
The Role of Occupational Therapy in Managing Food Selectivity of Children with Autism Spectrum Disorder: A Scoping Review

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
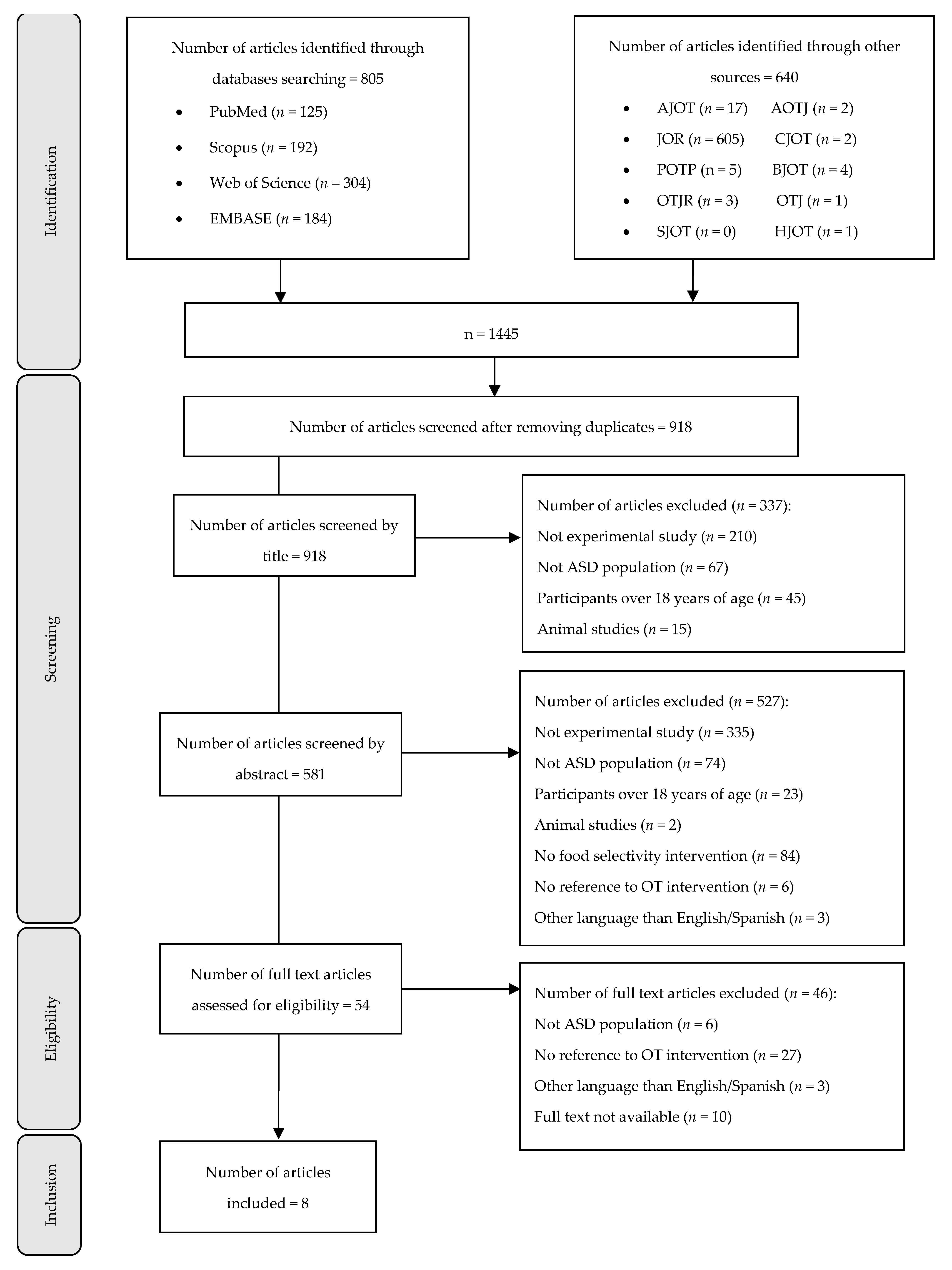
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
3. Results
3.1. Main Characteristics and Limitations of Included Studies
3.2. Interventions Including OT in Picky Eating
3.2.1. Sensory–Behavioral Interventions
3.2.2. Family-Focused Interventions
3.2.3. Other Interventions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chistol, L.T.; Bandini, L.G.; Must, A.; Phillips, S.; Cermak, S.A.; Curtin, C. Sensory Sensitivity and Food Selectivity in Children with Autism Spectrum Disorder. J. Autism. Dev. Disord. 2018, 48, 583–591. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Paraphilic Disorders. Diagnostic and Statistical Manual of Mental Disorders; American Psychology Association: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- Chiarotti, F.; Venerosi, A. Epidemiology of Autism Spectrum Disorders: A Review of Worldwide Prevalence Estimates Since 2014. Brain Sci. 2020, 10, 274. [Google Scholar] [CrossRef]
- Trastornos del Espectro Autista. Available online: https://www.who.int/es/news-room/fact-sheets/detail/autism-spectrum-disorders (accessed on 23 July 2021).
- Elsabbagh, M.; Divan, G.; Koh, Y.-J.; Kim, Y.S.; Kauchali, S.; Marcín, C.; Montiel-Nava, C.; Patel, V.; Paula, C.S.; Wang, C.; et al. Global Prevalence of Autism and Other Pervasive Developmental Disorders. Autism Res. 2012, 5, 160–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaaf, R.C.; Toth-Cohen, S.; Johnson, S.L.; Outten, G.; Benevides, T.W. The Everyday Routines of Families of Children with Autism: Examining the Impact of Sensory Processing Difficulties on the Family. Autism 2011, 15, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Lockner, D.W.; Crowe, T.K.; Skipper, B.J. Dietary Intake and Parents’ Perception of Mealtime Behaviors in Preschool-Age Children with Autism Spectrum Disorder and in Typically Developing Children. J Am. Diet. Assoc. 2008, 108, 1360–1363. [Google Scholar] [CrossRef]
- Patel, M.D.; Donovan, S.M.; Lee, S.-Y. Considering Nature and Nurture in the Etiology and Prevention of Picky Eating: A Narrative Review. Nutrients 2020, 12, 3409. [Google Scholar] [CrossRef]
- Cermak, S.A.; Curtin, C.; Bandini, L.G. Food Selectivity and Sensory Sensitivity in Children with Autism Spectrum Disorders. J. Am. Diet. Assoc. 2010, 110, 238–246. [Google Scholar] [CrossRef] [Green Version]
- Tanner, K.; Case-Smith, J.; Nahikian-Nelms, M.; Ratliff-Schaub, K.; Spees, C.; Darragh, A.R. Behavioral and Physiological Factors Associated With Selective Eating in Children With Autism Spectrum Disorder. Am. J. Occup. Ther. 2015, 69, 6906180030p1–6906180030p8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerwing, M.; Eicher, P.; Gelsinger, J. Parental Report of Eating Problems and Gastrointestinal Symptoms in Children With Pervasive Developmental Disorders. Child. Health Care 2010, 34, 217–234. [Google Scholar] [CrossRef]
- Williams, P.G.; Dalrymple, N.; Neal, J. Eating Habits of Children with Autism. Pediatr. Nurs. 2000, 26, 259–264. [Google Scholar] [PubMed]
- Bicer, A.H.; Alsaffar, A.A. Body Mass Index, Dietary Intake and Feeding Problems of Turkish Children with Autism Spectrum Disorder (ASD). Res. Dev. Disabil. 2013, 34, 3978–3987. [Google Scholar] [CrossRef] [PubMed]
- Viviers, M.; Jongh, M.; Dickonson, L.; Malan, R.; Pike, T. Parent-Reported Feeding and Swallowing Difficulties of Children with Autism Spectrum Disorders (Aged 3 to 5 Years) Compared to Typically Developing Peers: A South African Study. Afr. Health Sci. 2020, 20, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Brzóska, A.; Kazek, B.; Kozioł, K.; Kapinos-Gorczyca, A.; Ferlewicz, M.; Babraj, A.; Makosz-Raczek, A.; Likus, W.; Paprocka, J.; Matusik, P.; et al. Eating Behaviors of Children with Autism—Pilot Study. Nutrients 2021, 13, 2687. [Google Scholar] [CrossRef] [PubMed]
- Margari, L.; Marzulli, L.; Gabellone, A.; de Giambattista, C. Eating and Mealtime Behaviors in Patients with Autism Spectrum Disorder: Current Perspectives. Neuropsychiatr. Dis. Treat. 2020, 16, 2083–2102. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.L.; Vander Schaaf, E.B.; Cohen, G.M.; Irby, M.B.; Skelton, J.A. Association of Picky Eating and Food Neophobia with Weight: A Systematic Review. Child. Obes. 2016, 12, 247–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhi, P.; Saini, S.; Bharti, B.; Attri, S.; Sankhyan, N. Sensory Processing Dysfunction and Mealtime Behavior Problems in Children With Autism. Indian Pediatr. 2021, 58, 842–845. [Google Scholar] [CrossRef] [PubMed]
- Barnhill, K.; Gutierrez, A.; Ghossainy, M.; Marediya, Z.; Devlin, M.; Sachdev, P.; Marti, C.N.; Hewitson, L. Dietary Status and Nutrient Intake of Children with Autism Spectrum Disorder: A Case-Control Study. Res. Autism Spectr. Disord. 2018, 50, 51–59. [Google Scholar] [CrossRef]
- Piwowarczyk, A.; Horvath, A.; Pisula, E.; Kawa, R.; Szajewska, H. Gluten-Free Diet in Children with Autism Spectrum Disorders: A Randomized, Controlled, Single-Blinded Trial. J. Autism Dev. Disord. 2020, 50, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Boquin, M.M.; Moskowitz, H.R.; Donovan, S.M.; Lee, S.-Y. Defining Perceptions of Picky Eating Obtained through Focus Groups and Conjoint Analysis. J. Sens. Stud. 2014, 29, 126–138. [Google Scholar] [CrossRef]
- Curtin, C.; Hubbard, K.; Anderson, S.E.; Mick, E.; Must, A.; Bandini, L.G. Food Selectivity, Mealtime Behavior Problems, Spousal Stress, and Family Food Choices in Children with and without Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 3308–3315. [Google Scholar] [CrossRef] [Green Version]
- Postorino, V.; Sanges, V.; Giovagnoli, G.; Fatta, L.M.; De Peppo, L.; Armando, M.; Vicari, S.; Mazzone, L. Clinical Differences in Children with Autism Spectrum Disorder with and without Food Selectivity. Appetite 2015, 92, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.L.; Farrow, C.; Haycraft, E.; Meyer, C. Parental Influences on Children’s Eating Behaviour and Characteristics of Successful Parent-Focussed Interventions. Appetite 2013, 60, 85–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, B.K.; Wolery, M.; Kaiser, A.P. Treatment of Food Selectivity in a Young Child with Autism. Focus Autism Other Dev. Disabil. 2009, 24, 169–177. [Google Scholar] [CrossRef]
- Penrod, B.; Gardella, L.; Fernand, J. An evaluation of a progressive high-probability instructional sequence combined with low-probability demand fading in the treatment of food selectivity. J. Appl. Behav. Anal. 2012, 45, 527–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizzo, B.; Coyle, M.; Seiverling, L.; Williams, K. Plate A–Plate B: Use of Sequential Presentation in the Treatment of Food Selectivity. Behav. Interv. 2012, 27, 175–184. [Google Scholar] [CrossRef]
- Valdimarsdóttir, H.; Halldórsdóttir, L.Ý.; SigurÐardóttir, Z.G. Increasing the variety of foods consumed by a picky eater: Generalization of effects across caregivers and settings. J. Appl. Behav. Anal. 2010, 43, 101–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najdowski, A.C.; Tarbox, J.; Wilke, A.E. Utilizing Antecedent Manipulations and Reinforcement in the Treatment of Food Selectivity by Texture. Educ. Treat. Child. 2012, 35, 101–110. [Google Scholar] [CrossRef]
- Paul, C.; Williams, K.E.; Riegel, K.; Gibbons, B. Combining Repeated Taste Exposure and Escape Prevention: An Intervention for the Treatment of Extreme Food Selectivity. Appetite 2007, 49, 708–711. [Google Scholar] [CrossRef] [PubMed]
- Miyajima, A.; Tateyama, K.; Fuji, S.; Nakaoka, K.; Hirao, K.; Higaki, K. Development of an Intervention Programme for Selective Eating in Children with Autism Spectrum Disorder. Hong Kong J. Occup. Ther. 2017, 30, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Pender, R.; Fearon, P.; Heron, J.; Mandy, W. The Longitudinal Heterogeneity of Autistic Traits: A Systematic Review. Res. Autism Spectr. Disord. 2020, 79, 101671. [Google Scholar] [CrossRef]
- Ozonoff, S.; Gangi, D.; Hanzel, E.P.; Hill, A.; Hill, M.M.; Miller, M.; Schwichtenberg, A.J.; Steinfeld, M.B.; Parikh, C.; Iosif, A.-M. Onset Patterns in Autism: Variation across Informants, Methods, and Timing. Autism Res. 2018, 11, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Manual Cochrane de revisiones sistemáticas de intervenciones. Cochrane Collab. 2011, 1, 639. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook/current (accessed on 11 February 2021).
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping Studies: Advancing the Methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A Scoping Review on the Conduct and Reporting of Scoping Reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.; Godfrey, C.; McInerney, P.; Munn, Z.; Trico, A.; Khalil, H. Chapter 11: Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; Joanna Briggs Institute (JBI): Adelaide, Australia, 2020; ISBN 978-0-648-84880-6. [Google Scholar]
- Peterson, K.M.; Piazza, C.C.; Volkert, V.M. A Comparison of a Modified Sequential Oral Sensory Approach to an Applied Behavior-Analytic Approach in the Treatment of Food Selectivity in Children with Autism Spectrum Disorder. J. Appl. Behav. Anal. 2016, 49, 485–511. [Google Scholar] [CrossRef]
- Kuschner, E.S.; Morton, H.E.; Maddox, B.B.; de Marchena, A.; Anthony, L.G.; Reaven, J. The BUFFET Program: Development of a Cognitive Behavioral Treatment for Selective Eating in Youth with Autism Spectrum Disorder. Clin. Child. Fam. Psychol. Rev. 2017, 20, 403–421. [Google Scholar] [CrossRef]
- Sharp, W.G.; Jaquess, D.L. Bite Size and Texture Assessments to Prescribe Treatment for Severe Food Selectivity in Autism. Behav. Interv. 2009, 24, 157–170. [Google Scholar] [CrossRef]
- Suarez, M.A. Multicomponent Treatment for Food Selectivity in Children: Description and Case Report. Nutr. Clin. Pract. 2015, 30, 425–431. [Google Scholar] [CrossRef]
- Whipple, H.; Scherr, R.; Kozlowski, A.M. Simultaneous Presentation to Decrease Packing in a Child With a Feeding Disorder. Behav. Anal. Pract. 2020, 13, 197–204. [Google Scholar] [CrossRef]
- Seiverling, L.; Anderson, K.; Rogan, C.; Alaimo, C.; Argott, P.; Panora, J. A Comparison of a Behavioral Feeding Intervention With and Without Pre-Meal Sensory Integration Therapy. J. Autism Dev. Disord. 2018, 48, 3344–3353. [Google Scholar] [CrossRef] [PubMed]
- Cosbey, J.; Muldoon, D. EAT-UP™ Family-Centered Feeding Intervention to Promote Food Acceptance and Decrease Challenging Behaviors: A Single-Case Experimental Design Replicated Across Three Families of Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2017, 47, 564–578. [Google Scholar] [CrossRef] [PubMed]
- Kumazaki, H.; Sumioka, H.; Muramatsu, T.; Yoshikawa, Y.; Shimaya, J.; Iwanaga, R.; Ishiguro, H.; Sumiyoshi, T.; Mimura, M. Brief Report: The Effectiveness of Hugging a Huggable Device Before Having a Conversation with an Unfamiliar Person for Autism Spectrum Disorders. J. Autism Dev. Disord. 2021. [Google Scholar] [CrossRef]
- Scheerer, N.; Curcin, K.; Stojanoski, B.; Anagnostou, E.; Nicolson, R.; Kelley, E.; Georgiades, S.; Liu, X.; Stevenson, R. Exploring Sensory Phenotypes in Autism Spectrum Disorder. Mol. Autism 2021, 12, 67. [Google Scholar] [CrossRef]
- Taylor, C.M.; Emmett, P.M. Picky Eating in Children: Causes and Consequences. Proc. Nutr. Soc. 2019, 78, 161–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, C.G.; Haszard, J.J.; Taylor, R.W.; Heath, A.-L.M.; Taylor, B.; Campbell, K.J. Parental Feeding Practices Associated with Children’s Eating and Weight: What Are Parents of Toddlers and Preschool Children Doing? Appetite 2018, 128, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Thullen, M.; Bonsall, A. Co-Parenting Quality, Parenting Stress, and Feeding Challenges in Families with a Child Diagnosed with Autism Spectrum Disorder. J. Autism Dev. Disord. 2017, 47, 878–886. [Google Scholar] [CrossRef]
- Wyse, R.; Campbell, E.; Nathan, N.; Wolfenden, L. Associations between Characteristics of the Home Food Environment and Fruit and Vegetable Intake in Preschool Children: A Cross-Sectional Study. BMC Public Health 2011, 11, 938. [Google Scholar] [CrossRef] [Green Version]
- Machado, B.C.; Dias, P.; Lima, V.S.; Campos, J.; Gonçalves, S. Prevalence and Correlates of Picky Eating in Preschool-Aged Children: A Population-Based Study. Eat. Behav. 2016, 22, 16–21. [Google Scholar] [CrossRef]
- Hafstad, G.S.; Abebe, D.S.; Torgersen, L.; von Soest, T. Picky Eating in Preschool Children: The Predictive Role of the Child’s Temperament and Mother’s Negative Affectivity. Eat. Behav. 2013, 14, 274–277. [Google Scholar] [CrossRef]
- Lepinioti, M.; Specht, I.O.; Rohde, J.F.; Stougaard, M.; Händel, M.N.; Olsen, N.J.; Heitmann, B.L. Associations between Child Mental Well-Being or Conflicts during Mealtime and Picky Eating Behaviour. Int J. Environ. Res. Public Health 2021, 18, 5621. [Google Scholar] [CrossRef]
- Harris, H.A.; Micali, N.; Moll, H.A.; van Berckelaer-Onnes, I.; Hillegers, M.; Jansen, P.W. The Role of Food Selectivity in the Association between Child Autistic Traits and Constipation. Int. J. Eat. Disord. 2021, 54, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Pliner, P.; Loewen, E.R. Temperament and Food Neophobia in Children and Their Mothers. Appetite 1997, 28, 239–254. [Google Scholar] [CrossRef]
- Dovey, T.M.; Staples, P.A.; Gibson, E.L.; Halford, J.C.G. Food Neophobia and “picky/Fussy” Eating in Children: A Review. Appetite 2008, 50, 181–193. [Google Scholar] [CrossRef]
- Chatoor, I. Feeding Disorders in Infants and Toddlers: Diagnosis and Treatment. Child. Adolesc. Psychiatr. Clin. N. Am. 2002, 11, 163–183. [Google Scholar] [CrossRef]
- Aswathy, A.K.; Manoharan, A.; Manoharan, A. Addressing Oral Sensory Issues and Possible Remediation in Children with Autism Spectrum Disorders: Illustrated with a Case Study. Int. Sch. Sci. Res. Innov. 2016, 10, 400–403. [Google Scholar]
- Farrow, C.V.; Coulthard, H. Relationships between Sensory Sensitivity, Anxiety and Selective Eating in Children. Appetite 2012, 58, 842–846. [Google Scholar] [CrossRef] [Green Version]
- Rylatt, L.; Cartwright, T. Parental Feeding Behaviour and Motivations Regarding Pre-School Age Children: A Thematic Synthesis of Qualitative Studies. Appetite 2016, 99, 285–297. [Google Scholar] [CrossRef]
- Nadon, G.; Feldman, D.; Dunn, W.; Gisel, E. Mealtime Problems in Children with Autism Spectrum Disorder and Their Typically Developing Siblings: A Comparison Study. Autism Int. J. Res. Pract. 2011, 15, 98–113. [Google Scholar] [CrossRef]
- Panjwani, A.A.; Bailey, R.L.; Kelleher, B.L. COVID-19 and Behaviors in Children with Autism Spectrum Disorder: Disparities by Income and Food Security Status. Res. Dev. Disabil. 2021, 115, 104002. [Google Scholar] [CrossRef] [PubMed]
- Hayter, A.K.M.; Draper, A.K.; Ohly, H.R.; Rees, G.A.; Pettinger, C.; McGlone, P.; Watt, R.G. A Qualitative Study Exploring Parental Accounts of Feeding Pre-School Children in Two Low-Income Populations in the UK. Matern. Child. Nutr. 2015, 11, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Angell, A. Selective Eaters and Tactile Sensitivity: A Review of Classification and Treatment Methods That Address Anxiety and Support a Child’s Need for a Sense of Control. ICAN Infant Child. Adolesc. Nutr. 2010, 2, 299–303. [Google Scholar] [CrossRef]
- Levine, A.; Bachar, L.; Tsangen, Z.; Mizrachi, A.; Levy, A.; Dalal, I.; Kornfeld, L.; Levy, Y.; Zadik, Z.; Turner, D.; et al. Screening Criteria for Diagnosis of Infantile Feeding Disorders as a Cause of Poor Feeding or Food Refusal. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 563–568. [Google Scholar] [CrossRef]
- Zeedyk, S.M.; Cohen, S.R.; Eisenhower, A.; Blacher, J. Perceived Social Competence and Loneliness Among Young Children with ASD: Child, Parent and Teacher Reports. J. Autism Dev. Disord. 2016, 46, 436–449. [Google Scholar] [CrossRef]
- Stolar, O.; Zachor, D.A.; Ben-Itzchak, E. Food Selectivity Is Associated with More Severe Autism Symptoms in Toddlers with Autism Spectrum Disorder. Acta Paediatr. 2021, 110, 1–3. [Google Scholar] [CrossRef]
- Brown, T.; Gutman, S.A.; Ho, Y.-S.; Fong, K.N.K. A Bibliometric Analysis of Occupational Therapy Publications. Scand. J. Occup. Ther. 2018, 25, 1–14. [Google Scholar] [CrossRef]
- Dallman, A.R.; Artis, J.; Watson, L.; Wright, S. Systematic Review of Disparities and Differences in the Access and Use of Allied Health Services Amongst Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2021, 51, 1316–1330. [Google Scholar] [CrossRef]


{kind=link}
| Author, Country, Year | Design | Sample (n), Age | Evaluation | Main Results | Limitations |
|---|---|---|---|---|---|
| Seiverling et al., USA, 2018 [46] | Case series | 2, 5–6 years | Baseline, pre-, post-int, 8-w f-u | - Increase in the grams of foods and drinks consumed without inappropriate behaviors in both participants after the interventions (p-value NS). | Carry-over effect, lack of f-u, lack of information on the development of the treatment. |
| Peterson et al., USA, 2015 [41] | Parallel RCT | 6, 4–6 years | Baseline, pre-, post-int | - Increase in food consumption in children who received ABA therapy, but not for children who received the M-SOS (p-value NS). | No continuous training of parents in M-SOS therapy, food presentation not typical for M-SOS, lack of f-u. |
| Sharp and Jaquess., USA, 2009 [43] | Case report | 1, 3 years | Pre-, post-int | - Improvement in the acceptance of all bites and textures, with no expulsions or gagging (p-values NS). | NS |
| Miyajima et al., Japan, 2017 [31] | nRCT | 23, 3–6 years | Baseline, pre-, post-int | - Increase in the number of food items consumed by children (p < 0.001), in parents’ degree of self-efficacy (p < 0.018), and in the number of recommendations conducted by parents (p < 0.001) - Decrease in subjective view of children’s dietary imbalance (p < 0.001). | Difficulty in assessing dietary selectivity, difficulties for parents to follow dietary recommendations. |
| Cosbey and Muldoon., Mexico, 2016 [47] | Case series | 3, 6–8 years | Pre-, post-int | - Decrease in the child’s challenging mealtime behaviors and increased food acceptance (p-value NS). | Low generalizability of the results, small sample size, limited duration of the intervention. |
| Suarez., USA, 2014 [44] | Case report | 1, 8 years | Each w of int. | - Increase in food acceptance (p-value NS). | Small sample size, low effectiveness for severe food selectivity, lack of nutritional status assessment. |
| Whipple et al., USA, 2019 [45] | Case report | 1, 4 years | Baseline, pre-int, 4-w f-u | - Decrease in packing and meal duration (p-values NS). | Difficulty in eliminating preferred products, small sample size. |
| Kuschner et al., USA, 2017 [42] | Open pilot trial | 11, 8–12 years | Pre-,post-int,4- and 12-w f-u | - High satisfaction with the intervention (p-value NS) and high rate of parents reported that the intervention helps to reduce selective feeding (88%). | No control group, small sample size, low generalizability of the results. |
| Author, Country, Year | Eating Problem | Intervention | Interventions Description | Duration (w) | Sessions | Measuring Instruments | Occupational Therapist’s Role |
|---|---|---|---|---|---|---|---|
| Seiverling et al., USA, 2018 [46] | Food selectivity, especially with liquids or pureed foods | Behavioral dietary intervention without and with SI therapy | CG: Behavioral feeding intervention without SI. Experimenters alternated between presenting a mouthful of food and a drink. IG: Behavioral feeding intervention with SI. CG intervention + SI activities before each meal (proprioceptive and tactile input). | 1–2 | 8–15 sessions. Four daily 20 min sessions. | - IMB assessed through the observation of video recording. - Food intake assessed through the number of foods consumed it is was consumed within 10 s after presentation. - Total intake was assessed through the comparison of pre- and post-food weight. | Evaluation, activity development and training of experimenters in the implementation of sensory integration activities. MT: psychologists, feeding therapists, occupational therapists. |
| Peterson et al., USA, 2015 [41] | Food selectivity | ABA and M-SOS | CG: M-SOS. A 6-step hierarchy food presentation, which included visual tolerance, interaction, smell, taste, and eating. IG: ABA. A sequential bites presentation of a single target food (such as broccoli) every 30s until the presentation of five bites. | NS | 1,5 h session. Number and frequency of sessions NS. | - IMB assessed through the observation of video recording. - Total grams of food consumed assessed through the observation of video recording. - Acceptance assessed through the observation of video recording. - Mouth clean assessed through the observation of video recording. | Checking the integrity of the treatment. MT: Therapists and occupational therapists. |
| Sharp and Jaquess., USA, 2009 [43] | Food selectivity and food rejection | Day treatment program through texture reduction | 16 foods were initially presented at pureed texture using a 2-pea bite size. During sessions, both texture and bite size were gradually increased. | 4 | 4 daily 30- to 45 min meals/sessions. Number of sessions NS. | - Mouth clean assessed through observation. - IMB assessed through observation. - Expulsions assessed through observation. - Gagging assessed through observation. | Assessment and treatment to increase oral motor skills. MT: psychologists, dietitians, and occupational therapists. |
| Miyajima et al., Japan, 2017 [31] | Food selectivity | Intervention for parents based on the person–environment–occupation model. | Seminars for parents of children with ASD. The intervention helped parents learn about selective eating and, therefore, improve their children’s care. | 8 | 2 sessions and two discussions. One-monthly 40 min sessions. | - Degree of difficulty experienced by parents assessed through a VAS. - Degree of parents’ self-efficacy assessed through the SAPS. - Number of recommendations implemented by parents assessed through a 50 items questionnaire. - Changes in the eating patterns of children with ASD assessed through the number of foods that the children chose to eat (47 items) and the parents’ subjective view of the degree of dietary imbalance (VAS). | Interviewing and counseling parents on how to address concerns. No MT. |
| Cosbey and Muldoon., Mexico, 2016 [47] | Food selectivity and inappropriate behavior | Family centered food intervention EAT-UP | Phase 1 “coaching intervention”: sessions with coaching and feedback, such as visual supports. Phase 2 “stand-alone intervention”: sessions with only feedback. | 20 | Number of sessions varied between participants (5–21 sessions). Duration of sessions NS | - Children’s food acceptance and dietary diversity were assessed through the use of a Food Frequency Questionnaire and a 24 h food recall. - Children’s mealtime behaviors assessed through the BAMBI and the BPFAS. | Intervention. No MT. |
| Suarez., USA, 2014 [44] | Food selectivity | Multicomponent treatment | A combination of sensory integration, systematic desensitization, behavior modification, positive reinforcement, extinction of escape and parent and home education. | 40 | 22 sessions. 1-weekly session. Duration of sessions NS | - Children’s food consumption assessed through a food inventory. - Children’s sensory processing difficulties assessed through the SSP. | Intervention. No MT. |
| Whipple et al., USA, 2019 [45] | Food selectivity, packing and inappropriate behaviors | Simultaneous presentation | Simultaneous presentation of preferred and non-preferred foods on the spoon. | NS | 50 sessions. Three—to four—weekly 45 min sessions. | - Packing frequency assessed through the observation of video recording. - IMB assessed through the observation of video recording. - Expulsions assessed through the observation of video recording. - Meal duration assessed through the observation of video recording. | Oral motor skills assessment. MT: Trained therapists and occupational therapists. |
| Kuschner et al., USA, 2017 [42] | Food selectivity | BUFFET cognitive–behavioral treatment (food flexibility and exposure treatment program) | Multifamily intervention. Children were helped to develop strategies to act flexibly with new or non-preferred foods. | 16 | 14 sessions. One-weekly 90 min sessions. | - Acceptability of BUFFET assessed through session attendance, and individual session ratings. - Global parent satisfaction assessed through the CSQ-8 | Development of the intervention program. MT: Trained research assistants, doctoral- or masters-level clinicians, and occupational therapists. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reche-Olmedo, L.; Torres-Collado, L.; Compañ-Gabucio, L.M.; Garcia-de-la-Hera, M. The Role of Occupational Therapy in Managing Food Selectivity of Children with Autism Spectrum Disorder: A Scoping Review. Children 2021, 8, 1024. https://doi.org/10.3390/children8111024
Reche-Olmedo L, Torres-Collado L, Compañ-Gabucio LM, Garcia-de-la-Hera M. The Role of Occupational Therapy in Managing Food Selectivity of Children with Autism Spectrum Disorder: A Scoping Review. Children. 2021; 8(11):1024. https://doi.org/10.3390/children8111024
Chicago/Turabian StyleReche-Olmedo, Laura, Laura Torres-Collado, Laura María Compañ-Gabucio, and Manuela Garcia-de-la-Hera. 2021. "The Role of Occupational Therapy in Managing Food Selectivity of Children with Autism Spectrum Disorder: A Scoping Review" Children 8, no. 11: 1024. https://doi.org/10.3390/children8111024
APA StyleReche-Olmedo, L., Torres-Collado, L., Compañ-Gabucio, L. M., & Garcia-de-la-Hera, M. (2021). The Role of Occupational Therapy in Managing Food Selectivity of Children with Autism Spectrum Disorder: A Scoping Review. Children, 8(11), 1024. https://doi.org/10.3390/children8111024