
Digital Technologies for Children and Parents Sharing Self-Management in Childhood Chronic or Long-Term Conditions: A Scoping Review


{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Eligibility Criteria
3.1. Inclusion
- Children aged from 5–18 years with a long-term condition and parents of children from birth–18 years with a long-term condition.
- Since a focus of this review was digital apps, we chose a publication start date of 2003. This is when the 3G networks arrived in the United Kingdom [24]. Mobile apps required this network to function.
- All types of primary research studies that focused on using digital technology within self-management of physical long-term conditions by children and/or parents were considered for inclusion. We were interested in studies that explored how technologies may be used to develop self-management skills and knowledge to assist with self-management in our population group.
3.2. Exclusion
- Studies not reporting primary research were excluded
- Papers published prior to 2003 were excluded.
- Papers that were not written in the English language as we did not have the resources to translate papers into English.
- Studies that focused on children with cancer, mental health problems, learning disabilities and/or cognitive impairment were excluded due to resource limitations.
- All literature reviews, editorials, letters, conference papers and PhD theses.
3.3. Identifying Information Resources
3.3.1. Search Strategy
3.3.2. Selection of Information Sources
3.4. Quality Appraisal
3.5. Data Extraction, Charting and Synthesis
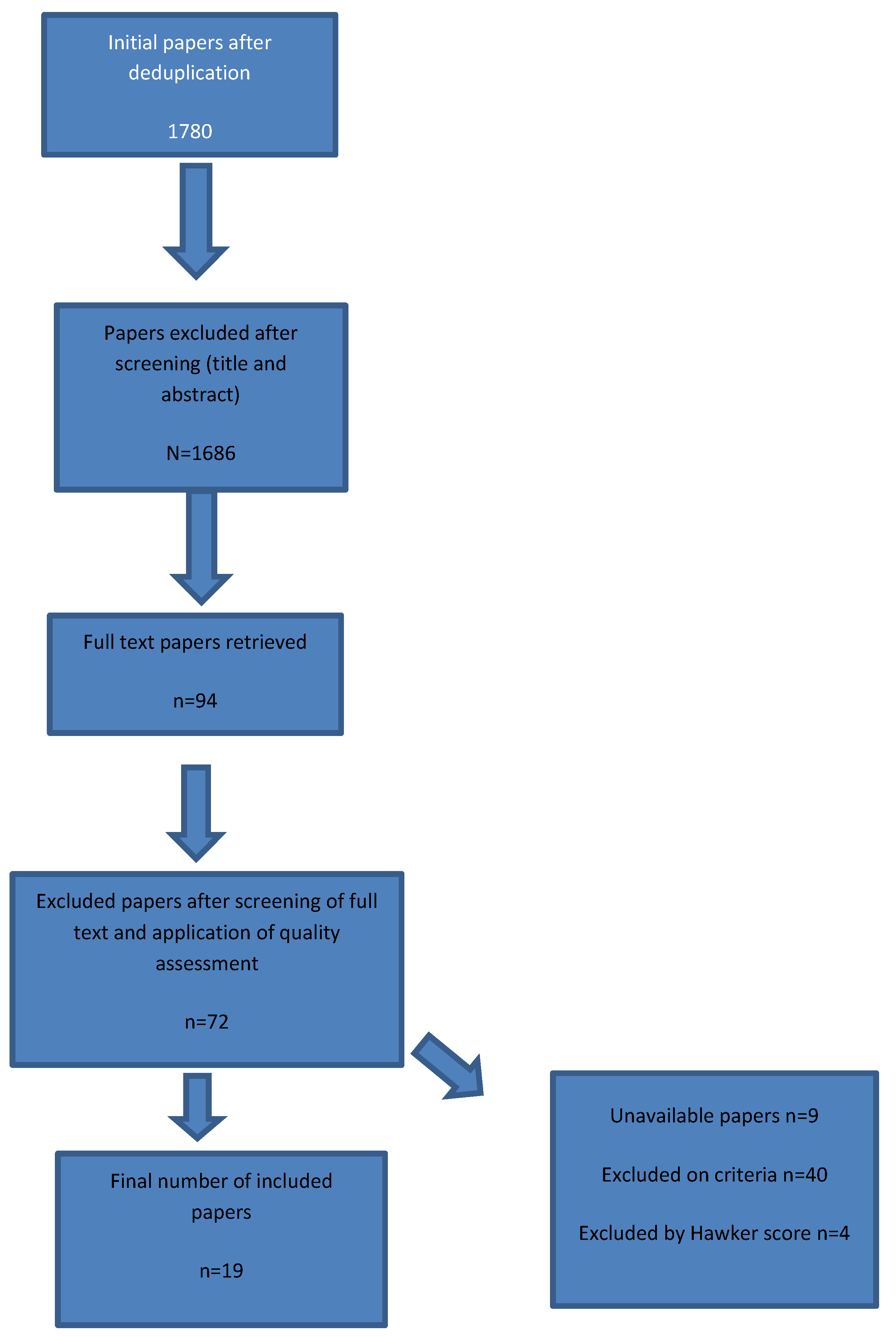
4. Results
4.1. Summary of Papers
4.2. Theme 1: The Feasibility and Acceptability of Using Technology
4.3. Theme 2: The Usability of Technologies
4.4. Theme 3: The Effect of Technologies on Adherence to Treatment Regimens and Improving Shared Self-Management Skills
5. Discussion
6. Strengths and Limitations
7. Future Research
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
| Query | Limiters/Expanders | |
| S45 | S7 AND S30 AND S41 AND S44 | Search modes—Boolean/Phrase |
| S44 | S42 OR S43 | Search modes—Boolean/Phrase |
| S43 | (MH “Self Care+”) | Search modes—Boolean/Phrase |
| S42 | TI “self help” or “self care” or “self manage *” | Search modes—Boolean/Phrase |
| S41 | S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 | Search modes—Boolean/Phrase |
| S40 | TX iPhone * or “mobile health” or digital or video * or game * or quiz * or blog * or twitter * or tweet * or Instagram or “social media” | Search modes—Boolean/Phrase |
| S39 | TX (smartphone * or phone * or ipad *) | Search modes—Boolean/Phrase |
| S38 | (MH “Smartphone+”) | Search modes—Boolean/Phrase |
| S37 | (MH “Computer Assisted Instruction”) | Search modes—Boolean/Phrase |
| S36 | TI (online or telemecidine) | Search modes—Boolean/Phrase |
| S35 | TX (mobile N2 device *) | Search modes—Boolean/Phrase |
| S34 | TI ((cell * or mobile *) N3 phone *) | Search modes—Boolean/Phrase |
| S33 | (MH “Social Media”) | Search modes—Boolean/Phrase |
| S32 | (MH “Computers, Hand-Held+”) | Search modes—Boolean/Phrase |
| S31 | (MH “Cellular Phone+”) | Search modes—Boolean/Phrase |
| S30 | S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 | Search modes—Boolean/Phrase |
| S29 | (MH “Chronic Disease”) | Search modes—Boolean/Phrase |
| S28 | TX long term condition * | Search modes—Boolean/Phrase |
| S27 | TI ((long-term or life-long or “long term” or “life long” or progressive or degenerative or non communicable or non-communicable) N2 (“health problem *” or illness * or condition * or disease * or disorder *)) | Search modes—Boolean/Phrase |
| S26 | TI (chronic * N1 (problem or illness * or condition * or disease * or disorder *)) | Search modes—Boolean/Phrase |
| S25 | TI ((chronic * or “long term” or long-term or life-long or “life long”) N1 pain) | Search modes—Boolean/Phrase |
| S24 | (MM “Chronic Pain”) | Search modes—Boolean/Phrase |
| S23 | (MM “Pain”) | Search modes—Boolean/Phrase |
| S22 | TX asthma * | Search modes—Boolean/Phrase |
| S21 | TX (epilepsy * or epileptic *) | Search modes—Boolean/Phrase |
| S20 | TX ((brain N2 (“cancer * or malignanc *” or neoplasm *or tumor *)) | Search modes—Boolean/Phrase |
| S19 | TX sarcoma * | Search modes—Boolean/Phrase |
| S18 | TX (haematologic * N2 (“cancer * or malignanc *” or neoplasm * or tumor *)) | Search modes—Boolean/Phrase |
| S17 | TX (hematologic * N2 (“cancer * or malignanc *” or neoplasm * or tumor *)) | Search modes—Boolean/Phrase |
| S16 | TX diabetes | Search modes—Boolean/Phrase |
| S15 | (MH “Status Asthmaticus”) | Search modes—Boolean/Phrase |
| S14 | (MH “Asthma, Exercise-Induced”) | Search modes—Boolean/Phrase |
| S13 | (MH “Asthma+”) | Search modes—Boolean/Phrase |
| S12 | (MH “Epilepsy+”) | Search modes—Boolean/Phrase |
| S11 | (MH “Neoplasms+”) | Search modes—Boolean/Phrase |
| S10 | (MH “Sarcoma+”) | Search modes—Boolean/Phrase |
| S9 | (MH “Hematologic Neoplasms+”) | Search modes—Boolean/Phrase |
| S8 | (MH “Diabetes Mellitus+”) | Search modes—Boolean/Phrase |
| S7 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 | Search modes—Boolean/Phrase |
| S6 | TX infant or infancy or infants or “young people” or “young person” or “young adult *” or “schoolchild *” or neonat * or preterm * or prematurity or postmature * or baby or babies or toddler * | Search modes—Boolean/Phrase |
| S5 | (MH “Child, Preschool”) | Search modes—Boolean/Phrase |
| S4 | (MH “Young Adult”) | Search modes—Boolean/Phrase |
| S3 | (MH “Pediatrics+”) | Search modes—Boolean/Phrase |
| S2 | (MH “Infant+”) | Search modes—Boolean/Phrase |
| S1 | TX (child or children or childhood or adolescen * or teen or teens or teenager * or youth or youths or girl or girls or boy or boys or p * ediatric * or juvenil *) | Search modes—Boolean/Phrase |
Appendix B. Characteristics of Papers
| Authors | Title of Paper | Population | Intervention | Control | Outcome | Design of Study | Hawker Tool Quality Assessment Total Score | Country | |
| 1 | Albanese-O’Neil, A, Schatz D.A, Bernhardt JM & Elder, JH. 2016 | Educational needs and technological preferences of Fathers of youth with type 1 Diabetes | Fathers of adolescents 6–17 years. | Identified the educational needs and technological preferences of fathers of youths. | No | Data supported feasibility/acceptability of diabetes education via mobile technology. Found interest in receiving education via smartphone technology. High levels of unmet needs in diabetes education. | mixed methods | 31 | USA |
| 2 | Borus JS, Blood E, Volkening LK, Laffel L & Shrier LA. 2013 | Momentary assessment of social context and glucose monitoring adherence with type 1 diabetes | 36 participants aged 14–18 years. Mean age 16.6. | Explored the association between sociocontextual factors and glucose level monitoring. | No | Identified some social influences on monitoring blood glucose. Found desire of individuals to blend in with friends may support glucose monitoring and desire to impress others may impede it. | Real time assessments | 24 | USA |
| 3 | Breakey VR, Ignas DM, Warias AV, White M, Blanchette VS & Stinson J. 2014 | A pilot randomized control trial to evaluate the feasibility of an internet-based self-management and transitional care program for youth with hemophilia | 29 participants. 13 –18 years. | Evaluate internet based self-management and transitional care program for hemophilia. | Yes | Significant improvements in knowledge in intervention group compared to control group. Web site found to be comprehensive and easy to use. Coach and weekly calls helped tailor learning to individual. | Feasibility (RCT) | 30 | Canada |
| 4 | Burbank AJ, Lewis SD, Hewes M, Schellhase DE, Rettiganti M, Hall-Barrow J, Bylander LA, Brown RH & Perry TT. 2015 | Mobile-based asthma action plans for adolescents | 20 participants. 13–18 years. | Examined feasibility and utilization of a mobile asthma action plan. | No | Utilization of mobile app by adolescents to deliver asthma action plan feasible. Asthma better controlled when app utilized. | Single-arm, feasibility and proof-of-concept study | 22 | USA |
| 5 | Carroll AE, Dimeglio LA, Stein S & Marrero DG. 2011 | Using a cell phone-based glucose monitoring system for adolescent diabetes management | 40 participants (36 completed study). 13–18 years. 19 girls and 20 boys. | Assess the feasibility of the combined phone and glucose meter system and the extent to which it would be acceptable to adolescents and parents. | No | The integrated phone and meter reported to be very useful and 75% of participates stated they would switch if available. Well-received by parents and adolescents. Using device increased knowledge and self-management. | Surveys | 22 | USA |
| 6 | Chan D, Callahan C, Sheets S, Moreno C & Malone F. 2003. | An Internet-based store-and-forward video home telehealth system for improving asthma outcomes in children | 10 participants 6–17 years. 5 boys and 5 girls. | Test feasibility and effectiveness of internet-based education programme versus office-based education. | No | Adherence and disease control. Compared office face to face consultations with video home tele system. Some connectivity issues reported due to technical problems in rural areas. Time-consuming method for health professionals. | Randomised study | 24 | USA |
| 7 | Clements MA & Staggs VS. 2017. | A Mobile App for Synchronizing Glucometer Data: Impact on Adherence and Glycemic Control Among Youths with Type 1 Diabetes in Routine Care | 81 participants 10–15 years Median age 14. 49% male | Whether mobile apps can improve self-management of glucose levels. Assessed impact of the frequency of glucometer-based data synchronization via a mobile app on HbA1c. | No | Found no statistical significance between rate of glucometer data synchronization and glucose control. Correlation to frequency of synchronization and monitoring of blood glucose. | Retrospective study/quantitative | 24 | USA |
| 8 | Gammon D, Arsand E, Walseth OA, Andersson N, Jenssen M, & Taylor T. 2005. | Parent-child interaction using a mobile and wireless system for blood glucose monitoring | 30 participants children and adolescents (aged 9–15 years. Boys n = 11 Girls n = 4) and their parent. Mothers 9 Fathers 1 15 families in total. | Testing of prototype designed to automatically transfer readings from child’s glucose meter to parents’ mobile phone. | No | Found self-management improvements of blood glucose levels and quality of life. Potential to increase pre-existing conflict between parents and children. Children concerned about increased parental surveillance. May be biased to those who are confident with technology | Pilot/mixed methods | 22 | Norway |
| 9 | Grey M, Whittemore R, Jeon S, Murphy K, Faulkner M & Delamater A. 2013 | Internet psycho-education programs to improve outcomes with type 1 diabetes | 320 participants 11–14 years. 55% female. | Comparison of two internet programmes on primary outcomes HbA1c and quality of life (QoL). | No | Adherence/QOL- compared two internet programmes to teach coping skills. QOL improved and HbA1c improved. Low income may affect engagement due to limited access to internet. | Clinical trial | 27 | USA |
| 10 | Han y, Faulker M, Fadoju D, Muir A, Abowd G, Head L & Arriaga R. 2015. | A Pilot Randomized Trial of Text-Messaging for Symptom Awareness and Diabetes Knowledge in Adolescents with Type 1 Diabetes | 30 participants aged 10–17 years (27 completed the study). Mean age 13.7%, 57% female | Piloting of text messages and examination of effects on symptom awareness and knowledge of diabetes. | Yes | Found some improvements in quality of life for adolescents in symptom awareness and knowledge (SK) group. No significant changes in QOL at baseline and follow up in control group and symptom (S) group. Diabetes quality of life for youth (DQOLY)- satisfaction did increase for S and SK groups. | Mixed methods | 22 | USA |
| 11 | Harris M, Freeman K & Duke D. 2015 | Seeing Is Believing: using Skype to Improve Diabetes Outcomes in Youth | 90 participants 12–18 years and their carers. Mean age of participants 15.04 and 55% male. Most carer mothers 76.7%. | Effectiveness of delivery of online behavioural family systems therapy (BFST) & glucose monitoring. Viable via video conferencing to address non-adherence. | No | Improvements found before and after the intervention and were maintained at 3 month follow up. BFST effective via video conferencing and Conventional method (i.e., in clinic setting). | Quantitative | 25 | USA |
| 12 | Hosseini A, Buonocore CM, Hashemzadeh S, Hojaul H, Kalantarian H, Sideris C, Bui AAT, King CE & Sarrafzadeh M.2017. | Feasibility of a Secure Wireless Sensing Smartwatch Application for the Self-Management of Pediatric Asthma | 2 participants. 1 child (7–12 years) and 1 adult | Assess whether a child could wear and use smartwatch app to alert to potential asthma attacks. | No | During feasibility testing, system able to accurately assess asthma risk in adult and during usability testing it was able to continuously collect data and alert to potential asthma attacks. Found child could wear smartwatch and understand alerts. | Feasibility | 22 | USA |
| 13 | Padman R, Jaladi S, Kim S, Kumar S, Orbeta P, Rudolph K & Tran T. 2013. | An evaluation framework and a pilot study of a mobile platform for diabetes self-management: insights from pediatric users | 8 participants. 10–18 years. | Evaluation of app for diabetes self-management | No | Found positive trends in user engagement and blood glucose variability. Increased satisfaction with diabetes management. Detected high variability in user’s interaction with application. | Evaluation | 23 | USA |
| 14 | Palermo T, Law E, Fales J, Bromberg M, Jessen-Fiddick T & Tai G. 2016. | Internet-delivered cognitive-behavioural treatment for adolescents with chronic pain and their parents: a randomized controlled multicentre trial | 273 adolescents aged 11–17 years and their parents | Comparison of internet delivered cognitive behavioural therapy and internet education. | Yes | Effectiveness of CBT treatment via internet. Reduction in depression, anxiety and self-blame. | Quantitative | 36 | USA |
| 15 | Palermo T, Wilson A, Peters M, Lewandowski A & Somhegyi H. 2009. | Randomized controlled trial of an Internet—delivered family cognitive-behavioral therapy intervention for children and adolescents with chronic pain | 48 participants children and adolescents aged 11–17 years & parents | Explored acceptability of internet CBT programme for children and parents. | Yes | Significantly greater reduction in activity limitations and pain intensity at post treatment for internet group and effects maintained after 3 months. Internet treatment acceptable to children and parents. | Quantitative | 35 | USA |
| 16 | Rhee H, Allen J, Mammen J & Swift M. 2014. | Mobile phone-based asthma self-management aid for adolescents (mASMAA): a feasibility study | 15 participants-dyads 9 males and 6 female 13–17 years 12 mothers | Development of self-management aid for adolescent with asthmas using texting feature. Feasibility and acceptability of mobile app for asthma self-management via text messaging. | No | Improved awareness of symptoms and five parents believed system useful and beneficial for those whose asthmas was not controlled well. General acceptable and feasible to use the app. Some difficulties in initial connection to system. | Qualitative | 36 | USA |
| 17 | St George SM, Delemater SM, Pulgaron ER, Daigre A & Sanchez J. 2016. | Access to and Interest in Using Smartphone Technology for the Management of Type 1 Diabetes in Ethnic Minority Adolescents and Their Parents | Participants 50 adolescents aged 11–16 (52% female) and 49 parents | Examined access and interest in using web based and smartphone technology for managing diabetes in ethnic minority adolescents. | No | Most participants reported high interest in using diabetes specific app. More parents than adolescents expressed interest in using it. Identified barriers to use but majority had access to smartphones and internet. | Quantitative | 32 | USA |
| 18 | Stinson J, McGrath P, Hodnett E, Feldman B, Duffy C, Huber A, Gtucker L, Hetherington R, Tse S, Spiegel L, Campillo S, Gill N & White M.2010. | Usability Testing of an Online Self-management Program for Adolescents with Juvenile Idiopathic Arthritis | 38 participants aged 12–18 years and parents. | Explored the usability of the self-management program for youth and parents. | No | Found adolescents more comfortable using computers than parents. Interactive features of program made them feel supported and not alone in coping with their illness. | Qualitative | 36 | Canada |
| 19 | Whittemore R, Grey M, Lindemann E, Ambrosino J & Jaser S. 2010. | Development of an Internet coping skills training program for teenagers with type 1 diabetes | 12 participants aged 13–16 years. Mean age 14.4 58% female. | Development of an internet coping skills training program | Yes | Found feasible and acceptance of internet coping skills training programme. Developing online resources complex and requires multi-disciplinary approach. Wide range of skills needed for coping, and email not good way to communicate with teens. | Mixed methods | 25 | USA |
References
- Chief Medical Officer. Annual Report of the Chief Medical Officer-Our Children Deserve Better: Prevention Pays; Department of Health: London, UK, 2012.
- Department of Health. Long Term Conditions Compendium of Information, 3rd ed.; Department of Health: London, UK, 2012. [Google Scholar]
- Nolte, E.; McKee, M. Caring for People with Chronic Conditions: A Health System Perspective; McGraw Hill/Open University Press: London, UK, 2008. [Google Scholar]
- Nolte, S.; Osborne, R.H. A systematic review of outcomes of chronic disease self-management interventions. Qual. Life Res. 2013, 22, 1805–1816. [Google Scholar] [CrossRef]
- Wong-Chung, R.; Willemen, A.; Voorman, J.; Ketelaar, M.; Becher, J.; Verheijden, J.; Schuengel, C. Managing oneself or managing together? Parents’ perspectives on chronic condition self-management in Dutch pediatric rehabilitation services. Disabil. Rehabil. 2020, 42, 3348–3358. [Google Scholar] [CrossRef] [Green Version]
- Camp-Spivey, L.J.; Logan, A.; Nichols, M. Theoretical and contextual considerations for self-management strategies of children and adolescents with chronic diseases: An integrative review. J. Child Health Care 2021, 29. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, R.; Friedl, S.; Swallow, V. Parents’ learning needs and preferences when sharing management of their child’s long-term/chronic condition: A systematic review. Patient Educ. Couns. 2015, 11, 1329–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijlaars, P.; Gilbert, R.; Hardelid, P. Chronic conditions in children and young people: Learning from administrative data. Arch. Dis. Child. 2016, 101, 881–885. [Google Scholar] [CrossRef] [Green Version]
- Knafl, K.; Deatrick, J.A.; Gallo, A.; Dixon, J.; Grey, M.; Knafl, G.; O’Malley, J. Assessment of the Psychometric Properties of the Family Management Measure. J. Pediatr. Psychol. 2011, 36, 494–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nightingale, R.; McHugh, G.; Kirk, S.; Swallow, V. Supporting children and young people to assume responsibility from their parents for the self-management of their long-term condition: An integrative review. Child Care Health Dev. 2019, 45, 175–188. [Google Scholar] [CrossRef]
- Swallow, V.; Carolan, I.; Smith, T.; Webb, N.J.; Knafl, K.; Santacroce, S.; Campbell, M.; Harper-Jones, M.; Hanif, N.; Hall, A. A novel Interactive Health Communication Application (IHCA) for parents of children with long-term conditions: Development, implementation and feasibility assessment. Inform. Health Soc. Care 2016, 41, 20–46. [Google Scholar] [CrossRef]
- Swallow, V.M.; Knafl, K.; Santacroce, S.; Campbell, M.; Hall, A.G.; Smith, T.; Carolan, I. An interactive health communication application for supporting parents managing childhood long-term conditions: Outcomes of a randomized controlled feasibility trial. JMIR Res. Protoc. 2014, 3, e69. [Google Scholar] [CrossRef]
- Blower, S.; Swallow, V.; Maturana, C.; Stones, S.; Phillips, R.; Dimitri, P.; Marshman, Z.; Knapp, P.; Dean, A.; Higgins, S.; et al. Children and young people’s concerns and needs relating to their use of health technology to self-manage long-term conditions: A scoping review. Arch. Dis. Child. 2020, 105, 1093–1104. [Google Scholar] [CrossRef]
- Savage, E.; Beirne, P.V.; Chroinin, M.N.; Duff, A.; Fitzgerald, T.; Farrell, D. Self-management education for cystic fibrosis. Cochrane Database Syst. Rev. 2014, 9. [Google Scholar] [CrossRef] [Green Version]
- Theng, Y.L.; Lee, J.W.Y.; Patinadan, P.V.; Foo, S.S.B. The use of videogames, gamification, and virtual environments in the self-management of diabetes: A systematic review of evidence. Games Health J. 2015, 4, 352–361. [Google Scholar] [CrossRef]
- Huby, K.; Swallow, V.; Smith, T.; Carolan, I. Children and young people’s views on access to a web-based application to support personal management of long-term conditions: A qualitative study. Child Care Health Dev. 2017, 43, 126–132. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, S.; Kingsnorth, S.; Mcdougall, C.; Keating, H. A systematic review of self-management interventions for children and youth with physical disabilities. Disabil. Rehabil. 2014, 36, 276–288. [Google Scholar] [CrossRef] [Green Version]
- Lozano, P.; Houtrow, A. Supporting self-management in children and adolescents with complex chronic conditions. Pediatrics 2018, 141 (Suppl. 3), S233–S241. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Henning, P.; Wong, G.; McTaggart, S.; Mackie, F.; Carroll, R.P.; Craig, J.C. Experiences and perspectives of adolescents and young adults with advanced CKD. Am. J. Kidney Dis. 2013, 61, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, R.; Hall, A.; Gelder, C.; Friedl, S.; Brennan, E.; Swallow, V. Desirable Components for a Customized, Home-Based, Digital Care-Management App for Children and Young People With Long-Term, Chronic Conditions: A Qualitative Exploration. J. Med. Internet Res. 2017, 19, e235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nightingale, R.; Wirz, L.; Cook, W.; Swallow, V. Collaborating with parents of children with chronic conditions and professionals to design, develop and pre-pilot PLAnT (the Parent Learning Needs and Preferences Assessment Tool). J. Pediatr. Nurs. 2017, 35, 90–97. [Google Scholar] [CrossRef]
- Birkhoff, S.D.; Smeltzer, S.C. Perceptions of Smartphone User-Centered Mobile Health Tracking Apps Across Various Chronic Illness Populations: An Integrative Review. J. Nurs. Scholarsh. 2017, 49, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Grundy, Q.H.; Wang, Z.; Bero, L.A. Challenges in Assessing Mobile Health App Quality: A Systematic Review of Prevalent and Innovative Methods. Am. J. Prev. Med. 2016, 51, 1051–1059. [Google Scholar] [CrossRef]
- Majeed-Ariss, R.; Baildam, E.; Campbell, M.; Chieng, A.; Fallon, D.; Hall, A.; McDonagh, J.E.; Stones, S.R.; Thomson, W.; Swallow, V. Apps and adolescents: A systematic review of adolescents’ use of mobile phone and tablet apps that support personal management of their chronic or long-term physical conditions. J. Med. Internet Res. 2015, 17, e287. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Perez, B.; de la Torre-Diez, I.; Lopez-Coronado, M.; Sainz-de-Abajo, B.; Robles, M.; Garcia-Gomez, J. Mobile clinical decision support systems and applications: A literature and commercial review. J. Med. Syst. 2014, 38, 4. [Google Scholar] [CrossRef] [PubMed]
- Pérez, Y.I.V.; Medlow, S.; Ho, J.; Steinbeck, K. Mobile and web-based Apps that support self-management and transition in young people with chronic illness: Systematic review. J. Med. Internet Res. 2019, 21, e13579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Mahmoud, Z.; Angelé-Halgand, N.; Churruca, K.; Ellis, L.A.; Braithwaite, J. The impact of lean management on frontline healthcare professionals: A scoping review of the literature. BMC Health Serv. Res. 2021, 21, 383. [Google Scholar] [CrossRef]
- Kim, K.-J.; Choi, M.-J.; Kim, K.-J. Effects of Nursing Simulation Using Mixed Reality: A Scoping Review. Healthcare 2021, 9, 947. [Google Scholar] [CrossRef] [PubMed]
- Hawker, S.; Payne, S.; Kerr, C.; Hardey, M.; Powell, J. Pearls, pith, and provocation. Appraising the evidence: Reviewing disparate data systematically. Qual. Health Res. 2002, 12, 1284–1299. [Google Scholar] [CrossRef]
- Skelton, B.; Knafl, K.; Van Riper, M.; Fleming, L.; Swallow, V. Care Coordination Needs of Families of Children with Down Syndrome: A Scoping Review to Inform Development of mHealth Applications for Families. Children 2021, 8, 558. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V.; Cooper, H. Thematic analysis. In APA Handbook of Research Methods in Psychology, Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological; Camic, P.M., Long, L.D., Panter, A.T., Rindskopf, D.E., Sher, K.J., Eds.; American Psychological Association: Washington DC, USA, 2012; Volume 2, pp. 57–71. [Google Scholar] [CrossRef]
- St. George, S.M.; Delamater, A.M.; Pulgaron, E.R.; Daigre, A.; Sanchez, J. Access to and interest in using smartphone technology for the management of type 1 diabetes in ethnic minority adolescents and their parents. Diabetes Technol. Ther. 2016, 18, 104–109. [Google Scholar] [CrossRef]
- Albanese-O’Neill, A.; Schatz, D.A.; Bernhardt, J.M.; Elder, J.H. Educational needs and technological preferences of fathers of youth with type 1 diabetes. Diabetes Educ. 2016, 42, 209–219. [Google Scholar] [CrossRef]
- Burbank, A.J.; Shannon, D.; Lewis, R.N.; Hewes, M.; Schellhase, D.E.; Rettiganti, M.; Hall-Barrow, J.; Bylander, L.A.; Brown, R.H.; Perry, T.T. Mobile-based asthma action plans for adolescents. J. Asthma 2015, 52, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Carroll, A.E.; DiMeglio, L.A.; Stein, S.; Marrero, D.G. Using a cell phone-based glucose monitoring system for adolescent diabetes management. Diabetes Educ. 2011, 37, 59–66. [Google Scholar] [CrossRef] [Green Version]
- Gammon, D.; Årsand, E.; Walseth, O.A.; Andersson, N.; Jenssen, M.; Taylor, T. Parent-child interaction using a mobile and wireless system for blood glucose monitoring. J. Med. Internet Res. 2005, 7, e57. [Google Scholar] [CrossRef]
- Grey, M.; Whittemore, R.; Jeon, S.; Murphy, K.; Faulkner, M.S.; Delamater, A. TeenCope Study Group; Internet psycho-education programs improve outcomes in youth with type 1 diabetes. Diabetes Care 2013, 36, 2475–2482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, Y.; Faulkner, M.S.; Frit, H.; Fadoju, D.; Muir, A.; Abowd, G.D.; Head, L.; Arriaga, R.I. A pilot randomized trial of text-messaging for symptom awareness and diabetes knowledge in adolescents with type 1 diabetes. J. Pediatr. Nurs. 2015, 30, 850–861. [Google Scholar] [CrossRef] [Green Version]
- Harris, M.A.; Freeman, K.A.; Duke, D.C. Seeing is believing: Using Skype to improve diabetes outcomes in youth. Diabetes Care 2015, 38, 1427–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseini, A.; Buonocore, C.M.; Hashemzadeh, S.; Hojaiji, H.; Kalantarian, H.; Sideris, C.; Bui, A.A.; King, C.E.; Sarrafzadeh, M. Feasibility of a secure wireless sensing smartwatch application for the self-management of pediatric asthma. Sensors 2017, 17, 1780. [Google Scholar] [CrossRef]
- Palermo, T.M.; Wilson, A.C.; Peters, M.; Lewandowski, A.; Somhegyi, H. Randomized controlled trial of an Internet-delivered family cognitive behavioral therapy intervention for children and adolescents with chronic pain. Pain 2009, 146, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Rhee, H.; Allen, J.; Mammen, J.; Swift, M. Mobile phone-based asthma self-management aid for adolescents (mASMAA): A feasibility study. Patient Prefer. Adherence 2014, 7, 63–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stinson, J.; McGrath, P.; Hodnett, E.; Feldman, B.; Duffy, C.; Huber, A.; Tucker, L.; Hetherington, R.; Tse, S.; Spiegel, L. Usability testing of an online self-management program for adolescents with juvenile idiopathic arthritis. J. Med. Internet Res. 2010, 12, e30. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Grey, M.; Lindemann, E.; Ambrosino, J.; Jaser, S. Development of an Internet coping skills training program for teenagers with type 1 diabetes. Comput. Inform. Nurs. 2010, 28, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breakey, V.R.; Ignas, M.; Warias, A.V.; White, M.; Blanchette, V.S.; Stinson, J.N. A pilot randomized control trial to evaluate the feasibility of an Internet-based self-management and transitional care program for youth with haemophilia. Haemophilia 2014, 20, 784–793. [Google Scholar] [CrossRef]
- Palermo, T.M.; Law, E.F.; Fales, J.; Bromberg, M.H.; Jessen-Fiddick, T.; Tai, G. Internet-delivered cognitive-behavioral treatment for adolescents with chronic pain and their parents: A randomized controlled multicenter trial. Pain 2016, 157, 174. [Google Scholar] [CrossRef] [PubMed]
- Clements, M.A.; Staggs, V.S. A mobile app for synchronizing glucometer data: Impact on adherence and glycemic control among youths with type 1 diabetes in routine care. J. Diabetes Sci. Technol. 2017, 11, 461–467. [Google Scholar] [CrossRef]
- Padman, R.; Jaladi, S.; Kim, S.; Kumar, S.; Orbeta, P.; Rudolph, K.; Tran, T. An evaluation framework and a pilot study of a mobile platform for diabetes self-management: Insights from pediatric users. Stud. Health Technol. Inform. 2013, 192, 333–337. [Google Scholar] [PubMed]
- Borus, J.S.; Blood, E.; Volkening, L.K.; Laffel, L.; Shrier, L.A. Momentary assessment of social context and glucose monitoring adherence in adolescents with type 1 diabetes. J. Adolesc. Health 2013, 52, 578–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, D.S.; Callahan, C.W.; Sheets, S.J.; Moreno, C.N.; Malone, F.J. An Internet-based store-and-forward video home telehealth system for improving asthma outcomes in children. Am. J. Health Syst. 2003, 60, 1976–1981. [Google Scholar] [CrossRef] [PubMed]
- Waite-Jones, J.; Swallow, V.; Smith, J.; Stones, S.; Majeed-Ariss, R.; van Rooyen, V. Developing a mobile-app to aid young people’s self-management of chronic rheumatic disease: A qualitative study. Rheumatology 2017, 56 (Suppl. 6), kex356.001. [Google Scholar] [CrossRef] [Green Version]
- Stein, R.E.K.; Jessop, D.J. A Non-Categorical Approach to Chronic Childhood Illness. Public Health Rep. 1982, 97, 354–362. [Google Scholar]
- Waite-Jones, J.; Majeed-Ariss, R.; Smith, J.; Stones, S.R.; van Rooyen, V.; Swallow, V. Young-people’s, parents’ and professionals’ views on required components of mobile applications to support self-management of chronic rheumatic disease: A qualitative study. JMIR mHealth uHealth 2017, 6, e25. [Google Scholar] [CrossRef] [PubMed]
- Office of National Statistics. Exploring the UK’s Digital Divide: The Scale of Digital Exclusion in the UK; Those Who Aren’t Currently Using the Internet, How Digital Skills Vary for Different Groups of the Population and Some of the Barriers to Digital Inclusion. 2019. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/householdcharacteristics/homeinternetandsocialmediausage/articles/exploringtheuksdigitaldivide/2019-03-04 (accessed on 19 March 2021).
- Social Metrics Commission. Measuring Poverty. 2019. Available online: https://socialmetricscommission.org.uk/wp-content/uploads/2019/07/SMC_measuring-poverty-201908_full-report.pdf (accessed on 7 December 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edwards, J.; Waite-Jones, J.; Schwarz, T.; Swallow, V. Digital Technologies for Children and Parents Sharing Self-Management in Childhood Chronic or Long-Term Conditions: A Scoping Review. Children 2021, 8, 1203. https://doi.org/10.3390/children8121203
Edwards J, Waite-Jones J, Schwarz T, Swallow V. Digital Technologies for Children and Parents Sharing Self-Management in Childhood Chronic or Long-Term Conditions: A Scoping Review. Children. 2021; 8(12):1203. https://doi.org/10.3390/children8121203
Chicago/Turabian StyleEdwards, Jill, Jenny Waite-Jones, Toni Schwarz, and Veronica Swallow. 2021. "Digital Technologies for Children and Parents Sharing Self-Management in Childhood Chronic or Long-Term Conditions: A Scoping Review" Children 8, no. 12: 1203. https://doi.org/10.3390/children8121203
APA StyleEdwards, J., Waite-Jones, J., Schwarz, T., & Swallow, V. (2021). Digital Technologies for Children and Parents Sharing Self-Management in Childhood Chronic or Long-Term Conditions: A Scoping Review. Children, 8(12), 1203. https://doi.org/10.3390/children8121203