


Balance Rehabilitation Approach by Bobath and Vojta Methods in Cerebral Palsy: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
- children diagnosed with CP;
- children aged between 3–11 years;
- children capable of understanding and executing commands;
- children without other associated diseases;
- children who did not participate in recovery programs that were based on the two methods, NDT Bobath and Vojta;
- children with GMFCS level I-IV;
- children who can adopt the orthostatic position necessary to assess balance.
- children with mental retardation;
- children who cannot participate constantly in physical therapy sessions;
- children with deformities of the locomotor system;
- children with visual or hearing impairments;
- children with spasticity more then 2 on Ashworth scale.
2.2. Evaluation of Subjects with CP
2.3. Statistical Analysis
2.4. Rehabilitation Program
2.4.1. Vojta Therapy
- Exercise 1. Reflex crawling
- Exercise 2. First position
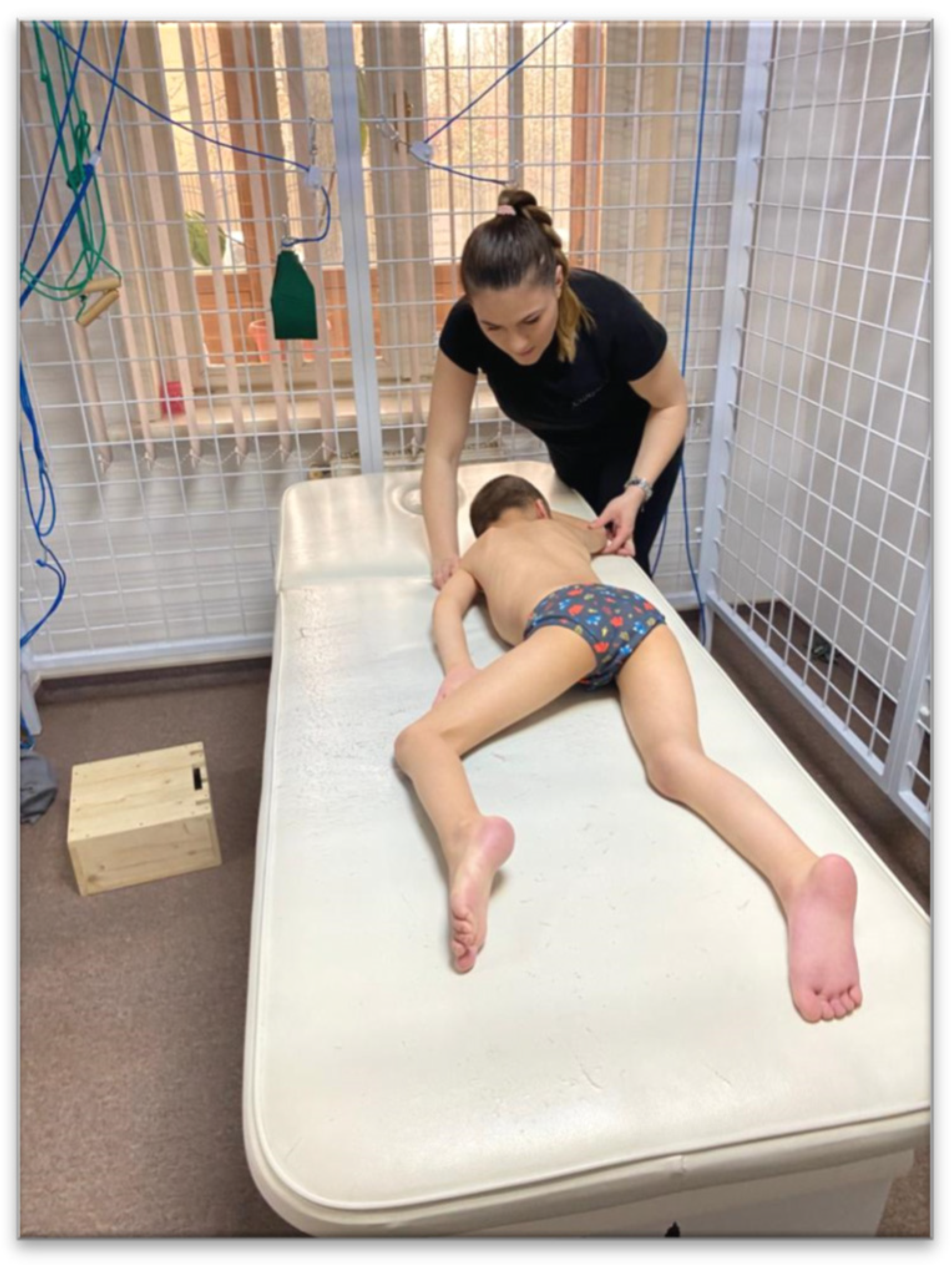
2.4.2. NDT Bobath Therapy
- Exercise 1. Quadruped imbalances (Figure 5)
- Exercise 2—Imbalances from the “kneeling” position (Figure 6)
- Exercise 3—The Cervant Knight (Figure 7)
3. Results
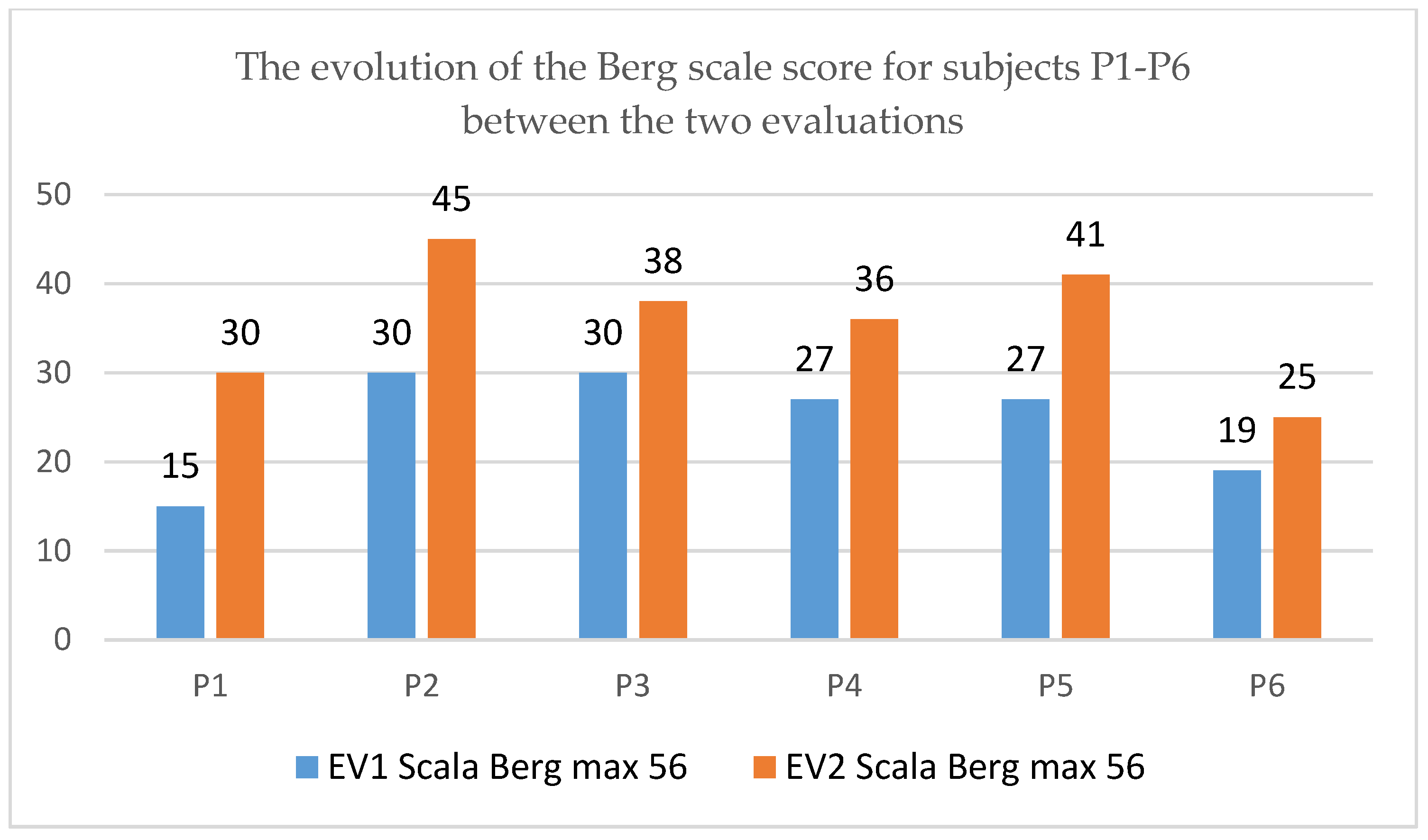
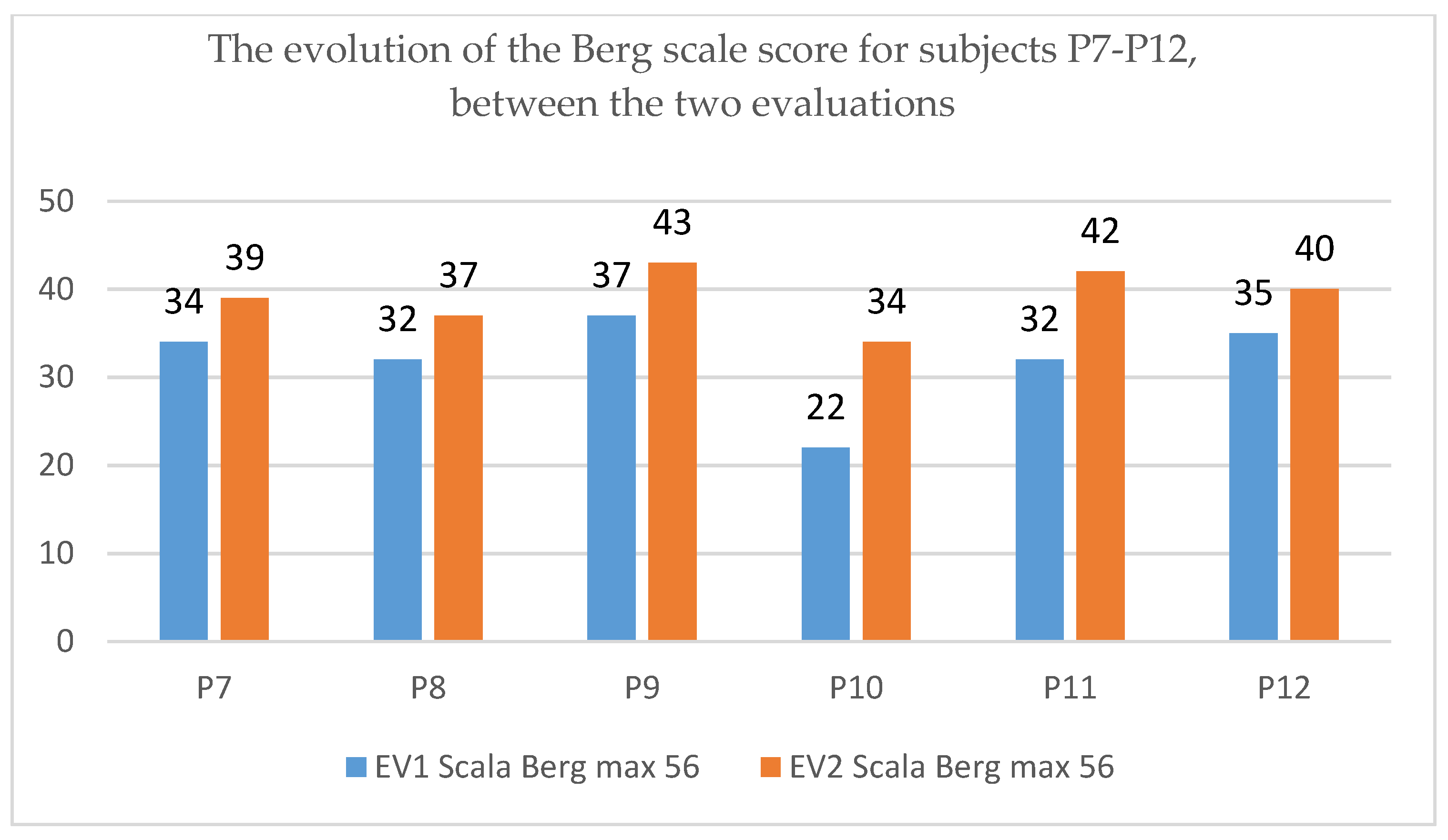
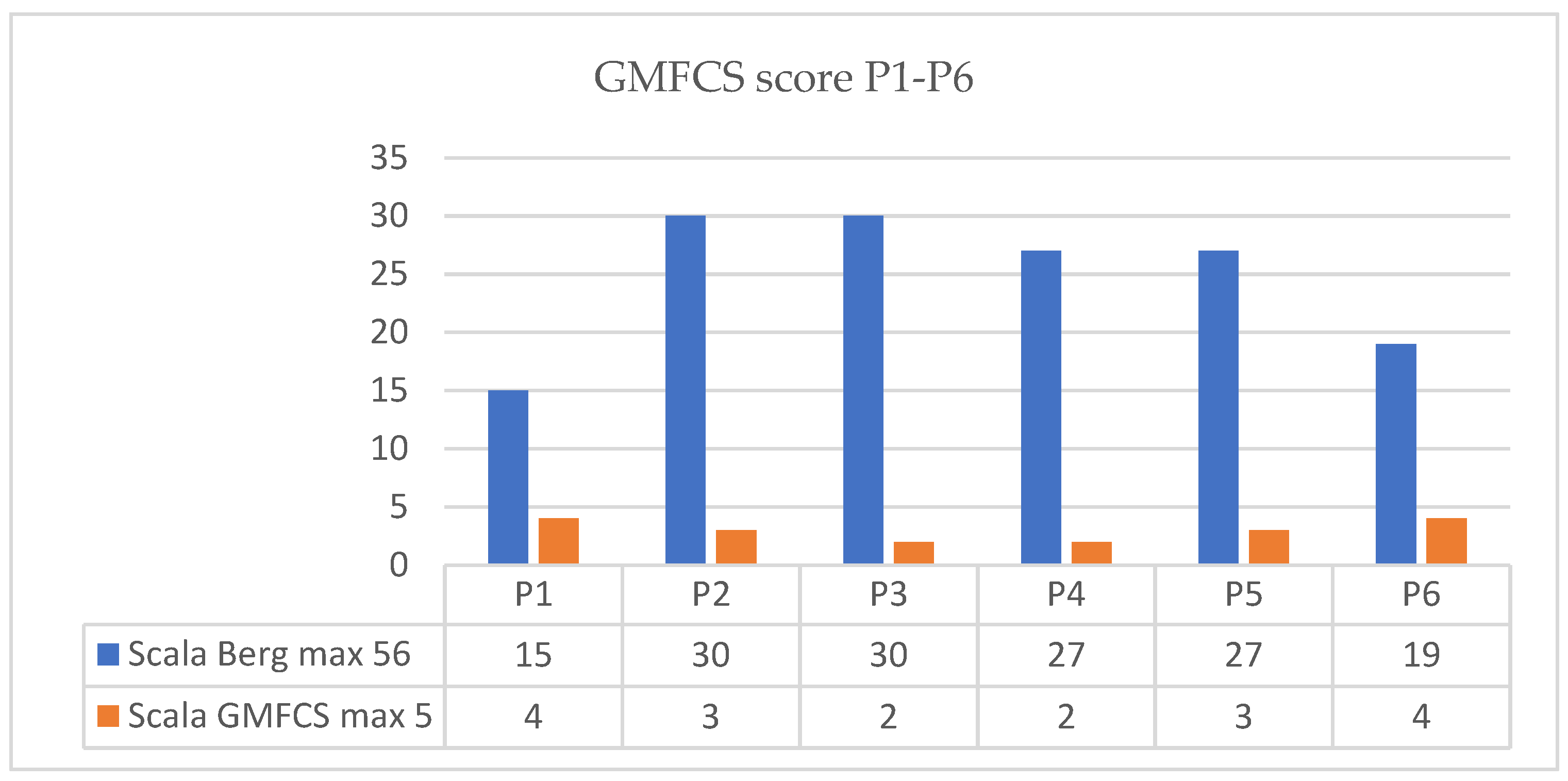
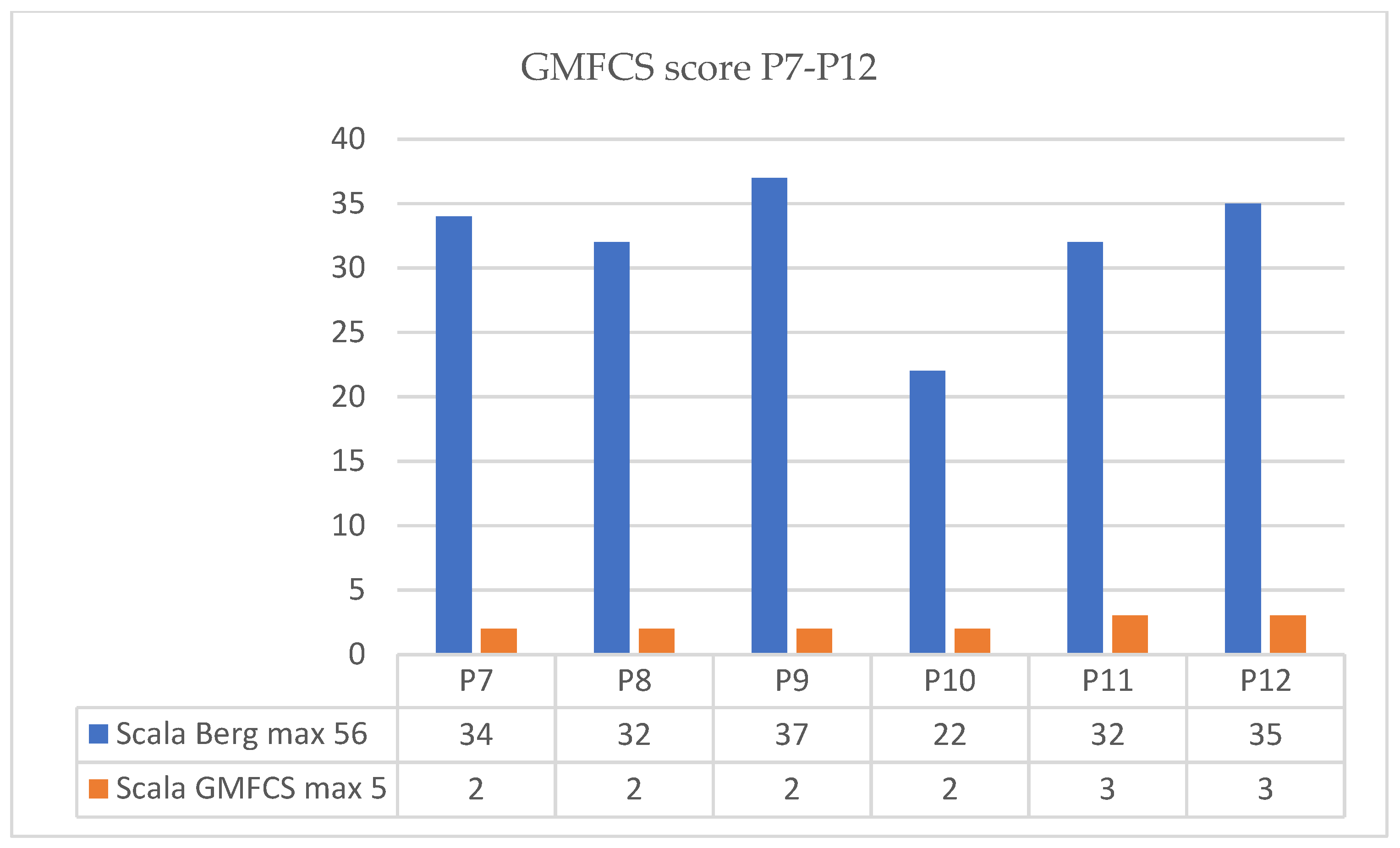
3.1. Functional Clinical Evaluation
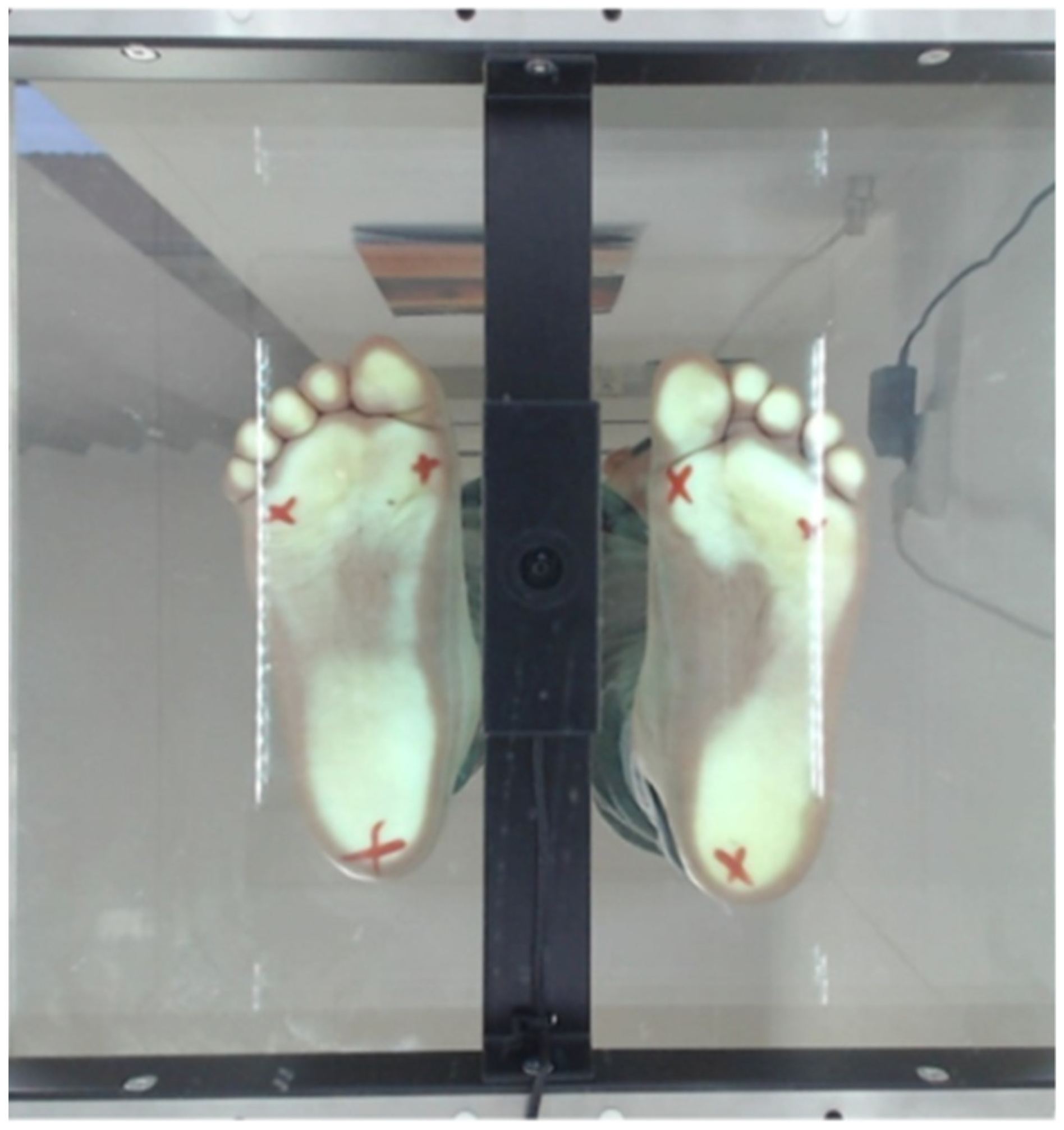
3.2. The Results of the Biomechanical Evaluation
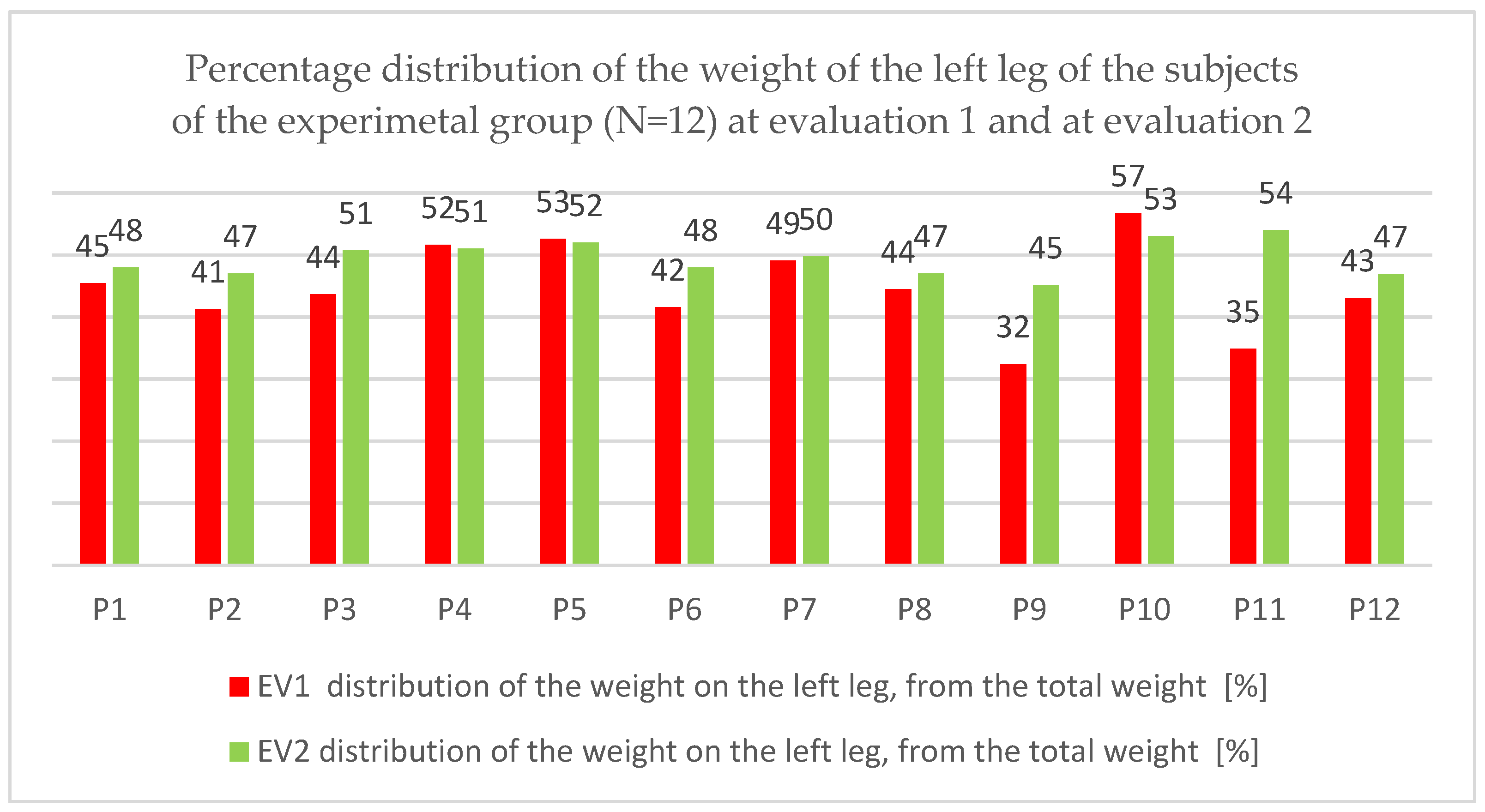
3.2.1. Weight Distribution on the Left Leg
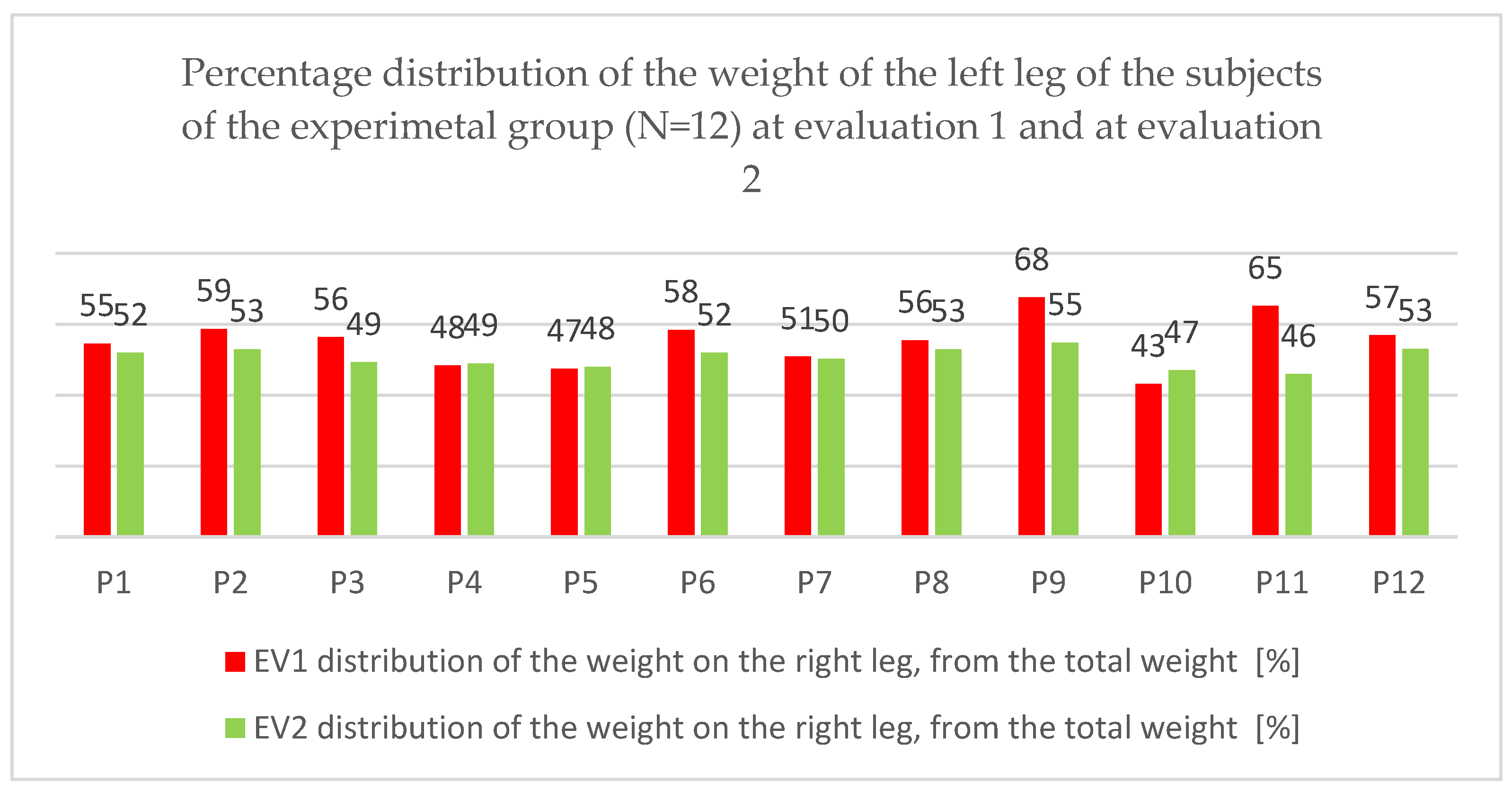
3.2.2. Weight Distribution on the Right Leg
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Puderbaugh, M.; Emmady, P.D. Neuroplasticity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Nettle, D.; Bateson, M. Adaptive developmental plasticity: What is it, how can we recognize it and when can it evolve? Proc. R. Soc. 2015, 282, 20151005. [Google Scholar] [CrossRef] [PubMed]
- Faingold, C.L. Chapter 7-Network Control Mechanisms: Cellular Inputs, Neuroactive Substances, and Synaptic Changes. In Hal Blumenfeld, Neuronal Networks in Brain Function, CNS Disorders, and Therapeutics; Faingold, C.L., Ed.; Academic Press: Cambridge, MA, USA, 2014; pp. 91–101. ISBN 9780124158047. [Google Scholar] [CrossRef]
- Yang, J.F.; Livingstone, D.; Brunton, K.; Kim, D.; Lopetinsky, B.; Roy, F.; Gorassini, M. Training to enhance walking in children with cerebral palsy: Are we missing the window of opportunity? Semin. Pediatr. Neurol. 2013, 20, 106–115. [Google Scholar] [CrossRef]
- Nielsen, J.B. How we walk: Central control of muscle activity during human walking. Neuroscientist 2003, 9, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, H.G. Delayed gait recovery with recovery of an injured corticoreticulospinal tract in a chronic hemiparetic patient: A case report. Medicine 2016, 95, e5277. [Google Scholar] [CrossRef] [PubMed]
- Trompetto, C.; Marinelli, L.; Mori, L.; Pelosin, E.; Currà, A.; Molfetta, L.; Abbruzzese, G. Pathophysiology of Spasticity: Implications for Neurorehabilitatio. BioMed Res. Int. 2014, 8, 354906. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.V.; Hoon, A.H., Jr. Cerebral palsy. Neuromolecular Med. 2006, 8, 435–450. [Google Scholar] [CrossRef]
- Abo, M.; Kakuda, W. Rehabilitation with Rtms; Springer: New York, NY, USA, 2015; 208p. [Google Scholar]
- Bhinde, S.; Patel, K.; Kori, V.; Rajagopala, S. Management of spastic cerebral palsy through multiple Ayurveda treatment modalities. AYU Int. Q. J. Res. Ayurveda 2014, 35, 462. [Google Scholar] [CrossRef]
- Levin, H.S.; Song, J.; Ewing-Cobbs, L.; Chapman, S.B.; Mendelsohn, D. Word fluency in relation to severity of closed head injury, associated frontal brain lesions, and age at injury in children. Neuropsihologia 2001, 39, 122–131. [Google Scholar] [CrossRef]
- Bobath, K.; Bobath, B. The Neuro-Developmental Treatment of Cerebral Palsy. Phys. Ther. 1967, 47, 1039–1043. [Google Scholar] [CrossRef]
- Hyungwon Lim, T.K. Effects of Vojta Therapy on Gait of Children with Spastic Diplegia. J. Phys. Ther. Sci. 2013, 25, 1605–1608. [Google Scholar] [CrossRef]
- Marquez de la Plata, C.D.; Hart, T.; Hammond, F.M.; Frol, A.B.; Hudak, A.; Harper, C.R.; O’Neil-Pirozzi, T.M.; Whyte, J.; Carlile, M.; Diaz-Arrastia, R. Impact of age on long-term recovery from traumatic brain injury. Arch. Phys. Med. Rehabil. 2008, 89, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Beckung, E.; Carlsson, G.; Carlsdotter, S.; Uvebrant, P. The natural history of gross motor development in children with cerebral palsy aged 1 to 15 years. Dev. Med. Child. Neurol. 2007, 49, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.S.; Pitts, L.H.; Lovely, M.; Edwards, M.S.B.; Bartkowski, H.M. Outcome from severe head injury in children and adolescents. J. Neurosurg. 1985, 62, 194–199. Available online: https://thejns.org/view/journals/j-neurosurg/62/2/article-p194.xml (accessed on 4 September 2022). [CrossRef]
- Rain, S. The Current theoretical assumptions of the bobath concept as determined by the membres of BBTA. Psysiotherapy Theory Pract. 2007, 23, 137–157. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, G. Humeral external rotation handling by using the Bobath concept approach affects trunk extensor muscles electromyography in children with cerebral palsy. Reserch Dev. Disabil. 2014, 20, 134–141. [Google Scholar] [CrossRef]
- Rogers, B.; Msall, M.; Owens, T.; Guernsey, K.; Brody, A.; Buck, G.; Hudak, M. Cystic periventricular leukomalacia and type of cerebral palsy in preterm infants. J. Pediatr. 1994, 125, S1–S8. [Google Scholar] [CrossRef]
- Al Tawil, K.I.; El Mahdy, H.S.; Al Rifai, M.T.; Tamim, H.M.; Ahmed, I.A.; Al Saif, S.A. Risk Factors for Isolated Periventricular Leukomalacia. Pediatr. Neurol. 2012, 46, 149–153. [Google Scholar] [CrossRef]
- Ment, L.R.; Hirtz, D.; Hüppi, P.S. Imaging biomarkers of outcome in the developing preterm brain. Lancet Neurol. 2009, 8, 1042–1055. [Google Scholar] [CrossRef]
- Nanjundagowda, V.K. Cerebral Palsy Early Stimulation; Jaypee Brothers Medical Publishers (P) Ltd.: New Delhi, India, 2014; pp. 90–145. ISBN 10: 9350903016/13: 9789350903018. [Google Scholar]
- Berg, K.; Wood-Dauphinėe, S.; Williams, J.I.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Cațan, L.; Cerbu, S.; Amaricai, E.; Suciu, O.; Horhat, D.I.; Popoiu, C.M.; Adam, O.; Boia, E. Assessment of Static Plantar Pressure, Stabilometry, Vitamin D and Bone Mineral Density in Female Adolescents with Moderate Idiopathic Scoliosis. Int. J. Environ. Res. Public Health 2020, 17, 2167. [Google Scholar] [CrossRef]
- Vincent, W.; Weir, J. Statistics in Kinesiology. In Human Kinetics, 4th ed.; NRC Research Press: Champaign, IL, USA, 2012; ISBN 13 978-1-4504-0254-5. Available online: www.HumanKinetics.com (accessed on 4 September 2022).
- Addinsoft. XLSTAT Statistical and Data Analysis Solution; Addinsoft: New York, NY, USA, 2022; Available online: https://www.xlstat.com/en (accessed on 4 September 2022).
- Louie, D.R.; Eng, J.J. Berg balance scale score at admission can predict walking suitable for community ambulation at discharge from inpatient stroke rehabilitation. J. Rehabil. Med. 2018, 50, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Epple, C.; Maurer-Burkhard, B.; Lichti, M.C.; Steiner, T. Vojta therapy improves postural control in very early stroke rehabilitation: A randomised controlled pilot trial. Neurol. Res. Pract. 2020, 2, 23. [Google Scholar] [CrossRef] [PubMed]
- Kavlak, E. Effectiveness of Bobath therapy on balance in cerebral palsy. Cukurova Med. J. 2018, 43, 975–981. [Google Scholar] [CrossRef]
- Moazma, J.S. Effectiveness of Bobath and conventional tratment in cerebral palsy children. Rawal. Med. J. 2020, 45, 974–976. Available online: https://www.rmj.org.pk/fulltext/27-1563944706.pdf (accessed on 4 September 2022).
- Zanon, M.A.; Pacheco, R.L.; Latorraca, C.O.C.; Martimbianco, A.L.C.; Pachito, D.V.; Riera, R. Neurodevelopmental Treatment (Bobath) for Children with Cerebral Palsy: A Systematic Review. J. Child. Neurol. 2019, 34, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Mengibar, J.M.; Menendez-Pardiñas, M.; Santonja-Medina, F. Is the implementation of Vojta therapy associated with faster gross motor development in children with cerebral palsy? Clin. Neurosci. 2021, 74, 329–336. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject Code (n = 12) | Age [Years] | Weight G [kg] | Height I [cm] | BMI = G/I*I [Kg/m2] |
|---|---|---|---|---|
| P1 | 7 | 28.20 | 121.00 | 19.31 |
| P2 | 3 | 12.63 | 96.00 | 13.71 |
| P3 | 10 | 44.50 | 131.00 | 25.93 |
| P4 | 3 | 14.07 | 85.33 | 19.32 |
| P5 | 6 | 17.43 | 103.75 | 16.19 |
| P6 | 3 | 23.10 | 105.00 | 20.95 |
| P7 | 11 | 56.23 | 151.67 | 24.45 |
| P8 | 11 | 60.27 | 158.33 | 24.04 |
| P9 | 10 | 27.90 | 136.00 | 15.08 |
| P10 | 6 | 23.93 | 127.00 | 14.84 |
| P11 | 4 | 20.70 | 108.33 | 17.64 |
| P12 | 10 | 43.20 | 137.00 | 23.02 |
| Test | Average | SD | Minimum | Maximum | CV |
|---|---|---|---|---|---|
| EV1 | 28.33 | 6.69 | 15 | 37 | 23.62 |
| EV2 | 37.5 | 5.68 | 25 | 45 | 15.15 |
| Statistical Indicators of the Resulting Difference (EV2-EV1) | Bilateral Dependent Student t-Test | |||||
|---|---|---|---|---|---|---|
| Average | Standard Deviation | 95% Confidence Interval | Effect Size (Cohen D’test) | t Obs | df | p * |
| 9.16 | 3.97 | (6.64; 11.69) | 1.47 | 7.99 | 11 | 0.0001 |
| Average Difference (EV1-EV2) | Progress | Difference Size | The Progress Is | Null Hypotesis (Averages Are Equal) |
|---|---|---|---|---|
| 9.16 | 32.35% | Very high | Statistically significant | It is rejected |
| Patient Code | Total Weight (Kg) | Weight Distribution on Right Leg of Total Weight [%] | Weight Distribution on Right Leg of Total Weight [Kg] | Weight Distribution on Left Leg of Total Weight [%] | Weight Distribution on Left Leg of Total Weight [Kg] | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| EV1 | EV2 | EV1 | EV2 | EV1 | EV2 | EV1 | EV2 | EV1 | EV2 | |
| P1 | 28.44 | 28.36 | 45 | 48 | 12.92 | 13.61 | 55 | 52 | 15.52 | 14.75 |
| P2 | 11.72 | 12.93 | 41 | 47 | 4.84 | 6.08 | 59 | 53 | 6.88 | 6.85 |
| P3 | 42.78 | 45.81 | 44 | 51 | 18.67 | 23.23 | 56 | 49 | 24.12 | 22.58 |
| P4 | 12.76 | 15.33 | 52 | 51 | 6.59 | 7.82 | 48 | 49 | 6.18 | 7.51 |
| P5 | 15.77 | 17.46 | 53 | 52 | 8.29 | 9.08 | 47 | 48 | 7.48 | 8.38 |
| P6 | 19.37 | 23.65 | 42 | 48 | 8.05 | 11.35 | 58 | 52 | 11.31 | 12.30 |
| P7 | 51.51 | 58.83 | 49 | 50 | 25.30 | 29.26 | 51 | 50 | 26.22 | 29.57 |
| P8 | 57.35 | 64.37 | 44 | 47 | 25.50 | 30.26 | 56 | 53 | 31.84 | 34.12 |
| P9 | 25.07 | 30.68 | 32 | 45 | 8.13 | 13.85 | 68 | 55 | 16.94 | 16.83 |
| P10 | 22.67 | 24.07 | 57 | 53 | 12.87 | 12.75 | 43 | 47 | 9.80 | 11.31 |
| P11 | 13.98 | 21.04 | 35 | 54 | 4.88 | 11.35 | 65 | 46 | 9.10 | 9.68 |
| P12 | 42.74 | 43.80 | 43 | 47 | 18.41 | 20.54 | 57 | 53 | 24.32 | 23.26 |
| Min | 11.72 | 12.93 | 32.42 | 45.15 | 4.84 | 6.08 | 43.24 | 46.03 | 6.18 | 6.85 |
| Max | 57.35 | 64.37 | 56.76 | 53.97 | 25.50 | 30.26 | 67.58 | 54.85 | 31.84 | 34.12 |
| AV * | 28.68 | 32.19 | 44.74 | 49.37 | 12.87 | 15.77 | 55.26 | 50.63 | 15.81 | 16.43 |
| SD ** | 15.95 | 17.11 | 7.06 | 2.78 | 7.46 | 8.14 | 7.06 | 2.78 | 8.80 | 9.04 |
| CV *** | 55.62 | 53.13 | 15.78 | 5.62 | 58.00 | 51.62 | 12.77 | 5.48 | 55.64 | 55.00 |
| JB **** | 0.521 | 0.504 | 0.908 | 0.685 | 0.532 | 0.502 | 0.908 | 0.685 | 0.553 | 0.510 |
| Test | Average | SD | Minimum | Maximum | CV |
|---|---|---|---|---|---|
| EV1 | 55.26 | 7.06 | 43.24 | 67.58 | 12.77 |
| EV2 | 50.63 | 2.78 | 46.03 | 54.85 | 5.48 |
| Statistical Indicators of the Resulting Difference (EV2-EV1) | Bilateral Dependent Student t-Test | |||||
|---|---|---|---|---|---|---|
| Average | Standard Deviation | 95% Confidence Interval | Effect Size (Cohen D’test) | t obs | df | p * |
| 4.64 | 6.29 | (0.63; 8.63) | 0.86 | 2.552 | 11 | 0.027 |
| Average Difference (EV1-EV2) | Progress | Difference Size | The Progress Is | Null Hypotesis (Averages Are Equal) |
|---|---|---|---|---|
| 4.64 | 8.39% | Average | Statistically significant | It is rejected |
| Test | Average | SD | Minimum | Maximum | CV |
|---|---|---|---|---|---|
| EV1 | 44.74 | 7.06 | 32.42 | 56.76 | 15.78 |
| EV2 | 49.37 | 2.78 | 45.15 | 53.97 | 5.62 |
| Statistical Indicators of the Resulting Difference (EV2-EV1) | Bilateral Dependent Student t-Test | |||||
|---|---|---|---|---|---|---|
| Average | Standard Deviation | 95% Confidence Interval | Effect Size (Cohen D’test) | t Obs | df | p * |
| −4.64 | 6.29 | (8.63; 6.37) | 0.86 | 2.552 | 11 | 0.027 |
| Average Difference (EV1-EV2) | Progress | Difference Size | The Progress Is | Null Hypotesis (Averages Are Equal) |
|---|---|---|---|---|
| −4.64 | 10.36% | Big | Statistically significant | It is rejected |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ungureanu, A.; Rusu, L.; Rusu, M.R.; Marin, M.I. Balance Rehabilitation Approach by Bobath and Vojta Methods in Cerebral Palsy: A Pilot Study. Children 2022, 9, 1481. https://doi.org/10.3390/children9101481
Ungureanu A, Rusu L, Rusu MR, Marin MI. Balance Rehabilitation Approach by Bobath and Vojta Methods in Cerebral Palsy: A Pilot Study. Children. 2022; 9(10):1481. https://doi.org/10.3390/children9101481
Chicago/Turabian StyleUngureanu, Andreea, Ligia Rusu, Mihai Robert Rusu, and Mihnea Ion Marin. 2022. "Balance Rehabilitation Approach by Bobath and Vojta Methods in Cerebral Palsy: A Pilot Study" Children 9, no. 10: 1481. https://doi.org/10.3390/children9101481
APA StyleUngureanu, A., Rusu, L., Rusu, M. R., & Marin, M. I. (2022). Balance Rehabilitation Approach by Bobath and Vojta Methods in Cerebral Palsy: A Pilot Study. Children, 9(10), 1481. https://doi.org/10.3390/children9101481