
Visual Feedback and Virtual Reality in Gait Rehabilitation of Hemiparetic Children and Teenagers after Acquired Brain Injury: A Pilot Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
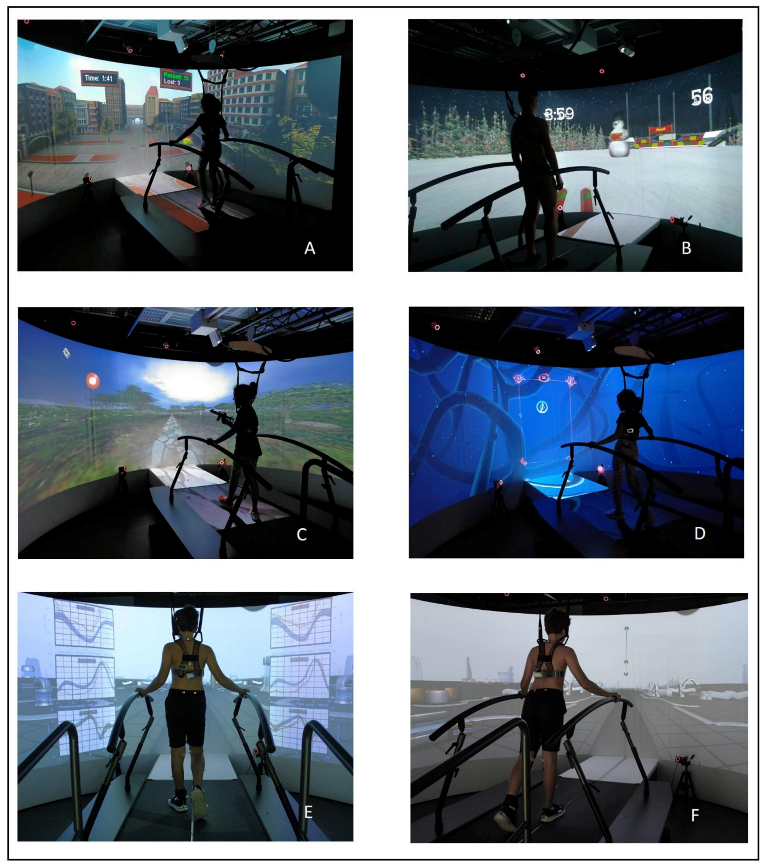
2.2. Grail
2.3. Outcome Measures
2.3.1. Gross Motor Function Measure
2.3.2. 6–Minute Walking Test
2.3.3. Three-Dimensional Gait Analysis (3dga) over the Grail System
2.4. Participants
2.5. Initial Assessment and Rehabilitation Program
2.6. Training
3. Results
Participants and Training Activities
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, H.S.; Park, Y.J.; Park, S.W. The Effects of Virtual Reality Training on Function in Chronic Stroke Patients: A Systematic Review and Meta-Analysis. Biomed Res. Int. 2019, 2019, 7595639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, T.; Nam, C.S.; Chen, K.B. Immersion of Virtual Reality for Rehabilitation—Review. Appl. Ergon. 2018, 69, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Aramaki, A.L.; Sampaio, R.F.; Caroline, A.; Reis, S.; Cavalcanti, A.; Caetano, F.; Silva, M. Virtual Reality in the Rehabilitation of Patients with Stroke: An Integrative Review. Arq Neuropsiquiatr. 2018, 77, 268–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darekar, A.; McFadyen, B.J.; Lamontagne, A.; Fung, J. Efficacy of Virtual Reality-Based Intervention on Balance and Mobility Disorders Post-Stroke: A Scoping Review. J. Neuroeng. Rehabil. 2015, 12, 46. [Google Scholar] [CrossRef] [Green Version]
- Laver, K.E.; Lange, B.; George, S.; Je, D.; Saposnik, G.; Crotty, M. Virtual Reality for Stroke Rehabilitation (Review). Cochrane Database Syst. Rev. 2018, 11, CD008349. [Google Scholar] [CrossRef]
- Booth, A.T.; Buizer, A.I.; Harlaar, J.; Steenbrink, F.; van der Krogt, M.M. Immediate Effects of Immersive Biofeedback on Gait in Children With Cerebral Palsy. Arch. Phys. Med. Rehabil. 2019, 100, 598–605. [Google Scholar] [CrossRef]
- Zhang, B.; Li, D.; Liu, Y.; Wang, J.; Xiao, Q. Virtual Reality for Limb Motor Function, Balance, Gait, Cognition and Daily Function of Stroke Patients: A Systematic Review and Meta—Analysis. J. Adv. Nurse 2020, 77, 3255–3273. [Google Scholar] [CrossRef]
- Luque-moreno, C.; Ferragut-garcías, A.; Rodríguez-blanco, C.; Heredia-rizo, A.M.; Oliva-pascual-vaca, J.; Kiper, P.; Oliva-pascual-vaca, Á. A Decade of Progress Using Virtual Reality for Poststroke Lower Extremity Rehabilitation: Systematic Review of the Intervention Methods. BioMed Res. Int. 2015, 2015, 342529. [Google Scholar] [CrossRef] [Green Version]
- Olivieri, I.; Chiappedi, M.; Meriggi, P.; Mazzola, M.; Grandi, A.; Angelini, L. Rehabilitation of Children with Hemiparesis: A Pilot Study on the Use of Virtual Reality. Biomed Res. Int. 2013, 2013, 695935. [Google Scholar] [CrossRef] [Green Version]
- Biffi, E.; Beretta, E.; Cesareo, A.; Maghini, C.; Turconi, A.C.; Reni, G.; Strazzer, S. An Immersive Virtual Reality Platform to Enhance Walking Ability of Children with Acquired Brain Injuries. Methods Inf. Med. 2017, 56, 119–126. [Google Scholar] [CrossRef]
- Beyaert, C.; Vasa, R.; Frykberg, G.E. Gait Post-Stroke: Pathophysiology and Rehabilitation Strategies La Marche Après Accident Vasculaire Cérébral: Physiopathologie et Stratégies de Rééducation. Neurophysiol. Clin. Clin. Neurophysiol. 2015, 45, 335–355. [Google Scholar] [CrossRef] [PubMed]
- Winters, T.F.; Gage, J.R.; Hicks, R. Gait Patterns in Spastic Hemiplegia in Children and Young Adults. J. Bone Jt. Surg. 1987, 69, 437–441. [Google Scholar]
- Mulroy, S.; Gronley, J.; Weiss, W.; Newsam, C.; Perry, J. Use of Cluster Analysis for Gait Pattern Classification of Patients in the Early and Late Reco v Ery Phases Following Stroke. Gait Posture 2003, 18, 114–125. [Google Scholar] [CrossRef]
- Wong, A.M.; Pei, Y.; Hong, W.; Chung, C.; Lau, Y.; Chen, C.P. Foot Contact Pattern Analysis in Hemiplegic Stroke Patients: An Implication for Neurologic Status Determination. Arch. Phys. Med. Rehabil. 2004, 85, 1625–1630. [Google Scholar] [CrossRef] [PubMed]
- Knutsson, E.; Richards, C. Different Types of Disturbed Motor Control in Gait of Hemiparetic Patients. Brain 1979, 102, 405–430. [Google Scholar] [CrossRef]
- Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Knaflitz, M. Multiple Gait Patterns within the Same Winters Class in Children with Hemiplegic Cerebral Palsy. Clin. Biomech. 2015, 30, 908–914. [Google Scholar] [CrossRef] [Green Version]
- Linder-Lucht, M.; Othmer, V.; Walther, M.; Vry, J.; Michaelis, U.; Stein, S.; Weissenmayer, H.; Korinthenberg, R.; Mall, V. Gross Motor Function Measure-Traumatic Brain Injury Study Group Validation of the Gross Motor Function Measure for Use in Children and Adolescents with Traumatic Brain Injuries. Pediatrics 2007, 120, e880-6. [Google Scholar] [CrossRef]
- Andersson, C.; Asztalos, L.; Mattsson, E. Six-Minute Walk Test in Adults with Cerebral Palsy. A Study of Reliability. Clin. Rehabil. 2006, 20, 488–495. [Google Scholar] [CrossRef]
- Mossberg, K.A.; Fortini, E. Responsiveness and Validity of the With Traumatic Brain Injury. Phys. Ther. 2012, 92, 726–733. [Google Scholar] [CrossRef]
- Geiger, R.; Strasak, A.; Treml, B.; Gasser, K.; Kleinsasser, A.; Fischer, V.; Geiger, H.; Loeckinger, A.; Stein, J.I. Six-Minute Walk Test in Children and Adolescents. J. Pediatr. 2007, 150, 395–399.e2. [Google Scholar] [CrossRef]
- Storm, F.A.; Petrarca, M.; Beretta, E.; Strazzer, S.; Piccinini, L.; Maghini, C.; Panzeri, D.; Corbetta, C.; Morganti, R.; Reni, G.; et al. Minimum Clinically Important Difference of Gross Motor Function and Gait Endurance in Children with Motor Impairment: A Comparison of Distribution-Based Approaches. Biomed Res. Int. 2020, 2020, 2794036. [Google Scholar] [CrossRef] [PubMed]
- Moreira, M.C.; Michelle, A.; Lima, D.A.; Monica, K.; Aurélio, M.; Rodrigues, B.; Cavalcanti, M.; Michelle, A.; Lima, D.A.; Monica, K.; et al. Use of Virtual Reality in Gait Recovery among Post Stroke Patients—A Systematic Literature Review. Disabil. Rehabil. Assist. Technol. 2013, 8, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Patritti, B.L.; Bonato, P.; Deutsch, J.E. Effects of Virtual Reality Training on Gait Biomechanics of Individuals Post-Stroke. Gait Posture 2010, 31, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, H.T.; Van Limbeek, J.; Geurts, A.C. Motor Recovery After Stroke: A systematic review of the literature. Arch. Phys. Med. Rehabil. 2002, 83, 1629–1637. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Subject ID | S1 | S2 | S3 | S4 | S5 | S6 |
|---|---|---|---|---|---|---|
| Age (years) | 9.8 | 18.3 | 7.8 | 15.9 | 12.8 | 14.3 |
| Sex | m | f | m | m | f | m |
| Impaired side | left | right | right | left | left | right |
| Time from injury (months) | 34 | 63 | 11 | 17 | 74 | 1 |
| Etiology | Resective Surgery for epilepsy | Stroke | Stroke | Traumatic brain injury | Brain tumor | Brain tumor |
| S1 | S2 | S3 | S4 | S5 | S6 | |
|---|---|---|---|---|---|---|
| 6MWT (m) | 525 | 490.2 | 442.2 | 557.4 | 405.4 | 221.5 |
| 6MWT %§ | −21% | −26% | −24% | −20% | −38% | −68% |
| GMFM% Dim D | 95 | 85 | 92 | 100 | 95 | 77 |
| GMFM% Dim E | 96 | 79 | 86 | 99 | 93 | 49 |
| GMFM-88% | 97 | 86 | 95 | 100 | 98 | 78 |
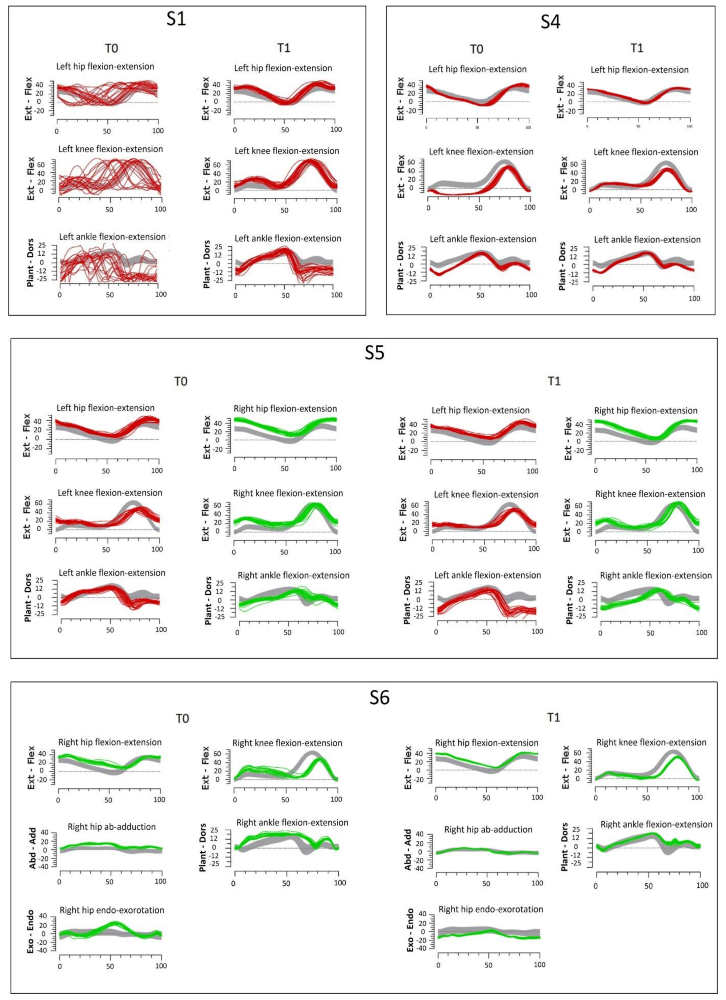
| Gait analysis | see Figure 3 | |||||
| Rehabilitation needs | GP | GMF | GP * | GP | WE, GP | WE, GP, GMF |
| S1 | S2 | S3 | S4 | S5 | S6 | |
|---|---|---|---|---|---|---|
| Walking resistance and spatiotemporal characteristics (WE) | 17 | 24 | 14 | 18 | 22 | 24 |
| Body weight transfer, dynamic balance, single-limb support (GMF) | 32 | 49 | 65 | 27 | 38 | 57 |
| Selective motor control and kinematics (GP) | 52 | 28 | 21 | 55 | 40 | 19 |
| S1 | S2 | S3 | S4 | S5 | S6 | |
|---|---|---|---|---|---|---|
| 6MWT (m) | −22.6 | 41.1 | −34 | −67.2 | 49.2 | 151.5 |
| GMFM% Dim D | 2 | 7 | 5 | 0 | 0 | 10 |
| GMFM% Dim E | 4 | 10 | 2 | 0 | 1 | 30 |
| GMFM-88 % | 2 | 6 | 2 | 0 | 0 | 14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panzeri, D.; Genova, C.; Poggi, G.; Strazzer, S.; Biffi, E. Visual Feedback and Virtual Reality in Gait Rehabilitation of Hemiparetic Children and Teenagers after Acquired Brain Injury: A Pilot Study. Children 2022, 9, 1760. https://doi.org/10.3390/children9111760
Panzeri D, Genova C, Poggi G, Strazzer S, Biffi E. Visual Feedback and Virtual Reality in Gait Rehabilitation of Hemiparetic Children and Teenagers after Acquired Brain Injury: A Pilot Study. Children. 2022; 9(11):1760. https://doi.org/10.3390/children9111760
Chicago/Turabian StylePanzeri, Daniele, Chiara Genova, Geraldina Poggi, Sandra Strazzer, and Emilia Biffi. 2022. "Visual Feedback and Virtual Reality in Gait Rehabilitation of Hemiparetic Children and Teenagers after Acquired Brain Injury: A Pilot Study" Children 9, no. 11: 1760. https://doi.org/10.3390/children9111760
APA StylePanzeri, D., Genova, C., Poggi, G., Strazzer, S., & Biffi, E. (2022). Visual Feedback and Virtual Reality in Gait Rehabilitation of Hemiparetic Children and Teenagers after Acquired Brain Injury: A Pilot Study. Children, 9(11), 1760. https://doi.org/10.3390/children9111760