
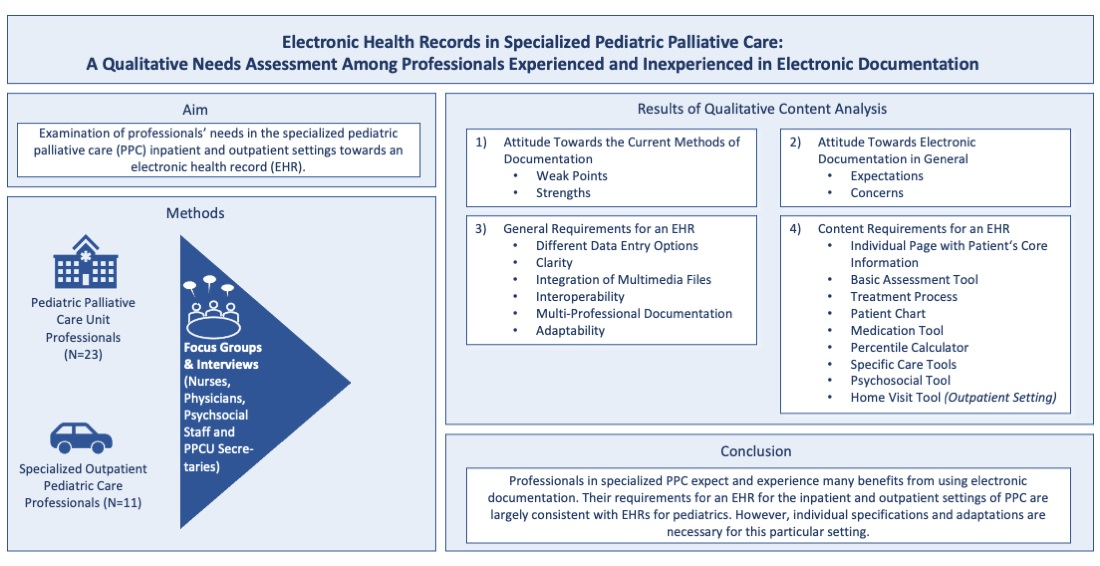
Electronic Health Records in Specialized Pediatric Palliative Care: A Qualitative Needs Assessment among Professionals Experienced and Inexperienced in Electronic Documentation

 , ,
, ,  ,
, 

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants and Recruitment
2.3. Data Collection
- Which are the greatest strengths and weak points of the currently used type of record (paper record/EHR for adult palliative care patients)?
- What are your wishes for and concerns about EHRs in general?
- We would like to go through the currently used paper records/EHRs for adult palliative care patients:
- ◦
- Which components do you generally like? And why?
- ◦
- Which components would you like to see incorporated into the new system? And why?
- ◦
- Which components would you like to be revised before being incorporated into the new system, e.g., concerning content, structure, and design?
- ◦
- Which new components would you like to add to the new system? What would they look like specifically?
2.4. Data Analysis
2.5. Ethical Approval
3. Results
3.1. Attitude towards the Current Methods of Documentation
3.1.1. Weak Points
“I’m searching for a document and at first I think ‘oh no, it’s missing’, but then I see that it was misfiled.”(FG_PPCU_Secretary_01:50-55)
“So, in [place] for example, it takes a very long time to boot, or in [place] I couldn’t access [the EHR; D.M.] because it took so long. When you need information quickly, that’s obviously difficult.”(I_SOPPC_Nurse_02:83)
“Well, because it crashes from time to time, and then you get kicked out with only half of your document […] And that’s why, as a precaution, we always document in [word processing program; D.M.].”(I_SOPPC_Psychosocial_01:55)
3.1.2. Strengths
“In fact, the greatest strength is that it is web-based. That you can actually easily access the data stored there from anywhere. That means, on every car journey to the family, on every home visit to the families, that you always can find something quickly. Even if it is just the insurance number or whatever. I think that is the greatest strength.”(I_SOPPC Nurse_03:13)
3.2. Attitude towards Electronic Documentation in General
3.2.1. Expectations
“I think about having nightshift in the hospital […] in the middle of the night, an ambulance and an emergency physician arrive and say: ‘Here is a child known in your PPCU […]’, but they did not bring any documents from the child’s home. Then I don’t know the medication.”(FG_PPCU_Physician_01:231-242)
“Perhaps the ladies of the coding department, they also browse through everything that could be relevant to them, what can still be billed. And if there are clear things where they just have to check up […] then this would accelerate the workflow; that there is a link, that they no longer have to search for everything they need […].”(FG_PPCU_Secretary_01:173)
3.2.2. Concerns
“To be honest, all of us in the team took it like this: ‘here comes something new again’. We have just managed to get used to something. I don’t know if the wish was that we needed something completely new. We would rather have wished that more of the wishes we had worked out together would gradually be adopted.”(I_ SOPPC_Physician_05:38)
“My only fear is that all the things that […] we have brought up to certain people again and again are simply not taken seriously and are not going to be implemented, right? […] So, I think it would be desirable […] if the perspectives of various professional groups were taken seriously. And actually, would simply be checked for practicability and then, if necessary, integrated or not, if they are simply not practicable.”(I_ SOPPC_Nurse_03:151)
3.3. General Requirements for an EHR
3.3.1. Different Data Entry Options
“[…] for us in nursing, some things cannot be well documented, in my opinion. Because there aren’t any structured forms behind it. If it somehow relates to wound management or tracheostomy care or in the direction of secretion management, there we still write a lot of running text. I think it would make it easier […] to have one short dataset to deposit [this information; D.M.].”(I_SOPPC_Nurse_03:29)
3.3.2. Clarity
“I think we will create sets […] such as a view for spastic and one for patients suffering from pain. But too many different views will become difficult. […] However, if these could be modified […].”(FG_PPCU_Physician_01:415-421)
“And especially in terminal care, there is so much going on […] that we would need to spread documentation space, so that everything we do could be documented.”(FG_PPCU_Physician_01:305)
“If you are looking for something specific, the filters and search functions are not super convenient. It is sometimes a bit difficult to find exactly what you are looking for. Someone called a few weeks ago and said that it was not easy. So, things like that, they get you bogged down quickly because there are too many levels.”(I_SOPPC_Physician_02:11)
3.3.3. Integration of Multimedia Files
“We do that often; videos about seizures, agitation. Maybe about [social; D.M.] interactions.”(FG_PPCU_Psychosocial_01:240)
3.3.4. Interoperability
“Basically, you need a system–these are patients who come and go. Sometimes they are inpatient, sometimes outpatient, then they are x-rayed, then they have laboratory tests, then they have microbiological tests, then there are genetic findings, and everything has to be merged in a meaningful way. That would be very desirable in that it becomes superfluous to transfer patients from one system to the other just as it is superfluous to log into other systems.”(I_SOPPC_Physician_04:85)
“[…] that a prescription is made here but ends up automatically–without requiring a fax or e-mail–at the relevant pharmacies.”(I_SOPPC_Physician_05:63)
3.3.5. Multi-Professional Documentation
“We work together in a multi-professional team and speak often […], but somehow our documentation is so extremely separate from each other.”(FG_PPCU_Psychosocial_01:31)
“Is there an option where all relevant information from all three professions could converge in one document? That would actually reflect it best. And where, perhaps, the least amount of information would be lost.”(FG_PPCU_Psychosocial_01:258)
3.3.6. Adaptability
“[…] how well can new systems or other documents, beyond a PDF, also be implemented? How flexible is the record when developing future documentation systems?”(FG_PPCU_Physician_01:92)
3.4. Content Requirements for an EHR
3.4.1. Individual Page with Patient’s Core Information
“It should note ‘guardian so and so’, contact person and phone number, and place of residence. […] I would actually put a genogram on it. You could also see diagnosis, name, place of residence, SOPPC, grade level, school. […] When you open that view, you have everything at a glance. And then, if you want to know more details you can search for healthcare providers, pharmacies, I don’t know, even speech therapy, occupational therapy.”(I_SOPPC_Psychosocial_01:13)
3.4.2. Basic Assessment Tool
“That means I simply need to extract a few other parameters for this patient group; how does he communicate, and so on […].”(FG_PPCU_Physician_01:540)
“But, for example, you could also go into detail by saying something like ‘can distinguish light and dark’ or ‘turns his head when noticing light and dark’.”(FG_PPCU_Psychosocial:119)
“I think, with all these templates, it´s still a little bit oriented towards an adult system. With regard to advance care planning, health care proxy, care proxy, who is entitled to care, for example, we write in the free text fields. That is not listed in detail.”(I_SOPPC_Physician_05:48)
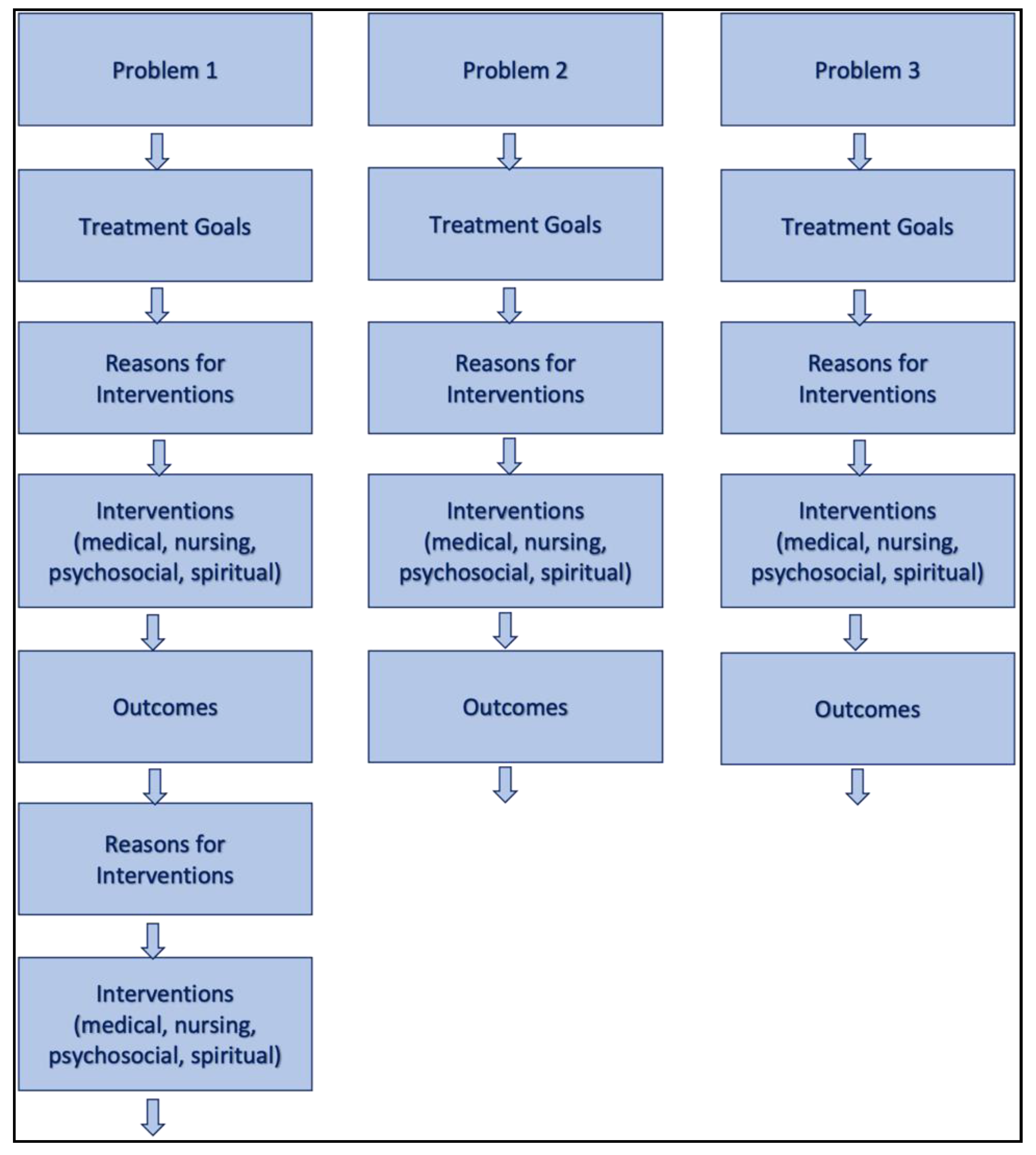
3.4.3. Treatment Process
“[…] a process documentation, that shows–apart from daily documentation–a summary of the entire process. That would be an advantage […] in case of readmission, to understand why we made that decision at the time.”(FG_PPCU_Physician_01:125)
“[…] What we always want is to have an overview; what are the symptoms? What are the orders? What has happened in terms of interventions? We accompany many families over many years, then they come for the second, third, fourth–whatever–time. So that one does not lose so much [information; D.M.] from the previous stays. But that you somehow have an overview, a kind of overview sheet, which is always immediately transferred to the next stay so that you can refer to it. Something clear, where the most important things are on it, so to speak. What one has is immediately presented again at the next stay.”(FG_PPCU_Psychosocial_01:38)
“P3: We accomplish most symptom control via phone. We are on a home visit, hear about it, tell the parents to ‘do this and that’, and call […] one, two, three, five days later to hear whether the interventions […] had any effect […]. I would really like to have an overview for each child; these are the painful symptoms, this was once the leading symptom, we made these interventions and the symptoms improved. […]
P1: Yes, I think that’s good, too. The distressing symptoms and then which interventions were made.”(FG_SOPPC_Nurse_01:31-32)
3.4.4. Patient Chart
“P2: So, when a symptom is mentioned and the nurse says ‘today he has so much secretion again’, we really think on three levels. We think medically, […] we think, maybe he has an infection now. We think which nurse has not positioned him properly […] so that it can drain. Maybe inhalations have been forgotten. He got so upset because his mother went home and he is breathing stertorously with more secretions again. So, if this concern arises…
P8: This complexity […]
P2: Exactly, represents.”(FG_PPCU_Physician_01:147-149)
“The documentation of observed behavior is often an issue. […] If you want to analyze agitation for instance, […] is it pain? […] Is it an interaction, boredom, whatever? That doesn´t work here.”(FG_PPCU_Psychosocial_01:190-196)
“We don’t even have any progress documentation right now [in the adult EHR; D.M.]. That means we just have a list of things, but no patient chart like in the inpatient settings. To be able to depict something over an entire day […]. that you can see one, two, three days next to each other […] so that you somehow have a short summary of the day above, perhaps including vital signs so that you get an overview of how the patient was, so to speak. I would find that quite useful.”(I_SOPPC_Physician_02:25)
3.4.5. Medication Tool
“The most important thing for me of course is the medication plan. It has to work one hundred percent. And that is also a document that we hand to the families, […] so that is important.”(I_SOPPC_Physician_03:11)
“Then the order, as I said. Somehow it happens that at some point the laxative is at the top [of the list; D.M.] and the strong analgesic in the middle. We would like to give out medication plans that are clearly arranged for the family. […] It would also be good if you could pull it by hand. […] That would be a help.”(I_SOPPC_Physician_03:19)
“Also, the different times could be clearer. It is different with adults. There is morning, noon, evening and maybe night. We sometimes have ten different times. And then it becomes confusing.”(FG_SOPPC_Nurse_01:156)
“Most of the patients don’t have just one drug, but rather 15 to 20. Then you are quite busy already. Somehow finding a consistent structure, […] I think it’s important. So that it is somehow a little bit better specified; […] first active ingredient, then application form, […] concentration or similar.”(I_SOPPC_Physician_02:41)
“Yes, there are 13 drops, three fixed administrations; that is three times 13 drops. Because that is what is important for the mother, who gives drops, not milligrams […]”.(I_SOPPC_Physician_02:37)
“And when I stop, it looks like this. That’s not very good either. If I delete it now, there will be no confirmation.”(I_SOPPC_Physician_02:41)
“Especially with children it is important to determine in how much volume it is administered. Sometimes ten milligrams are in five milliliters, but you can also have it in a hundred milliliters and that sometimes makes a difference for children. […] So i.v. or per os or in the buttocks and then at what times, […] what certain running speed. […] What the doctors […] strive for is the dose and that means the mass of the substance that the child should receive per kilo or per square meter [of the body surface; D.M.]. The most common is per kilo, but there are also situations where this is related to the body surface. And you can’t enter that here.”(I_SOPPC_Physician_04:26)
“It would also be nice if you had something about on-demand medication, where with the individual drugs you can say ‘it has been administered three times during the last 24 hours’, or ‘not at all’, or something. […] Of course, you can also indicate it in the free text, but then you have to search again to see if that was somehow an issue.”(I_SOPPC_Physician_03:19)
“[…] in this unit, there are patients who weigh 12 kilos at the age of 18”(FG_PPCU_Physician_01:653)
“Actually, you would like to have a system that supports you in calculating. Those are quite simple calculations; everyone can do them if they have time and are relaxed. But then you get three, four in a row. If you do this under time pressure or if you are stressed […], then mistakes happen quite regularly. […] And if you use software that somehow maps the medication process, then it is extremely desirable that you have a calculation aid.”(I_SOPPC_Physicians_04:28)
3.4.6. Percentile Calculator
“That would also be good if it could be done automatically. You enter the length and size and it automatically inserts this into the percentile curve.”(FG_PPCU_Nurse_02:179)
“There are things like percentiles, […] in other words, peculiarities that software developers never think of in children. […] to see are they properly nourished? Are they growing normally?”(I_SOPPC_Physician_04:100)
3.4.7. Specific Care Tools
“[…] for example, the breathing rate and oxygen saturation are queried, but it does not appear anywhere how much oxygen the patient currently needs and is being given. And that would be nice to be able to do somehow, put a tick next to the vital signs or something, whether it is a ventilated patient or not […]. Otherwise, such vital signs are sometimes not that informative.”(I_SOPPC_Nurse_03:35)
“Right now, yes, we have to look for a lot in the running text, so to speak. Like when colleague XY […] was with the family, then I have to look for when was she with the family and what did she notice, right? Did the stoma look good at that particular moment, or was there a high need for aspiration or not? And was the secretion yellowish because perhaps somehow there is an infection going on? Yes, something like that. Also for chronic wounds.”(I_SOPPC_Nurse_03:67-69)
“Like I said, we are missing an input screen for the NCP. Right now, the way we do it is we write an NCP as a (word processing program) document and then of course you have the option of uploading that, which is good, but of course it would be nice if that was a direct feature within the system.”(I_SOPPC_Nurse_02:45)
3.4.8. Psychosocial Tool
“I think that would be very good, then you have everything in one place that is psychosocial.”(FG_PPCU_Psychosocial_01:131)
3.4.9. Home Visit Tool
“But the documentation of symptoms also does not provide what is needed in pediatric care. We document an incredible amount in the comment field again in free text. […] I don’t know […] because people like to write a lot anyway […] or if the tools are missing where you can document so it’s a bit more standardized […] But most of it is still done in the comment field. And I think that’s always a sign that the other categories don’t allow that […] or that it’s not adapted.”(I_SOPPC_Physician_03:3-5)
“In other words, that the structure can be used to map the different levels that are addressed during a home visit. And then you could also do certain things, if you knew, okay, they are now in this section, then maybe you think about them.”(I_SOPPC_Physician_03:32)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bush, R.A.; Pérez, A.; Baum, T.; Etland, C.; Connelly, C.D. A systematic review of the use of the electronic health record for patient identification, communication, and clinical support in palliative care. JAMIA Open 2018, 1, 294–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratwani, R.M.; Savage, E.; Will, A.; Fong, A.; Karavite, D.; Muthu, N.; Rivera, A.J.; Gibson, C.; Asmonga, D.; Moscovitch, B.; et al. Identifying Electronic Health Record Usability And Safety Challenges In Pediatric Settings. Health Aff. 2018, 37, 1752–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, H.C.; Suresh, S. Electronic Documentation in Pediatrics: The Rationale and Functionality Requirements–Technical Report. Pediatrics 2020, 146, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Howe, J.L.; Adams, K.T.; Hettinger, A.Z.; Ratwani, R.M. Electronic Health Record Usability Issues and Potential Contribution to Patient Harm. JAMA 2018, 319, 1276–1278. [Google Scholar] [CrossRef] [PubMed]
- Melnick, E.R.; Dyrbye, L.N.; Sinsky, C.A.; Trockel, M.; West, C.P.; Nedelec, L.; Tutty, M.A.; Shanafelt, T. The Association between Perceived Electronic Health Record Usability and Professional Burnout among Us Physicians. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2020; pp. 476–487. [Google Scholar]
- Bevan, N.; Carter, J.; Harker, S. ISO 9241-11 Revised: What Have We Learnt About Usability since 1998? Springer International Publishing: Cham, Switzerland, 2015; pp. 143–151. [Google Scholar]
- Rödle, W.; Wimmer, S.; Zahn, J.; Prokosch, H.-U.; Hinkes, B.; Neubert, A.; Rascher, W.; Kraus, S.; Toddenroth, D.; Sedlmayr, B. User-Centered Development of an Online Platform for Drug Dosing Recommendations in Pediatrics. Appl. Clin. Inform. 2019, 10, 570–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bundschuh, B.B.; Majeed, R.W.; Bürkle, T.; Kuhn, K.; Sax, U.; Seggewies, C.; Vosseler, C.; Röhrig, R. Quality of human-computer interaction—Results of a national usability survey of hospital-IT in Germany. BMC Med. Inform. Decis. Mak. 2011, 11, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leu, M.G.; O’Connor, K.G.; Marshall, R.; Price, D.T.; Klein, J.D. Pediatricians’ Use of Health Information Technology: A National Survey. Pediatrics 2012, 130, e1441-6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, H.C.; Suresh, S.; Council on Clinical Information Technology. Electronic Documentation in Pediatrics: The Rationale and Functionality Requirements–Policy Statement. Pediatrics 2020, 146, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chambers, L. A Guide to Children’s Palliative Care; Goldman, A., Ed.; Together for Short Lives: Bristol, UK, 2018. [Google Scholar]
- Nolte-Buchholtz, S.; Zernikow, B.; Wager, J. Pediatric Patients Receiving Specialized Palliative Home Care According to German Law: A Prospective Multicenter Cohort Study. Children 2018, 5, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feudtner, C.; Kang, T.I.; Hexem, K.R.; Friedrichsdorf, S.J.; Osenga, K.; Siden, H.; E Friebert, S.; Hays, R.M.; Dussel, V.; Wolfe, J. Pediatric Palliative Care Patients: A Prospective Multicenter Cohort Study. Pediatrics 2011, 127, 1094–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, L.A.; Grégoire, M.-C. Challenging neurological symptoms in paediatric palliative care: An approach to symptom evaluation and management in children with neurological impairment. Paediatr. Child Health 2015, 20, 159–165. [Google Scholar] [CrossRef]
- Hoell, J.I.; Weber, H.; Warfsmann, J.; Trocan, L.; Gagnon, G.; Danneberg, M.; Balzer, S.; Keller, T.; Janßen, G.; Kuhlen, M. Facing the large variety of life-limiting conditions in children. Eur. J. Nucl. Med. Mol. Imaging 2019, 178, 1893–1902. [Google Scholar] [CrossRef]
- Schwantes, S.; O’Brien, H.W. Pediatric Palliative Care for Children with Complex Chronic Medical Conditions. Pediatr. Clin. North Am. 2014, 61, 797–821. [Google Scholar] [CrossRef] [PubMed]
- Garske, D.; Schmidt, P.; Hasan, C.; Wager, J.; Zernikow, B. Inpatient Paediatric Palliative Care–a Retrospective Study. Z. für Palliativmedizin 2016, 17, 302–307. [Google Scholar]
- Lin, W.T.; Shao, B.B. The relationship between user participation and system success: A simultaneous contingency approach. Inf. Manag. 2000, 37, 283–295. [Google Scholar] [CrossRef]
- Kushniruk, A.; Nøhr, C. Participatory Design, User Involvement and Health It Evaluation. In Evidence-Based Health Informatics; Ammenwerth, E., Rigby, M., Eds.; IOS Press: Amsterdam, The Netherlands, 2016; pp. 139–151. [Google Scholar]
- Huang, M.E. IT Is From Mars and Physicians From Venus: Bridging the Gap. PM&R 2017, 9, S19–S25. [Google Scholar] [CrossRef]
- Martikainen, S.; Kaipio, J.; Lääveri, T. End-user participation in health information systems (HIS) development: Physicians’ and nurses’ experiences. Int. J. Med. Inform. 2020, 137, 104117. [Google Scholar] [CrossRef] [PubMed]
- Mayring, P. Qualitative Content Analysis. Foundations and Procedures; Beltz: Weinheim, Germany; Basel, Switzerland, 2010. [Google Scholar]
- Liossi, C.; Hatira, P.; Mystakidou, K. The use of the genogram in palliative care. Palliat. Med. 1997, 11, 455–461. [Google Scholar] [CrossRef]
- Hoell, J.I.; Weber, H.L.; Balzer, S.; Danneberg, M.; Gagnon, G.; Trocan, L.; Borkhardt, A.; Jansen, G.; Kuhlen, M. Advance care planning and outcome in pediatric palliative home care. Oncotarget 2018, 9, 17867–17875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Alemán, J.L.; Señor, I.C.; Lozoya, P.Á.O.; Toval, A. Security and privacy in electronic health records: A systematic literature review. J. Biomed. Inform. 2013, 46, 541–562. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Liu, L.; Xue, R. Role-based and time-bound access and management of EHR data. Secur. Commun. Networks 2013, 7, 994–1015. [Google Scholar] [CrossRef]
- Craig, F.; Abu-Saad, H.H.; Benini, F.; Kuttner, L.; Wood, C.; Feraris, P.C.; Zernikow, B. Impacct: Standards for Paediatric Palliative Care in Europe. Eur. J. Palliat. Care 2007, 14, 109–114. [Google Scholar]
- Madhavan, S.; Sanders, A.E.; Chou, W.Y.; Shuster, A.; Boone, K.W.; Dente, M.A.; Shad, A.T.; Hesse, B.W. Pediatric Palliative Care and Ehealth Opportunities for Patient-Centered Care. Am. J. Prev. Med. 2011, 40 (Suppl. 2), S208–S216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begoyan, A. An Overview of Interoperability Standards for Electronic Health Records. In Proceedings of the Paper Presented at the 10th World Conference on Integrated Design and Process Technology (IDPT-2007), Antalya, Turkey, 3–8 June 2007. [Google Scholar]
- Spicer, S.; Macdonald, M.E.; Davies, D.; Vadeboncoeur, C.; Siden, H. Introducing a lexicon of terms for paediatric palliative care. Paediatr. Child Health 2015, 20, 155–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menezes, A.; Esplen, P.; Bartlett, P.; Turner, B.; Keel, M.; Etherington, V.; Conisbee, E.; Plant, A.; Haslam, V.; England, J. A system of electronic records developed by a childrens hospice. Int. J. Palliat. Nurs. 2007, 13, 237–242. [Google Scholar] [CrossRef]
- Kimland, E.; Böttiger, Y.; Lindemalm, S. Recent drug history in children visiting a pediatric emergency room and documentation in medical records. Eur. J. Clin. Pharmacol. 2011, 67, 1085–1089. [Google Scholar] [CrossRef] [PubMed]
- Kimland, E.; Odlind, V. Off-Label Drug Use in Pediatric Patients. Clin. Pharmacol. Ther. 2012, 91, 796–801. [Google Scholar] [CrossRef]
- García-López, I.; Vendrell, M.C.-M.; Romero, I.M.; de Noriega, I.; González, J.B.; Martino-Alba, R. Off-Label and Unlicensed Drugs in Pediatric Palliative Care: A Prospective Observational Study. J. Pain Symptom Manag. 2020, 60, 923–932. [Google Scholar] [CrossRef]
- Martikainen, S.; Korpela, M.; Tiihonen, T. User participation in healthcare IT development: A developers’ viewpoint in Finland. Int. J. Med Inform. 2014, 83, 189–200. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Inpatient a n (%) | Outpatient b n (%) | |
|---|---|---|
| Sex | ||
| Female | 15 (78.9) | 6 (66.7) |
| Male | 4 (21.1) | 3 (33.3) |
| Age in years (SD) | 42.9 (11.1) | 47.6 (6.9) |
| Profession | ||
| Nurse | 6 (31.6) | 4 (44.4) |
| Physician | 6 (31.6) | 5 (55.6) |
| Psychosocial | 5 (26.3) | |
| Secretary | 2 (10.5) | |
| Years of work experience | ||
| 0–10 | 7 (36.8) | |
| 10–20 | 4 (21.1) | 3 (33.3) |
| 20–30 | 4 (21.1) | 5 (55.6) |
| >30 | 4 (21.1) | 1 (11.1) |
| Years of experience in current position | ||
| 0–4 | 10 (52.6) | 3 (33.3) |
| 4–8 | 2 (10.5) | 2 (22.2) |
| 8–12 | 4 (21.1) | 3 (33.3) |
| >12 | 3 (15.8) | 1 (11.1) |
| Experience in professional use of EHRs | 7 (36.8) | 9 (100) |
| Years of experience in professional use of EHRs c | ||
| 0–4 | 2 (10.5) | 1 (11.1) |
| 4–8 | 3 (15.8) | 2 (22.2) |
| 8–12 | 1 (5.3) | 2 (22.2) |
| >12 | 1 (5.3) | 2 (22.2) |
| Subcategories of General Requirements | Specifications |
|---|---|
| 3.3.1 Different data entry options | • Speech recognition • ePens • Templates (discrete data, free text) |
| 3.3.2 Clarity | • Individualizable views • Scalability • Filter function |
| 3.3.3 Integration of multimedia files | • Photo files • Audio files • Video files |
| 3.3.4 Interoperability | • Data transfer between providers involved in the patient’s care |
| 3.3.5 Multi-professional documentation | • Integrative documentation of involved professions |
| 3.3.6 Adaptability | • Customizable contents • Flexibility to new requirements |
| Subcategories of Content Requirements | Specific Contents | |
|---|---|---|
| 3.4.1 Individual page with patient’s core information | • Patient’s core information • Medical Orders for life-sustaining treatment • Diagnoses • Admission reason | |
| 3.4.2 Basic Assessment Tool | Information about • Social background • Social law and care benefits • Abilities (e.g., linguistic abilities) • Degree of disability • Patient’s provider network • Educational institutions | |
| 3.4.3 Treatment Process | Comprehensible process documentation including • Patient’s main symptoms/issues • Interventions • Outcome | |
| 3.4.4 Patient Chart | Inpatient progress documentation • Vital signs • Documentation of symptom observation • Medication • Positioning | Outpatient progress documentation • Vital signs • Documentation of symptom observation • Nursing reports • Comments |
| 3.4.5 Medication Tool | • Medication chart • Calculator for dosages | |
| 3.4.6 Percentile Calculator | • Automatically generated growth charts • Percentile curves | |
| 3.4.7 Specific Care Tools | Templates for • Ventilation documentation • Tracheostoma care • Secretion management • Wound care • Nursing care plan | |
| 3.4.8 Psychosocial Tool | Template for • Psychosocial documentation subdivided by patients and family • Psychosocial care planning | |
| 3.5.9 Home Visit Tool a | Template should map home visit routine and include • Administrative data • Rationale for the home visit • List of distressing symptoms • Physical examination section • Psychosocial and socio-legal issues | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, D.; Kernebeck, S.; Busse, T.S.; Ehlers, J.; Wager, J.; Zernikow, B.; Dreier, L.A. Electronic Health Records in Specialized Pediatric Palliative Care: A Qualitative Needs Assessment among Professionals Experienced and Inexperienced in Electronic Documentation. Children 2021, 8, 249. https://doi.org/10.3390/children8030249
Meyer D, Kernebeck S, Busse TS, Ehlers J, Wager J, Zernikow B, Dreier LA. Electronic Health Records in Specialized Pediatric Palliative Care: A Qualitative Needs Assessment among Professionals Experienced and Inexperienced in Electronic Documentation. Children. 2021; 8(3):249. https://doi.org/10.3390/children8030249
Chicago/Turabian StyleMeyer, Dorothee, Sven Kernebeck, Theresa Sophie Busse, Jan Ehlers, Julia Wager, Boris Zernikow, and Larissa Alice Dreier. 2021. "Electronic Health Records in Specialized Pediatric Palliative Care: A Qualitative Needs Assessment among Professionals Experienced and Inexperienced in Electronic Documentation" Children 8, no. 3: 249. https://doi.org/10.3390/children8030249
APA StyleMeyer, D., Kernebeck, S., Busse, T. S., Ehlers, J., Wager, J., Zernikow, B., & Dreier, L. A. (2021). Electronic Health Records in Specialized Pediatric Palliative Care: A Qualitative Needs Assessment among Professionals Experienced and Inexperienced in Electronic Documentation. Children, 8(3), 249. https://doi.org/10.3390/children8030249