
Musculoskeletal and Gait Characteristics in Patients with Stickler Syndrome: A Cross-Sectional Study

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Musculoskeletal Characteristics, Muscular Strength, and Functional Tests
2.2. Calcaneus Quantitative Ultrasound (QUS)
2.3. Gait and Walking Test
2.4. Statistical Analysis
3. Results
3.1. Musculoskeletal Characteristics and Physical Examination
3.2. Calcaneus Quantitative Ultrasound, QUS
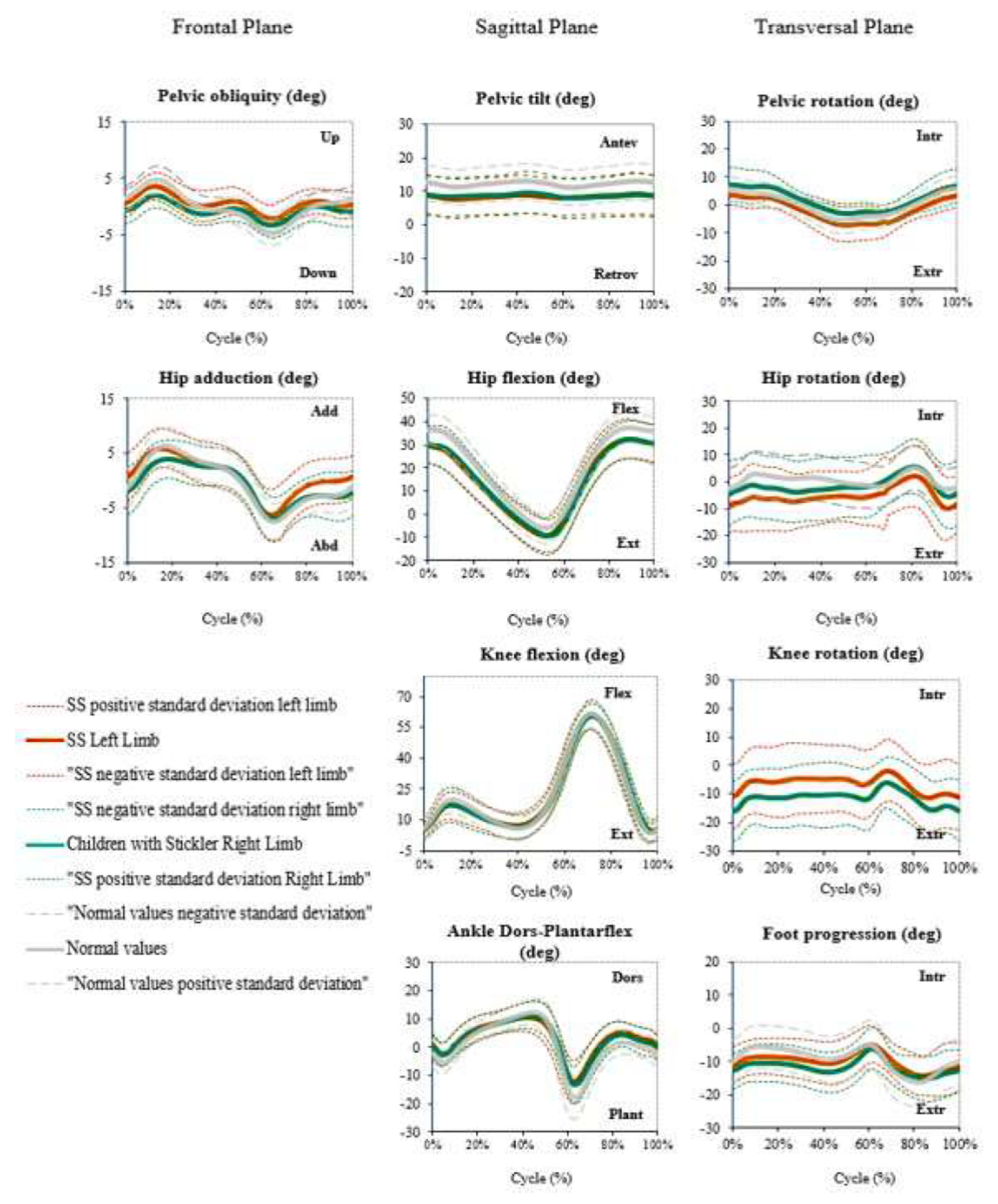
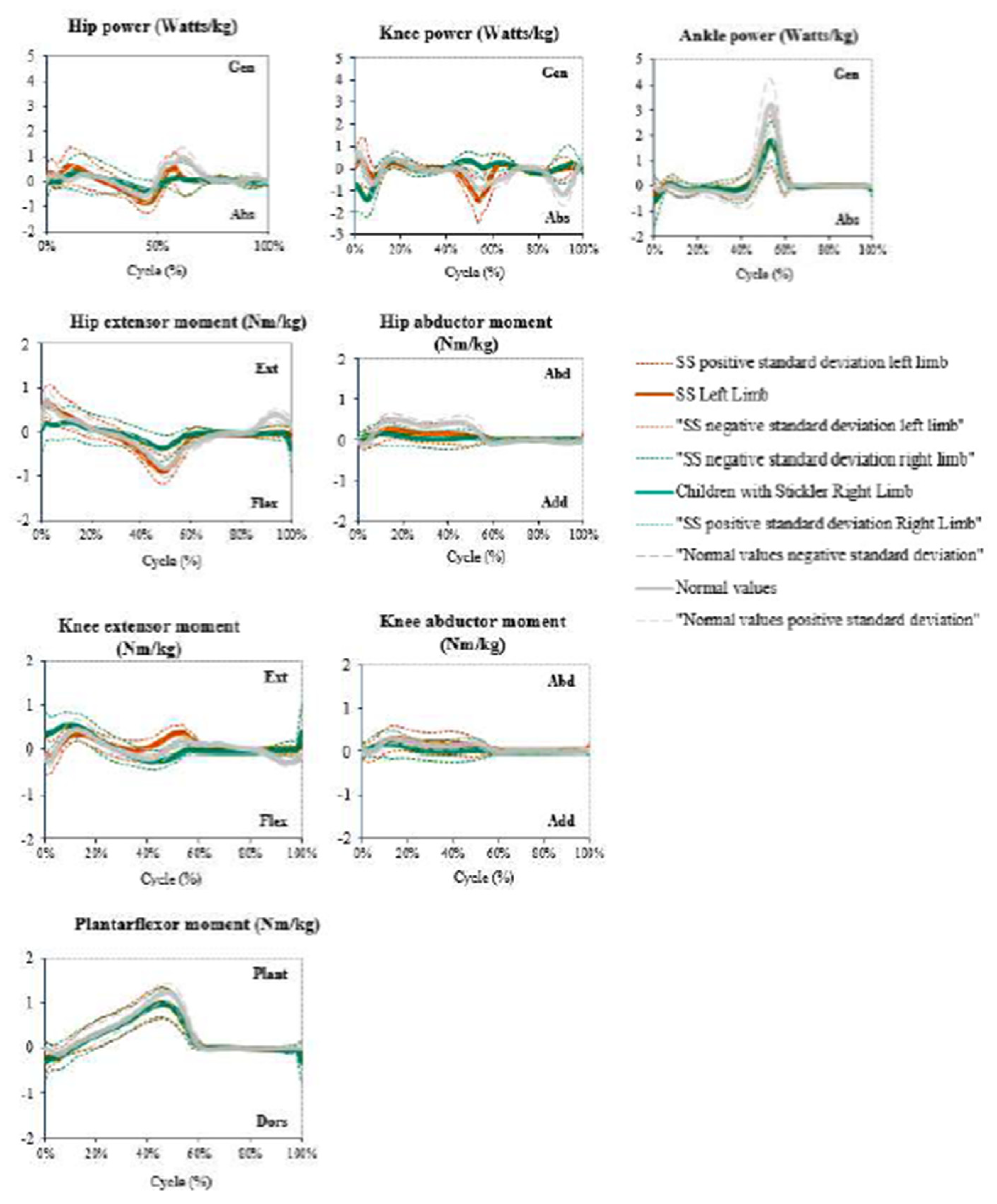
3.3. Gait Analysis (3D Gait Analysis and 6MWT)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stickler, G.B.; Belau, P.G.; Farrell, F.J.; Jones, J.D.; Pugh, D.G.; Steinberg, A.G.; Ward, L.E. Hereditary Progressive Arthro-Ophtalmopathy. Mayo Clin. Proc. 1965, 40, 433–455. [Google Scholar] [PubMed]
- Acke, F.R.E.; Dhooge, I.J.M.; Malfait, F.; De Leenheer, E.M.R. Hearing Impairment in Stickler Syndrome: A Systematic Review. Orphanet J. Rare Dis. 2012, 7, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snead, M.P.; McNinch, A.M.; Poulson, A.V.; Bearcroft, P.; Silverman, B.; Gomersall, P.; Parfect, V.; Richards, A.J. Stickler Syndrome, Ocular-Only Variants and a Key Diagnostic Role for the Ophthalmologist. Eye 2011, 25, 1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matute, G.R.; Alonso, E.R. Síndrome de Stickler. Semin. Fund. Esp. Reumatol. 2009, 10, 83–86. [Google Scholar] [CrossRef]
- Richards, A.J.; Baguley, D.M.; Yates, J.R.W.; Lane, C.; Nicol, M.; Harper, P.S.; Scott, J.D.; Snead, M.P. Variation in the Vitreous Phenotype of Stickler Syndrome Can Be Caused by Different Amino Acid Substitutions in the X Position of the Type II Collagen Gly-X-Y Triple Helix. Am. J. Hum. Genet. 2000, 67, 1083–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaschke, U.K.; Eikenberry, E.F.; Hulmes, D.J.S.; Galla, H.-J.; Bruckner, P. Collagen XI Nucleates Self-Assembly and Limits Lateral Growth of Cartilage Fibrils. J. Biol. Chem. 2000, 275, 10370–10378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, A.J.; McNinch, A.; Martin, H.; Oakhill, K.; Rai, H.; Waller, S.; Treacy, B.; Whittaker, J.; Meredith, S.; Poulson, A.; et al. Stickler Syndrome and the Vitreous Phenotype: Mutations in COL2A1 and COL11A1. Hum. Mutat. 2010, 31, E1461–E1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, P.S.; Levy, H.P.; Liberfarb, R.M.; Davis, J.; Szymko-Bennett, Y.; Rubin, B.I.; Tsilou, E.; Griffith, A.J.; Francomano, C.A. Stickler Syndrome: Clinical Characteristics and Diagnostic Criteria. Am. J. Med. Genet. A 2005, 138A, 199–207. [Google Scholar] [CrossRef]
- Webb, A.C.; Markus, A.F. The Diagnosis and Consequences of Stickler Syndrome. Br. J. Oral Maxillofac. Surg. 2002, 40, 49–51. [Google Scholar] [CrossRef] [PubMed]
- Letts, M.; Kabir, A.; Davidson, D. The Spinal Manifestations of Stickler’s Syndrome. Spine 1999, 24, 1260–1264. [Google Scholar] [CrossRef] [PubMed]
- Rose, P.S.; Ahn, N.U.; Levy, H.P.; Ahn, U.M.; Davis, J.; Liberfarb, R.M.; Nallamshetty, L.; Sponseller, P.D.; Francomano, C.A. Thoracolumbar Spinal Abnormalities in Stickler Syndrome. Spine 2001, 26, 403–409. [Google Scholar] [CrossRef]
- Richards, A.J.; Snead, M.P. The Influence of Pre-MRNA Splicing on Phenotypic Modification in Stickler’s Syndrome and Other Type II Collagenopathies. Eye 2008, 22, 1243–1250. [Google Scholar] [CrossRef] [Green Version]
- Rider, L.G.; Koziol, D.; Giannini, E.H.; Jain, M.S.; Smith, M.R.; Whitney-Mahoney, K.; Feldman, B.M.; Wright, S.J.; Lindsley, C.B.; Pachman, L.M.; et al. Validation of Manual Muscle Testing and a Subset of Eight Muscles for Adult and Juvenile Idiopathic Inflammatory Myopathies. Arthritis Care Res. 2010, 62, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Marks, M.C.; Alexander, J.; Sutherland, D.H.; Chambers, H.G. Clinical Utility of the Duncan-Ely Test for Rectus Femoris Dysfunction during the Swing Phase of Gait. Dev. Med. Child Neurol. 2003, 45, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Cooperstein, R.; Haneline, M.; Young, M. Mathematical Modeling of the Socalled Allis Test: A Field Study in Orthopedic Confusion. Chiropr. Osteopat. 2007, 15, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirpiris, M.; Wilkinson, A.J.; Rodda, J.; Nguyen, T.C.; Baker, R.J.; Nattrass, G.R.; Graham, H.K. Walking Speed in Children and Young Adults with Neuromuscular Disease: Comparison between Two Assessment Methods. J. Pediatr. Orthop 2003, 23, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Singh, D. Nils Silfverskiöld (1888–1957) and Gastrocnemius Contracture. Foot Ankle Surg. 2013, 19, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Baroncelli, G.I. Quantitative Ultrasound Methods to Assess Bone Mineral Status in Children: Technical Characteristics, Performance, and Clinical Application. Pediatr. Res. 2008, 63, 220–228. [Google Scholar] [CrossRef]
- Trimpou, P.; Bosaeus, I.; Bengtsson, B.Å.; Landin-Wilhelmsen, K. High Correlation between Quantitative Ultrasound and DXA during 7 Years of Follow-Up. Eur. J. Radiol. 2010, 73, 360–364. [Google Scholar] [CrossRef]
- Chin, K.-Y.; Ima-Nirwana, S. Calcaneal Quantitative Ultrasound as a Determinant of Bone Health Status: What Properties of Bone Does It Reflect? Int. J. Med. Sci. 2013, 10, 1778–1783. [Google Scholar] [CrossRef]
- Xu, Y.; Guo, B.; Gong, J.; Xu, H.; Bai, Z. The Correlation between Calcaneus Stiffness Index Calculated by QUS and Total Body BMD Assessed by DXA in Chinese Children and Adolescents. J. Bone Miner. Metab. 2014, 32, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of Lower Extremity Kinematics during Level Walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef]
- Baker, R.; McGinley, J.L.; Schwartz, M.H.; Beynon, S.; Rozumalski, A.; Graham, H.K.; Tirosh, O. The Gait Profile Score and Movement Analysis Profile. Gait Posture 2009, 30, 265–269. [Google Scholar] [CrossRef]
- Baker, R.; McGinley, J.L.; Schwartz, M.; Thomason, P.; Rodda, J.; Graham, H.K. The Minimal Clinically Important Difference for the Gait Profile Score. Gait Posture 2012, 35, 612–615. [Google Scholar] [CrossRef]
- Molloy, M.; McDowell, B.C.; Kerr, C.; Cosgrove, A.P. Further Evidence of Validity of the Gait Deviation Index. Gait Posture 2010, 31, 479–482. [Google Scholar] [CrossRef]
- Cheng, L.; Pohlabeln, H.; Ahrens, W.; Russo, P.; Veidebaum, T.; Hadjigeorgiou, C.; Molnár, D.; Hunsberger, M.; De Henauw, S.; Moreno, L.A.; et al. Cross-Sectional and Longitudinal Associations between Sleep Duration, Sleep Quality, and Bone Stiffness in European Children and Adolescents. Osteoporos. Int. 2021, 32, 853–863. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Pohlabeln, H.; Ahrens, W.; Russo, P.; Veidebaum, T.; Chadjigeorgiou, C.; Molnár, D.; Eiben, G.; De Henauw, S.; Moreno, L.; et al. Sex Differences in the Longitudinal Associations between Body Composition and Bone Stiffness Index in European Children and Adolescents. Bone 2020, 131, 115162. [Google Scholar] [CrossRef]
- de Lamas, C.; Sánchez-Pintos, P.; José de Castro, M.; Sáenz de Pipaon, M.; Couce, M.L. Screen Time and Bone Status in Children and Adolescents: A Systematic Review. Front. Pediatr. 2021, 9, 675214. [Google Scholar] [CrossRef] [PubMed]
- Burnham, J.M.; Shults, J.; Dubner, S.E.; Sembhi, H.; Zemel, B.S.; Leonard, M.B. Bone Density, Structure, and Strength in Juvenile Idiopathic Arthritis: Importance of Disease Severity and Muscle Deficits. Arthritis Rheum. 2008, 58, 2518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arshad, F.; Bishop, N. Osteogenesis Imperfecta in Children. Bone 2021, 148, 115914. [Google Scholar] [CrossRef]
- Burnham, J.M.; Shults, J.; Weinstein, R.; Lewis, J.D.; Leonard, M.B. Childhood Onset Arthritis Is Associated with an Increased Risk of Fracture: A Population Based Study Using the General Practice Research Database. Ann. Rheum. Dis. 2006, 65, 1074. [Google Scholar] [CrossRef] [PubMed]
- Clark, E.M.; Tobias, J.H.; Ness, A.R. Association Between Bone Density and Fractures in Children: A Systematic Review and Meta-Analysis. Pediatrics 2006, 117, e291. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.W.P.; Shorter, K.A.; Adamczyk, P.G.; Kuo, A.D. Mechanical and Energetic Consequences of Reduced Ankle Plantar-Flexion in Human Walking. J. Exp. Biol. 2015, 218, 3541–3550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, D.; Tomazos, I.C.; Moseley, S.; L’Italien, G.; Gomes da Silva, H.; Lerma Lara, S. Reliability and Validity of the 6-Minute Walk Test in Hypophosphatasia. JBMR Plus 2019, 3, e10131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mian, Q.; Rumsey, D.G.; Verschuren, O.; Moez, E.K.; Roy, M.; Kaup, C.; Pritchard, L. Reference Values for the Six Minute Walk Test in Children with Juvenile Idiopathic Arthritis. Phys. Occup. Ther. Pediatr. 2022, 42, 187–197. [Google Scholar] [CrossRef]
- Machol, K.; Hadley, T.D.; Schmidt, J.; Cuthbertson, D.; Traboulsi, H.; Silva, R.C.; Citron, C.; Khan, S.; Citron, K.; Carter, E.; et al. Mobility in Osteogenesis Imperfecta: A Multicenter North American Study. Am. J. Med. Genet. A 2020, 182, 697. [Google Scholar] [CrossRef]
- Ong, C.F.; Geijtenbeek, T.; Hicks, J.L.; Delp, S.L. Predicting Gait Adaptations Due to Ankle Plantarflexor Muscle Weakness and Contracture Using Physics-Based Musculoskeletal Simulations. PLoS Comput. Biol. 2019, 15, e1006993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Núñez, I.; Mondaca, F.; Casas, B.; Ferreira, C.; Zenteno, D. Normal Values of 6-Minute Walk Test in Healthy Children and Adolescents: A Systematic Review and Meta-Analysis. Rev. Chil. Pediatr. 2018, 89, 128–136. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Musculoskeletal SS’s Features (n = 23) | |||
|---|---|---|---|
| Variables | n | Value n (%) | 95% confidence interval |
| Osteoarthritis | 23 | 4 (17) | 0.6 to 34.1 |
| Ligament hyperlaxity syndrome | 23 | 7 (30) | 10.1 to 50.7 |
| Marfanoid habit | 23 | 4 (17) | 0.6 to 34.1 |
| Spinal dysplasia | 23 | 2 (9) | −3.8 to 21.1 |
| Muscular atrophy | 23 | 4 (17) | 0.6 to 34.1 |
| Functional Tests (n = 25) | |||
| Variables | n | Value (%) | |
| Duncan–Ely test | 25 | 3 (12) | |
| Galeazzi or Allis test | 25 | 2 (8) | |
| Thomas test | 25 | 4 (16) | |
| Silfverskiold test | 25 | 1 (4) | |
| Alteration in any test | 25 | 7 (28) | |
| Bone and Gait Characteristics | |||
|---|---|---|---|
| Outcomes | Sample (n) | 95% CI | Difference |
| Calcaneus SI | Total (26) | 71.8 to 87.4 | - |
| Male (9) | 61.7 to 85.1 | −24.9 to 5.9 | |
| Female (17) | 72.8 to 93.0 | ||
| Under 10 years (13) | 60.2 to 81.6 | −31.7 to −3.1 * | |
| Over 10 years (13) | 78.8 to 97.8 | ||
| 6MWT distance (m) | Total (22) | 512.7 to 607.5 | - |
| Male (7) | 445.7 to 646.7 | −134.3 to 93.7 | |
| Female (15) | 512.8 to 620.2 | ||
| Under 10 years (11) | 453.1 to 571.4 | −183.329 to −8.071 * | |
| Over 10 years (11) | 543.3 to 672.6 | ||
| GPS | Left side (26) | 6.7 to 8.1 | - |
| Right side (26) | 6.0 to 7.6 | ||
| GDI | Left side (26) | 91.6 to 99.0 | - |
| Right side (26) | 94.0 to 101.4 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Pérez, J.J.; Mascaraque-Ruiz, P.; Martín-Gómez, C.; Martínez-Caballero, I.; Otón, T.; Carmona, L.; Lerma-Lara, S. Musculoskeletal and Gait Characteristics in Patients with Stickler Syndrome: A Cross-Sectional Study. Children 2022, 9, 1895. https://doi.org/10.3390/children9121895
Fernández-Pérez JJ, Mascaraque-Ruiz P, Martín-Gómez C, Martínez-Caballero I, Otón T, Carmona L, Lerma-Lara S. Musculoskeletal and Gait Characteristics in Patients with Stickler Syndrome: A Cross-Sectional Study. Children. 2022; 9(12):1895. https://doi.org/10.3390/children9121895
Chicago/Turabian StyleFernández-Pérez, Juan José, Paloma Mascaraque-Ruiz, Carlos Martín-Gómez, Ignacio Martínez-Caballero, Teresa Otón, Loreto Carmona, and Sergio Lerma-Lara. 2022. "Musculoskeletal and Gait Characteristics in Patients with Stickler Syndrome: A Cross-Sectional Study" Children 9, no. 12: 1895. https://doi.org/10.3390/children9121895
APA StyleFernández-Pérez, J. J., Mascaraque-Ruiz, P., Martín-Gómez, C., Martínez-Caballero, I., Otón, T., Carmona, L., & Lerma-Lara, S. (2022). Musculoskeletal and Gait Characteristics in Patients with Stickler Syndrome: A Cross-Sectional Study. Children, 9(12), 1895. https://doi.org/10.3390/children9121895