
Anthropometric Indices of Giardia-Infected Under-Five Children Presenting with Moderate-to-Severe Diarrhea and Their Healthy Community Controls: Data from the Global Enteric Multicenter Study

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Consideration
2.2. Study Site
2.3. Study Design and Study Participants Enrollment Procedure
2.4. Specimen Collection and Laboratory Procedure
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muhsen, K.; Levine, M.M. A systematic review and meta-analysis of the association between Giardia lamblia and endemic pediatric diarrhea in developing countries. Clin. Infect. Dis. 2012, 55, S271–S293. [Google Scholar] [CrossRef]
- Hug, L.; Dharrow, D.; Zhong, K.; You, D. Levels and Trends in Child Mortality: Report 2018; The World Bank: Washington, DC, USA, 2018. [Google Scholar]
- Lanata, C.F.; Fischer-Walker, C.L.; Olascoaga, A.C.; Torres, C.X.; Aryee, M.J.; Black, R.E.; UNICEF. Global causes of diarrheal disease mortality in children < 5 years of age: A systematic review. PLoS ONE 2013, 8, e72788. [Google Scholar]
- Srijan, A.; Wongstitwilairoong, B.; Pitarangsi, C.; Serichantalergs, O.; Fukuda, C.D.; Bodhidatta, L.; Mason, C.J. Re-evaluation of commercially available enzyme-linked immunosorbent assay for the detection of Giardia lamblia and Cryptosporidium spp from stool specimens. Southeast Asian J. Trop. Med. Public Health 2005, 36 (Suppl. 4), 26–29. [Google Scholar]
- Lehto, K.M.; Fan, Y.M.; Oikarinen, S.; Nurminen, N.; Hallamaa, L.; Juuti, R.; Mangani, C.; Maleta, K.; Hyöty, H.; Ashorn, P. Presence of Giardia lamblia in stools of six-to 18-month old asymptomatic Malawians is associated with children’s growth failure. Acta Paediatr. 2019, 108, 1833–1840. [Google Scholar] [CrossRef] [Green Version]
- Caron, Y.; Hong, R.; Gauthier, L.; Laillou, A.; Wieringa, F.T.; Berger, J.; Poirot, E. Stunting, beyond acute diarrhoea: Giardia duodenalis, in Cambodia. Nutrients 2018, 10, 1420. [Google Scholar] [CrossRef] [Green Version]
- Dib, H.H.; Lu, S.Q.; Wen, S.F. Prevalence of Giardia lamblia with or without diarrhea in South East, South East Asia and the Far East. Parasitol. Res. 2008, 103, 239–251. [Google Scholar] [CrossRef]
- Khurana, S.; Aggarwal, A.; Malla, N. Comparative analysis of intestinal parasitic infections in slum, rural and urban populations in and around union Territory, Chandigarh. J. Commun. Dis. 2005, 37, 239–243. [Google Scholar]
- Suman, M.; Alam, M.; Pun, S.; Khair, A.; Ahmed, S.; Uchida, R. Prevalence of Giardia lamblia infection in children and calves in Bangladesh. Bangladesh J. Vet. Med. 2011, 9, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Guk, S.-M.; Seo, M.; Park, Y.-K.; Oh, M.-D.; Choe, K.-W.; Kim, J.-L.; Choi, M.-H.; Hong, S.-T.; Chai, J.-Y. Parasitic infections in HIV-infected patients who visited Seoul National University Hospital during the period 1995–2003. Korean J. Parasitol. 2005, 43, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Haque, R.; Mondal, D.; Kirkpatrick, B.D.; Akther, S.; Farr, B.M.; Sack, R.B.; Petri, W.A. Epidemiologic and clinical characteristics of acute diarrhea with emphasis on Entamoeba histolytica infections in preschool children in an urban slum of Dhaka, Bangladesh. Am. J. Trop. Med. Hyg. 2003, 69, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Haque, R.; Roy, S.; Kabir, M.; Stroup, S.E.; Mondal, D.; Houpt, E.R. Giardia assemblage A infection and diarrhea in Bangladesh. J. Infect. Dis. 2005, 192, 2171–2173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, M.J.; Faruque, A.; Faruque, S.; Sack, R.; Mahalanabis, D. Case-control study of enteropathogens associated with childhood diarrhea in Dhaka, Bangladesh. J. Clin. Microbiol. 1999, 37, 3458–3464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, M.M.; Kotloff, K.L.; Nataro, J.P.; Muhsen, K. The global enteric multicenter study (GEMS): Impetus, rationale, and genesis. Clin. Infect. Dis. 2012, 55, S215–S224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farag, T.H.; Nasrin, D.; Wu, Y.; Muhsen, K.; Blackwelder, W.C.; Sommerfelt, H.; Panchalingam, S.; Nataro, J.P.; Kotloff, K.L.; Levine, M.M. Some epidemiologic, clinical, microbiologic, and organizational assumptions that influenced the design and performance of the Global Enteric Multicenter Study (GEMS). Clin. Infect. Dis. 2012, 55 (Suppl. 4), S225–S231. [Google Scholar] [CrossRef] [PubMed]
- Kotloff, K.L.; Blackwelder, W.C.; Nasrin, D.; Nataro, J.P.; Farag, T.H.; van Eijk, A.; Adegbola, R.A.; Alonso, P.L.; Breiman, R.F.; Golam Faruque, A.S. The Global Enteric Multicenter Study (GEMS) of diarrheal disease in infants and young children in developing countries: Epidemiologic and clinical methods of the case/control study. Clin. Infect. Dis. 2012, 55, S232–S245. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006.
- Panchalingam, S.; Antonio, M.; Hossain, A.; Mandomando, I.; Ochieng, B.; Oundo, J.; Ramamurthy, T.; Tamboura, B.; Zaidi, A.K.; Petri, W. Diagnostic microbiologic methods in the GEMS-1 case/control study. Clin. Infect. Dis. 2012, 55 (Suppl. 4), S294–S302. [Google Scholar] [CrossRef] [Green Version]
- Abou-Shady, O.; El Raziky, M.S.; Zaki, M.M.; Mohamed, R.K. Impact of Giardia lamblia on growth, serum levels of zinc, copper, and iron in Egyptian children. Biol. Trace Elem. Res. 2011, 140, 1–6. [Google Scholar] [CrossRef]
- Botero-Garcés, J.H.; García-Montoya, G.M.; Grisales-Patiño, D.; Aguirre-Acevedo, D.C.; Álvarez-Uribe, M.C. Giardia intestinalis and nutritional status in children participating in the complementary nutrition program, Antioquia, Colombia, May to October 2006. Rev. Inst. Med. Trop. São Paulo 2009, 51, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Lass, A.; Karanis, P.; Korzeniewski, K. First detection and genotyping of Giardia intestinalis in stool samples collected from children in Ghazni Province, eastern Afghanistan and evaluation of the PCR assay in formalin-fixed specimens. Parasitol. Res. 2017, 116, 2255–2264. [Google Scholar] [CrossRef]
- Bello, J.; Núñez, F.; González, O.; Fernández, R.; Almirall, P.; Escobedo, A. Risk factors for Giardia infection among hospitalized children in Cuba. Ann. Trop. Med. Parasitol. 2011, 105, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Bartelt, L.A.; Sartor, R.B. Advances in understanding Giardia: Determinants and mechanisms of chronic sequelae. F1000prime Rep. 2015, 7, 62. [Google Scholar] [CrossRef] [Green Version]
- Ashraf, S.; Nizame, F.A.; Islam, M.; Dutta, N.C.; Yeasmin, D.; Akhter, S.; Abedin, J.; Winch, P.J.; Ram, P.K.; Unicomb, L. Nonrandomized trial of feasibility and acceptability of strategies for promotion of soapy water as a handwashing agent in rural Bangladesh. Am. J. Trop. Med. Hyg. 2017, 96, 421. [Google Scholar] [CrossRef] [Green Version]
- Rogawski, E.T.; Liu, J.; Platts-Mills, J.A.; Kabir, F.; Lertsethtakarn, P.; Siguas, M.; Khan, S.S.; Praharaj, I.; Murei, A.; Nshama, R. Use of quantitative molecular diagnostic methods to investigate the effect of enteropathogen infections on linear growth in children in low-resource settings: Longitudinal analysis of results from the MAL-ED cohort study. Lancet Glob. Health 2018, 6, e1319–e1328. [Google Scholar] [CrossRef] [Green Version]
- Boeke, C.E.; Mora-Plazas, M.; Forero, Y.; Villamor, E. Intestinal protozoan infections in relation to nutritional status and gastrointestinal morbidity in Colombian school children. J. Trop. Pediatrics 2010, 56, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajjampur, S.; Koshy, B.; Venkataramani, M.; Sarkar, R.; Joseph, A.; Jacob, K.; Ward, H.; Kang, G. Effect of cryptosporidial and giardial diarrhoea on social maturity, intelligence and physical growth in children in a semi-urban slum in south India. Ann. Trop. Paediatr. 2011, 31, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Centeno-Lima, S.; Rosado-Marques, V.; Ferreira, F.; Rodrigues, R.; Indeque, B.; Camará, I.; De Sousa, B.; Aguiar, P.; Nunes, B.; Ferrinho, P. Giardia duodenalis and chronic malnutrition in children under five from a rural area of Guinea-Bissau. Acta Med. Port. 2013, 26, 721–724. [Google Scholar]
- Koot, B.G.; ten Kate, F.J.; Juffrie, M.; Rosalina, I.; Taminiau, J.J.; Benninga, M.A. Does Giardia lamblia cause villous atrophy in children?: A retrospective cohort study of the histological abnormalities in giardiasis. J. Pediatric Gastroenterol. Nutr. 2009, 49, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Denno, D.M.; VanBuskirk, K.; Nelson, Z.C.; Musser, C.A.; Hay Burgess, D.C.; Tarr, P.I. Use of the lactulose to mannitol ratio to evaluate childhood environmental enteric dysfunction: A systematic review. Clin. Infect. Dis. 2014, 59 (Suppl. 4), S213–S219. [Google Scholar] [CrossRef] [Green Version]
- Astiazaran-Garcia, H.; Lopez-Teros, V.; Valencia, M.E.; Vazquez-Ortiz, F.; Sotelo-Cruz, N.; Quihui-Cota, L. Giardia lamblia infection and its implications for vitamin A liver stores in school children. Ann. Nutr. Metab. 2010, 57, 228–233. [Google Scholar] [CrossRef]
- Nematian, J.; Gholamrezanezhad, A.; Nematian, E. Giardiasis and other intestinal parasitic infections in relation to anthropometric indicators of malnutrition: A large, population-based survey of schoolchildren in Tehran. Ann. Trop. Med. Parasitol. 2008, 102, 209–214. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicators | Cases Giardia (n = 1151) (%) | Healthy Controls Giardia (n = 2094) (%) | (Unadjusted) OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age of the participants in months | ||||
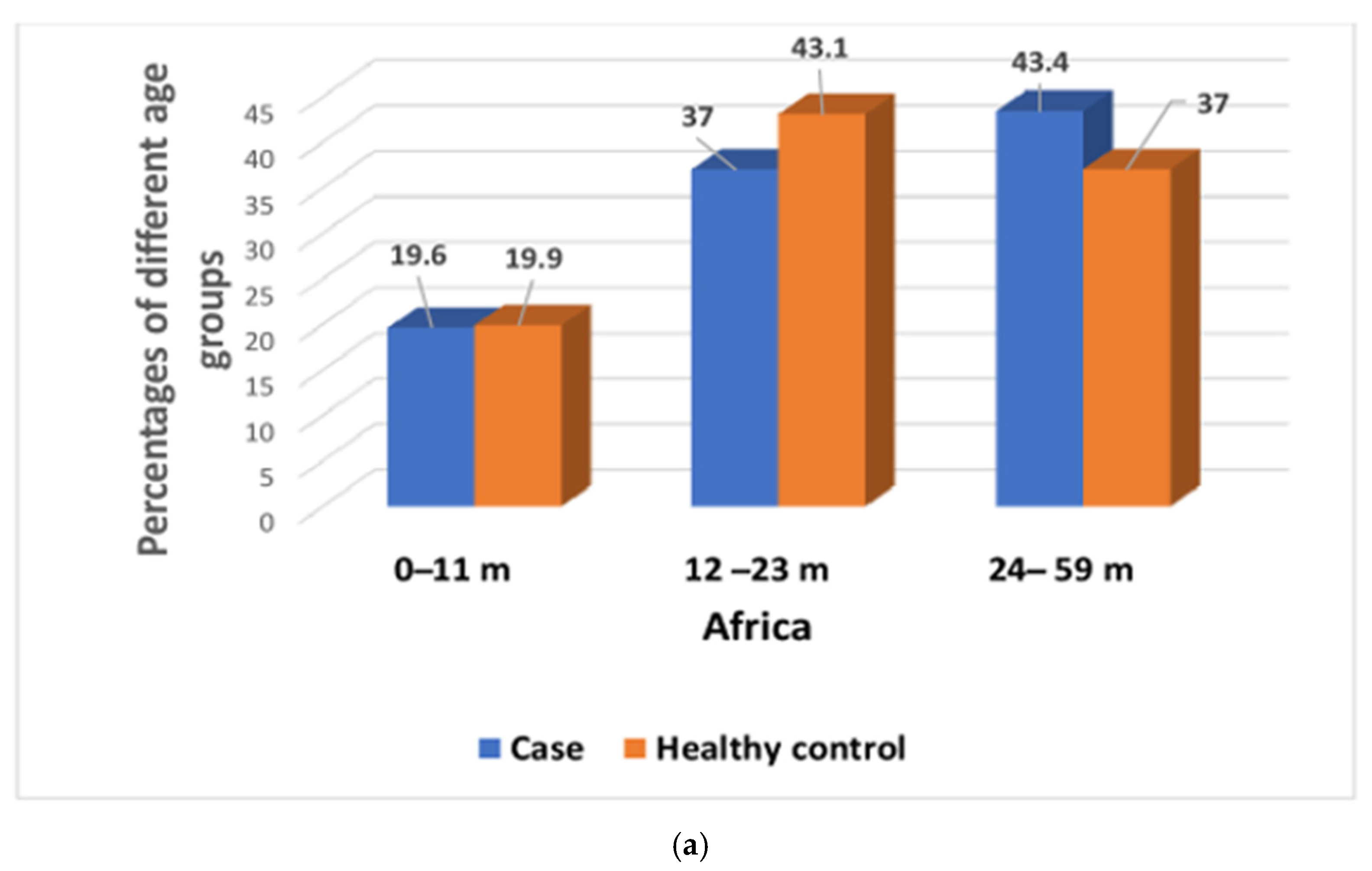
| 0–11 | 226 (19.6%) | 417 (19.9%) | 0.98 (0.82–1.17) | 0.884 |
| 12–23 | 426 (37.0%) | 902 (43.1%) | 0.77 (0.66–0.90) | 0.0001 |
| 24–59 | 499 (43.4%) | 775 (37.0%) | 1.30 (1.12–1.50) | 0.001 |
| Sex of the participants | ||||
| Female | 537 (46.7%) | 933 (44.6%) | 1.08 (0.94–1.25) | 0.265 |
| Wealth quintile | ||||
| Rich | 706 (61.3%) | 1188 (56.8%) | 1.20 (1.04–1.40) | 0.012 |
| Poor | 445 (38.7%) | 905 (43.2%) | 0.83 (0.71–0.96) | 0.012 |
| Source of water | ||||
| Deep tube well | 1141 (99.1%) | 2077 (99.2%) | 0.93 (0.43–2.04) | 0.975 |
| Shallow tube well | 10 (0.9%) | 17 (0.8%) | 1.07 (0.48–2.34) | 0.975 |
| Use treated water | ||||
| Yes | 246 (21.4%) | 358 (17.1%) | 1.31(1.09–1.57) | 0.003 |
| No | 905 (78.6%) | 1736 (82.9%) | ||
| Toilet facility | ||||
| Sanitary | 1086 (94.4%) | 1964 (93.8%) | 1.10 (0.81–1.50) | 0.571 |
| Non-sanitary | 65 (5.6%) | 130 (6.2%) | 0.90 (0.66–1.22) | 0.571 |
| Hand-washing practices: Before eating | ||||
| Yes | 1031 (89.6%) | 1935 (92.4%) | 0.70 (0.55–0.90) | 0.007 |
| No | 120 (10.4%) | 159 (7.6%) | ||
| Before cooking | ||||
| Yes | 624 (54.2%) | 1519 (72.5%) | 0.44 (0.38–0.52) | 0.001 |
| No | 527 (45.8%) | 575 (27.5%) | ||
| After defecation | ||||
| Yes | 804 (69.9%) | 1660 (79.3%) | 0.60 (0.51–0.71) | 0.001 |
| No | 347 (30.1%) | 434 (20.7%) | ||
| After cleaning the bottom of child following defecation | ||||
| Yes | 399 (34.7%) | 1129 (53.9%) | 0.45 (0.39–0.52) | 0.001 |
| No | 752 (65.3%) | 965 (46.1%) | ||
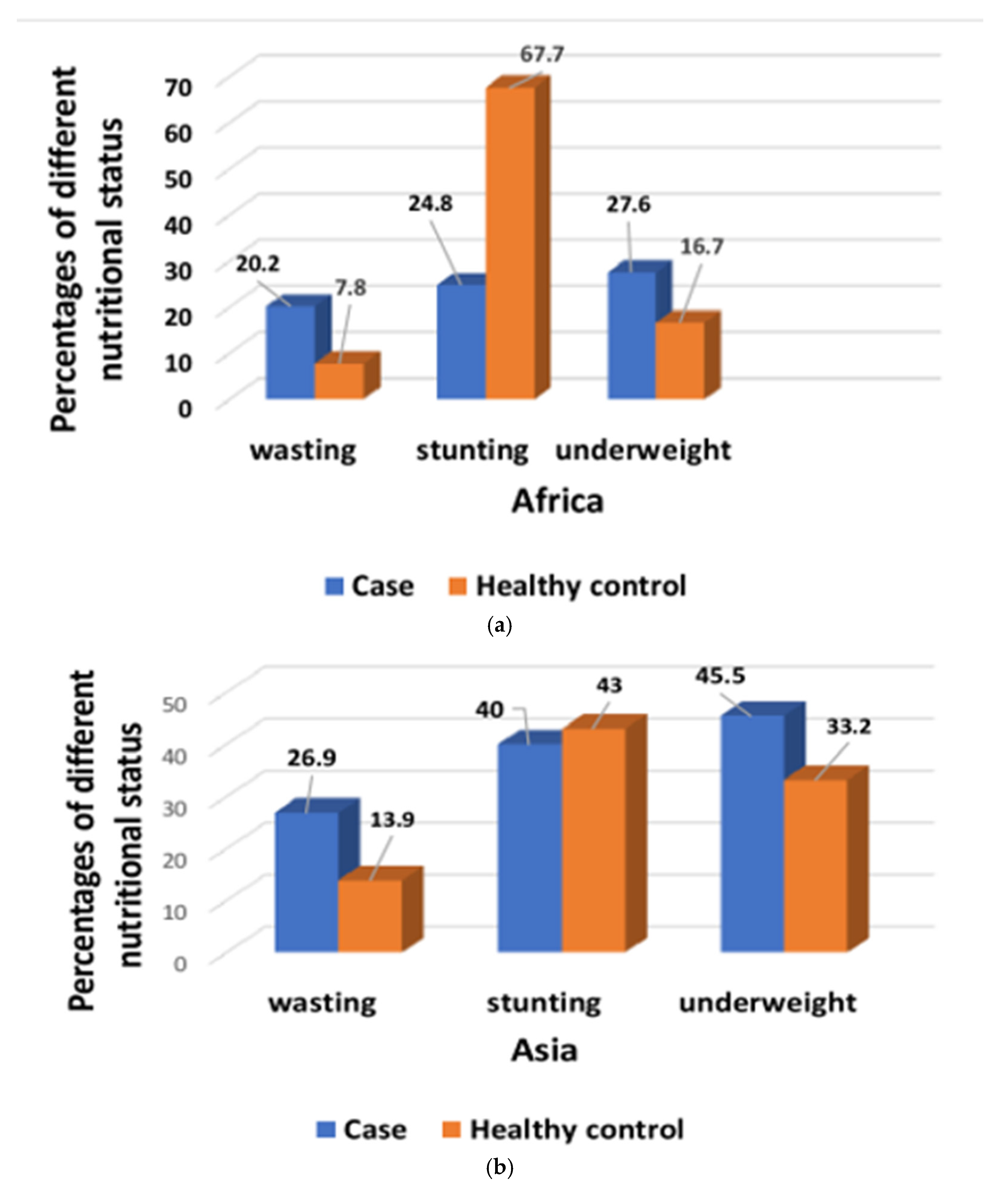
| Nutritional status: Wasting | ||||
| Yes | 232 (20.2%) | 163 (7.8%) | 2.99 (2.41–3.70) | 0.001 |
| No | 918 (79.8%) | 1927 (92.2%) | ||
| Stunting | ||||
| Yes | 285 (24.8%) | 597 (67.7%) | 0.82 (0.70–0.97) | 0.024 |
| No | 865 (75.2%) | 1496 (71.5%) | ||
| Underweight | ||||
| Yes | 318 (27.6%) | 350 (16.7%) | 1.90 (1.60–2.26) | 0.001 |
| No | 833 (72.4%) | 1743 (83.3%) | ||
| Indicators | Cases Giardia (n = 635) (%) | Healthy Controls Giardia (n = 1376) (%) | (Unadjusted) OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age of the participants in months | ||||
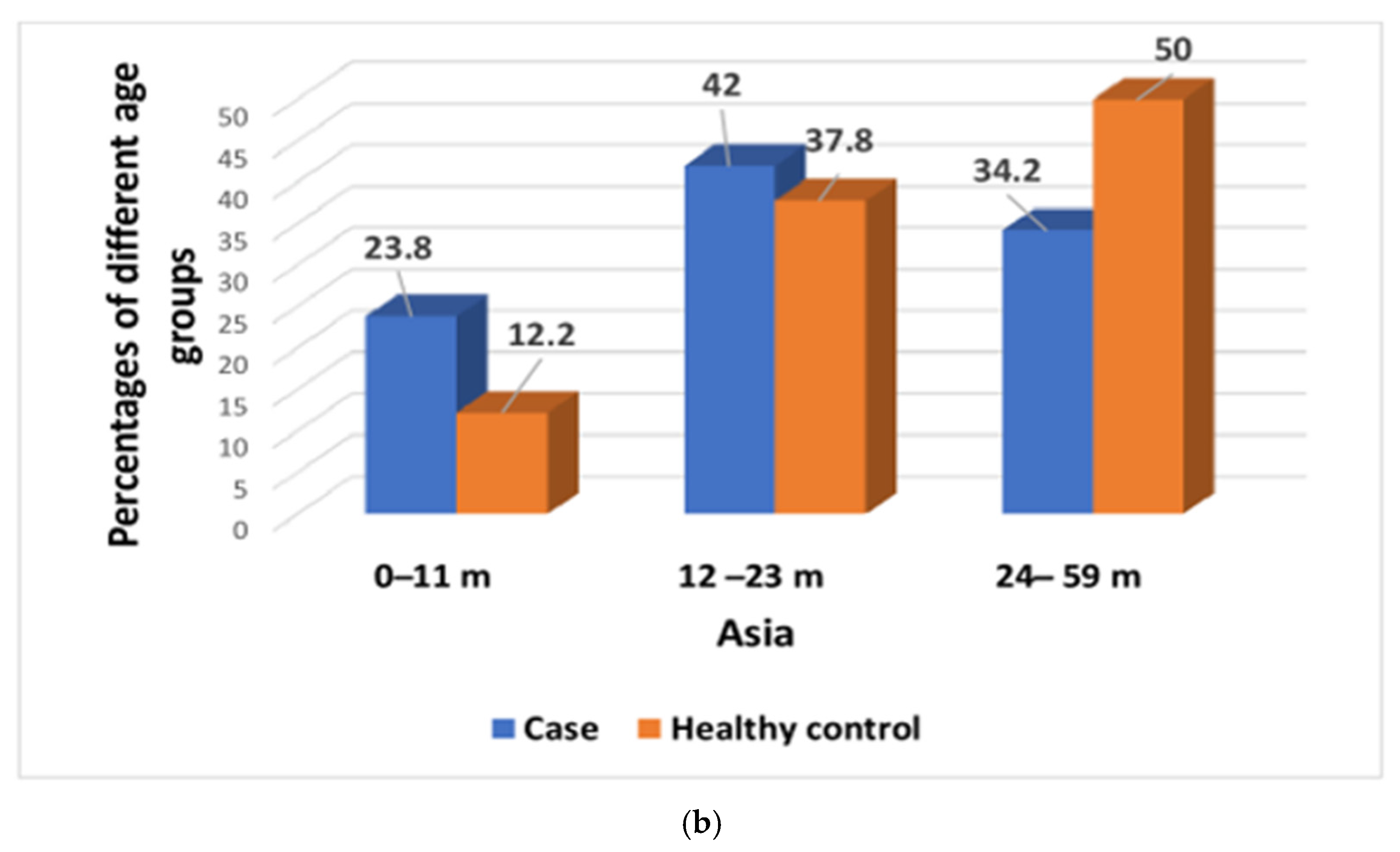
| 0–11 | 151 (23.8%) | 168 (12.2%) | 2.24 (1.75–2.86) | <0.001 |
| 12–23 | 267 (42.0%) | 520 (37.8%) | 1.19 (0.98–1.44) | 0.077 |
| 24–59 | 217 (34.2%) | 688 (50.0%) | 0.52 (0.43–0.63) | <0.001 |
| Sex of the participants | ||||
| Female | 286 (45.0%) | 584 (42.4%) | 1.11 (0.92–1.34) | 0.296 |
| Wealth quintile | ||||
| Rich | 331 (52.1%) | 838 (60.9%) | 0.69 (0.58–0.85) | 0.002 |
| Poor | 304 (47.9%) | 538 (39.1%) | 1.43 (1.18–1.73) | 0.002 |
| Source of water | ||||
| Deep tube well | 585 (92.1%) | 1222 (88.8%) | 1.47 (1.05–2.05) | 0.027 |
| Shallow tube well | 50 (7.9%) | 154 (11.2%) | 0.68 (0.48–0.95) | 0.027 |
| Use treated water | ||||
| Yes | 204 (32.1%) | 297 (21.6%) | 1.71 (1.39–2.12) | 0.001 |
| No | 431 (67.9%) | 1079 (78.4%) | ||
| Toilet facility | ||||
| Sanitary | 611 (96.2%) | 1306 (94.9%) | 1.36 (0.85–2.19) | 0.238 |
| Non-sanitary | 24 (3.8%) | 70 (5.1%) | 0.73 (0.45–1.17) | 0.238 |
| Hand-washing practices: Before eating | ||||
| Yes | 491 (77.3%) | 1037 (75.4%) | 1.11 (0.89–1.39) | 0.368 |
| No | 144 (22.7%) | 339 (24.6%) | ||
| Before cooking | ||||
| Yes | 466 (73.4%) | 990 (71.9%) | 1.07 (0.87–1.32) | 0.537 |
| No | 169 (26.6%) | 386 (28.1%) | ||
| After defecation | ||||
| Yes | 474 (74.6%) | 909 (66.1%) | 1.51 (1.22–1.86) | 0.001 |
| No | 161 (25.4%) | 467 (33.9%) | ||
| After cleaning the bottom of child following defecation | ||||
| Yes | 362 (57.0%) | 570 (41.4%) | 1.87 (1.55–2.26) | 0.001 |
| No | 273 (43.0%) | 806 (58.6) | ||
| Nutritional status: Wasting | ||||
| Yes | 171 (26.9%) | 191 (13.9%) | 2.22 (1.81–2.89) | 0.001 |
| No | 464 (73.1%) | 1182 (86.1%) | ||
| Stunting | ||||
| Yes | 254 (40.0%) | 591 (43.0%) | 0.89 (0.73–1.07) | 0.231 |
| No | 381 (60%) | 783 (57.0%) | ||
| Underweight | ||||
| Yes | 289 (45.5%) | 457 (33.2%) | 1.68 (1.39–2.03) | 0.001 |
| Indicators Africa | Asia | |||||
|---|---|---|---|---|---|---|
| Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | |
| Age group (0–11 m) | (Reference group) | |||||
| Age group (24–59 m) | 0.79 | (0.63–0.98) | 0.026 | 2.41 | (1.81–3.22) | <0.001 |
| Age group (12–23 m) | 0.70 | (0.62–0.89) | <0.001 | 1.49 | (1.20–1.86) | <0.001 |
| Wealth quintile, poor | 0.80 | (0.69–0.93) | 0.006 | 1.52 | (1.23–1.88) | <0.001 |
| Use treated water | - | - | - | 0.66 | (0.51–0.82) | <0.001 |
| Handwashing before eating | 1.42 | (1.10–1.86) | 0.008 | - | - | - |
| Handwashing before cooking | 2.11 | (1.80–2.46) | <0.001 | - | - | - |
| Handwashing after defecation | 1.23 | (1.03–1.48) | 0.021 | 0.68 | (0.53–0.84) | <0.001 |
| Handwashing after cleaning the bottom of the child following defecation | 2.06 | (1.76–2.41) | <0.001 | 0.59 | (0.48–0.72) | <0.001 |
| Wasting | 2.60 | (1.96–3.46) | <0.001 | 1.69 | (1.26–2.27) | <0.001 |
| Stunting | 0.66 | (0.53–0.80) | <0.001 | 0.66 | (0.51–0.84) | <0.001 |
| underweight | 1.57 | (1.20–2.03) | <0.001 | 1.72 | (1.30–2.30) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaima, S.N.; Das, S.K.; Ahmed, S.; Jahan, Y.; Khan, S.H.; Mamun, G.M.S.; Shahid, A.S.M.S.B.; Parvin, I.; Ahmed, T.; Faruque, A.S.G.; et al. Anthropometric Indices of Giardia-Infected Under-Five Children Presenting with Moderate-to-Severe Diarrhea and Their Healthy Community Controls: Data from the Global Enteric Multicenter Study. Children 2021, 8, 1186. https://doi.org/10.3390/children8121186
Shaima SN, Das SK, Ahmed S, Jahan Y, Khan SH, Mamun GMS, Shahid ASMSB, Parvin I, Ahmed T, Faruque ASG, et al. Anthropometric Indices of Giardia-Infected Under-Five Children Presenting with Moderate-to-Severe Diarrhea and Their Healthy Community Controls: Data from the Global Enteric Multicenter Study. Children. 2021; 8(12):1186. https://doi.org/10.3390/children8121186
Chicago/Turabian StyleShaima, Shamsun Nahar, Sumon Kumar Das, Shahnawaz Ahmed, Yasmin Jahan, Soroar Hossain Khan, Gazi Md. Salahuddin Mamun, Abu Sadat Mohammad Sayeem Bin Shahid, Irin Parvin, Tahmeed Ahmed, A. S. G. Faruque, and et al. 2021. "Anthropometric Indices of Giardia-Infected Under-Five Children Presenting with Moderate-to-Severe Diarrhea and Their Healthy Community Controls: Data from the Global Enteric Multicenter Study" Children 8, no. 12: 1186. https://doi.org/10.3390/children8121186
APA StyleShaima, S. N., Das, S. K., Ahmed, S., Jahan, Y., Khan, S. H., Mamun, G. M. S., Shahid, A. S. M. S. B., Parvin, I., Ahmed, T., Faruque, A. S. G., & Chisti, M. J. (2021). Anthropometric Indices of Giardia-Infected Under-Five Children Presenting with Moderate-to-Severe Diarrhea and Their Healthy Community Controls: Data from the Global Enteric Multicenter Study. Children, 8(12), 1186. https://doi.org/10.3390/children8121186