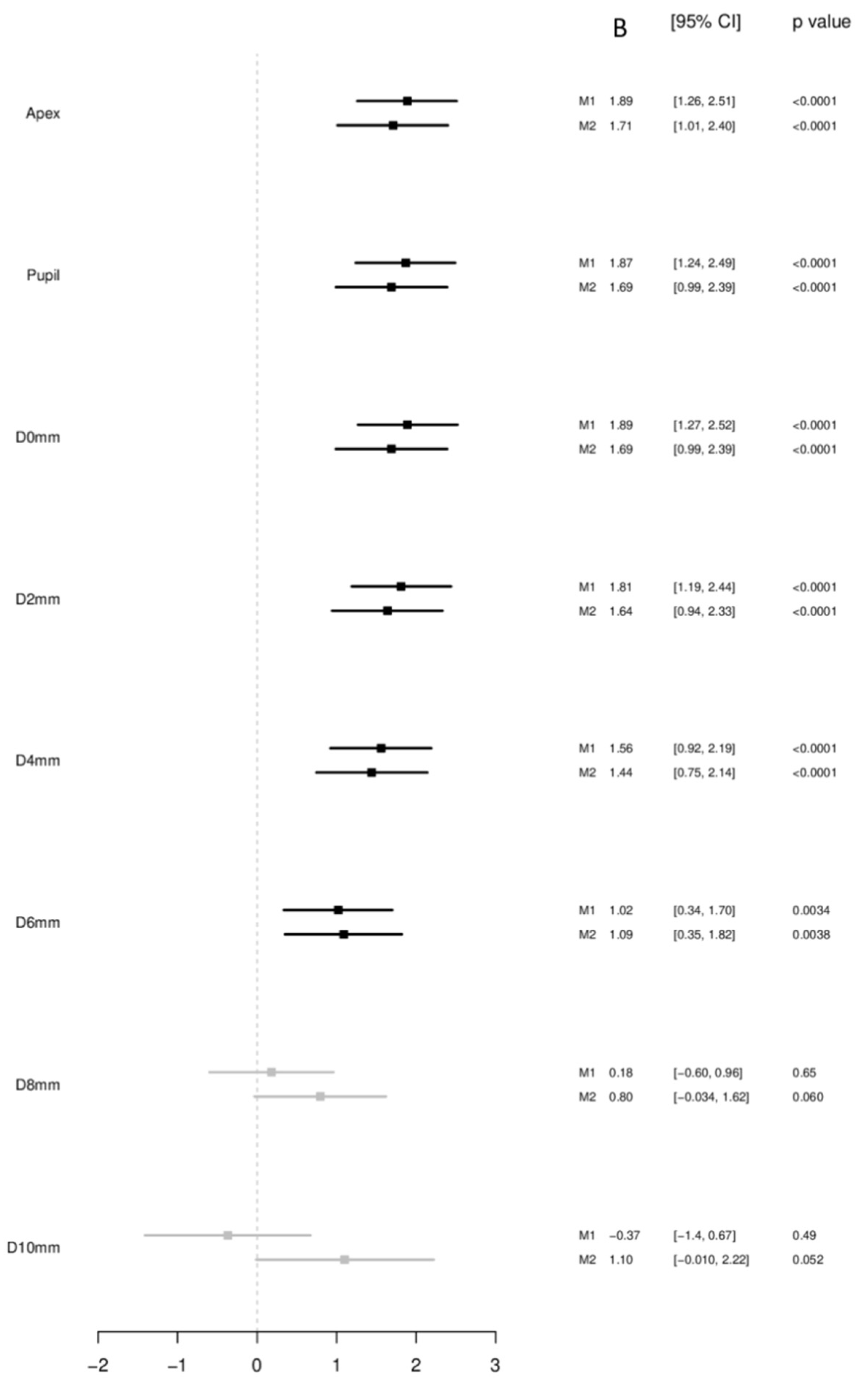
3.2. Birth Weight as a Continuous Variable
3.2.1. Corneal Thickness at the Corneal Apex and Pupil
3.2.2. Corneal Thickness Minimum and Periphery
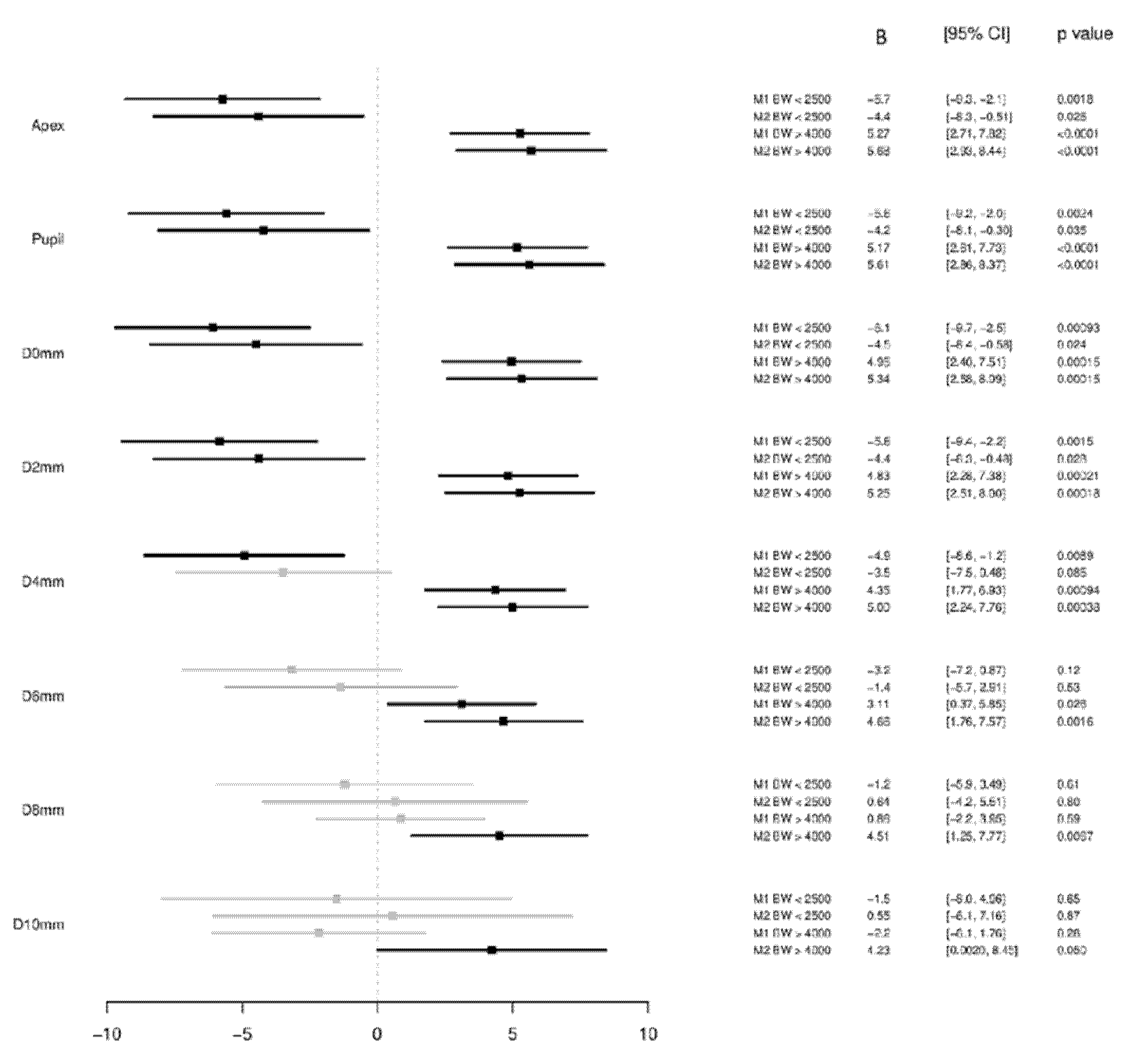
3.3. Birth Weight Categorized into Low, Normal and High Birth Weight
3.3.1. Corneal Thickness at the Corneal Apex and Pupil
3.3.2. Corneal Thickness Minimum and Periphery
4. Discussion
4.1. Strengths and Limitations
4.2. Summary
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kirwan, C.; O’Keefe, M.; Fitzsimon, S. Central corneal thickness and corneal diameter in premature infants. Acta Ophthalmol. Scand. 2005, 83, 751–753. [Google Scholar] [CrossRef] [PubMed]
- Autzen, T.; Bjornstrom, L. Central corneal thickness in premature babies. Acta Ophthalmol. 1991, 69, 251–252. [Google Scholar] [CrossRef]
- Kardaras, D.; Papageorgiou, E.; Gaitana, K.; Grivea, I.; Dimitriou, V.A.; Androudi, S.; Gounaris, A.; Tsironi, E.E. The Association Between Retinopathy of Prematurity and Ocular Growth. Investig. Ophthalmol. Vis. Sci. 2019, 60, 98–106. [Google Scholar] [CrossRef]
- Wu, W.C.; Lin, R.I.; Shih, C.P.; Wang, N.K.; Chen, Y.P.; Chao, A.N.; Chen, K.J.; Chen, T.L.; Hwang, Y.S.; Lai, C.C.; et al. Visual acuity, optical components, and macular abnormalities in patients with a history of retinopathy of prematurity. Ophthalmology 2012, 119, 1907–1916. [Google Scholar] [CrossRef]
- Fieß, A.; Kolb-Keerl, R.; Knuf, M.; Kirchhof, B.; Blecha, C.; Oberacher-Velten, I.; Muether, P.S.; Bauer, J. Axial Length and Anterior Segment Alterations in Former Preterm Infants and Full-Term Neonates Analyzed With Scheimpflug Imaging. Cornea 2017, 36, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Cook, A.; White, S.; Batterbury, M.; Clark, D. Ocular growth and refractive error development in premature infants with or without retinopathy of prematurity. Investig. Ophthalmol. Vis. Sci. 2008, 49, 5199–5207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fieß, A.; Schuster, A.K.; Pfeiffer, N.; Nickels, S. Association of birth weight with corneal power in early adolescence: Results from the National Health and Nutrition Examination Survey (NHANES) 1999–2008. PLoS ONE 2017, 12, e0186723. [Google Scholar] [CrossRef] [PubMed]
- Ojaimi, E.; Robaei, D.; Rochtchina, E.; Rose, K.A.; Morgan, I.G.; Mitchell, P. Impact of birth parameters on eye size in a population-based study of 6-year-old Australian children. Am. J. Ophthalmol. 2005, 140, 535–537. [Google Scholar] [CrossRef] [PubMed]
- Fieß, A.; Schuster, A.K.; Nickels, S.; Urschitz, M.S.; Elflein, H.M.; Schulz, A.; Munzel, T.; Wild, P.S.; Beutel, M.E.; Schmidtmann, I.; et al. Association of Low Birth Weight with Altered Corneal Geometry and Axial Length in Adulthood in the German Gutenberg Health Study. JAMA Ophthalmol. 2019, 137, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Jethani, J.; Shah, K.; Jethani, M. Evaluating the change in central corneal thickness in neonates (term and preterm) in Indian population and the factors affecting it. Indian J. Ophthalmol. 2015, 63, 501–503. [Google Scholar] [CrossRef] [PubMed]
- Acar, D.E.; Acar, U.; Tunay, Z.O.; Ozdemir, O.; Dolgun, A.; Erdurmus, M. The intraocular pressure and central corneal thickness in healthy premature infants. J. Am. Assoc. Pediatric Ophthalmol. Strabismus 2015, 19, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Gunay, M.; Celik, G.; Gunay, B.O.; Dogru, M.; Gursoy, T.; Ovali, H.F. Central corneal thickness measurements in premature infants. Int. J. Ophthalmol. 2014, 7, 496–500. [Google Scholar] [CrossRef]
- Kıvanç, S.A.; Akova Budak, B.; Olcaysü, O.O. Association of Birth Parameters with Corneal Thickness in Prematurely Born and Full-Term School-Aged Children. Cornea 2016, 35, 634–637. [Google Scholar] [CrossRef] [PubMed]
- Yeter, V.; Aritürk, N.; Bİrİncİ, H.; Süllü, Y.; Güngör, İ. Effects of Birth Weight on Anterior Segment Measurements in Full-Term Children Without Low Birth Weight by Dual-Scheimpflug Analyzer. Am. J. Ophthalmol. 2015, 160, 832–840. [Google Scholar] [CrossRef]
- Pan, C.-W.; Qian, Y.-X.; Zhong, H.; Li, J.; Liu, H.; Chen, Q. Central Corneal Thickness and Its Association with Birth Parameters in Chinese Adolescents. Ophthalmic Epidemiol. 2019, 26, 360–366. [Google Scholar] [CrossRef]
- Fledelius, H.C. Ophthalmic changes from age of 10 to 18 years. A longitudinal study of sequels to low birth weight. III. Ultrasound oculometry and keratometry of anterior eye segment. Acta Ophthalmol. 1982, 60, 393–402. [Google Scholar] [CrossRef]
- Ho, T.; Cheng, A.C.; Rao, S.K.; Lau, S.; Leung, C.K.; Lam, D.S. Central corneal thickness measurements using Orbscan II, Visante, ultrasound, and Pentacam pachymetry after laser in situ keratomileusis for myopia. J. Cataract Refract. Surg. 2007, 33, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Lam, A.K. Intrasession and intersession repeatability of the Pentacam system on posterior corneal assessment in the normal human eye. J. Cataract Refract. Surg. 2007, 33, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Ecsedy, M.; Kovacs, I.; Mihaltz, K.; Recsan, Z.; Szigeti, A.; Juhasz, E.; Nemeth, J.; Nagy, Z.Z. Scheimpflug imaging for long-term evaluation of optical components in Hungarian children with a history of preterm birth. J. Pediatric Ophthalmol. Strabismus 2014, 51, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Marques, S.N.; Barros, R.S.; Miranda, F.A.; Cardoso, N.J.; Parreira, S.; Fonseca, T.; Donaire, M.N.; Campos, N. Scheimpflug Imaging for Evaluation of Optical Components in Portuguese Children with history of preterm birth. Oftalmologia 2016, 40, 139–144. [Google Scholar]
- Hoffmann, E.M.; Lamparter, J.; Mirshahi, A.; Elflein, H.; Hoehn, R.; Wolfram, C.; Lorenz, K.; Adler, M.; Wild, P.S.; Schulz, A.; et al. Distribution of central corneal thickness and its association with ocular parameters in a large central European cohort: The Gutenberg health study. PLoS ONE 2013, 8, e66158. [Google Scholar] [CrossRef]
- Wild, P.S.; Zeller, T.; Beutel, M.; Blettner, M.; Dugi, K.A.; Lackner, K.J.; Pfeiffer, N.; Munzel, T.; Blankenberg, S. The Gutenberg Health Study. Bundesgesundheitsblatt Gesundh. Gesundh. 2012, 55, 824–829. [Google Scholar] [CrossRef]
- Fieß, A.; Elbaz, H.; Korb, C.A.; Nickels, S.; Schulz, A.; Münzel, T.; Wild, P.S.; Beutel, M.E.; Schmidtmann, I.; Lackner, K.J.; et al. Low Birth Weight Is Linked to Age-Related Macular Degeneration: Results From the Population-Based Gutenberg Health Study (GHS). Investig. Ophthalmol. Vis. Sci. 2019, 60, 4943–4950. [Google Scholar] [CrossRef] [Green Version]
- Fieß, A.; Schuster, A.K.; Nickels, S.; Elflein, H.M.; Schulz, A.; Beutel, M.E.; Blettner, M.; Pfeiffer, N. Association of low birth weight with myopic refractive error and lower visual acuity in adulthood: Results from the population-based Gutenberg Health Study (GHS). Br. J. Ophthalmol. 2019, 103, 99–105. [Google Scholar] [CrossRef]
- Fieß, A.; Elflein, H.M.; Urschitz, M.S.; Pesudovs, K.; Münzel, T.; Wild, P.S.; Michal, M.; Lackner, K.J.; Pfeiffer, N.; Nickels, S.; et al. Prevalence of Strabismus and Its Impact on Vision-Related Quality of Life: Results from the German Population-Based Gutenberg Health Study. Ophthalmology 2020, 127, 1113–1122. [Google Scholar] [CrossRef]
- German Federal Statistical Office. Bevölkerung und Erwerbstätigkeit, Bevölkerungsbewegung. 1972–1980. (accessed on 7 May 2020).
- Hohn, R.; Kottler, U.; Peto, T.; Blettner, M.; Munzel, T.; Blankenberg, S.; Lackner, K.J.; Beutel, M.; Wild, P.S.; Pfeiffer, N. The ophthalmic branch of the Gutenberg Health Study: Study design, cohort profile and self-reported diseases. PLoS ONE 2015, 10, e0120476. [Google Scholar] [CrossRef] [Green Version]
- Elflein, H.M.; Pfeiffer, N.; Hoffmann, E.M.; Hoehn, R.; Kottler, U.; Lorenz, K.; Zwiener, I.; Wild, P.S.; Mirshahi, A. Correlations between central corneal thickness and general anthropometric characteristics and cardiovascular parameters in a large European cohort from the Gutenberg Health Study. Cornea 2014, 33, 359–365. [Google Scholar] [CrossRef]
- Wong, T.T.; Wong, T.Y.; Foster, P.J.; Crowston, J.G.; Fong, C.W.; Aung, T. The relationship of intraocular pressure with age, systolic blood pressure, and central corneal thickness in an asian population. Investig. Ophthalmol. Vis. Sci. 2009, 50, 4097–4102. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2016. [Google Scholar]
- Gordon-Shaag, A.; Millodot, M.; Kaiserman, I.; Sela, T.; Barnett Itzhaki, G.; Zerbib, Y.; Matityahu, E.; Shkedi, S.; Miroshnichenko, S.; Shneor, E. Risk factors for keratoconus in Israel: A case-control study. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. 2015, 35, 673–681. [Google Scholar] [CrossRef]
- Remón, L.; Cristóbal, J.A.; Castillo, J.; Palomar, T.; Palomar, A.; Pérez, J. Central and peripheral corneal thickness in full-term newborns by ultrasonic pachymetry. Investig. Ophthalmol. Vis. Sci. 1992, 33, 3080–3083. [Google Scholar]
- Ehlers, N.; Sorensen, T.; Bramsen, T.; Poulsen, E.H. Central corneal thickness in newborns and children. Acta Ophthalmol 1976, 54, 285–290. [Google Scholar] [CrossRef]
- Uva, M.G.; Reibaldi, M.; Longo, A.; Avitabile, T.; Gagliano, C.; Scollo, D.; Lionetti, E.; Reibaldi, A. Intraocular pressure and central corneal thickness in premature and full-term newborns. J. Am. Assoc. Pediatric Ophthalmol. Strabismus 2011, 15, 367–369. [Google Scholar] [CrossRef]
- Portellinha, W.; Belfort, R., Jr. Central and peripheral corneal thickness in newborns. Acta Ophthalmol. 1991, 69, 247–250. [Google Scholar] [CrossRef]
- Al-Umran, K.U.; Pandolfi, M.F. Corneal diameter in premature infants. Br. J. Ophthalmol. 1992, 76, 292–293. [Google Scholar] [CrossRef] [Green Version]
- Fielder, A.R.; Levene, M.I.; Russell-Eggitt, I.M.; Weale, R.A. Temperature--a factor in ocular development? Dev. Med. Child Neurol. 1986, 28, 279–284. [Google Scholar] [CrossRef]
- Nangia, V.; Jonas, J.B.; Sinha, A.; Matin, A.; Kulkarni, M. Central corneal thickness and its association with ocular and general parameters in Indians: The Central India Eye and Medical Study. Ophthalmology 2010, 117, 705–710. [Google Scholar] [CrossRef]
- Nemesure, B.; Wu, S.Y.; Hennis, A.; Leske, M.C. Corneal thickness and intraocular pressure in the Barbados eye studies. Arch. Ophthalmol. 2003, 121, 240–244. [Google Scholar] [CrossRef]
- Tomidokoro, A.; Araie, M.; Iwase, A. Corneal thickness and relating factors in a population-based study in Japan: The Tajimi study. Am. J. Ophthalmol. 2007, 144, 152–154. [Google Scholar] [CrossRef]
- Dai, E.; Gunderson, C.A. Pediatric central corneal thickness variation among major ethnic populations. J. Am. Assoc. Pediatric Ophthalmol. Strabismus 2006, 10, 22–25. [Google Scholar] [CrossRef]
- Pfeiffer, N.; Torri, V.; Miglior, S.; Zeyen, T.; Adamsons, I.; Cunha-Vaz, J. Central corneal thickness in the European Glaucoma Prevention Study. Ophthalmology 2007, 114, 454–459. [Google Scholar] [CrossRef]
- Vijaya, L.; George, R.; Arvind, H.; Ve Ramesh, S.; Baskaran, M.; Raju, P.; Asokan, R.; Velumuri, L. Central corneal thickness in adult South Indians: The Chennai Glaucoma Study. Ophthalmology 2010, 117, 700–704. [Google Scholar] [CrossRef]
- Kawase, K.; Tomidokoro, A.; Araie, M.; Iwase, A.; Yamamoto, T. Ocular and systemic factors related to intraocular pressure in Japanese adults: The Tajimi study. Br. J. Ophthalmol. 2008, 92, 1175–1179. [Google Scholar] [CrossRef]
- Rochtchina, E.; Mitchell, P.; Wang, J.J. Relationship between age and intraocular pressure: The Blue Mountains Eye Study. Clin. Exp. Ophthalmol. 2002, 30, 173–175. [Google Scholar] [CrossRef]
- Zhang, H.; Xu, L.; Chen, C.; Jonas, J.B. Central corneal thickness in adult Chinese. Association with ocular and general parameters. The Beijing Eye Study. Graefe Arch. Clin. Exp. Ophthalmol. 2008, 246, 587–592. [Google Scholar] [CrossRef]
- Fieß, A.; Marx-Groß, S.; Wasielica-Poslednik, J.; Nagler, M.; Schmidtmann, I.; Wild, P.S.; Münzel, T.; Beutel, M.E.; Lackner, K.J.; Pfeiffer, N.; et al. Peripheral corneal thickness and associated factors—Results from the population-based German Gutenberg Health Study. Acta Ophthalmol. 2021. in production. [Google Scholar] [CrossRef]
- Fieß, A.; Ponto, K.A.; Urschitz, M.S.; Nickels, S.; Schulz, A.; Münzel, T.; Wild, P.S.; Beutel, M.E.; Lackner, K.J.; Pfeiffer, N.; et al. Birthweight and its association with retinal vessel equivalents—Results from the population-based German Gutenberg Health Study. Acta Ophthalmol. 2021, 99, e773–e774. [Google Scholar] [CrossRef]
- Fieß, A.; Schuster, A.K.; Kölb-Keerl, R.; Knuf, M.; Kirchhof, B.; Muether, P.S.; Bauer, J. Corneal Aberrations in Former Preterm Infants: Results from The Wiesbaden Prematurity Study. Investig. Ophthalmol. Vis. Science. 2017, 58, 6374–6378. [Google Scholar] [CrossRef] [Green Version]
- Fieß, A.; Janz, J.; Schuster, A.K.; Kölb-Keerl, R.; Knuf, M.; Kirchhof, B.; Muether, P.S.; Bauer, J. Macular morphology in former preterm and full-term infants aged 4 to 10 years. Graefe Arch. Clin. Exp. Ophthalmol. 2017, 255, 1433–1442. [Google Scholar] [CrossRef]
- Fieß, A.; Christian, L.; Kölb-Keerl, R.; Knuf, M.; Kirchhof, B.; Muether, P.S.; Bauer, J. Peripapillary Choroidal Thickness in Former Preterm and Full-Term Infants Aged From 4 to 10 Years. Investig. Ophthalmol. Vis. Sci. 2016, 57, 6548–6553. [Google Scholar] [CrossRef] [Green Version]
- Fieß, A.; Christian, L.; Janz, J.; Kölb-Keerl, R.; Knuf, M.; Kirchhof, B.; Muether, P.S.; Bauer, J. Prematurity Eye Study Group. Functional analysis and associated factors of the peripapillary retinal nerve fibre layer in former preterm and full-term infants. Br. J. Ophthalmol. 2017, 101, 1405–1411. [Google Scholar] [CrossRef]
- Sun, C.; Ponsonby, A.L.; Brown, S.A.; Kearns, L.S.; Mackinnon, J.R.; Barbour, J.M.; Ruddle, J.B.; Hewitt, A.W.; Wright, M.J.; Martin, N.G.; et al. Associations of birth weight with ocular biometry, refraction, and glaucomatous endophenotypes: The Australian Twins Eye Study. Am. J. Ophthalmol. 2010, 150, 909–916. [Google Scholar] [CrossRef]
- Grewal, D.S.; Brar, G.S.; Grewal, S.P. Assessment of central corneal thickness in normal, keratoconus, and post-laser in situ keratomileusis eyes using Scheimpflug imaging, spectral domain optical coherence tomography, and ultrasound pachymetry. J. Cataract Refract. Surg. 2010, 36, 954–964. [Google Scholar] [CrossRef]
- Barkana, Y.; Gerber, Y.; Elbaz, U.; Schwartz, S.; Ken-Dror, G.; Avni, I.; Zadok, D. Central corneal thickness measurement with the Pentacam Scheimpflug system, optical low-coherence reflectometry pachymeter, and ultrasound pachymetry. J. Cataract Refract. Surg. 2005, 31, 1729–1735. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | Male | Female |
|---|---|---|---|
| Participants (n) | 5657 | 2638 | 3019 |
| Sex (Women) | 53.4% (3019) | 0% (0) | 100% (3019) |
| Age (y) | 56.0 ± 10.3 | 56.1 ± 10.3 | 56.0 ± 10.3 |
| Height (cm) | 171 ± 10 | 178 ± 7 | 164 ± 7 |
| Weight (kg) | 79.9 ± 17.2 | 88.7 ± 14.7 | 72.1 ± ^5.3 |
| BMI | 26.5 (23.7/30.0) | 27.2 (24.9/30.2) | 25.6 (22.7/29.7) |
| Socioeconomic status (score) | 13.78 ± 4.26 | 14.55 ± 4.22 | 13.11 ± 4.18 |
| Birth weight (g) | 3395 ± 648 | 3530 ± 650 | 3277 ± 623 |
| Cardiovascular parameters | |||
| Hypertension (yes) | 46.6% (2632) | 53.1% (1401) | 40.8% (1231) |
| Diabetes (yes) | 7.4% (421) | 9.7% (255) | 5.5% (166) |
| Dyslipidemia (yes) | 29.6% (1673) | 37.9% (997) | 22.4% (676) |
| Smoker (yes) | 16.7% (942) | 17.3% (457) | 16.1% (485) |
| Ocular disease: | |||
| Self-reported glaucoma (yes) | 3.1% (176) | 3.1% (77) | 3.2% (99) |
| Self-reported AMD (yes) | 1.3% (71) | 1.0% (27) | 1.5% (44) |
| Ocular parameters: | |||
| Visual acuity OD (logMAR) | 0.10 (0/0.20) | 0 (0/0.10) | 0.10 (0/0.20) |
| Visual acuity OS (logMAR) | 0.00 (0/0.10) | 0 (0/0.10) | 0 (0/0.10) |
| Spherical equivalent OD (diopter) | −0.25 (−1.50/0.62) | −0.25 (−1.50/0.62) | −0.25 (−1.50/0.75) |
| Spherical equivalent OS (diopter) | −0.25 (−1.50/0.62) | −0.25 (−1.50/0.62) | −0.25 (−1.50/0.75) |
| Intraocular pressure OD (mmHg) | 14.73 ± 2.96 | 14.89 ± 3.11 | 14.59 ± 2.81 |
| Intraocular pressure OS (mmHg) | 14.80 ± 2.95 | 14.99 ± 3.06 | 14.65 ± 2.84 |
| Mean corneal radius OD (mm) | 7.77 ± 0.28 | 7.84 ± 0.28 | 7.70 ± 0.26 |
| Mean corneal radius OS (mm) | 7.77 ± 0.28 | 7.84 ± 0.28 | 7.71 ± 0.26 |
| White-to-white OD (mm) | 12.2 ± 0.4 | 12.3 ± 0.4 | 12.1 ± 0.4 |
| White-to-white OS (mm) | 12.2 ± 0.4 | 12.3 ± 0.4 | 12.2 ± 0.4 |
| Axial length OD (mm) | 23.8 ± 1.3 | 24.1 ± 1.3 | 23.5 ± 1.3 |
| Axial length OS (mm) | 23.8 ± 1.3 | 24.1 ± 1.3 | 23.5 ± 1.2 |
| Variable in µm | <2.5 kg (315) | 2.5–4.0 kg (4655) | >4.0 kg (687) | p Value |
|---|---|---|---|---|
| Corneal thickness | ||||
| Apex OD | 552 ± 32 | 558 ± 32 | 563 ± 32 | <0.001 |
| Apex OS | 553 ± 32 | 558 ± 33 | 564 ± 32 | <0.001 |
| Pupil OD | 551 ± 32 | 556 ± 32 | 561 ± 32 | <0.001 |
| Pupil OS | 551 ± 32 | 557 ± 33 | 562 ± 32 | <0.001 |
| Corneal thickness in circles | ||||
| around corneal thickness minimum | ||||
| D 0 mm OD | 546 ± 32 | 552 ± 33 | 557 ± 32 | <0.001 |
| D 0 mm OS | 546 ± 32 | 552 ± 33 | 557 ± 33 | <0.001 |
| D 2 mm OD | 555 ± 32 | 561 ± 32 | 566 ± 32 | <0.001 |
| D 2 mm OS | 555 ± 32 | 561 ± 33 | 566 ± 33 | <0.001 |
| D 4 mm OD | 583 ± 33 | 588 ± 33 | 592 ± 33 | <0.001 |
| D 4 mm OS | 583 ± 33 | 588 ± 33 | 592 ± 33 | <0.001 |
| D 6 mm OD | 627 ± 37 | 630 ± 35 | 633 ± 35 | 0.013 |
| D 6 mm OS | 627 ± 36 | 630 ± 35 | 633 ± 35 | 0.007 |
| D 8 mm OD | 690 ± 42 | 692 ± 40 | 692 ± 39 | 0.54 |
| D 8 mm OS | 691 ± 42 | 692 ± 40 | 693 ± 39 | 0.36 |
| D 10 mm OD | 776 ± 54 | 777 ± 51 | 774 ± 47 | 0.58 |
| D 10 mm OS | 777 ± 53 | 778 ± 50 | 776 ± 48 | 0.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fieß, A.; Urschitz, M.S.; Marx-Groß, S.; Nagler, M.; Wild, P.S.; Münzel, T.; Beutel, M.E.; Lackner, K.J.; Pfeiffer, N.; Schuster, A.K. Association of Birth Weight with Central and Peripheral Corneal Thickness in Adulthood—Results from the Population-Based German Gutenberg Health Study. Children 2021, 8, 1006. https://doi.org/10.3390/children8111006
Fieß A, Urschitz MS, Marx-Groß S, Nagler M, Wild PS, Münzel T, Beutel ME, Lackner KJ, Pfeiffer N, Schuster AK. Association of Birth Weight with Central and Peripheral Corneal Thickness in Adulthood—Results from the Population-Based German Gutenberg Health Study. Children. 2021; 8(11):1006. https://doi.org/10.3390/children8111006
Chicago/Turabian StyleFieß, Achim, Michael S. Urschitz, Susanne Marx-Groß, Markus Nagler, Philipp S. Wild, Thomas Münzel, Manfred E. Beutel, Karl J. Lackner, Norbert Pfeiffer, and Alexander K. Schuster. 2021. "Association of Birth Weight with Central and Peripheral Corneal Thickness in Adulthood—Results from the Population-Based German Gutenberg Health Study" Children 8, no. 11: 1006. https://doi.org/10.3390/children8111006
APA StyleFieß, A., Urschitz, M. S., Marx-Groß, S., Nagler, M., Wild, P. S., Münzel, T., Beutel, M. E., Lackner, K. J., Pfeiffer, N., & Schuster, A. K. (2021). Association of Birth Weight with Central and Peripheral Corneal Thickness in Adulthood—Results from the Population-Based German Gutenberg Health Study. Children, 8(11), 1006. https://doi.org/10.3390/children8111006