
Long-Term Varicella Zoster Virus Immunity in Paediatric Liver Transplant Patients Can Be Achieved by Booster Vaccinations—A Single-Centre, Retrospective, Observational Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Acquisition
2.2. Statistical Analysis
3. Results
3.1. Study Population
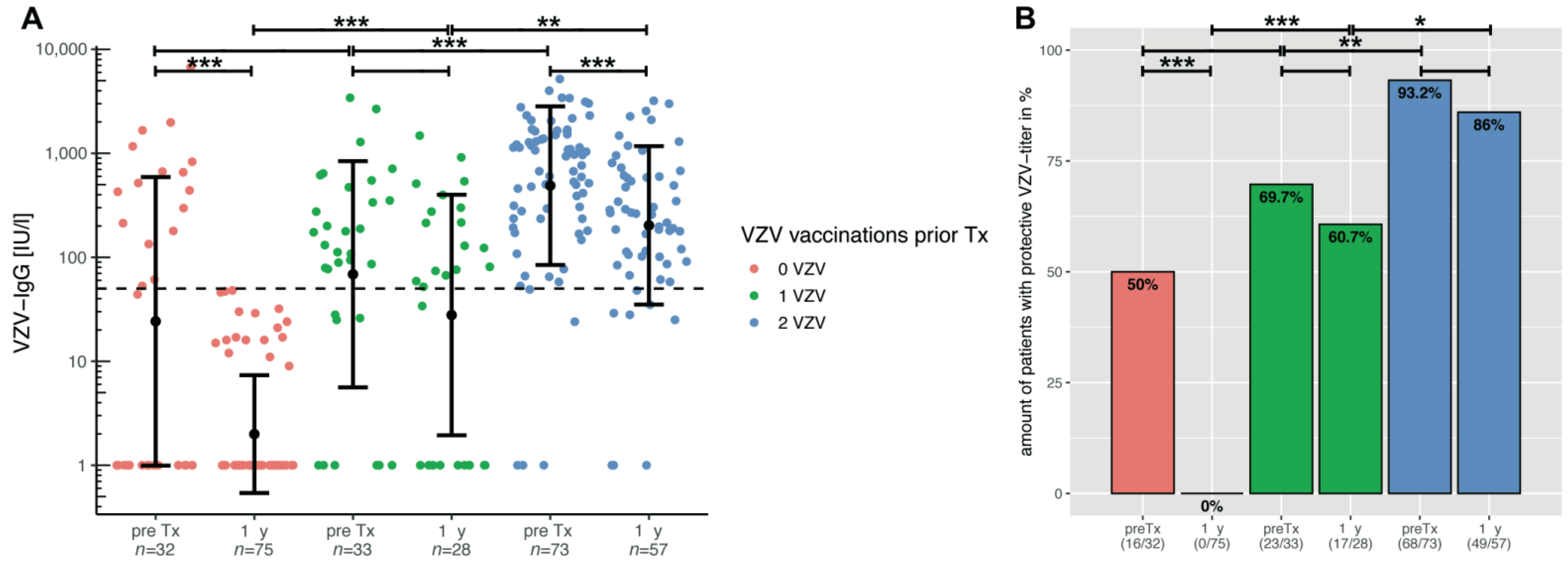
3.2. VZV Immunity in the First Year after Pediatric Liver Transplantion
3.3. VZV Immunization of VZV-Naïve Children after Transplantation and Titre
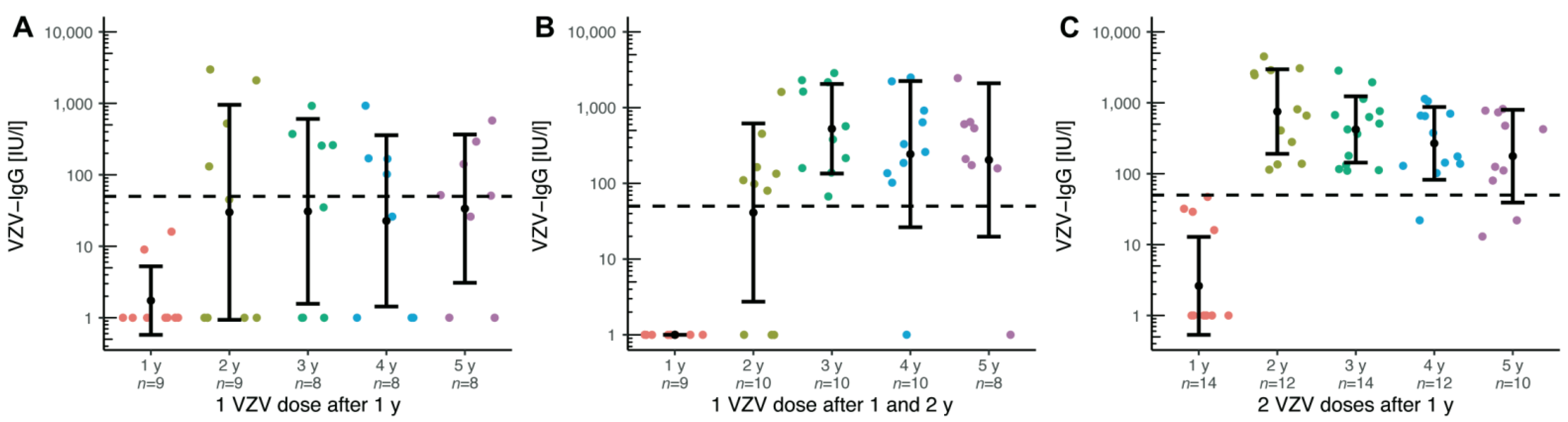
3.4. Response to Booster Vaccinations in Pre-Transplant Vaccinated Patients without Protective Titres at the First Annual Check-Up
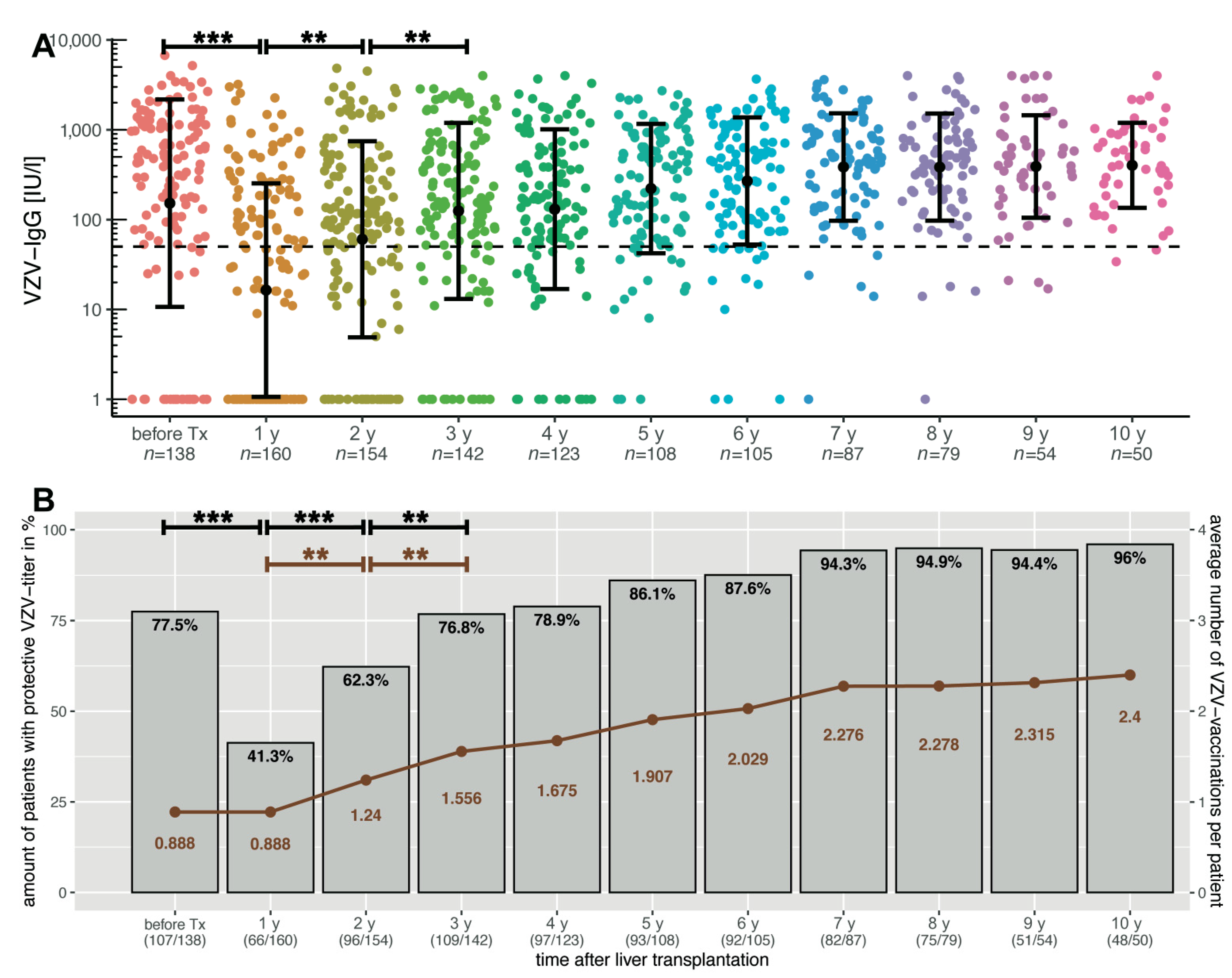
3.5. Long-Term Observation of VZV-Specific Titres and Immunity over 10 Years with Vaccination Course
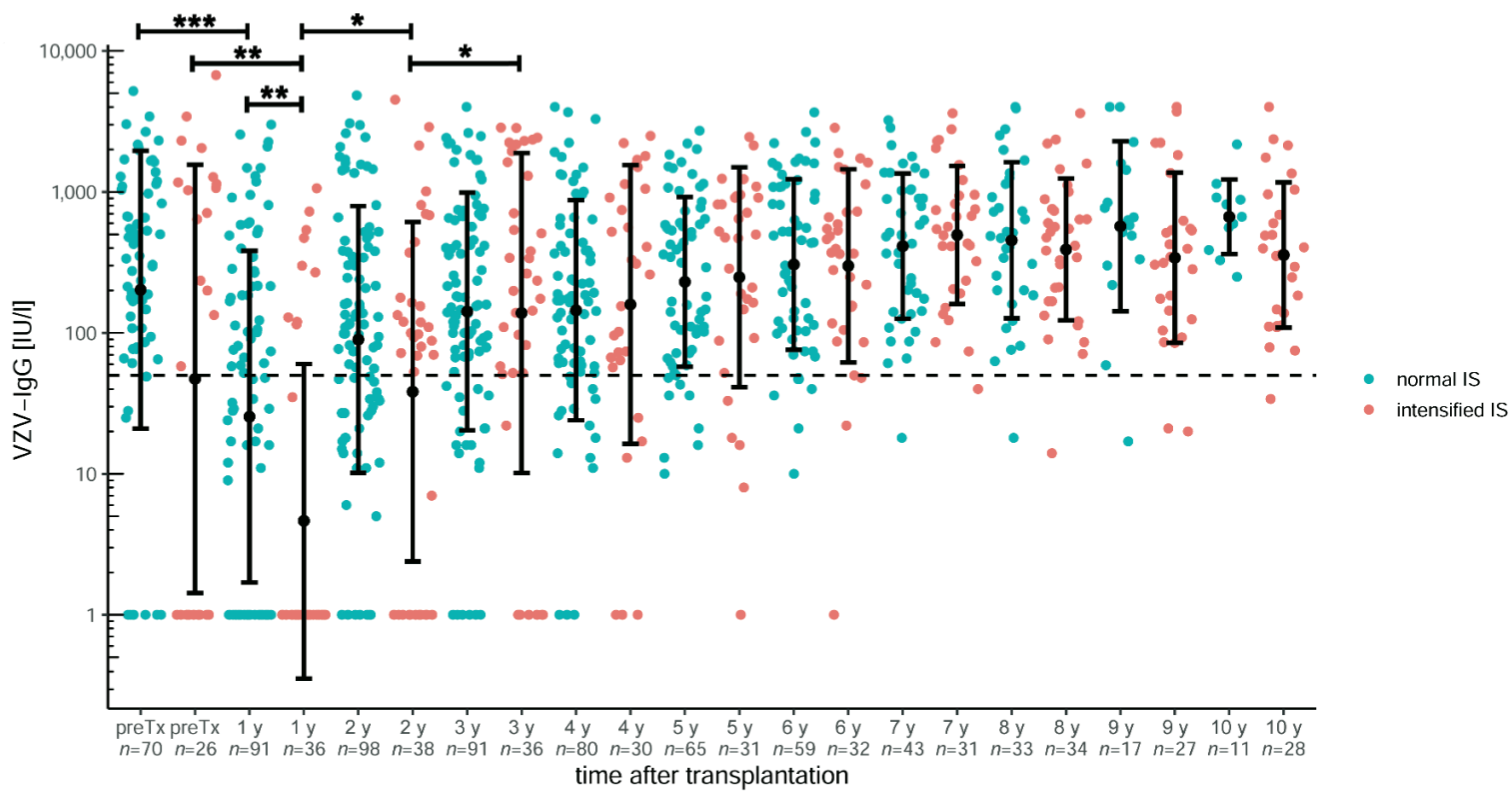
3.6. Influence of Immunosuppression on VZV Titres
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wallot, M.A.; Mathot, M.; Janssen, M.; Hölter, T.; Paul, K.; Buts, J.P.; Reding, R.; Otte, J.B.; Sokal, E.M. Long-term survival and late graft loss in pediatric liver transplant recipients—A 15-year single-center experience. Liver Transpl. 2002, 8, 615–622. [Google Scholar] [CrossRef]
- Leiskau, C.; Junge, N.; Pfister, E.; Goldschmidt, I.; Mutschler, F.; Laue, T.; Ohlendorf, J.; Nasser, H.; Beneke, J.; Richter, N.; et al. Recipient-Specific Risk Factors Impairing Patient and Graft Outcome after Pediatric Liver Transplantation—Analysis of 858 Transplantations in 38 Years. Children 2021, 8, 641. [Google Scholar] [CrossRef] [PubMed]
- Farmer, D.G.; Venick, R.S.; McDiarmid, S.V.; Ghobrial, R.M.; Gordon, S.A.; Yersiz, H.; Hong, J.; Candell, L.; Cholakians, A.; Wozniak, L.; et al. Predictors of outcomes after pediatric liver transplantation: An analysis of more than 800 cases performed at a single institution. J. Am. Coll. Surg. 2007, 204, 904–914. [Google Scholar] [CrossRef] [PubMed]
- Feldman, A.G.; Beaty, B.L.; Curtis, D.; Juarez-Colunga, E.; Kempe, A. Incidence of Hospitalization for Vaccine-Preventable Infections in Children Following Solid Organ Transplant and Associated Morbidity, Mortality, and Costs. JAMA Pediatr. 2019, 173, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Heininger, U.; Seward, J.F. Varicella. Lancet 2006, 368, 1365–1376. [Google Scholar] [CrossRef]
- Morgan, E.R.; Smalley, L.A. Varicella in immunocompromised children. Incidence of abdominal pain and organ involvement. Am. J. Dis. Child. 1983, 137, 883–885. [Google Scholar] [CrossRef]
- Pacini-Edelstein, S.J.; Mehra, M.; Ament, M.E.; Vargas, J.H.; Martin, M.G.; McDiarmid, S.V. Varicella in pediatric liver transplant patients: A retrospective analysis of treatment and outcome. J. Pediatr. Gastroenterol. Nutr. 2003, 37, 183–186. [Google Scholar] [CrossRef]
- Levitsky, J.; Kalil, A.C.; Meza, J.L.; Hurst, G.E.; Freifeld, A. Chicken pox after pediatric liver transplantation. Liver Transpl. 2005, 11, 1563–1566. [Google Scholar] [CrossRef]
- Yamada, N.; Sanada, Y.; Okada, N.; Wakiya, T.; Ihara, Y.; Urahashi, T.; Mizuta, K. Successful rescue of disseminated varicella infection with multiple organ failure in a pediatric living donor liver transplant recipient: A case report and literature review. Virol. J. 2015, 12, 91. [Google Scholar] [CrossRef] [Green Version]
- McGregor, R.S.; Zitelli, B.J.; Urbach, A.H.; Malatack, J.J.; Gartner, J.C., Jr. Varicella in pediatric orthotopic liver transplant recipients. Pediatrics 1989, 83, 256–261. [Google Scholar] [CrossRef]
- Recommended Child and Adolescent Immunization Schedule for Ages 18 Years or Younger, United States. Available online: https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html (accessed on 1 September 2021).
- Koch-Institut, Ständige Impfkommission (STIKO) beim Robert Empfehlungen der Ständigen Impfkommission beim Robert Koch-Institut—2020/2021. 2020, pp. 1–68. Available online: http://dx.doi.org/10.25646/7083.7 (accessed on 9 January 2022).
- Rubin, L.G.; Levin, M.J.; Ljungman, P.; Davies, E.G.; Avery, R.; Tomblyn, M.; Bousvaros, A.; Dhanireddy, S.; Sung, L.; Keyserling, H.; et al. Infectious Diseases Society of America 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin. Infect. Dis. 2014, 58, 309–318. [Google Scholar] [CrossRef]
- Höcker, B.; Aguilar, M.; Schnitzler, P.; Pape, L.; Bald, M.; König, J.; Marks, S.D.; Genc, G.; Büscher, A.; Kemper, M.J.; et al. Vaccination titres pre- and post-transplant in paediatric renal transplant recipients and the impact of immunosuppressive therapy. Pediatr. Nephrol. 2018, 33, 897–910. [Google Scholar] [CrossRef] [PubMed]
- Sommer, W.; Ius, F.; Müller, C.; Bobylev, D.; Kuehn, C.; Avsar, M.; Salman, J.; Siemeni, T.; Miha, O.J.; Horke, A.; et al. Extended criteria donor lungs do not impact recipient outcomes in pediatric transplantation. J. Heart Lung Transplant. 2019, 38, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Elisofon, S.A.; Magee, J.C.; Ng, V.L.; Horslen, S.P.; Fioravanti, V.; Economides, J.; Erinjeri, J.; Anand, R.; Mazariegos, G.V. Society of Pediatric Liver Transplantation Research Group Society of pediatric liver transplantation: Current registry status 2011–2018. Pediatr. Transplant. 2020, 24, e13605. [Google Scholar] [CrossRef] [PubMed]
- Feldman, A.G.; Sundaram, S.S.; Beaty, B.L.; Torres, R.; Curtis, D.J.; Kempe, A. Immunization Status at the Time of Liver Transplant in Children and Adolescents. JAMA 2019, 322, 1822–1824. [Google Scholar] [CrossRef]
- Laue, T.; Demir, Z.; Debray, D.; Cananzi, M.; Gaio, P.; Casotti, V.; D’Antiga, L.; Urbonas, V.; Baumann, U. Under-Vaccination in Pediatric Liver Transplant Candidates with Acute and Chronic Liver Disease—A Retrospective Observational Study of the European Reference Network TransplantChild. Children 2021, 8, 675. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, A.; Liu, K.; Bonnichsen, M.; Joshi, V.; Davis, R.J.; Strasser, S.I. Immunity to Vaccine-preventable Viral Infections in Australians Being Evaluated for Liver Transplantation. Transplantation 2019, 103, 2318–2322. [Google Scholar] [CrossRef]
- Abuali, M.M.; Arnon, R.; Posada, R. An update on immunizations before and after transplantation in the pediatric solid organ transplant recipient. Pediatr. Transplant. 2011, 15, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, A.; Horslen, S.P.; Kaufman, S.S.; Jesser, R.; Devoll-Zabrocki, A.; Fleckten, B.L.; Kochanowicz, S.; Seipel, K.R.; Levin, M.J. Safety and immunogenicity of varicella-zoster virus vaccine in pediatric liver and intestine transplant recipients. Am. J. Transplant. 2006, 6, 565–568. [Google Scholar] [CrossRef]
- Posfay-Barbe, K.M.; Pittet, L.F.; Sottas, C.; Grillet, S.; Wildhaber, B.E.; Rodriguez, M.; Kaiser, L.; Belli, D.C.; McLin, V.A.; Siegrist, C.A. Varicella-zoster immunization in pediatric liver transplant recipients: Safe and immunogenic. Am. J. Transplant. 2012, 12, 2974–2985. [Google Scholar] [CrossRef] [PubMed]
- Leuridan, E.; Hens, N.; Hutse, V.; Aerts, M.; Van Damme, P. Kinetics of maternal antibodies against rubella and varicella in infants. Vaccine 2011, 29, 2222–2226. [Google Scholar] [CrossRef] [Green Version]
- Sauerbrei, A.; Schäfler, A.; Hofmann, J.; Schacke, M.; Gruhn, B.; Wutzler, P. Evaluation of three commercial varicella-zoster virus IgG enzyme-linked immunosorbent assays in comparison to the fluorescent-antibody-to-membrane-antigen test. Clin. Vaccine Immunol. 2012, 19, 1261–1268. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2021. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Donati, M.; Zuckerman, M.; Dhawan, A.; Hadzic, N.; Heaton, N.; North-Lewis, P.; Mieli-Vergani, G. Response to varicella immunization in pediatric liver transplant recipients. Transplantation 2000, 70, 1401–1404. [Google Scholar] [CrossRef] [PubMed]
- Atjayutpokin, T.; Treepongkaruna, S.; Apiwattanakul, N.; Techasaensiri, C.; Lertudomphonwanit, C.; Getsuwan, S.; Boonsathorn, S. Immunogenicity of varicella zoster vaccine in pediatric liver transplantation. Pediatr. Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.F.; Ni, Y.H.; Chen, H.L.; Hsu, H.Y.; Lai, H.S.; Chang, M.H. Humoral immunogenicity to measles, rubella, and varicella-zoster vaccines in biliary atresia children. Vaccine 2009, 27, 2812–2815. [Google Scholar] [CrossRef]
- Wang, J.; Xu, Y.; Chen, Z.; Liang, J.; Lin, Z.; Liang, H.; Xu, Y.; Wu, Q.; Guo, X.; Nie, J.; et al. Liver Immune Profiling Reveals Pathogenesis and Therapeutics for Biliary Atresia. Cell 2020, 183, 1867–1883.e26. [Google Scholar] [CrossRef] [PubMed]
- Kuter, B.; Matthews, H.; Shinefield, H.; Black, S.; Dennehy, P.; Watson, B.; Reisinger, K.; Kim, L.L.; Lupinacci, L.; Hartzel, J.; et al. Study Group for Varivax Ten year follow-up of healthy children who received one or two injections of varicella vaccine. Pediatr. Infect. Dis. J. 2004, 23, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Yoeli, J.K.; Yoeli, D.; Miloh, T.A.; Rana, A.; Goss, J.A.; Munoz-Rivas, F. Measles, mumps, rubella (vaccine) and varicella vaccines in pediatric liver transplant: An initial analysis of post-transplant immunity. Pediatr. Transplant. 2019, 23, e13490. [Google Scholar] [CrossRef]
- Galil, K.; Fair, E.; Mountcastle, N.; Britz, P.; Seward, J. Younger age at vaccination may increase risk of varicella vaccine failure. J. Infect. Dis. 2002, 186, 102–105. [Google Scholar] [CrossRef]
- Michalik, D.E.; Steinberg, S.P.; Larussa, P.S.; Edwards, K.M.; Wright, P.F.; Arvin, A.M.; Gans, H.A.; Gershon, A.A. Primary vaccine failure after 1 dose of varicella vaccine in healthy children. J. Infect. Dis. 2008, 197, 944–949. [Google Scholar] [CrossRef] [PubMed]
- L’Huillier, A.G.; Hirzel, C.; Ferreira, V.H.; Ierullo, M.; Ku, T.; Selzner, N.; Schiff, J.; Juvet, S.; Miao, C.; Schmid, D.S.; et al. Evaluation of Recombinant Herpes Zoster Vaccine for Primary Immunization of Varicella-seronegative Transplant Recipients. Transplantation 2021, 105, 2316–2323. [Google Scholar] [CrossRef] [PubMed]
- Verolet, C.M.; Pittet, L.F.; Wildhaber, B.E.; McLin, V.A.; Rodriguez, M.; Grillet, S.; Siegrist, C.A.; Posfay-Barbe, K.M. Long-term Seroprotection of Varicella-zoster Immunization in Pediatric Liver Transplant Recipients. Transplantation 2019, 103, e355–e364. [Google Scholar] [CrossRef] [PubMed]
- Ritter, M.L.; Pirofski, L. Mycophenolate mofetil: Effects on cellular immune subsets, infectious complications, and antimicrobial activity. Transpl. Infect. Dis. 2009, 11, 290–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allison, A.C.; Eugui, E.M. Mechanisms of action of mycophenolate mofetil in preventing acute and chronic allograft rejection. Transplantation 2005, 80, S181–S190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohagura, T.; Kawabe, S.; Abe, N.; Nakaseko, H.; Iwata, N. Efficacy of hepatitis B vaccination in children with rheumatic diseases. Pediatr. Int. 2021, 63, 752–756. [Google Scholar] [CrossRef]
- Anonymous. Varicella vaccines. WHO position paper. Wkly. Epidemiol. Rec. 1998, 73, 241–248. [Google Scholar]
- Czajka, H.; Schuster, V.; Zepp, F.; Esposito, S.; Douha, M.; Willems, P. A combined measles, mumps, rubella and varicella vaccine (Priorix-Tetra): Immunogenicity and safety profile. Vaccine 2009, 27, 6504–6511. [Google Scholar] [CrossRef]
- Marchetti, F.; Cuccia, M. The effectiveness of Varivax and Varilrix vaccines. Vaccine 2010, 28, 4859–4860. [Google Scholar] [CrossRef]
- Küpke, N.K.; Matysiak-Klose, D.; Siedler, A.; Wichmann, O.; Diercke, M. Gesetz für den Schutz vor Masern und zur Stärkung der Impfprävention (Masernschutzgesetz); 2020; pp. 3–5. Available online: http://www.doi.org/10.25646/6526 (accessed on 1 September 2021).
- Feldman, A.G.; Kempe, A.; Beaty, B.L.; Sundaram, S.S. Studies of Pediatric Liver Transplantation (SPLIT) Research Group Immunization practices among pediatric transplant hepatologists. Pediatr. Transplant. 2016, 20, 1038–1044. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Children (n = 207) | |
|---|---|
| Gender, female (%) | 104 (50.2%) |
| Diagnosis | Biliary atresia: 96 (46.4%) Cryptogenic cirrhosis: 22 (10.6%) Hepatic malignancy: 21 (10.1%) Acute liver failure: 17 (8.2%) PFIC: 17 (8.2%) Cystic fibrosis: 8 (3.9%) Alagille syndrome: 7 (3.4%) Citrullinemia: 4 (1.9%) Neonatal hemochromatosis: 3 (1.4%) DGUOK deficiency: 2 (1.0%) Methylmalonic aciduria: 2 (1.0%) Alpha-1 antitrypsin deficiency: 2 (1.0%) Argininosuccinate lyase deficiency: 1 (0.5%) Ornithine transcarbamylase deficiency: 1 (0.5%) Glycogen storage disease type IV: 1 (0.5%) Congenital bile acid synthesis defect: 1 (0.5%) Amanita phalloides poisoning: 1 (0.5%) |
| Year of birth, median (IQR) | 2011 (2007–2015) |
| Number of VZV doses prior to transplantation | 0 vaccinations: 95 (45.9%) 1 vaccination: 38 (18.4%) 2 vaccinations: 74 (35.7%) |
| Age at 1st VZV vaccination prior to transplantation, median (IQR) | 1.04 (0.94–1.39) |
| Age at 2nd VZV vaccination prior to transplantation, median (IQR) | 1.49 (1.23–2.57) |
| Age at time of transplant, median (IQR) | 1.56 (0.65–4.77) |
| Year of liver transplantation, median (IQR) | 2014 (2010–2018) |
| Follow-up in years, median (IQR) | 6.2 (2.0–9.5) |
| Age at 1st VZV vaccination after transplantation, median (IQR) | 3.22 (2.18–5.62) |
| Age at 1st VZV vaccination after transplantation for VZV-naïve children, median (IQR) | 2.70 (2.00–3.51) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laue, T.; Oms, E.; Ohlendorf, J.; Baumann, U. Long-Term Varicella Zoster Virus Immunity in Paediatric Liver Transplant Patients Can Be Achieved by Booster Vaccinations—A Single-Centre, Retrospective, Observational Analysis. Children 2022, 9, 130. https://doi.org/10.3390/children9020130
Laue T, Oms E, Ohlendorf J, Baumann U. Long-Term Varicella Zoster Virus Immunity in Paediatric Liver Transplant Patients Can Be Achieved by Booster Vaccinations—A Single-Centre, Retrospective, Observational Analysis. Children. 2022; 9(2):130. https://doi.org/10.3390/children9020130
Chicago/Turabian StyleLaue, Tobias, Elisabeth Oms, Johanna Ohlendorf, and Ulrich Baumann. 2022. "Long-Term Varicella Zoster Virus Immunity in Paediatric Liver Transplant Patients Can Be Achieved by Booster Vaccinations—A Single-Centre, Retrospective, Observational Analysis" Children 9, no. 2: 130. https://doi.org/10.3390/children9020130
APA StyleLaue, T., Oms, E., Ohlendorf, J., & Baumann, U. (2022). Long-Term Varicella Zoster Virus Immunity in Paediatric Liver Transplant Patients Can Be Achieved by Booster Vaccinations—A Single-Centre, Retrospective, Observational Analysis. Children, 9(2), 130. https://doi.org/10.3390/children9020130