
Discordance between Clinical and Ultrasound Examinations in Juvenile Idiopathic Arthritis: An Experimental Approach

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Examination and MSUS Evaluation
- -
- Tendons: anterior, medial, and lateral ankle compartments; wrist flexor and extensor; II finger extensor and flexor. Common extensor tendon (elbow medial epicondyle), common flexor tendon (elbow lateral epicondyle).
- -
- Bursae: olecranon, prepatellar, pretibial, retrocalcaneal, and retroachilles.
2.3. Concordance Analysis
2.4. Subclinical Synovitis
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Concordance Analysis
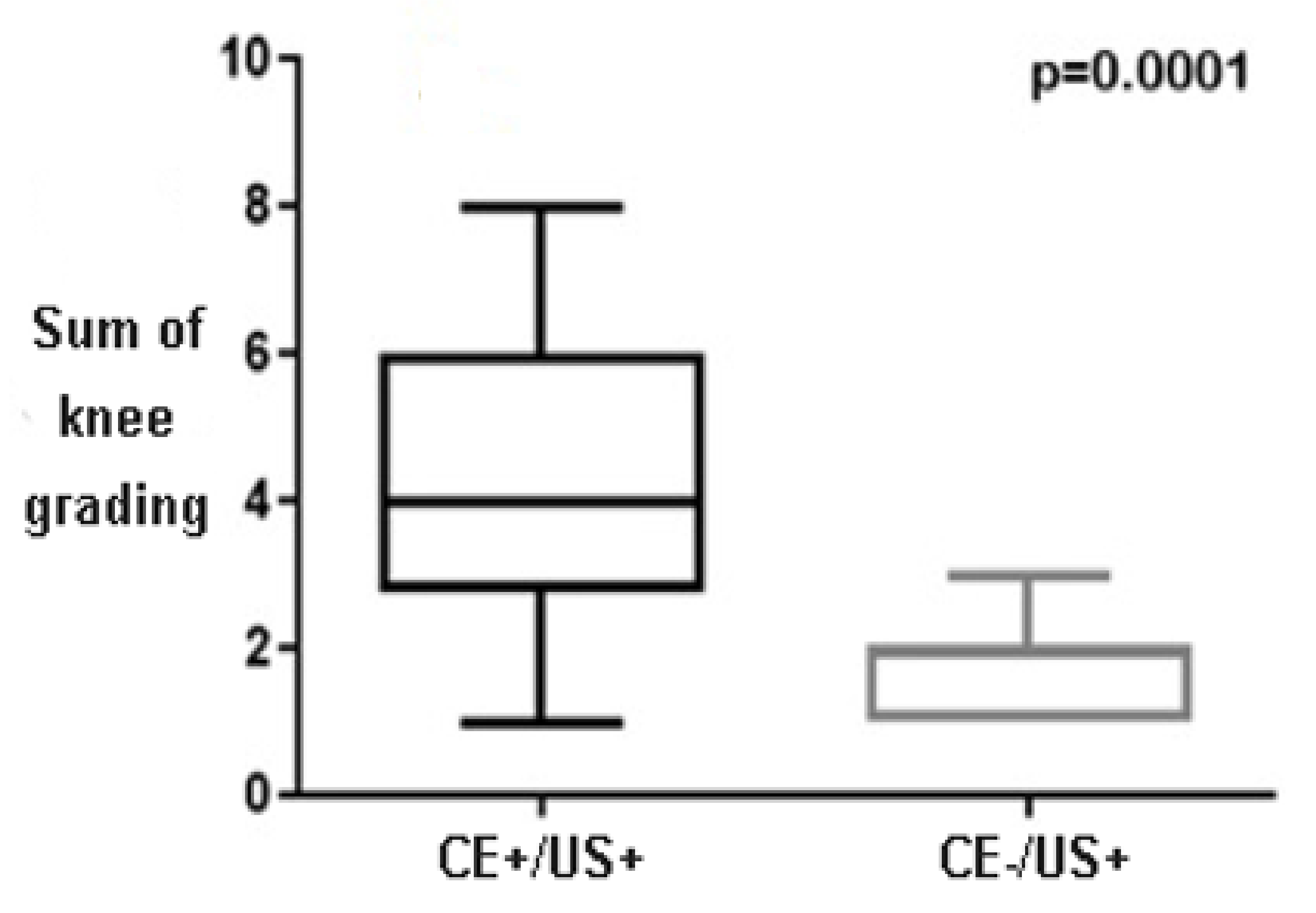
3.3. Subclinical Synovitis and Grading
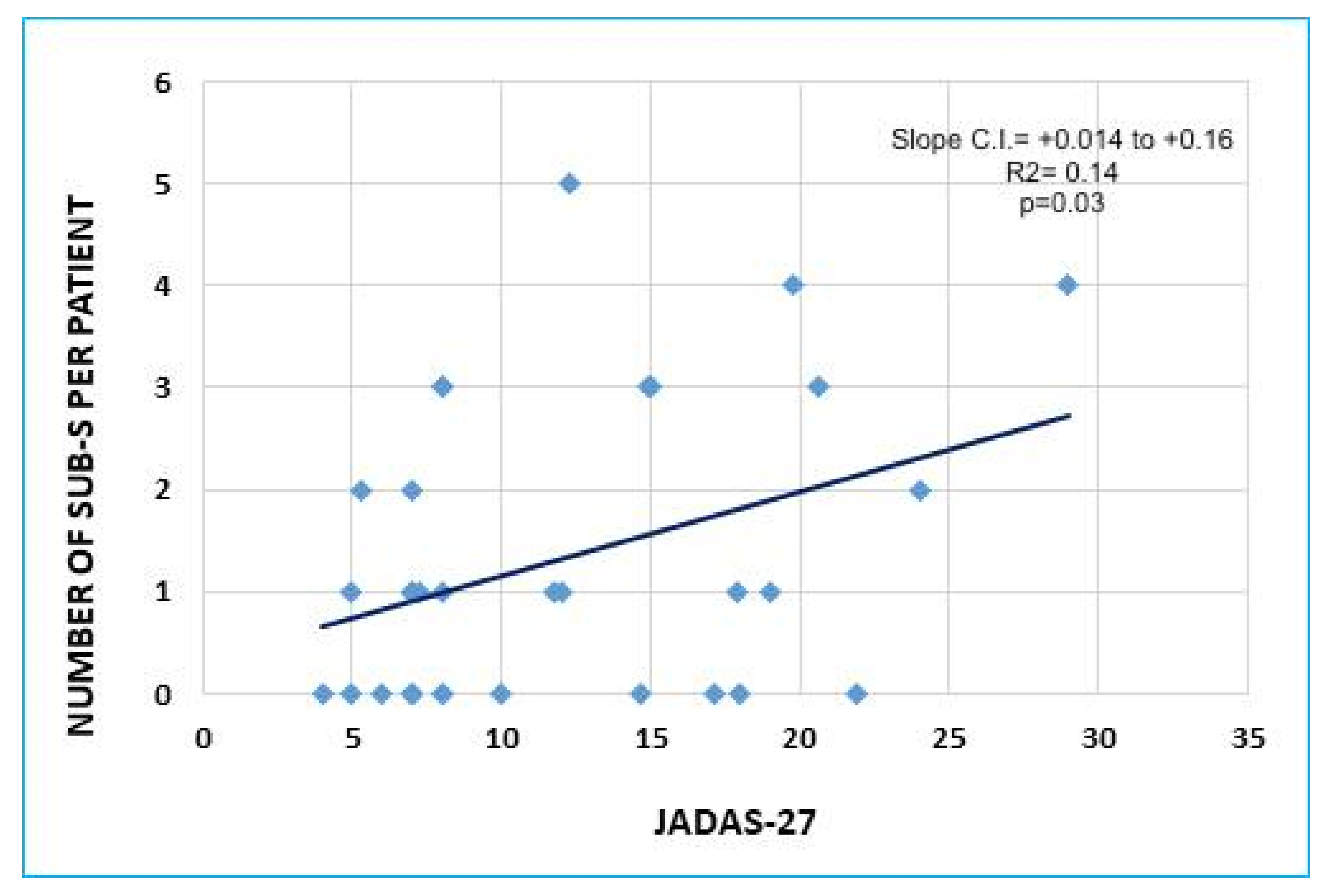
3.4. Subclinical Synovitis and Disease Status
4. Discussion and Conclusions
- Are CE+/US− articulations truly “false positive” or does inflammation interest other periarticular structures, such as tendon and bursae?
- 2.
- Is subclinical synovitis (CE−/US+) an incidental finding or is it correlated with disease activity?
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collado, P.; Neredo, E.; Calvo, C.; Gamir, M.L.; Merino, R.; Grana, J.; Bustabab, S.; Garrido, J. Reduced joint assessment vs comprehensive assessment for ultrasound detection of synovitis in juvenile idiopathic arthritis. Rheumatology 2013, 52, 1477–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magni-Manzoni, S.; Epis, O.; Ravelli, A.; Klersky, C.; Veisconti, C.; Lanni, S.; Muratore, V.; Scire, C.A.; Rossi, S.; Montecucco, C. Comparison of clinical versus ultrasound-determined synovitis in juvenile idiopathic arthritis. Arthritis Rheum. 2009, 61, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- Haslam, K.E.; McCann, L.J.; Wyatt, S.; Wakefield, R.J. The detection of subclinical synovitis by ultrasound in oligoarticular juvenile idiopathic arthritis: A pilot study. Rheumatology 2010, 49, 123–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Consolaro, A.; Bracciolini, G.; Ruperto, N.; Pistorio, A.; Magni-Manzoni, S.; Malattia, C.; Pederzoli, S.; Davi, S.; Martini, A.; Ravelli, A. Remission, minimal disease activity, and acceptable symptom state in juvenile idiopathic arthritis: Defining criteria based on the juvenile arthritis disease activity score. Arthritis Rheum. 2012, 64, 2366–2374. [Google Scholar] [CrossRef] [PubMed]
- Roth, J.; Ravagnani, V.; Backhaus, M.; Balint, P.; Bruns, A.; Bruyn, G.A.; Collado, P.; De la Cruz, L.; Guillaume-Czitrom, S.; Herlin, T.; et al. Preliminary Definitions for the Sonographic Features of Synovitis in Children. Arthritis Care Res. 2017, 69, 1217–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terslev, L.; Iagnocco, A.; Bruyn, G.A.W.; Neredo, E.; Vojnovic, J.; Collado, P.; Damjanov, N.; Filer, A.; Filippou, G.; Finzel, S.; et al. The OMERACT Ultrasound Group: A Report from the OMERACT 2016 Meeting and Perspectives. J. Rheumatol. 2017, 44, 1740–1743. [Google Scholar] [CrossRef] [PubMed]
- Windschall, D.; Collado, P.; Vojinovic, J.; Magni-Manzoni, S.; Balint, P.; Bruyn, G.A.W.; Hernandez-Diaz, C.; Nieto, J.C.; Ravagnani, V.; Tzaribachev, N.; et al. Age-related vascularization and ossification of joints in children: An international pilot study to test multi-observer ultrasound reliability. Arthritis Care Res. 2017, 72, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Collado, P.; Vojnovic, J.; Nieto, J.C.; Windschall, D.; Magni-Manzoni, S.; Bruyn, G.A.; Iagnocco, A.; D’agostino, M.A.; Naredo, E. Toward Standardized Musculoskeletal Ultrasound in Pediatric Rheumatology: Normal Age-Related Ultrasound Findings. Arthritis Care Res. 2016, 68, 348–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascoli, L.; Wright, S.; McAllister, C.; Rooney, M. Prospective Evaluation of Clinical and Ultrasound Findings in Ankle Disease in Juvenile Idiopathic Arthritis: Importance of Ankle Ultrasound. J. Rheumatol. 2010, 37, 2409–2414. [Google Scholar] [CrossRef] [PubMed]
- Lanni, S.; Bovis, F.; Ravelli, A.; Viola, S.; Magnaguagno, F.; Pistorio, A.; Magnano, G.M.; Martini, A.; Malattia, C. Delineating the Application of Ultrasound in Detecting Synovial Abnormalities of the Subtalar Joint in Juvenile Idiopathic Arthritis. Arthritis Care Res. 2016, 68, 1346–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanni, S.; Marafon, D.P.; Civino, A.; Alongi, A.; Proverbio, E.; Agostoni, C.; Ravelli, A.; Filocamo, G. Comparison Between Clinical and Ultrasound Assessment of the Ankle Region in Children with Juvenile Idiopathic Arthritis. Arthritis Care Res. 2021, 73, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- De Lucia, O.; Ravagnani, V.; Pregnolato, F.; Hila, A.; Pontikaki, I.; Gattinara, M.; Romano, M.; Gerloni, V.; Pieropan, S.; Murgo, A.; et al. Baseline ultrasound examination as possible predictor of relapse in patients affected by juvenile idiopathic arthritis (JIA). Ann. Rheum. Dis. 2018, 77, 1426–1431. [Google Scholar] [CrossRef] [PubMed]
- Consolaro, A.; Ruperto, N.; Bazso, A.; Pistorio, A.; Magni-Manzoni, S.; Filocamo, G.; Malattia, C.; Viola, S.; Martini, A.; Ravelli, A. Development and validation of a composite disease activity score for juvenile idiopathic arthritis. Arthritis Rheum. 2009, 61, 658–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Active Group | Remission Group | p-Value | |
|---|---|---|---|
| Total number of patients | 35 | 15 | - |
| Female patients % | 80.0% | 73.3% | p = 0.71 |
| Mean age (months) | 102.7 ± 51.5 | 94 ± 39.5 | p = 0.43 |
| ILAR category | 21 with oligoarthritis (60%); 1 with polyarthritis RF pos (3%) 8 with polyarthritis RF neg (23%) 3 with psoriatic arthritis (8%); 2 with enthesitis-related arthritis (6%). | 9 with oligoarthritis (60%); 3 with polyarthritis RF neg (20%); 3 with psoriatic arthritis (20%); | p = 1.00 |
| Mean disease duration (months) | 27.7 ± 39.5 | 55.7 ± 37.1 | p = 0.002 |
| Disease status | 16 disease onset (45.7%); 8 relapse off-therapy (23%); 11 relapse in MTX (31.4%) | 15 disease remission | p < 0.0001 |
| ESR (n.v. < 20 mm/h) | 20.8 ± 20.5 | 4.3± 4.8 | p < 0.0001 |
| CRP (n.v. < 5 mg/L) | 7.4 ± 12.7 | 2.6 ± 2.7 | p = 0.61 |
| ANA positivity | 17 (48.6%) | 6 (40.0%) | p = 0.76 |
| CE+/US+ per patient | 1.0 ±1.2 | 0 | p < 0.0001 |
| CE−/US+ per patient | 1.3 ± 1.3 | 0.4 ± 0.7 | p = 0.03 |
| CE+ | CE− | ||
|---|---|---|---|
| ELBOW | US+ | 7% | 0% |
| US− | 2% | 91% | |
| KNEE | US+ | 31% | 24% |
| US− | 4% | 41% | |
| WRIST | US+ | 1% | 7% |
| US− | 6% | 86% | |
| ANKLE | US+ | 9% | 21% |
| US− | 11% | 59% | |
| II MCP | US+ | 4% | 10% |
| US− | 1% | 85% | |
| TOTAL | US+ | 11% | 13% |
| US− | 5% | 71% | |
| Articular Compartment | Articular + Extra-Articular Compartment | |
|---|---|---|
| ELBOW | k = 0.89 C.I. (0.70–1.0) | k = 0.89 C.I. (0.70–1.0) |
| KNEE | k = 0.45 C.I. (0.26–0.63) | k = 0.48 C.I. (0.27–0.65) |
| WRIST | k = 0.11 C.I. (0.00–0.43) | k = 0.41 C.I. (0.06–0.76) |
| ANKLE | k = 0.13 C.I. (0.00–0.38) | k = 0.27 C.I. (0.05–0.49) |
| II MCP | k = 0.38 C.I. (0.05–0.71) | k = 0.29 C.I. (0.00–0.58) |
| TOTAL | k = 0.43 C.I. (0.32–0.55) | k = 0.49 C.I. (0.37–0.59) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Licciardi, F.; Petraz, M.; Covizzi, C.; Santarelli, F.; Cirone, C.; Mulatero, R.; Robasto, F.; Dellepiane, M.; Martino, S.; Montin, D.; et al. Discordance between Clinical and Ultrasound Examinations in Juvenile Idiopathic Arthritis: An Experimental Approach. Children 2022, 9, 333. https://doi.org/10.3390/children9030333
Licciardi F, Petraz M, Covizzi C, Santarelli F, Cirone C, Mulatero R, Robasto F, Dellepiane M, Martino S, Montin D, et al. Discordance between Clinical and Ultrasound Examinations in Juvenile Idiopathic Arthritis: An Experimental Approach. Children. 2022; 9(3):333. https://doi.org/10.3390/children9030333
Chicago/Turabian StyleLicciardi, Francesco, Marco Petraz, Carlotta Covizzi, Francesca Santarelli, Carlotta Cirone, Roberta Mulatero, Francesca Robasto, Marta Dellepiane, Silvana Martino, Davide Montin, and et al. 2022. "Discordance between Clinical and Ultrasound Examinations in Juvenile Idiopathic Arthritis: An Experimental Approach" Children 9, no. 3: 333. https://doi.org/10.3390/children9030333
APA StyleLicciardi, F., Petraz, M., Covizzi, C., Santarelli, F., Cirone, C., Mulatero, R., Robasto, F., Dellepiane, M., Martino, S., Montin, D., & Ravagnani, V. (2022). Discordance between Clinical and Ultrasound Examinations in Juvenile Idiopathic Arthritis: An Experimental Approach. Children, 9(3), 333. https://doi.org/10.3390/children9030333