

Quality Improvement in a Pediatric Echocardiography Laboratory: A Collaborative Process

Abstract
:1. Introduction
2. Materials and Methods
2.1. Diagnostic Error Identification and Classification
2.2. QI Methodology
3. Results
3.1. Baseline State
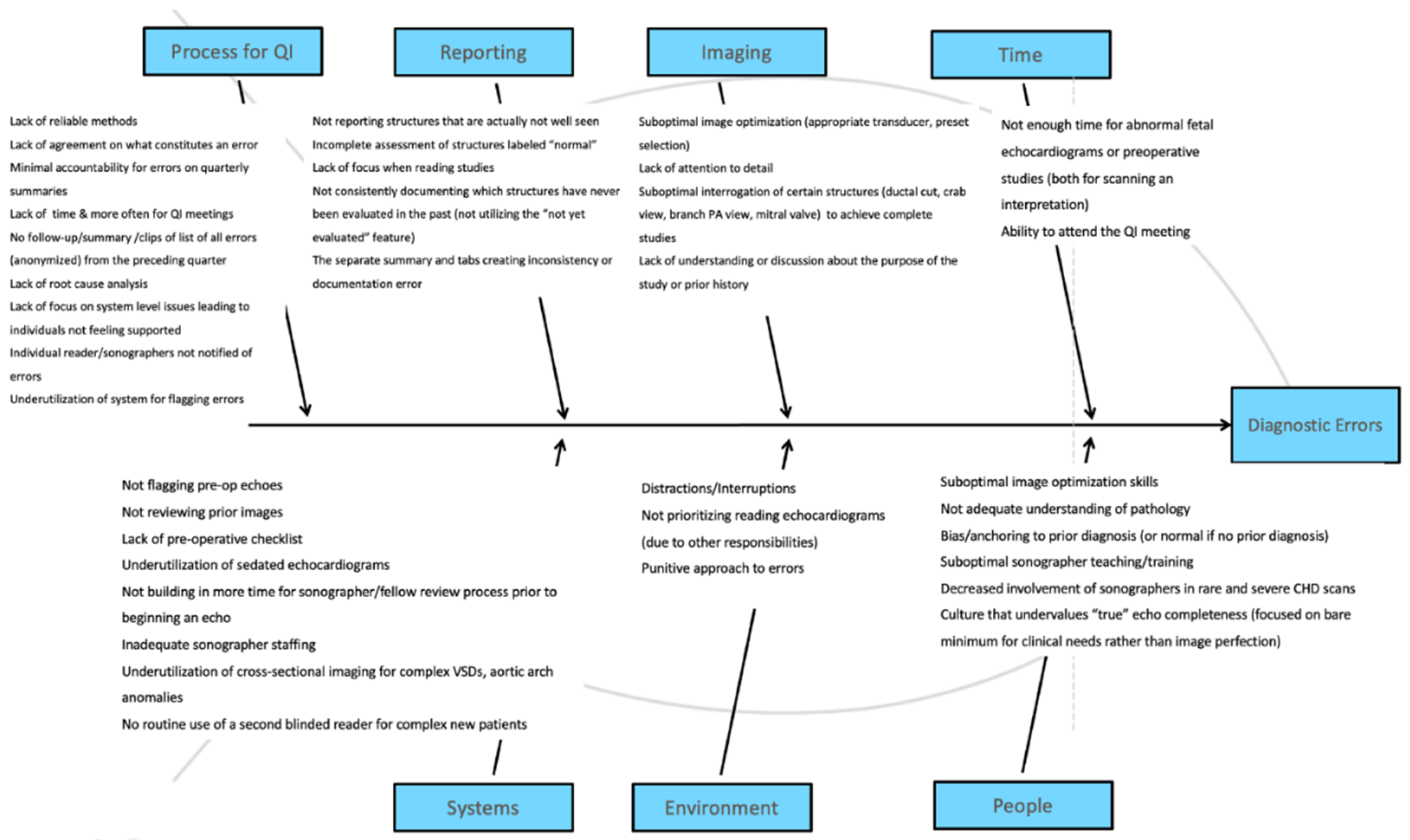
3.2. Root Cause Analysis
3.3. Intervention Design and Implementation
3.4. Follow Up Evaluation
4. Discussion
4.1. Discussion
4.2. Future Directions
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- IAC. IAC Standards & Guidelines for Pediatric Echocardiography Accreditation; Intersocietal Accreditation Commission: Ellicott City, MD, USA, 2017. [Google Scholar]
- American Society of Echocardiography Recommendations for Quality Echocardiography Laboratory Operations. Available online: https://www.asecho.org/document/760#page=1 (accessed on 2 June 2022).
- Benavidez, O.J.; Kavanaugh-McHugh, A.; Kovalchin, J.; Spevak, P.; Lopez, L.; Jone, P.-N. Echocardiography Diagnostic Accuracy. In ACPC Quality Metrics; American College of Cardiology: Washington, DC, USA, 2018. [Google Scholar]
- Benavidez, O.J.; Gauvreau, K.; Jenkins, K.J.; Geva, T. Diagnostic Errors in Pediatric Echocardiography: Development of Taxonomy and Identification of Risk Factors. Circulation 2008, 117, 2995–3001. [Google Scholar] [CrossRef]
- Recommendations for Quantification Methods During the Performance of a Pediatric Echocardiogram: A Report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. Available online: https://www.asecho.org/guideline/recommendations-for-quantification-methods-during-the-performance-of-a-pediatric-echocardiogram/ (accessed on 6 June 2022).
- Guidelines and Standards for the Performance of a Pediatric Echocardiogram: A Report from the Task Force of the Pediatric Council of the American Society of Echocardiography. Available online: https://www.asecho.org/guideline/guidelines-and-standards-for-the-performance-of-a-pediatric-echocardiogram/ (accessed on 6 June 2022).
- Impact of Accreditation on Quality in Echocardiograms: A Quantitative Approach—ClinicalKey. Available online: https://www-clinicalkey-com.laneproxy.stanford.edu/#!/content/playContent/1-s2.0-S0894731717304492?returnurl=null&referrer=null (accessed on 6 June 2022).
- White, B.R.; Ho, D.Y.; Rogers, L.S.; Natarajan, S.S. A Standardized Imaging Protocol Improves Quality and Reduces Practice Variability in Echocardiographic Assessment of Ventricular Function by First-Year Pediatric Cardiology Fellows. Echocardiography 2019, 36, 1515–1523. [Google Scholar] [CrossRef] [PubMed]
- Srnka, C.M.; Strohacker, C.M.; Balasubramanian, S.; Yu, S.; Lowery, R.; Lu, J.C. Improving Adherence to Echocardiogram Reporting Guidelines in Patients with Repaired Tetralogy of Fallot: A Quality Improvement Initiative. Echocardiography 2021, 38, 596–603. [Google Scholar] [CrossRef]
- Johnson, J.T.; Robinson, J.D.; Young, L.T.; Camarda, J.A. The Effect of Image Review before Patient Discharge on Study Completeness and Sonographer Job Satisfaction in a Pediatric Echocardiographic Laboratory. J. Am. Soc. Echocardiogr. 2016, 29, 1000–1005. [Google Scholar] [CrossRef]
- ACC/AAP/AHA/ASE/HRS/SCAI/SCCT/SCMR/SOPE 2014 Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology—ClinicalKey. Available online: https://www-clinicalkey-com.laneproxy.stanford.edu/#!/content/playContent/1-s2.0-S0894731714007445?returnurl=null&referrer=null (accessed on 6 June 2022).
- Improvement in Appropriateness of Pediatric Outpatient Echocardiography Orders Following Integration of the Appropriate Use Criteria within the Electronic Medical Record Ordering System—ClinicalKey. Available online: https://www-clinicalkey-com.laneproxy.stanford.edu/#!/content/playContent/1-s2.0-S0894731720303102?returnurl=null&referrer=null (accessed on 6 June 2022).
- Renno, M.S.; Lambert, A.N.; Kannankeril, P.; Johnson, D.P.; Parra, D.A. Impact of Clinician Engagement on Implementation of the Pediatric Echocardiography Appropriate Use Criteria. Pediatr. Cardiol. 2020, 41, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Frandsen, E.L.; Kourtidou, S.; Tieder, J.S.; Alberda, E.; Soriano, B.D. A Quality Initiative to Improve Appropriate Use of Initial Outpatient Echocardiography Among Pediatric Cardiologists. Pediatr. Qual. Saf. 2020, 5, e313. [Google Scholar] [CrossRef] [PubMed]
- Stern, K.W.D.; McCracken, C.E.; Gillespie, S.E.; Lang, S.M.; Statile, C.J.; Lopez, L.; Verghese, G.R.; Choueiter, N.F.; Sachdeva, R. Physician Variation in Ordering of Transthoracic Echocardiography in Outpatient Pediatric Cardiac Clinics. Echocardiography 2020, 37, 1056–1064. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Error | Anatomic Structure Involved | Type | Severity | Preventable |
|---|---|---|---|---|
| 1 | Ventricular septum | Discrepant diagnosis | Moderate | Preventable |
| 2 | Ventricular septum | False negative | Minor | Not preventable |
| 3 | Ventricular septum | Discrepant diagnosis | Moderate | Preventable |
| 4 | Atrial septum | Discrepant diagnosis | Minor | Preventable |
| 5 | Atrial septum | False negative | Minor | Preventable |
| 6 | Outflow tract | False negative | Severe | Preventable |
| 7 | Patent ductus arteriosus | Discrepant diagnosis | Minor | Preventable |
| 8 | Pulmonary arteries | False negative | Minor | Preventable |
| 9 | Atrial septum | False negative | Minor | Not preventable |
| 10 | Ventricular septum | False negative | Severe | Possibly preventable |
| 11 | Patent ductus arteriosus | False negative | Minor | Preventable |
| 12 | Mitral valve | Discrepant diagnosis | Minor | Not preventable |
| 13 | Atrial septum | False negative | Minor | Not preventable |
| 14 | Ventricular septum | Discrepant diagnosis | Minor | Preventable |
| 15 | Ventricular septum | False negative | Minor | Not preventable |
| 16 | Atrial septum | False negative | Minor | Preventable |
| 17 | Ventricles | Discrepant diagnosis | Minor | Preventable |
| 18 | Aortic arch | Discrepant diagnosis | Minor | Preventable |
| Error | Anatomic Structure | Type | Severity | Preventable |
|---|---|---|---|---|
| 1 | Aortic arch | False negative | Minor | Preventable |
| 2 | Atrial septum | False negative | Minor | Preventable |
| 3 | Aortic arch | False negative | Minor | Possibly preventable |
| 4 | Inferior vena cava | False negative | Minor | Preventable |
| 5 | Atrial septum | False negative | Minor | Possibly preventable |
| 6 | Ventricular septum | Discrepant diagnosis | Minor | Preventable |
| 7 | Coronary arteries | Discrepant diagnosis | Minor | Possibly Preventable |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sganga, D.; Behera, S.; Beattie, M.J.; Stauffer, K.J.; Burlinson, A.; Lopez, L.; Tierney, E.S.S. Quality Improvement in a Pediatric Echocardiography Laboratory: A Collaborative Process. Children 2022, 9, 1845. https://doi.org/10.3390/children9121845
Sganga D, Behera S, Beattie MJ, Stauffer KJ, Burlinson A, Lopez L, Tierney ESS. Quality Improvement in a Pediatric Echocardiography Laboratory: A Collaborative Process. Children. 2022; 9(12):1845. https://doi.org/10.3390/children9121845
Chicago/Turabian StyleSganga, Danielle, Sarina Behera, Meaghan J. Beattie, Katie Jo Stauffer, Aubrey Burlinson, Leo Lopez, and Elif Seda Selamet Tierney. 2022. "Quality Improvement in a Pediatric Echocardiography Laboratory: A Collaborative Process" Children 9, no. 12: 1845. https://doi.org/10.3390/children9121845
APA StyleSganga, D., Behera, S., Beattie, M. J., Stauffer, K. J., Burlinson, A., Lopez, L., & Tierney, E. S. S. (2022). Quality Improvement in a Pediatric Echocardiography Laboratory: A Collaborative Process. Children, 9(12), 1845. https://doi.org/10.3390/children9121845