
The Neurobehavioral Phenotype of School-Aged, Very Prematurely Born Children with No Serious Neurological Sequelae: A Quality of Life Predictor

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Method
2.1. Study Design and Population
2.2. Measurements Collected from the GPQOL Study Data
2.2.1. Clinical and Sociodemographic Data
2.2.2. Psychometric and Behavioral Evaluation Data (7–10 Years Old)
2.2.3. Quality of Life Data
2.2.4. Disability and Specific Cognitive Impairment Definition in the GPQoL Study
2.3. Ethics
2.4. Statistical Analysis
2.4.1. Descriptive Analysis
2.4.2. New Classification of Cognitive/Behavioral Impairments
2.4.3. QoL Analysis
3. Results
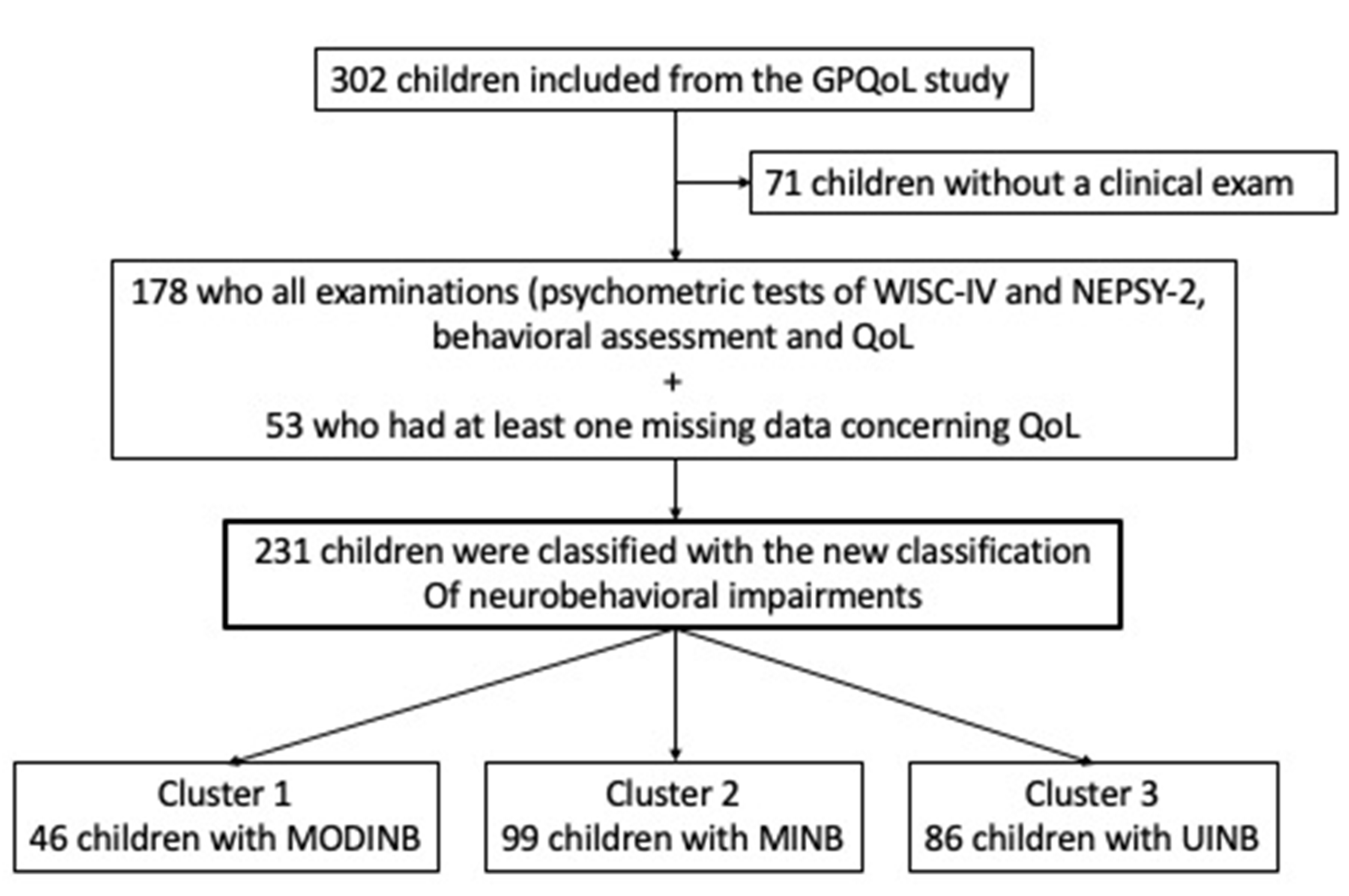
3.1. Population
3.2. Cognitive/Behavioral Impairments Profiles from New Classification
- Cluster 1 Moderate Impaired NeuroBehavior (MODINB) with multiple impairments and behavior troubles (n = 46 (20%));
- Cluster 2 Minor Impaired NeuroBehavior (MINB) with less severe multiple impairments and behavioral troubles, (n = 99 (43%)); and
- Cluster 3 (n = 86 (37%)), UnImpaired NeuroBehavior (UINB), with only slight emotional symptoms (mean score: 3.5 (SDs) = 2.56: slightly below average, therefore pathological), with a normal neurocognitive assessment outcome.
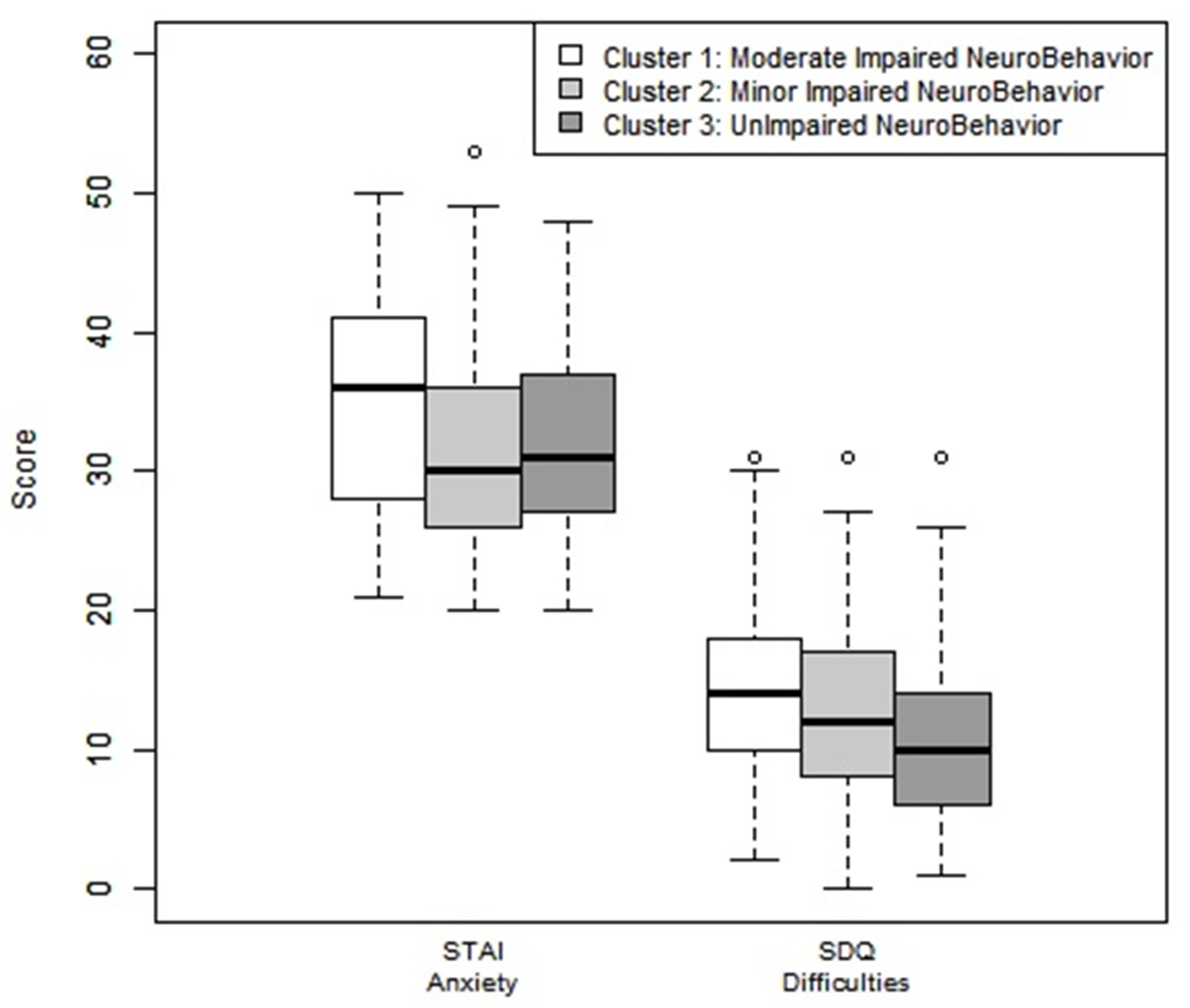
3.3. Neurobehavioral Impairment Profiles: Behavioral and Neurocognitive Comorbidities
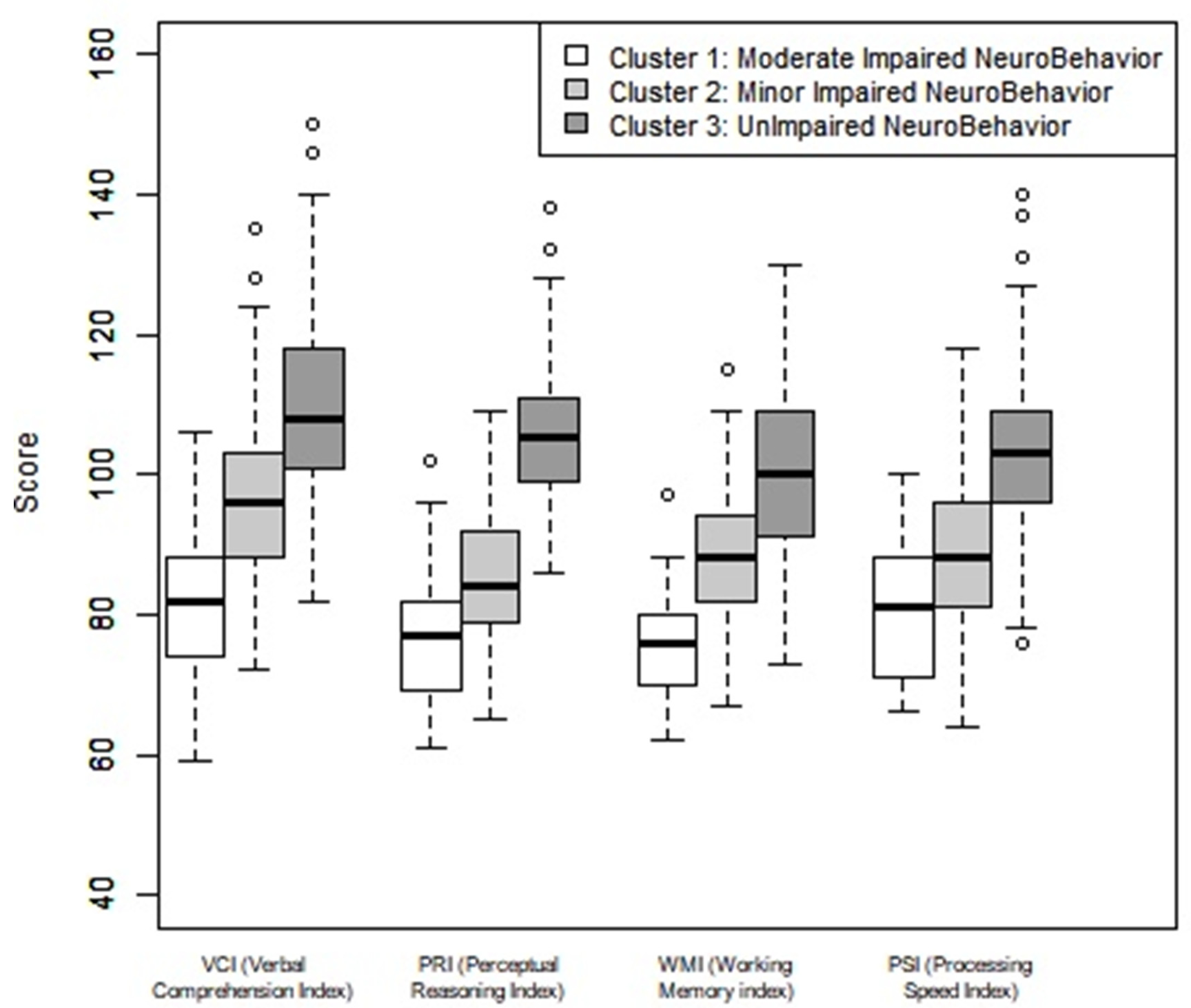
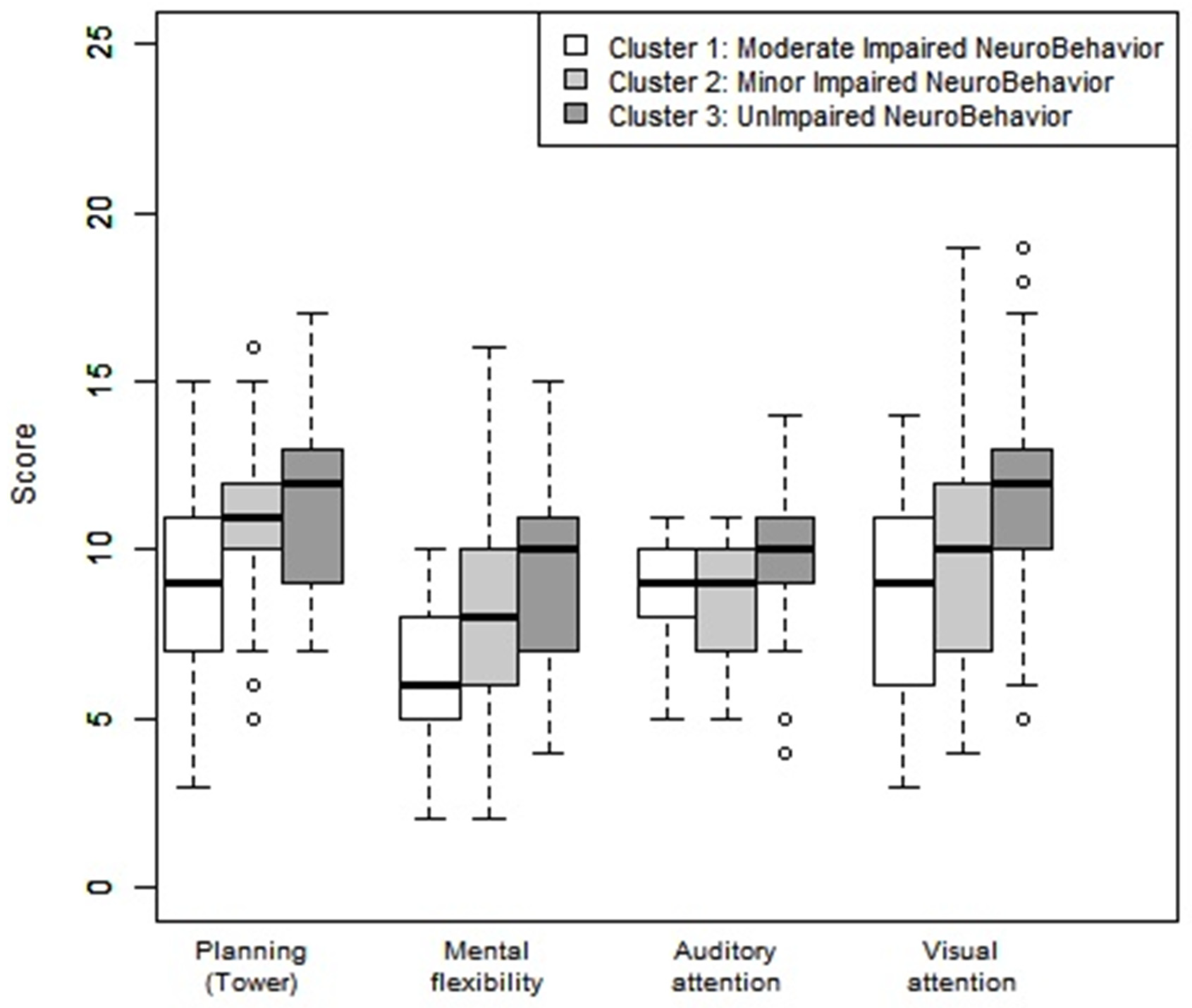
3.4. Neurobehavioral Cognitive Assessment by Cluster
3.5. Correlation of Population Study and Quality of Life
3.5.1. Quality of Life Comparisons between the Neurobehavior Impairment Clusters
3.5.2. Quality of Life in Cluster 3
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, S.; Marlow, N. Preterm Birth and Childhood Psychiatric Disorders. Pediatr. Res. 2011, 69, 11R–18R. [Google Scholar] [CrossRef]
- Anderson, P.J. Neuropsychological Outcomes of Children Born Very Preterm. Semin. Fetal Neonatal Med. 2014, 19, 90–96. [Google Scholar] [CrossRef]
- Bolk, J.; Farooqi, A.; Hafström, M.; Åden, U.; Serenius, F. Developmental Coordination Disorder and Its Association with Developmental Comorbidities at 6.5 Years in Apparently Healthy Children Born Extremely Preterm. JAMA Pediatr. 2018, 172, 765–774. [Google Scholar] [CrossRef]
- Bolk, J.; Fredriksson Kaul, Y.; Hellström-Westas, L.; Stjernqvist, K.; Padilla, N.; Serenius, F.; Hellgren, K.; Åden, U. National Population-Based Cohort Study Found that Visual-Motor Integration Was Commonly Affected in Extremely Preterm Born Children at Six-and-a-Half Years. Acta Paediatr. 2018, 107, 831–837. [Google Scholar] [CrossRef] [Green Version]
- Mathewson, K.J.; Chow, C.H.T.; Dobson, K.G.; Pope, E.I.; Schmidt, L.A.; Van Lieshout, R.J. Mental Health of Extremely Low Birth Weight Survivors: A Systematic Review and Meta-Analysis. Psychol. Bull. 2017, 143, 347–383. [Google Scholar] [CrossRef]
- Fitzallen, G.C.; Taylor, H.G.; Bora, S. What do We Know about the Preterm Behavioral Phenotype? A Narrative Review. Front. Psychiatry 2020, 11, 154. [Google Scholar] [CrossRef]
- Korkman, M.; Mikkola, K.; Ritari, N.; Tommiska, V.; Salokorpi, T.; Haataja, L.; Tammela, O.; Pääkkönen, L.; Olsén, P.; Fellman, V. Neurocognitive Test Profiles of Extremely Low Birth Weight Five-Year-Old Children Differ according to Neuromotor Status. Dev. Neuropsychol. 2008, 33, 637–655. [Google Scholar] [CrossRef]
- Heeren, T.; Joseph, R.M.; Allred, E.N.; O’Shea, T.M.; Leviton, A.; Kuban, K.C.K. Cognitive Functioning at the Age of 10 Years among Children Born Extremely Preterm: A Latent Profile Approach. Pediatr. Res. 2017, 82, 614–619. [Google Scholar] [CrossRef] [Green Version]
- Pierrat, V.; Marchand-Martin, L.; Marret, S.; Arnaud, C.; Benhammou, V.; Cambonie, G.; Debillon, T.; Dufourg, M.-N.; Gire, C.; Goffinet, F.; et al. Neurodevelopmental Outcomes at Age 5 among Children Born Preterm: EPIPAGE-2 Cohort Study. BMJ 2021, 373, n741. [Google Scholar] [CrossRef]
- Gire, C.; Resseguier, N.; Brévaut-Malaty, V.; Marret, S.; Cambonie, G.; Souksi-Medioni, I.; Müller, J.-B.; Garcia, P.; Berbis, J.; Tosello, B.; et al. Quality of Life of Extremely Preterm School-Age Children without Major Handicap: A Cross-Sectional Observational Study. Arch. Dis. Child. 2019, 104, 333–339. [Google Scholar] [CrossRef]
- Gire, C.; Tosello, B.; Marret, S.; Cambonie, G.; Souksi-Medioni, I.; Müller, J.-B.; Garcia, P.; Berbis, J.; Auquier, P.; Brévaut-Malaty, V.; et al. Specific Cognitive Correlates of the Quality of Life of Extremely Preterm School-Aged Children without Major Neurodevelopmental Disability. Pediatr. Res. 2020, 88, 642–652. [Google Scholar] [CrossRef]
- Kaufman, L.; Rousseeuw, P.J. Finding Groups in Data: An Introduction to Cluster Analysis; Wiley–Blackwell: Hoboken, NJ, USA, 2005; ISBN 978-0-471-73578-6. [Google Scholar]
- Kaufmann, L.; Rousseeuw, P. Clustering by Means of Medoids. In Data Analysis based on the L1-Norm and Related Methods; Elsevier Science Ltd.: Neuchatel, Switzerland, 1987; pp. 405–416. [Google Scholar]
- Johnson, S.; Wolke, D. Behavioural Outcomes and Psychopathology during Adolescence. Early Hum. Dev. 2013, 89, 199–207. [Google Scholar] [CrossRef]
- Samuelsson, M.; Holsti, A.; Adamsson, M.; Serenius, F.; Hägglöf, B.; Farooqi, A. Behavioral Patterns in Adolescents Born at 23 to 25 Weeks of Gestation. Pediatrics 2017, 140, e20170199. [Google Scholar] [CrossRef] [Green Version]
- Taylor, H.G.; Margevicius, S.; Schluchter, M.; Andreias, L.; Hack, M. Persisting Behavior Problems in Extremely Low Birth Weight Adolescents. J. Dev. Behav. Pediatr. 2015, 36, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Burnett, A.C.; Anderson, P.J.; Cheong, J.; Doyle, L.W.; Davey, C.G.; Wood, S.J. Prevalence of Psychiatric Diagnoses in Preterm and Full-Term Children, Adolescents and Young Adults: A Meta-Analysis. Psychol. Med. 2011, 41, 2463–2474. [Google Scholar] [CrossRef]
- Burnett, A.C.; Youssef, G.; Anderson, P.J.; Duff, J.; Doyle, L.W.; Cheong, J.L.Y.; Victorian Infant Collaborative Study Group. Exploring the “Preterm Behavioral Phenotype” in Children Born Extremely Preterm. J. Dev. Behav. Pediatr. 2019, 40, 200–207. [Google Scholar] [CrossRef]
- Korzeniewski, S.J.; Joseph, R.M.; Kim, S.H.; Allred, E.N.; O’Shea, T.M.; Leviton, A.; Kuban, K.C.K.; ELGAN Study Investigators. Social Responsiveness Scale Assessment of the Preterm Behavioral Phenotype in 10-Year-Olds Born Extremely Preterm. J. Dev. Behav. Pediatr. 2017, 38, 697–705. [Google Scholar] [CrossRef]
- Mulder, H.; Pitchford, N.J.; Marlow, N. Processing Speed and Working Memory Underlie Academic Attainment in Very Preterm Children. Arch. Dis. Child. Fetal Neonatal Ed. 2010, 95, F267–F272. [Google Scholar] [CrossRef]
- Aarnoudse-Moens, C.S.H.; Weisglas-Kuperus, N.; van Goudoever, J.B.; Oosterlaan, J. Meta-Analysis of Neurobehavioral Outcomes in Very Preterm and/or Very Low Birth Weight Children. Pediatrics 2009, 124, 717–728. [Google Scholar] [CrossRef]
- Mulder, H.; Pitchford, N.J.; Marlow, N. Processing Speed Mediates Executive Function Difficulties in Very Preterm Children in Middle Childhood. J. Int. Neuropsychol. Soc. 2011, 17, 445–454. [Google Scholar] [CrossRef]
- Omizzolo, C.; Scratch, S.E.; Stargatt, R.; Kidokoro, H.; Thompson, D.K.; Lee, K.J.; Cheong, J.; Neil, J.; Inder, T.E.; Doyle, L.W.; et al. Neonatal Brain Abnormalities and Memory and Learning Outcomes at 7 Years in Children Born Very Preterm. Memory 2014, 22, 605–615. [Google Scholar] [CrossRef] [Green Version]
- Hutchinson, E.A.; De Luca, C.R.; Doyle, L.W.; Roberts, G.; Anderson, P.J.; Victorian Infant Collaborative Study Group. School-Age Outcomes of Extremely Preterm or Extremely Low Birth Weight Children. Pediatrics 2013, 131, e1053–e1061. [Google Scholar] [CrossRef] [Green Version]
- Mulder, H.; Pitchford, N.J.; Hagger, M.S.; Marlow, N. Development of Executive Function and Attention in Preterm Children: A Systematic Review. Dev. Neuropsychol. 2009, 34, 393–421. [Google Scholar] [CrossRef]
- Ritchie, K.; Bora, S.; Woodward, L.J. Social Development of Children Born Very Preterm: A Systematic Review. Dev. Med. Child Neurol. 2015, 57, 899–918. [Google Scholar] [CrossRef]
- Conti, E.; Calderoni, S.; Marchi, V.; Muratori, F.; Cioni, G.; Guzzetta, A. The First 1000 Days of the Autistic Brain: A Systematic Review of Diffusion Imaging Studies. Front. Hum. Neurosci. 2015, 9, 159. [Google Scholar] [CrossRef]
- Tymofiyeva, O.; Gano, D.; Trevino, R.J.; Glass, H.C.; Flynn, T.; Lundy, S.M.; McQuillen, P.S.; Ferriero, D.M.; Barkovich, A.J.; Xu, D. Aberrant Structural Brain Connectivity in Adolescents with Attentional Problems Who Were Born Prematurely. AJNR Am. J. Neuroradiol. 2018, 39, 2140–2147. [Google Scholar] [CrossRef]
- Pyhälä, R.; Wolford, E.; Kautiainen, H.; Andersson, S.; Bartmann, P.; Baumann, N.; Brubakk, A.-M.; Evensen, K.A.I.; Hovi, P.; Kajantie, E.; et al. Self-Reported Mental Health Problems among Adults Born Preterm: A Meta-Analysis. Pediatrics 2017, 139, e20162690. [Google Scholar] [CrossRef] [Green Version]
- Wallin, L.; Eriksson, M. Newborn Individual Development Care and Assessment Program (NIDCAP): A Systematic Review of the Literature. Worldviews Evid.-Based Nurs. 2009, 6, 54–69. [Google Scholar] [CrossRef]
- Taylor, H.G.; Klein, N.; Drotar, D.; Schluchter, M.; Hack, M. Consequences and Risks of <1000-g Birth Weight for Neuropsychological Skills, Achievement, and Adaptive Functioning. J. Dev. Behav. Pediatr. 2006, 27, 459–469. [Google Scholar] [CrossRef]
- Ding, S.; Lemyre, B.; Daboval, T.; Barrowman, N.; Moore, G.P. A Meta-Analysis of Neurodevelopmental Outcomes at 4–10 Years in Children Born at 22–25 Weeks Gestation. Acta Paediatr. 2019, 108, 1237–1244. [Google Scholar] [CrossRef]
- Escovar, E.; Rosenberg-Lee, M.; Uddin, L.Q.; Menon, V. The Empathizing-Systemizing Theory, Social Abilities, and Mathematical Achievement in Children. Sci. Rep. 2016, 6, 23011. [Google Scholar] [CrossRef] [Green Version]
- Diamond, A.; Lee, K. Interventions Shown to Aid Executive Function Development in Children 4 to 12 Years Old. Science 2011, 333, 959–964. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of Clustered Pooling (N = 231) | ||||||
|---|---|---|---|---|---|---|
| MODINB Cluster 1 (N = 46) | MINB Cluster 2 (N = 99) | UINB Cluster 3 (N = 86) | P | |||
| Perinatal characteristics | ||||||
| GA in WA, mean (SD) | 26.13 (0.96) | 26.25 (0.82) | 26.29 (0.92) | 0.607 | ||
| Weight in grams, mean (SD) | 858.91 (181.77) | 878.77 (194.69) | 901.31 (171.47) | 0.430 | ||
| Male, n (%) | 20 (43.48) | 50 (51.02) | 38 (44.71) | 0.594 | ||
| SGA, n (%) | 5 (10.87) | 10 (10.10) | 1 (1.16) | 0.011 * | ||
| Multiple pregnancies, n (%) | 17 (36.96) | 30 (30.30) | 31 (36.05) | 0.625 | ||
| Severe BPD, n (%) | 25 (54.35) | 46 (47.92) | 47 (54.65) | 0.613 | ||
| Average age of child at the study inclusion, mean (SD) | 8.69 (0.65) | 8.43 (0.74) | 8.39 (0.72) | 0.056 | ||
| Parents’ educational level, professional activity, and socioeconomic status of family | ||||||
| Parents without higher education level, n (%) | 29 (74.36) | 46 (47.92) | 18 (21.43) | <0.001 * | ||
| Professional activity of parents, n (%) | 0.004 * | |||||
| Without professional activity | 8 (18.60) | 7 (7.14) | 3 (3.53) | |||
| Professional activity of one of two parents | 16 (37.21) | 37 (37.76) | 20 (23.53) | |||
| Professional activity of both parents | 19 (44.19) | 54 (55.10) | 62 (72.94) | |||
| Professional activity of mother, n (%) | 21 (48.84) | 63 (64.29) | 66 (79.52) | 0.002 | ||
| Professional activity of father, n (%) | 33 (82.50) | 82 (89.13) | 78 (92.86) | 0.243 | ||
| Elevated FAS Score, n (%) | 21 (45.65) | 57 (58.76) | 57 (67.06) | 0.059 | ||
| Quality of life 1, mean (SD) | ||||||
| VSP-Ae global index (evaluation by the child) | 64.38 (12.55) | 70.30 (13.07) | 70.16 (13.06) | 0.029 * | ||
| VSP-Ap global index (evaluation by the parents) | 64.38 (12.35) | 70.66 (10.51) | 71.25 (10.61) | 0.008 * | ||
| Kidscreen global index (evaluation by the child) | 68.43 (16.65) | 73.26 (17.43) | 71.91 (17.30) | 0.293 | ||
| Kidscreen global index (evaluation by the parents) | 62.52 (16.54) | 70.16 (14.50) | 71.33 (13.39) | 0.003 * | ||
| Neurocognitive assessment 2 | ||||||
| WISC-IV 2a, mean (SD) | ||||||
| VCI (Verbal comprehension index) | 80.93 (9.46) | 96.56 (11.75) | 109.51 (12.74) | <0.001 * | ||
| PRI (Perceptional reasoning index) | 77.26 (8.99) | 85.41 (9.24) | 106.73 (9.94) | <0.001 * | ||
| WMI (Working memory index) | 74.93 (11.07) | 88.85 (9.38) | 101.15 (11.41) | <0.001 * | ||
| PSI (Processing speed index) | 80.15 (8.96) | 88.49 (10.75) | 102.90 (12.61) | <0.001 * | ||
| NEPSY-2 2b, mean (SD) | ||||||
| Planification score (Tower) | 8.80 (3.04) | 10.81 (2.33) | 11.52 (2.43) | <0.001 * | ||
| Mental flexibility score | 6.50 (2.27) | 7.76 (2.72) | 9.48 (2.68) | <0.001 * | ||
| Auditive attention score | 8.61 (1.34) | 8.45 (1.51) | 9.66 (1.73) | <0.001 * | ||
| Visual attention score | 8.98 (2.73) | 9.78 (3.47) | 11.64 (3.03) | <0.001 * | ||
| Goodman-SDQ-parents 3, mean (SD) | ||||||
| Emotional symptoms | 4.05 (2.62) | 3.64 (2.37) | 3.15 (2.56) | 0.136 | ||
| Behavioral problems | 2.52 (1.99) | 1.94 (1.93) | 1.64 (1.73) | 0.040 * | ||
| Hyperactivity/Inattention | 5.32 (2.45) | 4.89 (2.56) | 3.93 (2.74) | 0.007 * | ||
| Relationship problems with others | 2.23 (1.92) | 2.17 (1.98) | 1.55 (1.77) | 0.051 | ||
| Prosocial behaviors | 8.59 (1.59) | 8.61 (1.70) | 8.89 (1.42) | 0.412 | ||
| Total difficulty scores | 14.11 (6.39) | 12.64 (6.63) | 10.27 (5.78) | 0.002 * | ||
| Anxiety, mean (SD) | ||||||
| Spielberg Index (STAIC) 4 | 35.30 (8.28) | 31.90 (7.71) | 32.25 (6.89) | 0.035 * | ||
| Impairment 5 | ||||||
| Language delay 5a, n (%) | 30 (65.22) | 16 (16.16) | 1 (1.16) | <0.001 * | ||
| Delay in visuospatial integration 5b, n (%) | 17 (36.96) | 18 (18.18) | 0 (0.00) | <0.001 * | ||
| Attention deficit disorder 5c, n (%) | 15 (32.61) | 19 (19.19) | 2 (2.33) | <0.001 * | ||
| Dysexecutive disorder 5d, n (%) | 44 (95.65) | 67 (67.68) | 26 (30.23) | <0.001 * | ||
| Ideomotor dyspraxia 5e, n (%) | 14 (30.43) | 10 (10.10) | 0 (0.00) | <0.001 * | ||
| Quality of Life between Study Population vs. Reference Population | Quality of Life between Three Clusters | Quality of Life between Cluster 3 vs. Reference Population | ||||||||||||||||||||||
| Study Population (n = 178) | Reference Population a | Difference | p | Effect Size 3 (Ranking) | Cluster 1 b (n = 32) | Cluster 2 c (n = 79) | Cluster 3 d (n = 67) | p | Reference Population | Difference | p | Effect Size 3 (Ranking) | ||||||||||||
| Mean | SD | Expected Mean | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Expected Mean | Mean | SD | |||||||||||
| VSP-A ENFANT 1 | ||||||||||||||||||||||||
| Vitality | 77.50 | 19.90 | 82.46 | −4.95 | 19.96 | 0.001 * | −0.25 | 77.03 | 20.90 | 77.22 | 19.77 | 78.06 | 0.958 | 82.31 | −4.25 | 19.77 | 0.083 | −0.22 | ||||||
| General well- being | 72.61 | 17.93 | 78.38 | −5.77 | 18.02 | <0.001 * | −0.32 | 68.15 | 17.56 | 74.33 | 17.23 | 72.72 | 18.79 | 0.259 | 78.42 | −5.70 | 18.73 | 0.015 * | −0.3 | 3 | ||||
| Relationship with friends | 46.89 | 28.11 | 58.91 | −12.02 | 28.17 | <0.001 * | −0.43 | 2 | 43.29 | 24.81 | 46.70 | 28.66 | 48.82 | 29.14 | 0.659 | 58.89 | −10.07 | 29.37 | 0.006 * | −0.34 | 1 | |||
| Leisure | 62.86 | 20.52 | 69.63 | −6.77 | 20.57 | <0.001 * | −0.33 | 3 | 60.16 | 18.21 | 63.96 | 20.81 | 62.85 | 21.37 | 0.679 | 69.39 | −6.54 | 21 | 0.013 * | −0.31 | 2 | |||
| Relationship with family | 74.10 | 19.05 | 73.19 | 0.91 | 19.10 | 0.528 | 0.05 | 74.38 | 17.33 | 74.97 | 18.55 | 72.94 | 20.58 | 0.813 | 73.00 | −0.06 | 20.77 | 0.981 | 0 | |||||
| School work | 76.19 | 23.50 | 82.08 | −5.88 | 23.45 | 0.001 * | −0.25 | 60.94 | 24.75 | 78.8 | 21.87 | 80.41 | 22.11 | <0.001 * | 82.16 | −1.75 | 21.98 | 0.518 | −0.08 | |||||
| Self esteem | 74.20 | 21.33 | 84.61 | −10.41 | 21.42 | <0.001 * | −0.49 | 1 | 63.54 | 22.71 | 74.74 | 21.39 | 78.67 | 19.00 | 0.004 * | 84.49 | −5.82 | 19.25 | 0.016 * | −0.3 | ||||
| Total index | 69.19 | 13.56 | 75.59 | −6.40 | 13.65 | <0.001 * | −0.47 | 63.93 | 11.5 | 70.1 | 13.35 | 70.64 | 14.27 | 0.050 | 75.51 | −4.87 | 14.31 | 0.007 * | −0.34 | |||||
| VSP-PARENTS 1 | ||||||||||||||||||||||||
| Vitality | 69.92 | 16.15 | 77.38 | −7.46 | 16.26 | <0.001 * | −0.46 | 65.23 | 16.43 | 69.86 | 16.14 | 72.23 | 15.77 | 0.131 | 77.36 | −5.13 | 15.66 | 0.009 * | −0.33 | 3 | ||||
| Psychological well-being | 70.19 | 20.43 | 81.34 | −11.15 | 20.50 | <0.001 * | −0.54 | 1 | 70.23 | 25.58 | 70.46 | 19.08 | 69.85 | 19.53 | 0.984 | 81.19 | −11.34 | 19.57 | <0.001 * | −0.58 | 1 | |||
| Relationship with friends | 59.18 | 20.04 | 64.53 | −5.36 | 20.15 | <0.001 * | −0.27 | 53.45 | 20.28 | 59.49 | 21.28 | 61.54 | 18.08 | 0.169 | 64.71 | −3.17 | 18.43 | 0.163 | −0.17 | |||||
| Leisure | 52.41 | 18.32 | 57.01 | −4.60 | 18.30 | 0.001 * | −0.25 | 50.13 | 17.53 | 54.11 | 19.03 | 51.49 | 17.91 | 0.512 | 57.85 | −5.36 | 17.85 | 0.017 * | −0.3 | |||||
| Relationship with family | 77.21 | 13.65 | 78.62 | −1.41 | 13.69 | 0.172 | −0.10 | 75.91 | 16.08 | 78.80 | 13.63 | 75.96 | 12.39 | 0.386 | 78.51 | −2.55 | 12.32 | 0.095 | −0.21 | |||||
| Physical well being | 75.78 | 16.18 | 78.60 | −2.82 | 16.19 | 0.021 * | −0.17 | 74.28 | 16.32 | 76.58 | 17.03 | 75.56 | 15.26 | 0.789 | 78.38 | −2.82 | 15 | 0.129 | −0.19 | |||||
| Relationship with teacher | 73.17 | 18.46 | 75.16 | −1.99 | 18.67 | 0.157 | −0.11 | 70.31 | 19.28 | 74.26 | 17.05 | 73.26 | 19.76 | 0.596 | 75.32 | −2.06 | 19.78 | 0.398 | −0.1 | |||||
| School work | 69.66 | 20.14 | 79.80 | −10.14 | 20.18 | <0.001 * | −0.50 | 2 | 60.94 | 22.17 | 67.41 | 18.17 | 76.49 | 19.40 | 0.001 * | 79.92 | −3.43 | 19.67 | 0.158 | −0.17 | ||||
| Self esteem | 78.93 | 27.33 | 88.44 | −9.50 | 27.43 | <0.001 * | −0.35 | 62.11 | 32.14 | 81.17 | 24.59 | 84.33 | 25.13 | <0.001 * | 88.09 | −3.76 | 25.71 | 0.236 | −0.15 | |||||
| General well- being | 72.72 | 15.81 | 80.12 | −7.41 | 15.89 | <0.001 * | −0.47 | 3 | 72.19 | 18.24 | 73.20 | 15.28 | 72.40 | 15.42 | 0.935 | 79.94 | −7.54 | 15.38 | <0.001 * | −0.49 | 2 | |||
| Total Index | 69.61 | 11.17 | 75.96 | −6.36 | 11.23 | <0.001 * | −0.57 | 64.73 | 12.38 | 70.24 | 10.59 | 71.19 | 10.75 | 0.021 * | 75.89 | −4.69 | 10.81 | 0.001 * | −0.43 | |||||
| KIDSCREEN-ENFANT 2 | ||||||||||||||||||||||||
| Total index | 72.23 | 17.63 | 76.87 | −4.65 | 17.74 | 0.001 * | −0.26 | 67.39 | 17.7 | 73.82 | 17.26 | 72.66 | 17.89 | 0.213 | 76.78 | −4.12 | 17.92 | 0.064 | −0.23 | |||||
| KIDSCREEN-PARENTS 2 | ||||||||||||||||||||||||
| Total index | 69.61 | 14.83 | 71.84 | −2.23 | 14.83 | 0.046 * | −0.15 | 64.91 | 16.16 | 70.01 | 14.94 | 71.37 | 13.74 | 0.121 | 71.84 | −0.47 | 13.74 | 0.781 | −0.03 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tosello, B.; Méziane, S.; Resseguier, N.; Marret, S.; Cambonie, G.; Zahed, M.; Brévaut-Malaty, V.; Beltran Anzola, A.; Gire, C.; for the GPQoL-Study Group. The Neurobehavioral Phenotype of School-Aged, Very Prematurely Born Children with No Serious Neurological Sequelae: A Quality of Life Predictor. Children 2021, 8, 943. https://doi.org/10.3390/children8110943
Tosello B, Méziane S, Resseguier N, Marret S, Cambonie G, Zahed M, Brévaut-Malaty V, Beltran Anzola A, Gire C, for the GPQoL-Study Group. The Neurobehavioral Phenotype of School-Aged, Very Prematurely Born Children with No Serious Neurological Sequelae: A Quality of Life Predictor. Children. 2021; 8(11):943. https://doi.org/10.3390/children8110943
Chicago/Turabian StyleTosello, Barthélémy, Sahra Méziane, Noémie Resseguier, Stéphane Marret, Gilles Cambonie, Meriem Zahed, Véronique Brévaut-Malaty, Any Beltran Anzola, Catherine Gire, and for the GPQoL-Study Group. 2021. "The Neurobehavioral Phenotype of School-Aged, Very Prematurely Born Children with No Serious Neurological Sequelae: A Quality of Life Predictor" Children 8, no. 11: 943. https://doi.org/10.3390/children8110943
APA StyleTosello, B., Méziane, S., Resseguier, N., Marret, S., Cambonie, G., Zahed, M., Brévaut-Malaty, V., Beltran Anzola, A., Gire, C., & for the GPQoL-Study Group. (2021). The Neurobehavioral Phenotype of School-Aged, Very Prematurely Born Children with No Serious Neurological Sequelae: A Quality of Life Predictor. Children, 8(11), 943. https://doi.org/10.3390/children8110943