
A Meta-Analysis of the Current State of Evidence of the Incredible Years Teacher-Classroom Management Program



Abstract
:1. Introduction
1.1. The Incredible Years
1.2. Research on IYTCM
1.3. Variability within the Research
1.4. Aims of the Current Study
- What is the overall effect size associated with improving teacher outcomes in the classroom post-intervention?
- What is the overall effective size associated with improving child outcomes in the classroom post-intervention?
- To what extent does the effect size of IYTCM differ based on target child (i.e., severity of child behavior), reporting methods, study design, and dosage?
2. Methods
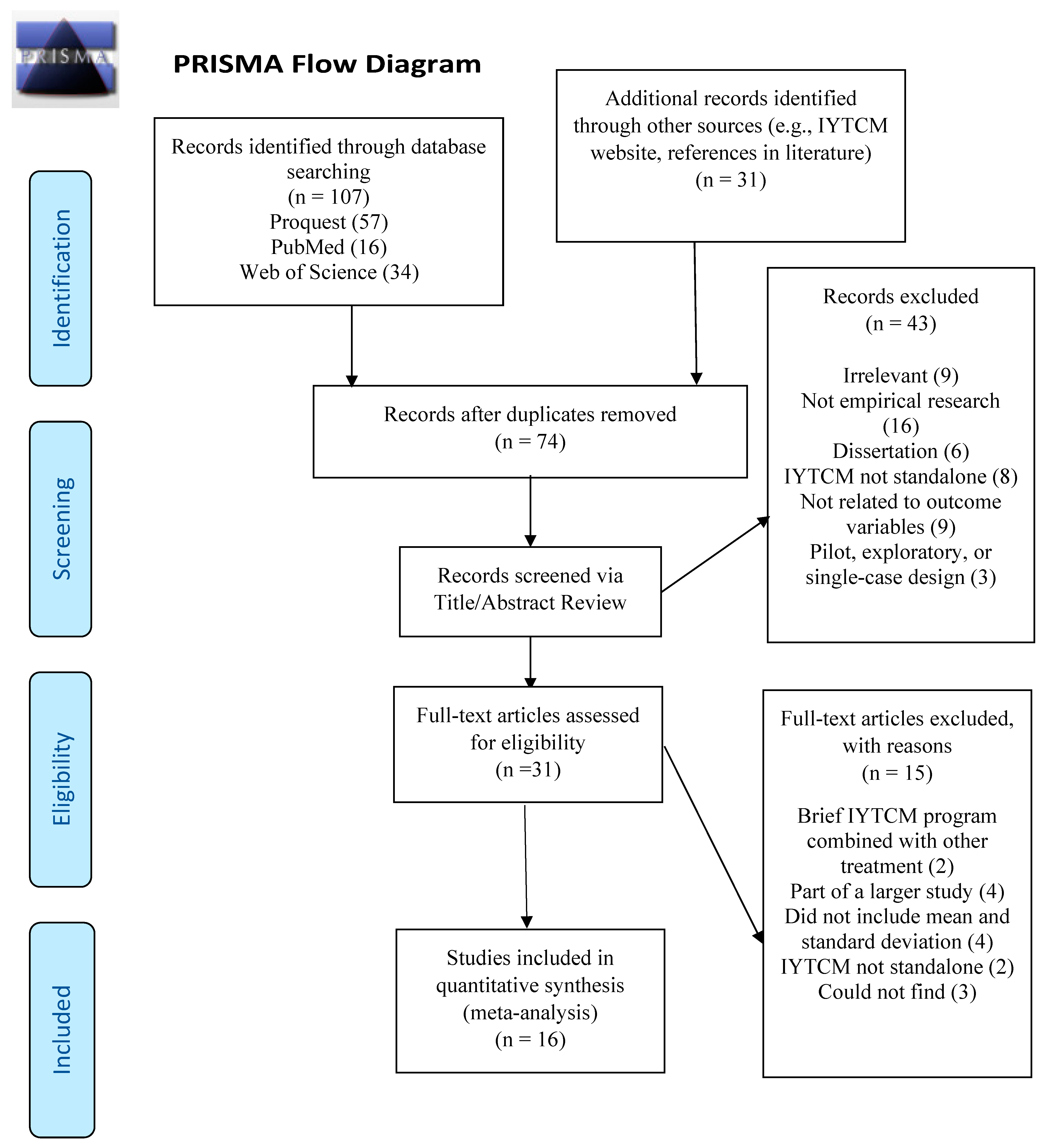
2.1. Literature Search Criteria and Study Identification
2.2. Study Coding
2.3. Data Extraction
3. Results
3.1. Teacher Outcomes
3.2. Child Outcomes
3.3. Moderating Variables
4. Discussion
5. Limitations
6. Implications for Research and Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Durlak, J.A.; Weissberg, R.P.; Dymnicki, A.B.; Taylor, R.D.; Schellinger, K.B. The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Dev. 2011, 82, 405–432. [Google Scholar] [CrossRef] [PubMed]
- Flower, A.; McKenna, J.W.; Haring, C.D. Behavior and classroom management: Are teacher preparation programs really preparing our teachers? Prev. Sch. Fail. Altern. Educ. Child. Youth 2017, 61, 163–169. [Google Scholar] [CrossRef]
- Jones, V.; Jones, L. Comprehensive Classroom Management: Creating Communities of Support and Solving Problems; Pearson Education: Boston, MA, USA, 2015. [Google Scholar]
- Mihalic, S.F.; Elliott, D.S. Evidence-based programs registry: Blueprints for healthy youth development. Eval. Program Plan. 2015, 48, 124–131. [Google Scholar] [CrossRef] [Green Version]
- Every Student Succeeds Act, Pub. L. No. 114–95, 20 U.S.C. 1 6301 et Seq. 2015. Available online: https://www.govinfo.gov/content/pkg/PLAW-114publ95/pdf/PLAW-114publ95.pdf (accessed on 28 November 2021).
- Kratochwill, T.R.; Shernoff, E.S. Evidence-based practice: Promoting evidence-based interventions in school psychology. Sch. Psych. Rev. 2004, 33, 34–48. [Google Scholar] [CrossRef]
- Webster-Stratton, C.; Reinke, W.M.; Herman, K.C.; Newcomer, L.L. The Incredible Years teacher classroom management training: The methods and principles that support fidelity of training delivery. Sch. Psych. Rev. 2011, 40, 509–529. [Google Scholar] [CrossRef]
- Patterson, G.R. Coercive Family Process; Castalia: Eugene, OR, USA, 1982. [Google Scholar]
- Weber, K.E.; Gold, B.; Prilop, C.N.; Kleinknecht, M. Promoting pre-service teachers’ professional vision of classroom management during practical school training: Effects of a structured online-and video-based self-reflection and feedback intervention. Teach. Teach. Educ. 2018, 76, 39–49. [Google Scholar] [CrossRef]
- Lee, M.; Van Vlack, S. Teachers’ emotional labour, discrete emotions, and classroom management self-efficacy. Educ. Psychol. 2018, 38, 669–686. [Google Scholar] [CrossRef]
- Sánchez-Cabrero, R.; Estrada-Chichón, J.L.; Abad-Mancheño, A.; Mañoso-Pacheco, L. Models on Teaching Effectiveness in Current Scientific Literature. Educ. Sci. 2021, 11, 409. [Google Scholar] [CrossRef]
- Serketich, W.J.; Dumas, J.E. The effectiveness of behavioral parent training to modify antisocial behavior in children: A meta-analysis. Behav. Ther. 1996, 27, 171–186. [Google Scholar] [CrossRef]
- Lundahl, B.; Risser, H.J.; Lovejoy, M.C. A meta-analysis of parent training: Moderators and follow-up effects. Clin. Psychol. Rev. 2006, 26, 86–104. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.; Hayes, R.; Byford, S.; Edwards, V.; Fletcher, M.; Logan, S.; Ganguli, P. The effectiveness and cost-effectiveness of the Incredible Years Teacher Classroom Management programme in primary school children: Results of the STARS cluster randomised controlled trial. Psychol. Med. 2018, 49, 828–842. [Google Scholar] [CrossRef] [Green Version]
- Webster-Stratton, C. The Incredible Years: Parents, teachers, and children training series. Resid. Treat. Child. Youth 2001, 18, 31–45. [Google Scholar] [CrossRef]
- Webster-Stratton, C.; Reid, M.J. The Incredible Years Classroom Management Teacher Training Program: Content, Methods, and Process. 2002. Available online: https://incredibleyears.com/wp-content/uploads/teacher-training-program-classroom-mgmt-02.pdf (accessed on 28 November 2021).
- Menting, A.T.; de Castro, B.O.; Matthys, W. Effectiveness of the Incredible Years parent training to modify disruptive and prosocial child behavior: A meta-analytic review. Clin. Psychol. Rev. 2013, 33, 901–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsey, M.; Wilson, D.B. Practical Meta-Analysis; Sage Publications: Thousand Oaks, CA, USA, 2001; Volume 49. [Google Scholar]
- Webster-Stratton, C.; Reid, M.J.; Hammond, M. Preventing conduct problems, promoting social competence: A parent and teacher training partnership in Head Start. J. Clin. Child Psychol. 2001, 30, 283–302. [Google Scholar] [CrossRef]
- Webster-Stratton, C.; Reid, M.J.; Hammond, M. Treating children with early-onset conduct problems: Intervention outcomes for parent, child, and teacher training. J. Clin. Child Adolesc. Psychol. 2004, 33, 105–124. [Google Scholar] [CrossRef]
- Webster-Stratton, C.; Reid, M.J.; Stoolmiller, M. Preventing conduct problems and improving school readiness: Evaluation of the Incredible Years Teacher and Child Training Programs in high-risk schools. J. Child Psychol. Psychiatry 2008, 49, 471–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchings, J.; Daley, D.; Jones, K.; Martin, P.; Bywater, T.; Gwyn, R. Early results from developing and researching the Webster-Stratton Incredible Years Teacher Classroom Management Training Programme in North West Wales. J. Child Serv. 2007, 2, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Hutchings, J.; Martin-Forbes, P.; Daley, D.; Williams, M.E. A randomized controlled trial of the impact of a teacher classroom management program on the classroom behavior of children with and without behavior problems. J. Sch. Psychol. 2013, 51, 571–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fergusson, D.M.; Horwood, L.J.; Stanley, L. A preliminary evaluation of the Incredible Years teacher programme. N. Z. J. Psychol. 2013, 42, 51–56. [Google Scholar]
- Hickey, G.; McGilloway, S.; Hyland, L.; Leckey, Y.; Kelly, P.; Bywater, T.; O’Neill, D. Exploring the effects of a universal classroom management training programme on teacher and child behaviour: A group randomised controlled trial and cost analysis. J. Early Child. Res. 2017, 15, 174–194. [Google Scholar] [CrossRef]
- Aasheim, M.; Reedtz, C.; Handegård, B.H.; Martinussen, M.; Mørch, W.T. Evaluation of the Incredible Years Teacher Classroom Management Program in a regular Norwegian school setting. Scand J. Educ. Res. 2018, 62, 1–14. [Google Scholar] [CrossRef]
- Fossum, S.; Handegård, B.H.; Drugli, M.B. The Incredible Years teacher classroom management programme in kindergartens: Effects of a universal preventive effort. J. Child Fam. Stud. 2017, 26, 2215–2223. [Google Scholar] [CrossRef] [Green Version]
- Kirkhaug, B.; Drugli, M.B.; Handegård, B.H.; Lydersen, S.; Åsheim, M.; Fossum, S. Does the Incredible Years Teacher Classroom Management training programme have positive effects for young children exhibiting severe externalizing problems in school?: A quasi-experimental pre-post study. BMC Psychiatry 2016, 16, 362–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker-Henningham, H.; Scott, S.; Jones, K.; Walker, S. Reducing child conduct problems and promoting social skills in a middle-income country: Cluster randomised controlled trial. Br. J. Psychiatry 2012, 201, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Seabra-Santos, M.J.; Gaspar, M.F.; Major, S.O.; Patras, J.; Azevedo, A.F.; Homem, T.C.; Vale, V. Promoting mental health in disadvantaged preschoolers: A cluster randomized controlled trial of teacher training effects. J. Child Fam. Stud. 2018, 27, 3909–3921. [Google Scholar] [CrossRef]
- Raver, C.C.; Jones, S.M.; Li-Grining, C.P.; Metzger, M.; Smallwood, K.; Sardin, L. Improving preschool classroom processes: Preliminary findings from a randomized trial implemented in Head Start settings. Early Child. Res. Q. 2008, 23, 10–26. [Google Scholar] [CrossRef] [Green Version]
- Williford, A.P.; Shelton, T.L. Using mental health consultation to decrease disruptive behaviors in preschoolers: Adapting an empirically-supported intervention. J. Child Psychol. Psychiatry 2008, 49, 191–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker-Henningham, H.; Walker, S. Effect of transporting an evidence-based, violence prevention intervention to Jamaican preschools on teacher and class-wide child behaviour: A cluster randomised trial. Glob. Ment. Health 2018, 5, e7. [Google Scholar] [CrossRef] [Green Version]
- Murray, D.W.; Murr, N.; Rabiner, D.L. Preliminary Effects of the Incredible Years Teacher Training Program on Classroom Management Skills; Society for Research on Education Effectiveness: Washington, DC, USA, 2012. [Google Scholar]
- Murray, D.W.; Rabiner, D.L.; Carrig, M.M. Grade Level Effects of the Incredible Years Teacher Training Program on Emotion Regulation and Attention; Society for Research on Education Effectiveness: Washington, DC, USA, 2012. [Google Scholar]
- Murray, D.W.; Rabiner, D.L.; Kuhn, L.; Pan, Y.; Sabet, R.F. Investigating teacher and student effects of the Incredible Years Classroom Management Program in early elementary school. J. Sch. Psychol. 2017, 67, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Reinke, W.M.; Herman, K.C.; Dong, N. The Incredible Years teacher classroom management program: Outcomes from a group randomized trial. Prev. Sci. 2016, 8, 1043–1054. [Google Scholar] [CrossRef]
- Carlson, J.S.; Tiret, H.B.; Bender, S.L.; Benson, L. The influence of group training in the Incredible Years Teacher Classroom Management Program on preschool teachers’ classroom management strategies. J. Appl. Sch. Psychol. 2011, 27, 134–154. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: Chichester, UK, 2009. [Google Scholar]
- Forman, S.G.; Shapiro, E.S.; Codding, R.S.; Gonzales, J.E.; Reddy, L.A.; Rosenfield, S.A.; Stoiber, K.C. Implementation science and school psychology. Sch. Psychol. Q. 2013, 28, 77–100. [Google Scholar] [CrossRef] [Green Version]
- Leckey, Y.; Hyland, L.; Hickey, G.; Lodge, A.; Kelly, P.; Bywater, T.; McGilloway, S. A mixed-methods evaluation of the longer-term implementation and utility of a teacher classroom management training programme in Irish primary schools. Ir. Educ. Stud. 2016, 35, 35–55. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson, K.D.; Schmidt, F.L. Impact of experimental design on effect size: Findings from the research literature on training. J. Appl. Psychol. 1999, 84, 851–862. [Google Scholar] [CrossRef]
- Hoyt, W.T.; Del Re, A.C. Effect size calculation in meta-analyses of psychotherapy outcome research. Psychother. Res. 2018, 28, 379–388. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Egger, M.; Moher, D. Chapter 10: Addressing Reporting Biases. In Cochrane Handbook for Systematic Reviews of Intervention; Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011; Available online: www.handbook.cochrane.org (accessed on 28 November 2021).
- Gasparrini, A. Package Mvmeta [Statistical Software]. 2019. Available online: http://cran.r-project.org/web/packages/mvmeta/mvmeta.pdf (accessed on 28 November 2021).
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, F.L.; Hunter, J.E. Methods of Meta-Analysis: Correcting Error and Bias in Research Findings; Sage Publications: London, UK, 2014. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]


{kind=link}
| Study | Outcome Variable | Study Design | Dosage | Target Child | Reporting Method | Quality of Study |
|---|---|---|---|---|---|---|
| Aasheim et al. (2018) [26] | Positive Teacher Outcomes Negative Teacher Outcomes | QED | High Dosage | Low Risk | TR | 7 |
| Baker-Henningham et al. (2012) [29] | Positive Teacher Outcomes Negative Teacher Outcomes | RCT | High Dosage | High Risk | Obs. TR | 8 |
| Baker-Henningham & Walker (2018) [33] | Positive Teacher Outcomes | RCT | High Dosage | NA | NA | 7 |
| Carlson et al. (2011) [38] | Perceived Usefulness | QED | Low Dosage | NA | NA | 2 |
| Fergusson et al. (2013) [24] | Perceived Usefulness | QED | High Dosage | NA | NA | 2 |
| Ford et al. (2018) [14] | Prosocial Behavior Externalizing Behavior | RCT | High Dosage | Low Risk | TR | 4 |
| Fossum et al. (2017) [27] | Prosocial Behavior Externalizing Behavior | QED | Low Dosage | Low Risk | TR | 5 |
| Hickey et al. (2017) [25] | Positive Teacher Outcomes Negative Teacher Outcomes Perceived Usefulness Prosocial Behavior Externalizing Behavior | RCT | Low Dosage | Low Risk | Obs. TR | 6 |
| Hutchings et al. (2007) [22] | Perceived Usefulness Positive Teacher Outcomes Negative teacher Outcomes | QED | Low Dosage | High Risk | Obs. | 2 |
| Hutchings et al. (2013) [23] | Positive Teacher Outcomes Negative Teacher Outcomes | RCT | Low Dosage | Low Risk | Obs. | 8 |
| Kirkhaug et al. (2016) [28] | Prosocial Behavior Externalizing Behavior | QED | High Dosage | High Risk | TR | 4 |
| Murray et al. (2017) [36] | Positive Teacher Outcomes Prosocial Child Outcomes | RCT | Low Dosage | Could not tell | TR | 7 |
| Murray, Murr, & Rabiner (2012) [34] | Positive Teacher Outcomes Negative Teacher Outcomes | RCT | Low Dosage | Could not tell | TR | 6 |
| Murray, Rabiner, & Carrig (2012) [35] | Positive Teacher Outcomes | RCT | Low Dosage | NA | NA | 4 |
| Raver et al. (2008) [31] | Positive Teacher Outcomes Negative Teacher Outcomes | RCT | Low Dosage | NA | NA | 7 |
| Seabra-Santos et al. (2018) [30] | Prosocial Behavior Externalizing Behavior | QED | Low Dosage | Low Risk | TR | 4 |
| ρ = 0 | ρ = 0.2 | ρ = 0.5 | ρ = 0.7 | ρ = 0.95 | |
|---|---|---|---|---|---|
| Outcome Variable | g (SE) 95% CI [LL, UL] | g (SE) 95% CI [LL, UL] | g (SE) 95% CI [LL, UL] | g (SE) 95% CI [LL, UL] | g (SE) 95% CI [LL, UL] |
| Teacher Positive | 0.70 (0.27) ** [0.17, 1.24] | 0.71 (0.27) ** [0.18, 1.24] | 0.72 (0.27) ** [0.19, 1.24] | 0.72 (0.26) ** [0.20, 1.24] | 0.73 (0.26) ** [0.22, 1.24] |
| Teacher Negative | −0.59 (0.16) *** [−0.90, −0.27] | −0.57 (0.15) *** [−0.86, −0.28] | −0.53 (0.13) *** [−0.79, −0.28] | −0.52 (0.12) *** [−0.76, −0.28] | −0.50 (0.11) *** [−0.72, −0.27] |
| Child Prosocial | 0.19 (0.06) ** [0.07, 0.32] | 0.20 (0.06) ** [0.07, 0.32] | 0.20 (0.06) ** [0.08, 0.33] | 0.20 (0.06) ** [0.08, 0.33] | 0.21 (0.06) ** [0.08, 0.33] |
| Child Externalizing | −0.14 (0.07) * [−0.28, −0.01] | −0.14 (0.07) * [−0.29, −0.01] | −0.15 (0.07) * [−0.29, −0.01] | −0.15 (0.07) * [−0.30, −0.01] | −0. 16 (0.06) * [−0.30, −0.01] |
| Child Prosocial | Child Externalizing | Teacher Positive | Teacher Negative | Teacher Usefulness | |||
|---|---|---|---|---|---|---|---|
| Obs. | TR | Obs. | TR | ||||
| Article | g (SE) | g (SE) | g (SE) | g (SE) | g (SE) | g (SE) | g (SE) |
| Aasheim et al. (2018) [26] | 0.16 (0.006) | −0.03 (0.032) | |||||
| Baker-Henningham et al. (2012) [29] | 0.29 (0.08) | 0.60 (0.08) | −0.23 (0.082) | −0.514 (0.09) | |||
| Baker-Henningham & Walker (2018) [33] | 2.3 (0.3) | ||||||
| Carlson et al. (2011) [38] | 0.78 (0.23) | ||||||
| Fergusson et al. (2013) [24] | 0.88 (0.08) | ||||||
| Ford et al. (2018) [14] | 0.20 (0.045) | −0.15 (0.045) | |||||
| Fossum et al. (2017) [27] | 0.13 (0.06) | −0.12 (0.045) | |||||
| Hickey et al. (2017) [25] | 0.14 (0.14) | 0.12 (0.13) | −0.26 (0.14) | −0.29 (0.14) | 0.48 (0.42) | −10.0 (0.44) | 0.94 (0.44) |
| Hutchings et al. (2007) [22] | 0.92 (0.67) | −0.15 (0.65) | |||||
| Hutchings et al. (2013) [23] | −0.25 (0.19) | −0.3 (0.19) | 0.69 (0.55) | −0.46 (0.54) | |||
| Kirkhaug et al. (2016) [28] | 0.29 (0.22) | −0.56 (0.22) | |||||
| Murray et al. (2017) [36] | 00.03 (0.06) | 0.15 (0.15) | −0.26 (0.22) | ||||
| Murray, Murr, & Rabiner (2012) [34] | 0.44 (0.22) | −0.42 (0.20) | |||||
| Murray, Rabiner, & Carrig (2012) [35] | −0.03 (0.06) | 0.23 (0.02) | −0.34 (0.20) | ||||
| Raver et al. (2008) [31] | 0.73 (0.02) | −0.66 (0.21) | |||||
| Seabra-Santos et al. (2018) [30] | 0.14 (0.05) | −0.07 (0.048) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korest, R.; Carlson, J.S. A Meta-Analysis of the Current State of Evidence of the Incredible Years Teacher-Classroom Management Program. Children 2022, 9, 24. https://doi.org/10.3390/children9010024
Korest R, Carlson JS. A Meta-Analysis of the Current State of Evidence of the Incredible Years Teacher-Classroom Management Program. Children. 2022; 9(1):24. https://doi.org/10.3390/children9010024
Chicago/Turabian StyleKorest, Rachel, and John S. Carlson. 2022. "A Meta-Analysis of the Current State of Evidence of the Incredible Years Teacher-Classroom Management Program" Children 9, no. 1: 24. https://doi.org/10.3390/children9010024
APA StyleKorest, R., & Carlson, J. S. (2022). A Meta-Analysis of the Current State of Evidence of the Incredible Years Teacher-Classroom Management Program. Children, 9(1), 24. https://doi.org/10.3390/children9010024