
Parental Stress Assessment with the Parenting Stress Index (PSI): A Systematic Review of Its Psychometric Properties




Abstract
:1. Introduction
Present Study
2. Materials and Methods
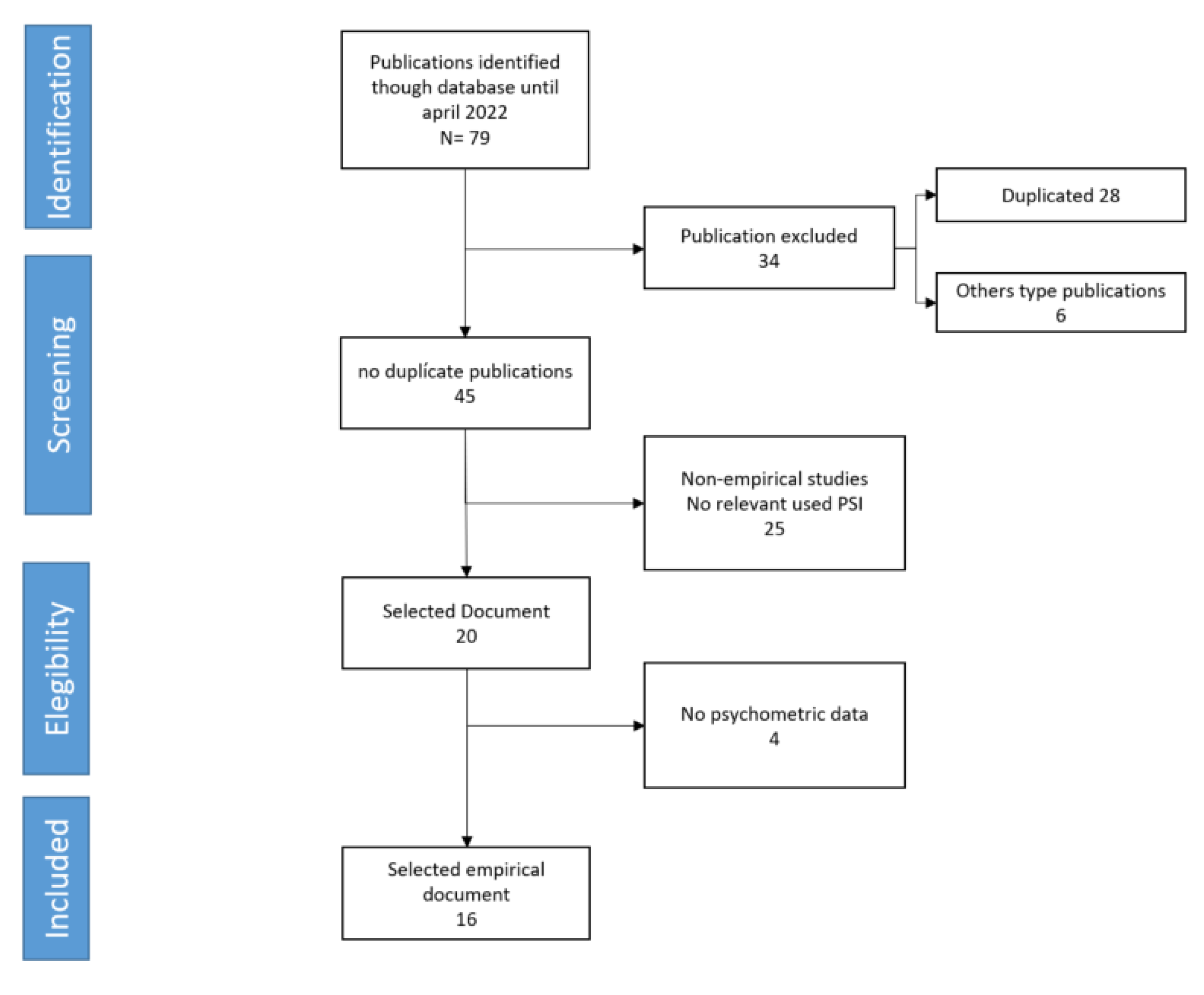
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Procedure
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haskett, M.E.; Smith-Scott, S.; Sabourin-Ward, C. Subgroups of physically abusive parents based on cluster analysis of parenting behavior and affect. Am. J. Orthopsychiatry 2004, 74, 436–447. [Google Scholar] [CrossRef] [PubMed]
- McPherson, A.V.; Lewis, K.M.; Lynn, A.E.; Haskett, M.E.; Behrend, T.S. Predictors of parenting stress for abusive and non-abusive mothers. J. Child Fam. Stud. 2009, 18, 61–69. [Google Scholar] [CrossRef]
- Bosquet-Enlow, M.; Petty, C.; Svelnys, C.; Gusman, M.; Huezo, M.; Malin, A.; Wright, R.J. Differential Effects of Stress Exposures, Caregiving Quality, and Temperament in Early Life on Working Memory versus Inhibitory Control in Preschool-Aged Children. Dev. Neuropsychol. 2019, 44, 339–356. [Google Scholar] [CrossRef]
- Kochanova, K.; Pittman, L.D.; McNeela, L. Parenting Stress and Child Externalizing and Internalizing Problems Among Low-Income Families: Exploring Transactional Associations. Child Psychiatry Hum. Dev. Vol. 2022, 53, 76–88. [Google Scholar] [CrossRef]
- Ward, K.P.; Lee, S.J. Mothers’ and Fathers’ Parenting Stress, Responsiveness, and Child Well-being Among Low-Income Families. Child. Youth Serv. Rev. 2020, 116, 105218. [Google Scholar] [CrossRef] [PubMed]
- Anastopoulos, A.D.; Shelton, T.L.; DuPaul, G.J.; Guevremont, D.C. Parent training for attention-deficit hyperactivity disorder: Its impact on parent functioning. J. Abnorm. Child Psychol. 1993, 21, 581–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deater-Deckard, K.I.R.B.Y.; Dodge, K.A.; Bates, J.E.; Pettit, G.S. Multiple risk factors in the development of externalizing behavior problems: Group and individual differences. Dev. Psychopathol. 1998, 10, 469–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hastings, R.P.; Daley, D.; Burns, C.; Beck, A. Maternal distress and expressed emotion: Cross-sectional and longitudinal relationships with behavior problems of children with intellectual disabilities. Am. J. Ment. Retard. 2006, 11, 48–61. [Google Scholar] [CrossRef]
- Kersh, J.; Hedvat, T.T.; Hauser-Cram, P.; Warfield, M.E. The contribution of marital quality to the well-being of parents of children with developmental disabilities. J. Intellect. Disabil. Res. 2006, 50, 883–893. [Google Scholar] [CrossRef]
- Suarez, L.M.; Baker, B.L. Child externalizing behavior and parents’ stress: The role of social support. Fam. Relat. Interdiscip. J. Appl. Fam. Stud. 1997, 46, 373–381. [Google Scholar] [CrossRef]
- Eisenhower, A.S.; Baker, B.L.; Blacher, J. Children’s delayed development and behavior problems: Impact on mothers’ perceived physical health across early childhood. Soc. Sci. Med. 2009, 68, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Oelofsen, N.; Richardson, P. Sense of coherence and parenting stress in mothers and fathers of preschool children with developmental disability. J. Intellect. Dev. Disabil. 2006, 31, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Coldwell, J.; Pike, A.; Dunn, J. Household chaos-links with parenting and child behavior. J. Child Psychol. Psychiatry 2006, 47, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Crnic, K.A.; Gaze, C.; Hoffman, C. Cumulative parenting stress across the preschool period: Relations to maternal parenting and child behaviour at age 5. Infant Child Dev. 2005, 14, 117–132. [Google Scholar] [CrossRef]
- Baker, B.L.; McIntyre, L.L.; Blacher, J.; Crnic, K.; Edelbrock, C.; Low, C. Pre-school children with and without developmental delay: Behaviour problems and parenting stress over time. J. Intellect. Disabil. Res. 2003, 47, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Briggs-Gowan, M.J.; Carter, A.S.; Skuban, E.M.; Horwitz, S.M. Prevalence of social-emotional and behavioral problems in a community sample of 1-and 2-year-old children. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 811–819. [Google Scholar] [CrossRef]
- Donenberg, G.; Baker, B.L. The impact of young children with externalizing behaviors on their families. J. Abnorm. Child Psychol. 1993, 21, 179–198. [Google Scholar] [CrossRef]
- Johnston, C.; Mash, E.J. Families of children with attention-deficit/hyperactivity disorder: Review and recommendations for future research. Clin. Child Fam. Psychol. Rev. 2001, 4, 183–207. [Google Scholar] [CrossRef]
- Coldwell, J.; Pike, A.; Dunn, J. Maternal differential treatment and child adjustment: A multi-informant approach. Soc. Dev. 2008, 17, 596–612. [Google Scholar] [CrossRef]
- Holly, L.E.; Fenley, A.R.; Kritikos, T.K.; Merson, R.A.; Abidin, R.R.; Langer, D.A. Evidence-base update for parenting stress measures in clinical samples. J. Clin. Child Adolesc. Psychol. 2019, 48, 685–705. [Google Scholar] [CrossRef]
- Brannan, A.M.; Helflinger, C.A.; Bickman, L. The Caregiver Strain Questionnaire: Measuring the Impact on the Family of Living with a Child with Serious Emotional Disturbance. J. Emot. Behav. Disord. 1997, 5, 212–222. [Google Scholar] [CrossRef]
- Crnic, K.; Greenberg, M. Minor parenting stresses with young children. Child Dev. 1990, 61, 1628–1637. [Google Scholar] [CrossRef] [PubMed]
- Miles, M.; Funk, S.; Carison, J. Parental Stressor Scale: Neonatal intensive care unit. Nurs. Res. 1993, 42, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Sheras, P.; Abidin, R.; Konold, T.R. SIPA, Stress Index for Parents of Adolescents: Professional Manual; Lutz, F.L., Ed.; Psychological Assessment Resources, Inc.: Odessa, FL, USA, 1998. [Google Scholar]
- Friedrich, W.N.; Greenberg, M.T.; Crnic, K. A short-form of the Questionnaire on Resources and Stress. Am. J. Ment. Defic. 1983, 88, 41–48. [Google Scholar]
- Berry, J.; Jones, W. The Parental Stress Scale: Initial psychometric evidence. J. Soc. Pers. Relatsh. 1995, 12, 463–472. [Google Scholar] [CrossRef]
- Cutrona, C.E. Causal attributions and perinatal depression. J. Abnorm. Psychol. 1983, 92, 161–172. [Google Scholar] [CrossRef]
- Dennis, C.L.; Brown, H.K.; Brennenstuhl, S. Development, Psychometric Assessment, and Predictive Validity of the Postpartum Childcare Stress Checklist. Nurs. Res. 2018, 67, 439–446. [Google Scholar] [CrossRef]
- Hung, C.H. Measuring postpartum stress. J. Adv. Nurs. 2005, 50, 417–424. [Google Scholar] [CrossRef]
- Park, J.H.; Karmaus, W.; Zhang, H.M. Prevalence of a Risk Factors for Depressive Symptoms in Korean Women throughout Pregnancy and in Postpartum Period. Asian Nurs. Res. 2015, 9, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Abidin, R. Parenting Stress Index; Pediatric Psychology Press: Charlottesville, VA, USA, 1983. [Google Scholar]
- Haskett, M.E.; Ahern, L.S.; Ward, C.S.; Allaire, J.C. Factor Structure Validity of the Parenting Stress Index-Short Form. J. Clin. Child Adolesc. Psychol. 2006, 35, 302–312. [Google Scholar] [CrossRef]
- Zaidman-Zait, A.; Mirenda, P.; Zumbo, B.D.; Wellington, S.; Dua, V.; Kalynchuk, K. An item response theory analysis of the Parenting Stress Index-Short Form with parents of children with Autism Spectrum Disorders. J. Child Psychol. Psychiatry 2010, 51, 1269–1277. [Google Scholar] [CrossRef]
- Miodrag, N.; Burke, M.; Tanner-Smith, E.; Hodapp, R.M. Adverse health in parents of children with disabilities and chronic health conditions: A meta-analysis using the Parenting Stress Index’s Health Sub-domain. J. Intellect. Disabil. Res. 2015, 59, 257–271. [Google Scholar] [CrossRef]
- Abidin, R. Parenting Stress Index; Pediatric Psychology Press: Charlottesville, VA, USA, 1990. [Google Scholar]
- Basa, J. Estrés Parental con Hijos Autistas: Un Estudio Comparativo. Doctoral Dissertation Facultad “Teresa de Ávila”, Paraná: Unpublished Work. 2010. Available online: https://repositorio.uca.edu.ar/handle/123456789/578 (accessed on 5 June 2022).
- Abidin, R. Parenting Stress Index Fourth Edition (PSI-4); PAR: Odessa, FL, USA, 2012. [Google Scholar]
- Tam, K.K.; Chan, Y.C.; Wong, C.K.M. Validation of the Parenting Stress Index among Chinese mothers in Hong Kong. J. Community Psychol. 1994, 22, 211–223. [Google Scholar] [CrossRef]
- Leung, S.S.L.; Leung, C.; Chan, R. Perceived child behavior problems, parenting stress, and marital satisfaction: Comparison of new arrival and local parents of preschool children in Hong Kong. Hong Kong Med. J. 2007, 13, 364–371. Available online: https://www.hkmj.org/abstracts/v13n5/364.htm (accessed on 7 June 2022).
- Santos, S.V. Adaptaçao portuguesa, para crianças emidade escolar, do Parenting Stress Index (PSI): Resultados preliminares. Rev. Port. Psicol. 1992, 28, 115–132. Available online: https://sites.google.com/site/revistaportuguesadepsicologia/numeros-publicados/vol-28-1992/resumo-28-115 (accessed on 10 July 2022).
- Touchèque, M.; Etienne, A.M.; Stassart, C.; Catale, C. Validation of the French version of the Parenting Stress Index-Short form (fourth edition). J. Community Psychol. 2016, 44, 419–425. [Google Scholar] [CrossRef]
- Bigras, M.; LaFreniere, P.J.; Dumas, J.E. Discriminant validity of the parent and child scales of the Parenting Stress Index. Early Educ. Dev. 1996, 7, 167–178. [Google Scholar] [CrossRef]
- Tarkka, M.T. Predictors of maternal competence by first-time mothers when the child is 8 months old. J. Adv. Nurs. 2003, 41, 233–240. [Google Scholar] [CrossRef]
- Vermaes, I.P.; Janssens, J.M.A.M.; Mullaart, R.A.; Vinck, A.; Gerris, J.R.M. Parents’ personality and parenting stress in families of children with spina bifida. Child Care Health Dev. 2008, 34, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Wang, M.C.; Gao, Y.; Zeng, H.; Yang, W.; Chen, W.; Zhao, S.; Qi, S. Refining the Parenting Stress Index-Short Form (PSI-SF) in Chinese Parents. Assessment 2021, 28, 551–566. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Gopalan, G.; Harrington, D. Validation of the Parenting Stress Index-Short Form with Minority Caregivers. Res. Soc. Work Pract. 2016, 26, 429–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenaro, C.; Gutiérrez-Bermejo, B. Análisis de la escala de estrés parental-forma abreviada en padres de hijos con discapacidad intelectual mediante el modelo de Rasch. Rev. Iberoam. Diagn. Eval. Psicol. 2015, 1, 68–76. Available online: https://www.redalyc.org/pdf/4596/459645431007.pdf (accessed on 6 July 2022).
- Rivas, G.R.; Arruabarrena, I.; de Paúl, J. Parenting Stress Index-Short Form: Psychometric properties of the Spanish version in mothers of children aged 0 to 8 years. Psychosoc. Interv. 2021, 27, 27–34. [Google Scholar] [CrossRef]
- Pérez-Padilla, J.; Menéndez, S.; Lozano, O. Validity of the Parenting Stress Index Short Form in a Sample of At-Risk Mothers. Eval. Rev. 2015, 39, 428–446. [Google Scholar] [CrossRef]
- Aracena, M.; Gómez, E.; Undurraga, C.; Leiva, L.; Marinkovic, K.; Molina, Y. Validity and Reliability of the Parenting Stress Index Short Form (PSI-SF) Applied to a Chilean Sample. J. Child Fam. Stud. 2016, 25, 3554–3564. [Google Scholar] [CrossRef]
- Dardas, L.A.; Ahmad, M.M. Psychometric properties of the Parenting Stress Index with parents of children with autistic disorder. J. Intellect. Disabil. Res. 2014, 58, 560–571. [Google Scholar] [CrossRef]
- Derguy, C.; Loyal, D.; Devouche, E.; Cappe, E. Should we use the Parental Stress Index-Short Form in parents of children with ASD? A French validation study. Res. Dev. Disabil. 2020, 104, 103716. [Google Scholar] [CrossRef]
- Emam, M.M.; Al-Hendawi, M.; Gaafar Ali, D. Stress in families of children with disabilities: An examination of the parenting stress index-short form (PSI-SF) in three Arab Countries. Int. J. Ment. Health 2022. [Google Scholar] [CrossRef]
- Gao, X.; Lee, K. Factorial Structure and Cross-Cultural Invariance of the Parenting Stress Index-Short Form in Hong Kong and Thailand. Front. Psychol. 2021, 12, 661972. [Google Scholar] [CrossRef] [PubMed]
- Park, E.Y.; Chae, S. Rasch analysis of the Korean Parenting Stress Index Short Form (K-PSI-SF) in mothers of children with cerebral palsy. Int. J. Environ. Res. Public Health 2020, 17, 7010. [Google Scholar] [CrossRef]
- Wang, Y.; Song, J.; Chen, J.; Zhang, Y.; Wan, Q.; Huang, Z. Examining the psychometric properties of the simplified Parenting Stress Index-Short Form with Chinese parents of children with cerebral palsy. Soc. Behav. Personal. 2021, 49, 1–10. [Google Scholar] [CrossRef]
- Barroso, N.E.; Hungerford, G.M.; García, D.; Graziano, P.A.; Bagner, D.M. Psychometric properties of the Parenting Stress Index-Short Form (PSI-SF) in a high-risk sample of mothers and their infants. Psychol. Assess. 2016, 28, 1331–1335. [Google Scholar] [CrossRef] [PubMed]
- Çekiç, A.; Akbaş, T.; Hamamci, Z. Adaptation of Parenting Stress Index into Turkish: The Validity and the Realiability Study. Gaziantep Univ. J. Soc. Sci. 2015, 14, 647–667. [Google Scholar] [CrossRef] [Green Version]
- Pereira, L.M.; Viera, C.S.; De Oliveira Toso, B.R.G.; Da Silva Carvalho, A.R.; Bugs, B.M. Validation of the Parenting Stress Index for Brazilian Portuguese. Acta Paul. Enferm. 2016, 29, 671–677. [Google Scholar] [CrossRef]
- Abidin, R. The determinants of parenting behavior. J. Clin. Child Psychol. 1992, 21, 407–412. [Google Scholar] [CrossRef]
- Hambleton, R.K.; Merenda, P.; Spielberger, C. Adapting Educational and Psychological Tests for Cross Cultural Assessment; Lawrence Erlbaum Publishers: Hillsdale, NJ, USA, 2005. [Google Scholar]
- Muñiz, J.; Elosua, E.; Hambleton, R. Guidelines for the translation and adaptation of the tests: Second edition. Psicothema 2013, 25, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Brown, T. Confirmatory Factor Analysis for Applied Research; The Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Bond, T.G.; Fox, C.M. Applying the Rasch Model: Fundamental Measurement in Human Sciences; LEA: New Jersey, NJ, USA, 2001. [Google Scholar]
- de Ayala, R.J. The Theory and Practice of Item Response Theory; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Díaz-Herrero, A.; Brito, A.G.; López, J.A.; Pérez-López, J.; Martínez-Fuentes, M.T. Estructura factorial y consistencia interna de la versión española del Parenting Stress Index-Short Form. Psicothema 2010, 22, 1033–1038. Available online: https://www.psicothema.com/pdf/3837.pdf (accessed on 9 July 2022). [PubMed]


{kind=link}
| Form | Citation | Population | Reliability | Validity | |||||
|---|---|---|---|---|---|---|---|---|---|
| Sample N | Specific Sample | Internal Consistency Cronbach’s α McDonald’s ω ISR | Test–Retest | Inter-Rater Correlations | ICC | Concurrent Validity | Factorial Structure | ||
| SF-3 | Aracena et al. (2016) [50] | 336 dyads mother–child | Clinical (low-income mother–child dyads from 24 health care centers) | GPS = 0.92 PD = 0.81 P–CDI = 0.89 DC = 0.88 | NA | NA | NA | GGHQ r = 0.86 | EFA Three-factor compatible with the original version |
| SF-3 | Dardas and Ahmad (2014) [51] | N = 184 parents of children with autistic disorder (114 female) | Clinical (parents of children with autistic disorder) | GPS = 0.91 | NA | NA | NA | NA | EFA (principal components and varimax rotation) Three-factor compatible CFA |
| SF-3 | Derguy et al. (2020) [52] | N = 370 (5 samples). Parents of children with autism spectrum disorder (73.2% female and 26.8% male) | Clinical (parents of children with autism spectrum disorder) participants in various parents’ support programs on parental stress | GPS = 0.87 PD = 0.86 P–CDI = 0.82 DC = 0.80 | NA | GPS = 0.52 PD = 0.56 P–CDI = 0.33 DC = 0.49 | GPS = 0.71 PD = 0.73 P–CDI = 0.52 DC = 0.70 | HADS PD and anxiety r = 0.71 Global and Anxiety 0.60 Global and Depression 0.50 WHOQOL-BREF R = −0.50 ALES T = 0.50 L = 0.60 C = −0.23 | CFA poor confirmation three-factorial structure EFA unweighted least squares (ULS) extraction method and oblimin rotation |
| SF-3 | Emam et al. (2022) [53] | N = 867 parents had at least one child with a disability | Arabic version and trans-country studies (Oman: 380 parents; Saudi Arabia: 300 parents; Qatar: 187 parents) | GPS = 0.7 | NA | NA | NA | NA | CFA Three-factor structure supported |
| SF-3 | Gao and Lee (2021) [54] | N = 448 parent–child dyads | Cross-cultural study (Hong Kong: 258 parent–child dyads; Thailand: 190 parent–-child dyads) 15 items reduced version used | ω = 0.71 to 0.78 | NA | NA | NA | KPDS r= 0.37 to 0.42 PSDQ r = −0.25 to −0.49 | CFA Three-factor structure supported |
| SF-3 | Jenaro and Gutiérrez Bermejo (2015) [47] | N = 542 participants, parents or guardians of children with intellectual disabilities (374 female and 168 male) | Clinical (parents or guardians of children with intellectual disabilities) | ISR = 0.99 PSR = 0.94 | NA | NA | NA | NA | NA |
| SF-3 | Lee et al. (2016) [46] | N = 240 caregivers (204 mothers, 7 fathers, 1 parent, 10 grandparents, 13 others) | Clinical (Black and Latino caregivers of children with behavioral difficulties) | NA | NA | NA | NA | CES-D GPS and CES-D r = 0.61 IOWA GPS and IOWA-IO r = 0.26 GPS and IOWA-OD r = 0.45 | CFA Three-factor structure supported |
| SF-3 | Luo et al. (2021) [45] | 683 mother–father dyads | Non-clinical (Mainland Chinese parents of nonclinical children to develop a psychometrically abbreviated version of the PSI-SF) | GPS 0.86 to 0.87 PD 0.71 to 0.72 P-CDI 0.78 to 0.82 DC 0.78 to 0.79 | NA | GPS = 0.96 PD = 0.90 P-CDI = 0.92 DC = 0.93 | NA | PBQ Positive parenting −0.21 to −0.42 Corporal punishment 0.40 to 0.46 Overlook 0.20 to 0.36 CES-D r = 0.28 to 0.35 SDQ Emotion 0.25 to 0.44 Hyperactivity 0.16 to 0.39 Prosocial −0.22 to −0.37 | EFA Principal axis factor and promax rotation CFA No three-factor structure supported |
| SF-3 | Park and Chae (2020) [55] | N = 114 mothers of children with cerebral palsy | Clinical (mothers of children with cerebral palsy) | GPS 0.91 PD 0.90 P-CDI 0.78 DC 0.83 PSR = 0.92 ISR = 0.95 | NA | NA | NA | NA | NA |
| SF-3 | Pérez-Padilla et al. (2015) [49] | N = 149 mothers (109 at-risk mothers and 40 mothers, sample of community families) | Clinical (sample of at-risk mothers) | GPS 0.89 PD 0.79 Child rearing stress 0.85 | NA | NA | NA | PSOC 0.48 PLOC −0.34 GGHQ 0.39 | NA |
| SF-3 | Rivas et al. (2021) [48] | N = 309 mothers (203 with difficulties managing their children’s behavior and 106 from the general population) | Clinical (mothers with problems to cope with their children’s behavior) and community sample | GPS 0.88 to 0.93 PD 0.85 to 0.86 P-CDI 0.86 to 0.91 DC 0.79 to 0.85 | NA | NA | NA | BDI-II r = 0.51 B-CPAI r = 0.46 ECBI Intensity r = 0.50 Problem r = 0.54 | CFA Three-factor structure supported |
| SF-3 | Wang et al. (2021) [56] | N = 486 (117 fathers and 369 mothers) | Clinical (parents of children with cerebral palsy) | GPS PD 0.83 P-CDI 0.87 DC 0.76 | NA | NA | NA | MSPS −0.34 | CFA Three-factor structure supported |
| SF-4 | Barroso et al. (2016) [57] | N = 58 mothers and their 12- to 15-month-old infants (predominately Hispanic low-incoming backgrounds) | Clinical (mothers of infants with clinical behavior problems in 3 times assessment) | GPS 0.91 0.92 0.93 PD 0.75 0.71 0.79 P-CDI 0.85 0.87 0.83 DC 0.82 0.81 0.84 | 0.61 0.66 0.58 | NA | 0.77 0.78 0.77 | CES-D 0.53 PLOC-SF 0.44 ITSEA Externalizing 0.50 Internalizing 0.38 Dysregulation 0.44 | NA |
| SF-4 | Touchèque et al. (2016) [41] | N = 318 (4 samples) (Sample 1: 163 mothers, 47 fathers Sample 2: 19 mothers, 19 fathers Sample 3: 18 fathers, 17 mothers Sample 4: 18 mothers, 17 fathers) | GPS 0.89 PD 0.81 P-CDI 0.79 DC 0.79 | NA | NA | NA | STAIC −0.37 CDI 0.57 FES 0.70 | CFA Three-factor structure supported | |
| LF-4 | Çekiç et al. (2015) [58] | N = 386 parents (215 mothers; 171 fathers) | Clinical (parents of children with psychological problems) | DI 0.75 RE 0.56 MO 0.69 AC 0.81 AD 0.74 DE 0.86 TOTAL CD 0.92 CO 0.73 AT0.79 RO 0.79 DP 0.82 SP 0.89 IS 0.73 HE 0.70 Total PD 0.95 | 0.78 | NA | NA | NA | CFA Separately confirmed factor structure for child domain and parent domain. |
| LF-4 | Pereira et al. (2016) [59] | N = 53 mothers of premature infants | Clinical sample | DI 0.88 RE 0.88 MO 0.88 AC 0.89 AD 0.88 DE 0.88 TOTAL CD 0.87 CO 0.89 AT 0.91 RO 0.90 DP 0.88 SP 0.89 IS 0.88 HE 0.89 Total PD 0.88 PSI Global 0.91 | NA | NA | NA | NA | EFC Principal components and varimax rotation from 13 subdomains. Two factor structure (child domain and parent domain) are described |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ríos, M.; Zekri, S.; Alonso-Esteban, Y.; Navarro-Pardo, E. Parental Stress Assessment with the Parenting Stress Index (PSI): A Systematic Review of Its Psychometric Properties. Children 2022, 9, 1649. https://doi.org/10.3390/children9111649
Ríos M, Zekri S, Alonso-Esteban Y, Navarro-Pardo E. Parental Stress Assessment with the Parenting Stress Index (PSI): A Systematic Review of Its Psychometric Properties. Children. 2022; 9(11):1649. https://doi.org/10.3390/children9111649
Chicago/Turabian StyleRíos, Mercedes, Sara Zekri, Yurena Alonso-Esteban, and Esperanza Navarro-Pardo. 2022. "Parental Stress Assessment with the Parenting Stress Index (PSI): A Systematic Review of Its Psychometric Properties" Children 9, no. 11: 1649. https://doi.org/10.3390/children9111649
APA StyleRíos, M., Zekri, S., Alonso-Esteban, Y., & Navarro-Pardo, E. (2022). Parental Stress Assessment with the Parenting Stress Index (PSI): A Systematic Review of Its Psychometric Properties. Children, 9(11), 1649. https://doi.org/10.3390/children9111649