
A Quality Improvement Initiative to Reduce Bronchopulmonary Dysplasia in a Level 4 NICU—Golden Hour Management of Respiratory Distress Syndrome in Preterm Newborns

Abstract
:1. Introduction
2. Methods
2.1. Ethical Approval
2.2. Context
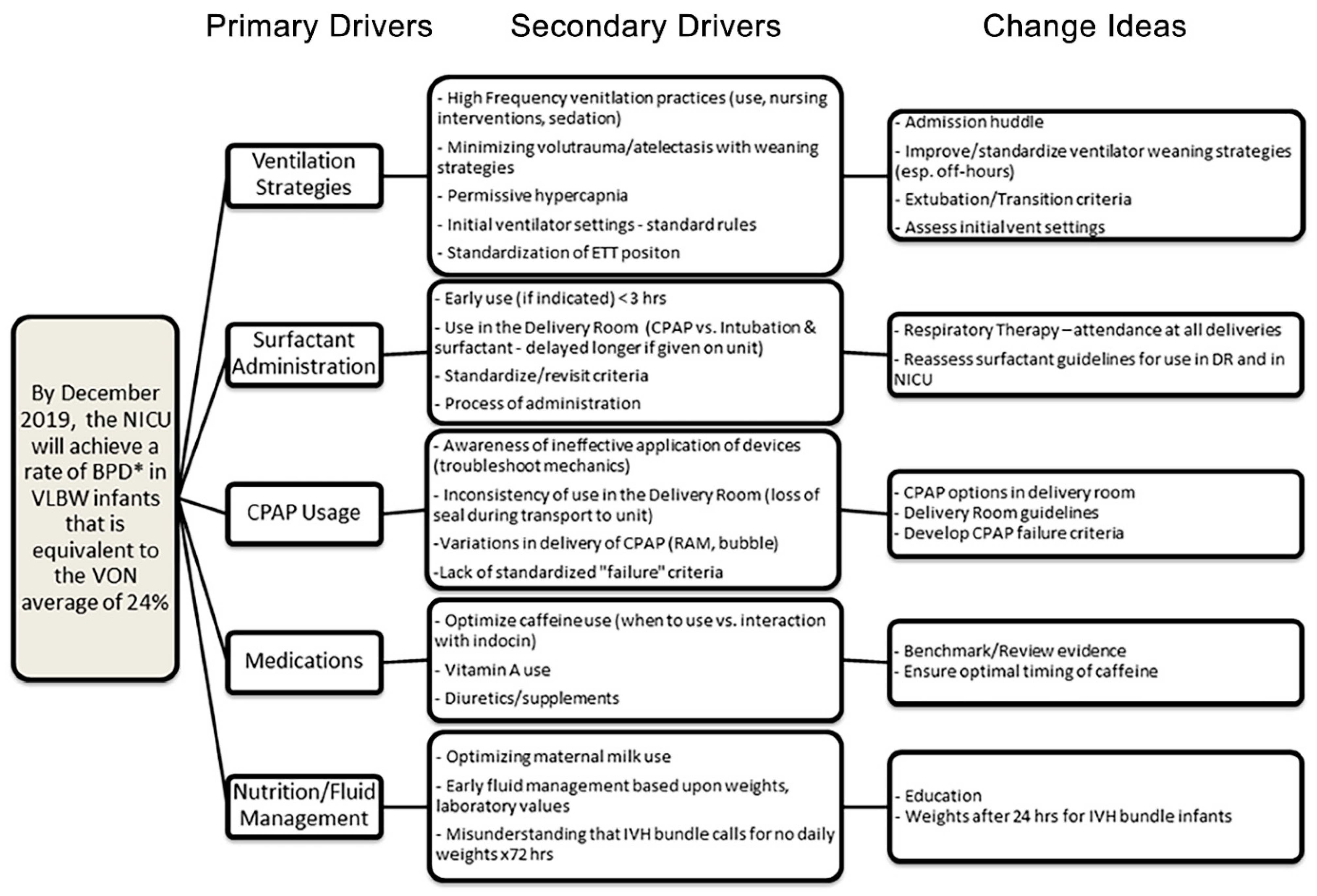
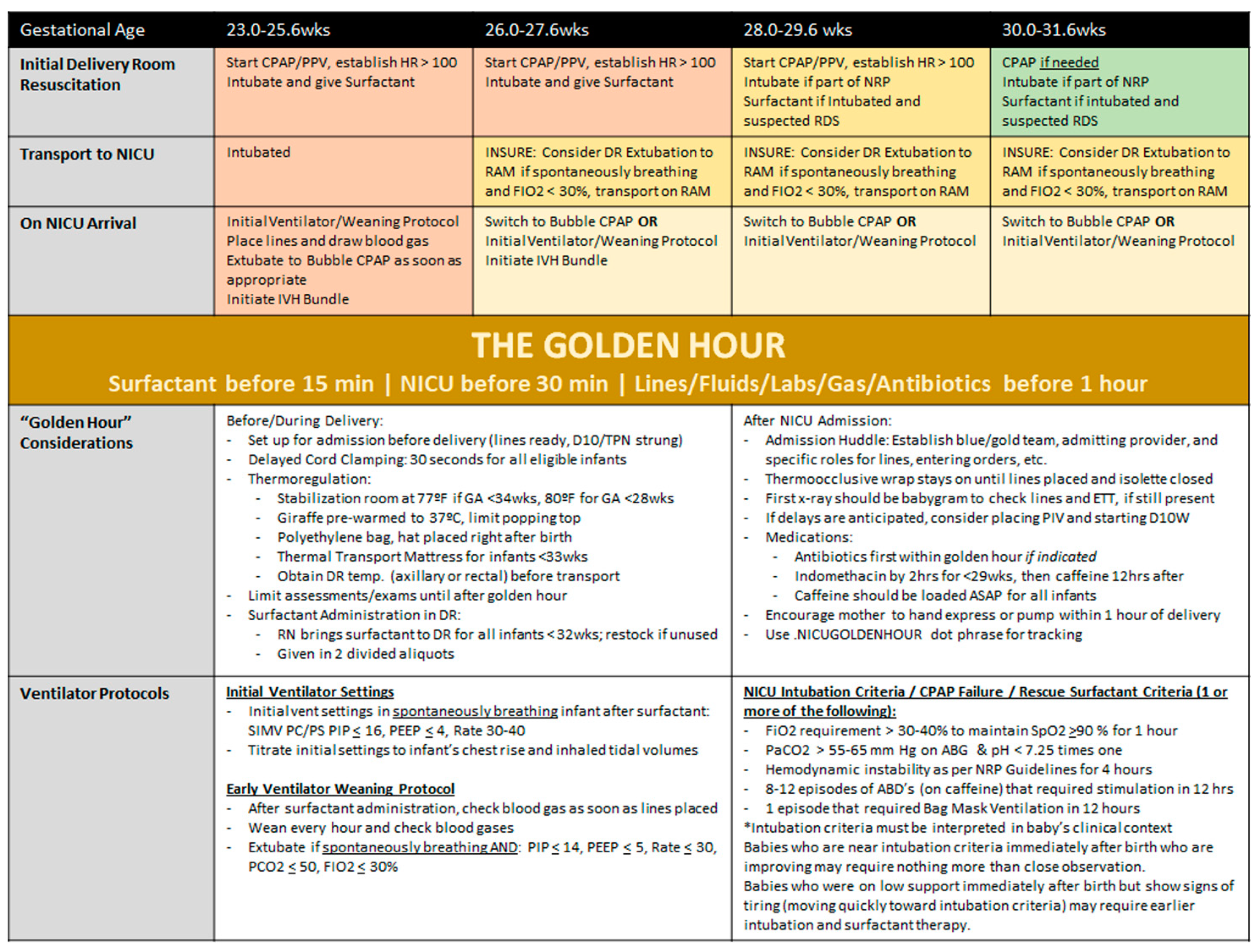
2.3. Interventions
2.4. Project Year 2018
2.5. Project Year 2019
2.6. Project Year 2020 and Ongoing Initiatives
2.7. Measures and Analysis
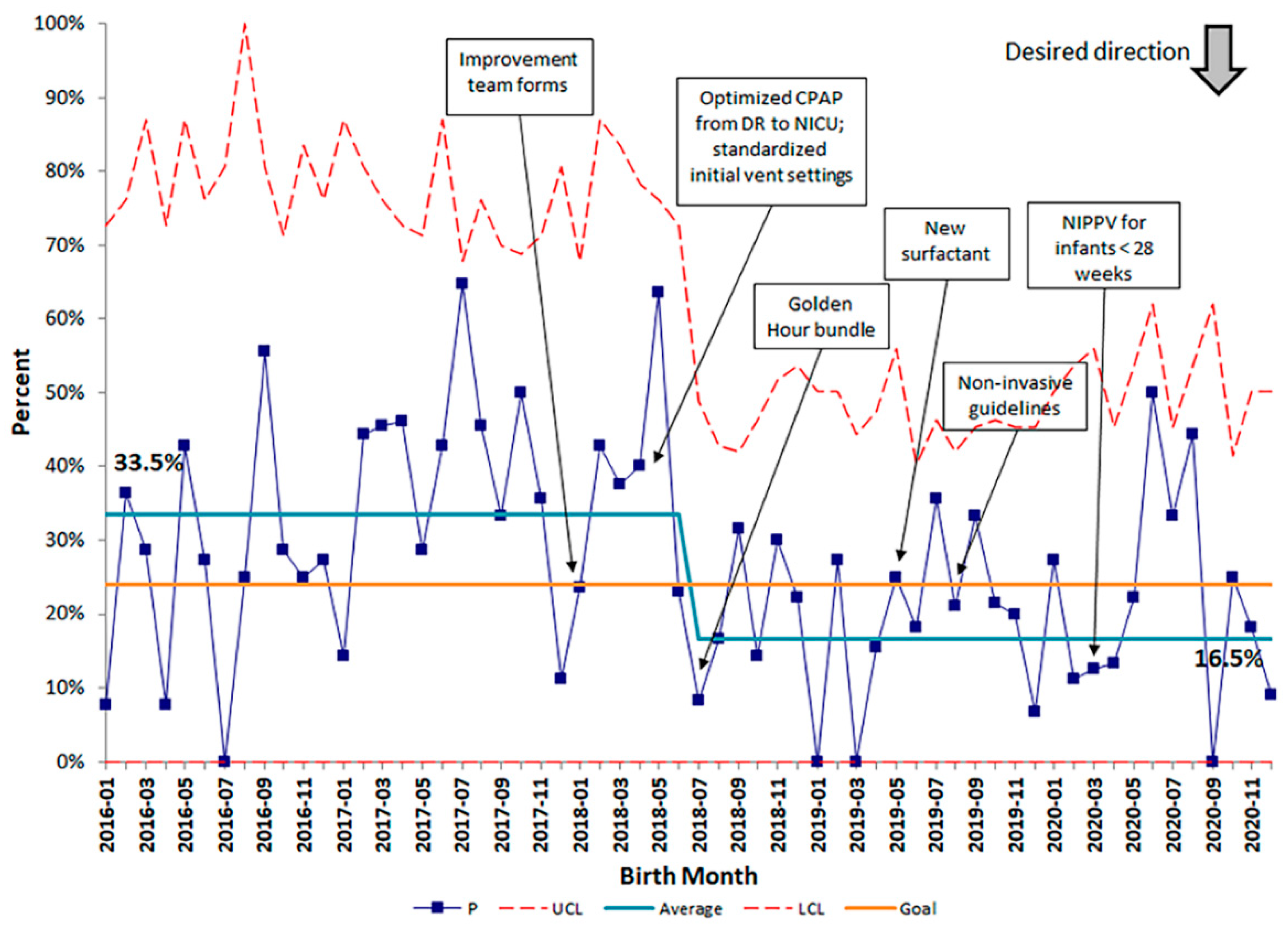
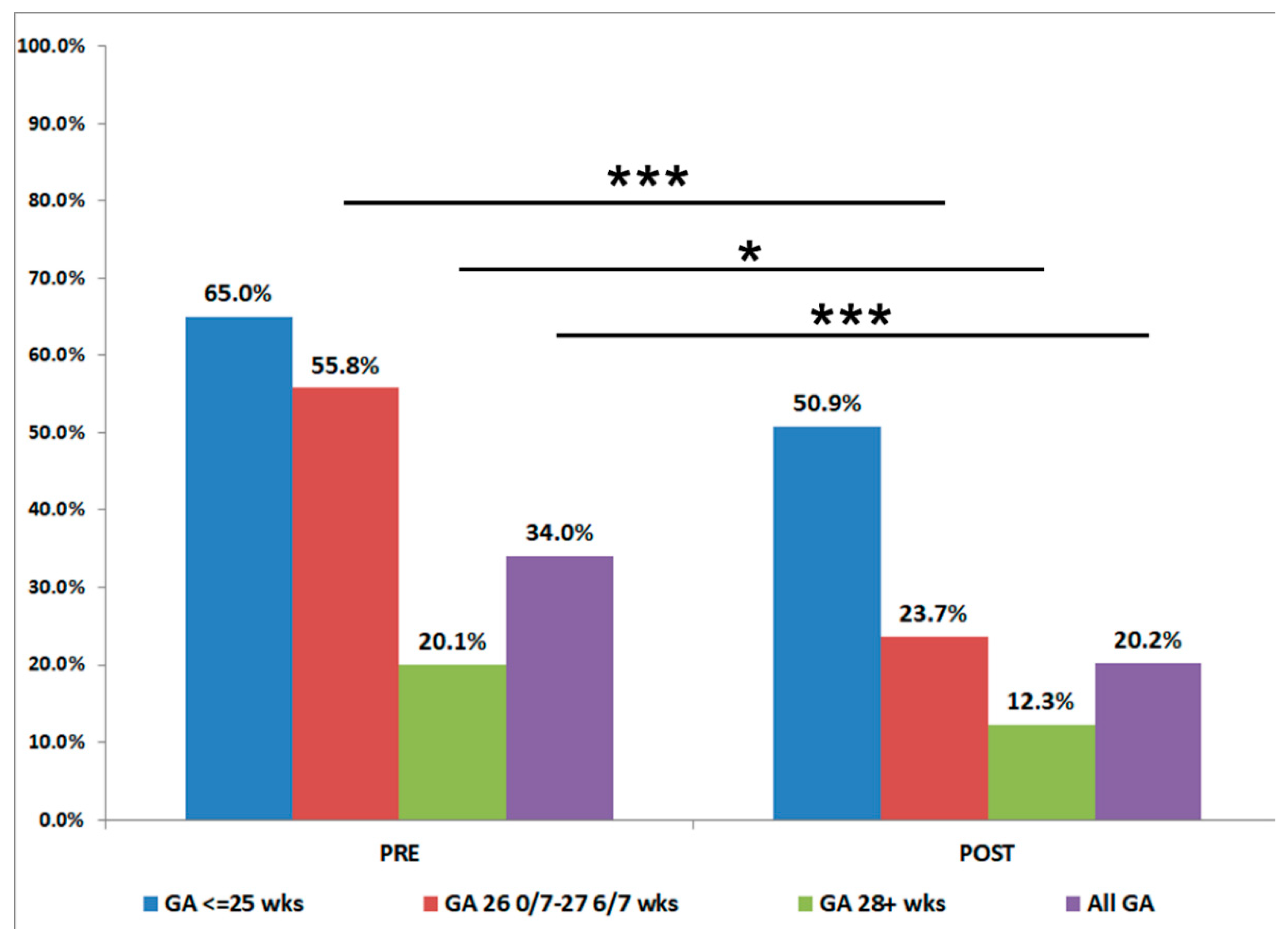
3. Results
4. Discussion
Summary and Interpretation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PDSA Cycle | Date | PDSA Focus | Description | Test or Implement |
|---|---|---|---|---|
| 1 | March 2018 | All Key Drivers | Review of Ventilation Practices | Test |
| 2 | May 2018 | Ventilation Strategies | Standardize Initial Ventilator Settings | Implement |
| 3 | July 2018 | Ventilation Strategies, Surfactant Administration, CPAP Usage, Admission Huddle | Golden Hour Bundle | Implement |
| 4 | May 2019 | Surfactant Administration | Changed surfactant products | Implement |
| 5 | July 2019 | CPAP Usage | Non-invasive Ventilation Guidelines | Implement |
| 6 | July 2019 | Medication Use | Stop use of prophylactic indomethacin | Implement |
| 7 | March 2020 | Ventilation Strategies, CPAP Usage | Extubation Guidelines, Revised Non-Invasive Guidelines | Test |
| 8 | November 2020 | Surfactant Administration | Less Invasive Surfactant Administration | Test/Implement |
| 9 | November 2020 | Bubble Relaunch | Maintenance of effective CPAP | Implement |
| Applicable Driver(s) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Measure Description | Numerator | Denominator | Unit | Data Source | Measurement Frequency | Ventilation Strategies | Surfactant Administration | CPAP Usage | Medications | Fluids/Nutrition |
| Compliance with DR Surfactant | N with DR Surfactant | N < 28 weeks | % | Neodata, Chart Audit | Monthly | X | ||||
| Compliance with Extubation Guidelines | N < 28 weeks extubated to NIPPV | N < 28 weeks extubated | % | Neodata, Chart Audit | Monthly | X | X | |||
| Description | Numerator | Denominator | Unit | Data Source | Frequency | Driver(s) |
|---|---|---|---|---|---|---|
| Outcome Measures | ||||||
| Von BPD | N BPD | VON Eligible Patients | % | Neodata, Chart Audit | Monthly | ALL |
| Jensen BPD | N Jensen BPD | VON Eligible Patients | % | Neodata | Monthly | ALL |
| Discharge Diuretic Use | N discharge diuretics | VON Eligible Patients | % | Neodata | BiMonthly | Medications |
| Opiate Use | N ≥ 10 doses opiates | VON Eligible Patients | % | Neodata | BiMonthly | Medications |
| Balancing Measures: | ||||||
| Repeat Surfactant | N with ≥ 1 dose surf | VON Eligible Patients | % | Neodata | BiMonthly | Surfactant Usage |
| Failed Extubations | N failing extubation ≤ 5 d | VON Eligible Patients | % | Neodata | BiMonthly | Ventilation Strategies, CPAP |
| Postnatal Steroids | N receiving > 7 days steroids > 14 days age | VON Eligible Patients | % | Neodata | BiMonthly | Medications |


References
- Underwood, M.A.; Danielsen, B.; Gilbert, W.M. Cost, causes and rates of rehospitalization of preterm infants. J. Perinatol. 2007, 27, 614–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapcharoensap, W.; Bennett, M.V.; Xu, X.; Lee, H.C.; Dukhovny, D. Hospitalization costs associated with bronchopulmonary dysplasia in the first year of life. J. Perinatol. 2020, 40, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Chess, P.R.; D’Angio, C.T.; Pryhuber, G.S.; Maniscalco, W.M. Pathogenesis of bronchopulmonary dysplasia. Semin. Perinatol. 2006, 30, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Isayama, T.; Iwami, H.; Mcdonald, S.; Beyene, J. Association of Noninvasive Ventilation Strategies with Mortality and Bronchopulmonary Dysplasia among Preterm Infants: A Systematic Review and Meta-analysis. JAMA 2016, 316, 611–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pillow, J.J.; Hillman, N.; Moss, T.J.M.; Polglase, G.; Bold, G.; Beaumont, C.; Ikegami, M.; Jobe, A.H. Bubble continuous positive airway pressure enhances lung volume and gas exchange in preterm lambs. Am. J. Respir. Crit. Care Med. 2007, 176, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Dunn, M.S.; Fenwick, M.; Shennan, A.T. A comparison of underwater bubble continuous positive airway pressure with ventilator-derived continuous positive airway pressure in premature neonates ready for extubation. Biol. Neonate 1998, 73, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Backes, C.H.; Cooper, J.N.; Notestine, J.L.; Alfred, C.M.; Ball, M.K.; Rivera, B.K.; Lamp, J.M.; Marzec, L.; Stenger, M.R.; Moallem, M. A trial comparing continuous positive airway pressure (CPAP) devices in preterm infants. J. Perinatol. 2020, 40, 1193–1201. [Google Scholar] [CrossRef] [PubMed]
- Provost, L.P.; Murray, S.K. The Healthcare Data Guide: Learning from Data for Improvement; Jossey-Bass: San Francisco, CA, USA, 2011. [Google Scholar]
- Dylag, A.M.; Kopin, H.G.; O’Reilly, M.A.; Wang, H.; Davis, S.D.; Ren, C.L.; Pryhuber, G.S. Early Neonatal Oxygen Exposure Predicts Pulmonary Morbidity and Functional Deficits at 1 Year. J. Pediatr. 2020, 223, 20–28.e2. [Google Scholar] [CrossRef] [PubMed]






| Before Intervention (1 January 2016–31 March 2018) | After Intervention (1 April 2018–31 December 2020) | p-Value | |
|---|---|---|---|
| Gestational Age < 30 weeks | 205 (63.7%) | 305 (65.5%) | 0.61 |
| Birth Weight < 1500 g and GA < 29 weeks | 117 (36.3%) | 161 (34.5%) | 0.61 |
| Male Sex | 172 (53.4%) | 223 (47.9%) | 0.12 |
| Inborn | 292 (90.7%) | 420 (90.1%) | 0.80 |
| Intrauterine Growth Restriction | 19 (5.9%) | 28 (6%) | 0.94 |
| Maternal Pre-eclampsia | 124 (38.5%) | 199 (42.7%) | 0.23 |
| Maternal Chorioamnionitis | 101 (31.4%) | 115 (24.7%) | 0.03 |
| Antenatal Steroids | 300 (93.2%) | 429 (92.1%) | 0.56 |
| Postnatal Steroids | 43 (13.4%) | 60 (12.9%) | 0.84 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dylag, A.M.; Tulloch, J.; Paul, K.E.; Meyers, J.M. A Quality Improvement Initiative to Reduce Bronchopulmonary Dysplasia in a Level 4 NICU—Golden Hour Management of Respiratory Distress Syndrome in Preterm Newborns. Children 2021, 8, 301. https://doi.org/10.3390/children8040301
Dylag AM, Tulloch J, Paul KE, Meyers JM. A Quality Improvement Initiative to Reduce Bronchopulmonary Dysplasia in a Level 4 NICU—Golden Hour Management of Respiratory Distress Syndrome in Preterm Newborns. Children. 2021; 8(4):301. https://doi.org/10.3390/children8040301
Chicago/Turabian StyleDylag, Andrew M., Jamey Tulloch, Karen E. Paul, and Jeffrey M. Meyers. 2021. "A Quality Improvement Initiative to Reduce Bronchopulmonary Dysplasia in a Level 4 NICU—Golden Hour Management of Respiratory Distress Syndrome in Preterm Newborns" Children 8, no. 4: 301. https://doi.org/10.3390/children8040301
APA StyleDylag, A. M., Tulloch, J., Paul, K. E., & Meyers, J. M. (2021). A Quality Improvement Initiative to Reduce Bronchopulmonary Dysplasia in a Level 4 NICU—Golden Hour Management of Respiratory Distress Syndrome in Preterm Newborns. Children, 8(4), 301. https://doi.org/10.3390/children8040301