
Effectiveness of Mental Health Literacy Programs in Primary and Secondary Schools: A Systematic Review with Meta-Analysis

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
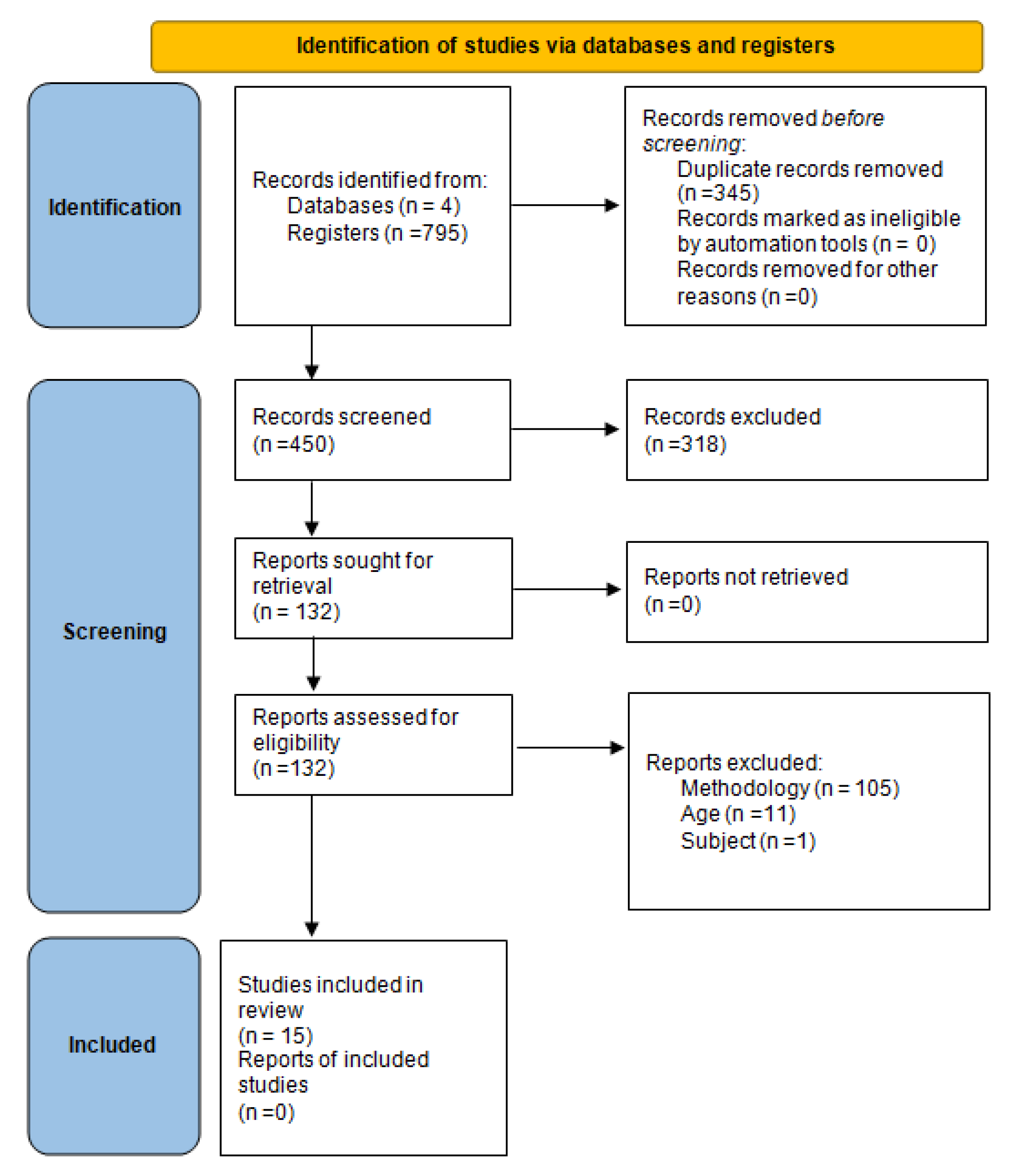
2.2. Study Search and Selection Strategy
2.3. Analysis
3. Results
3.1. Study Description
3.2. Study Quality
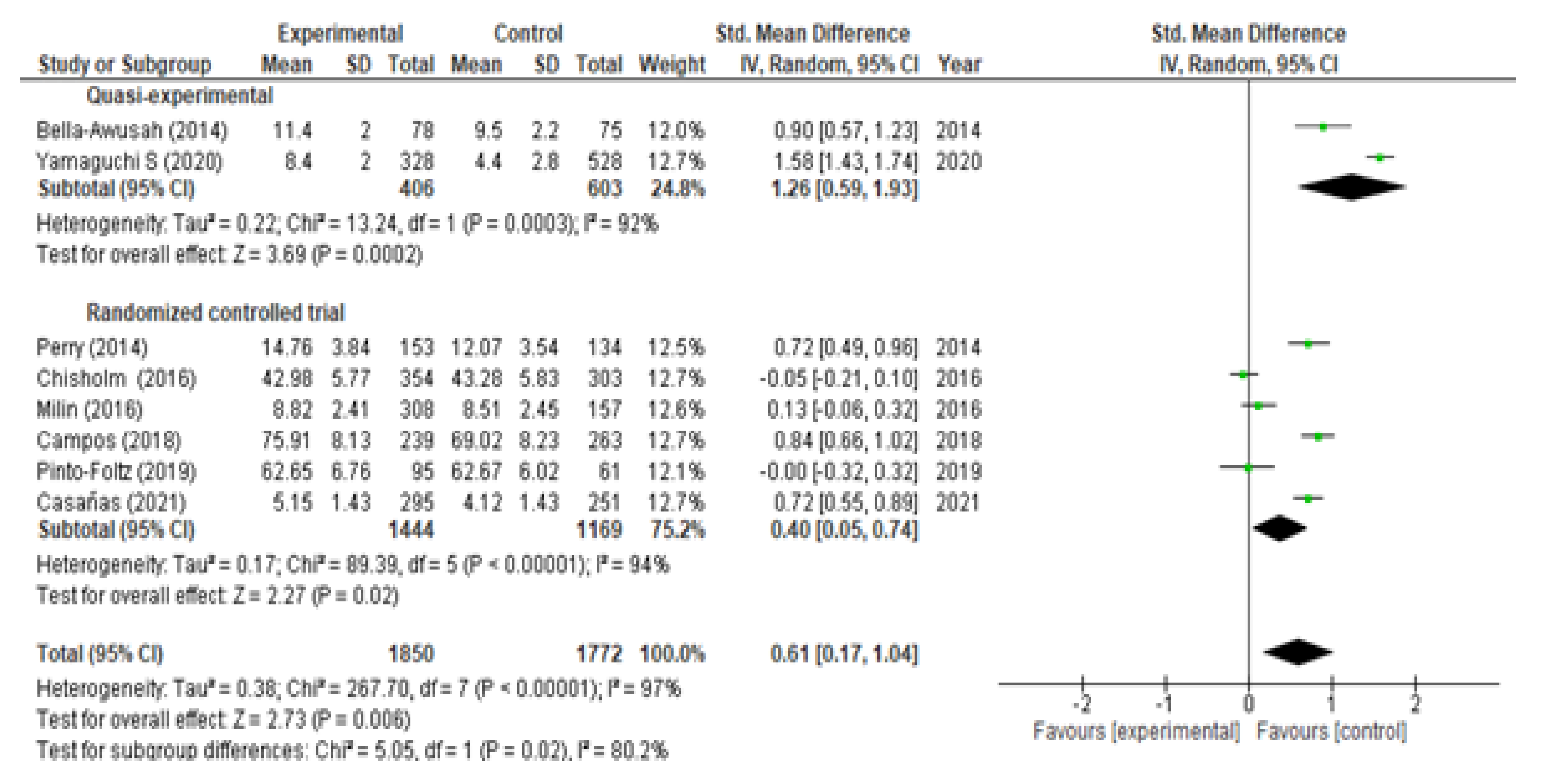
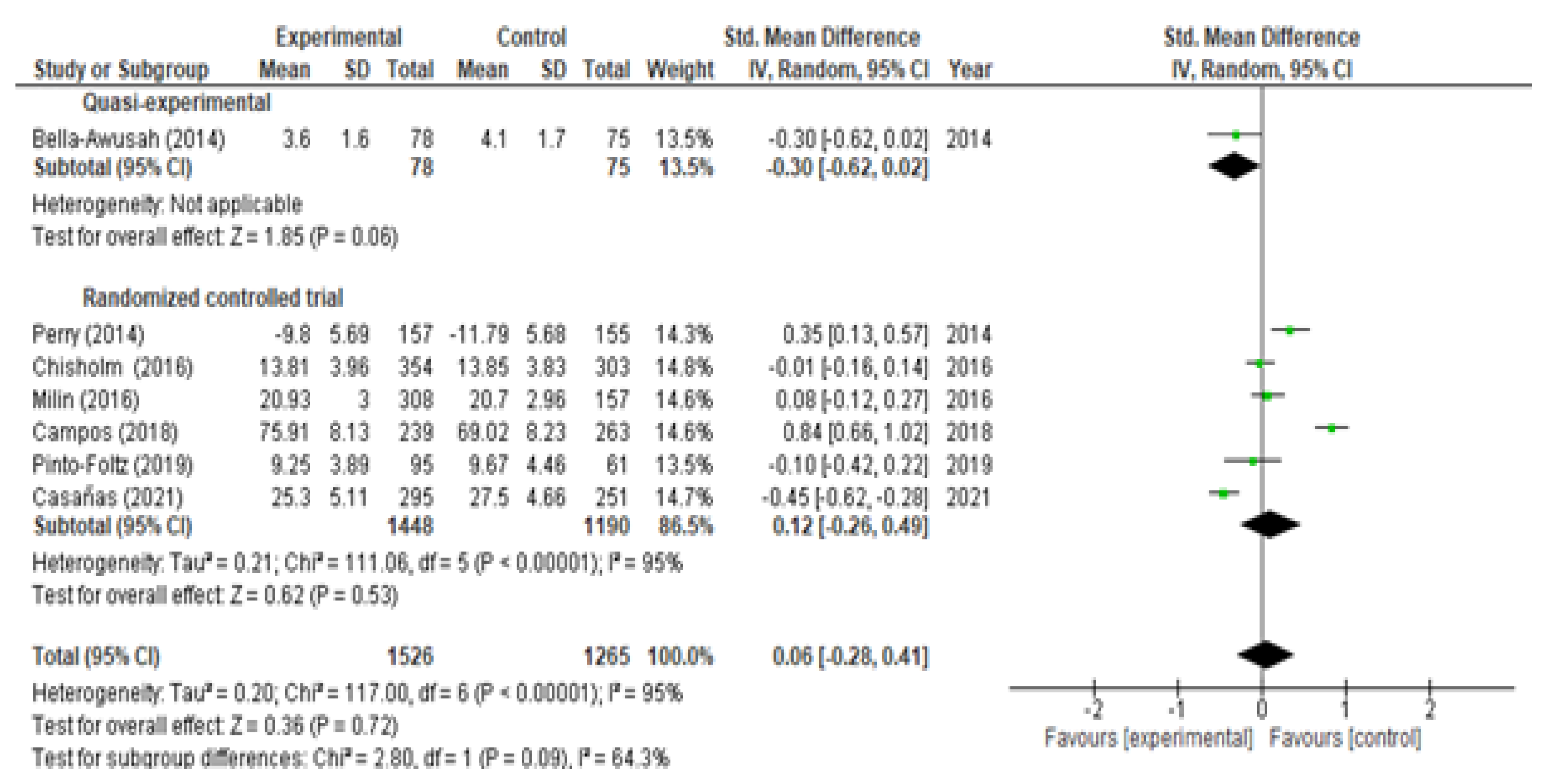
3.3. Evaluation of Mental Health Knowledge
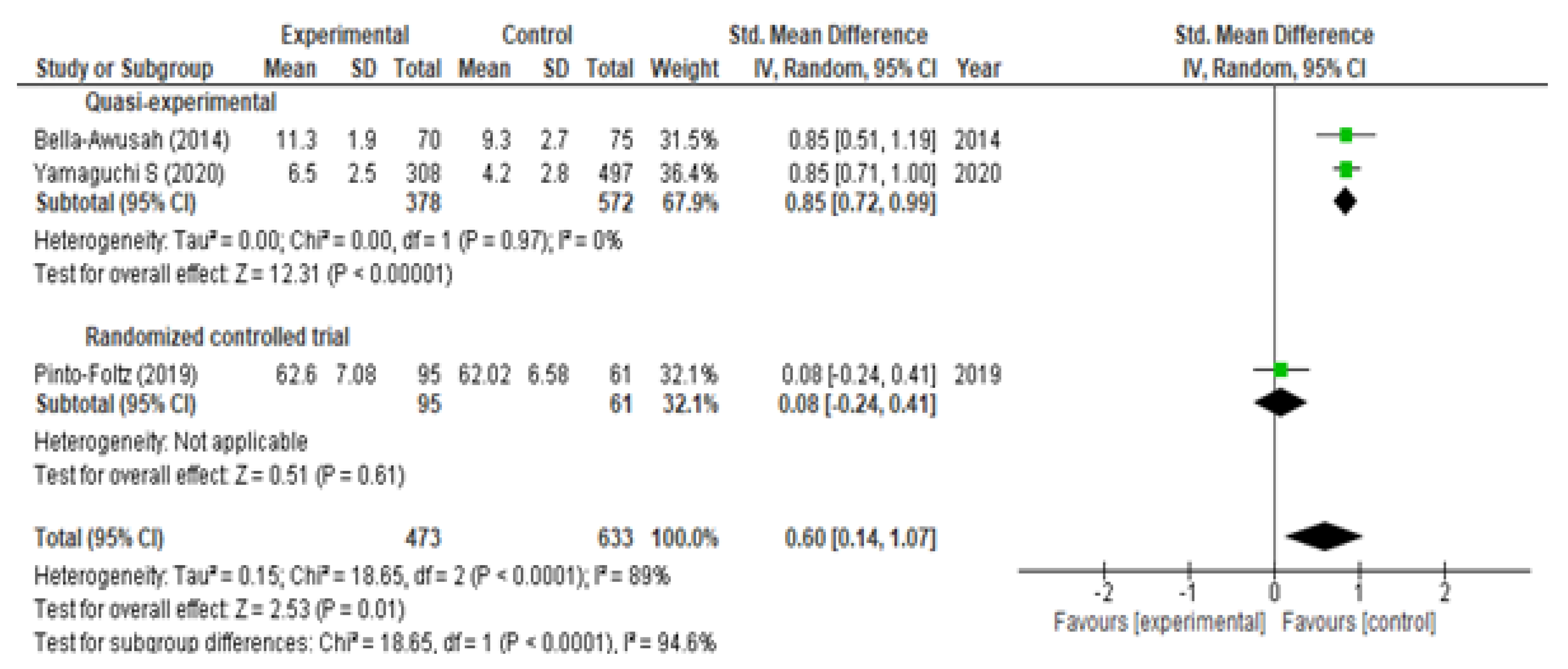
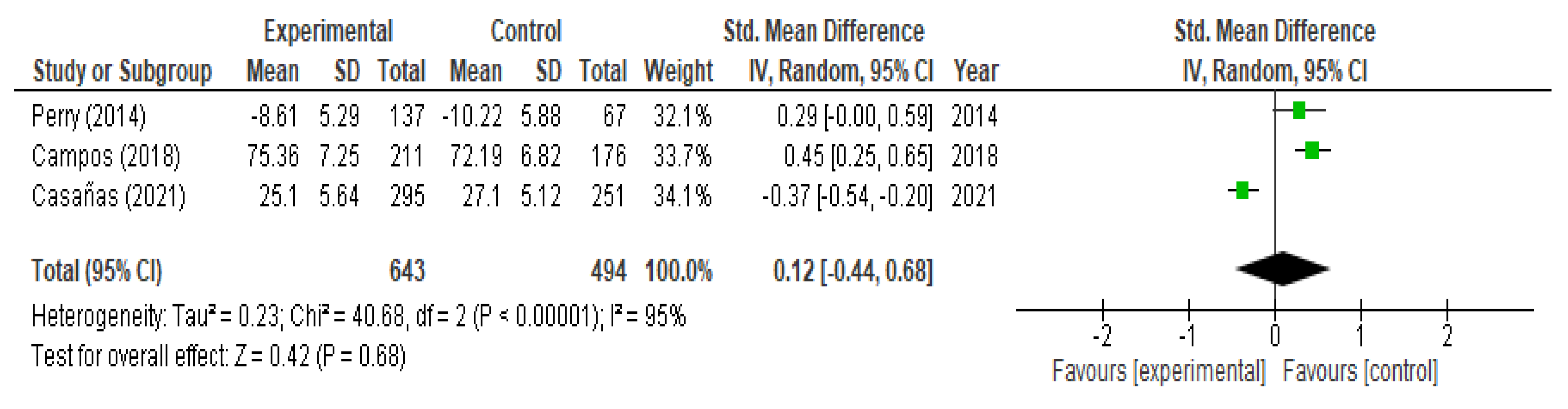
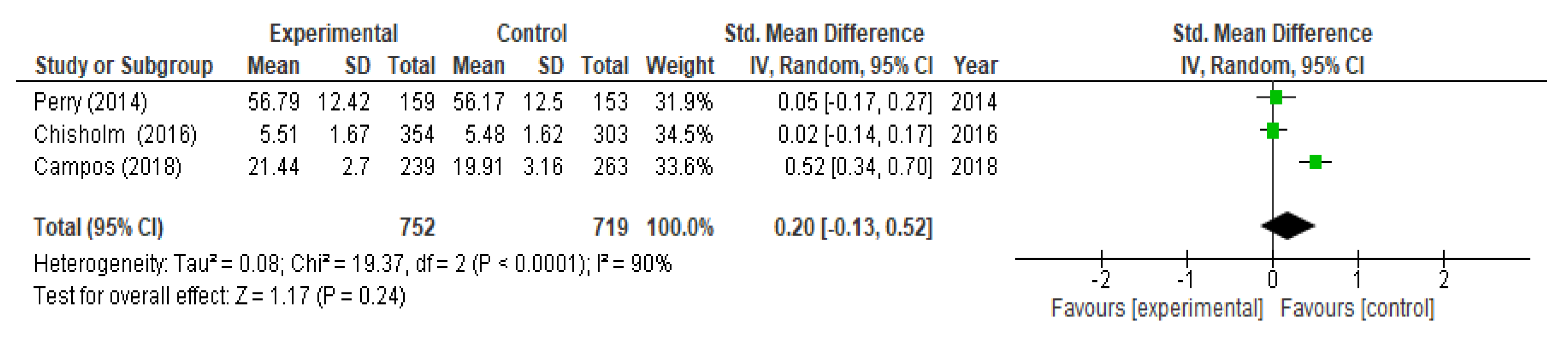
3.4. Evaluation of Mental Health Stigma/Attitudes
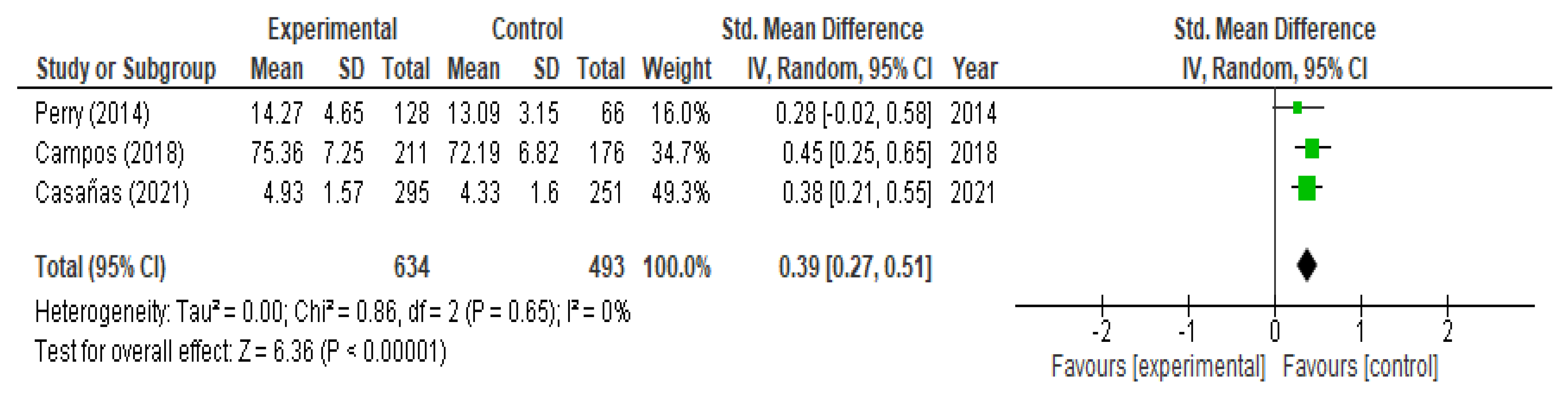
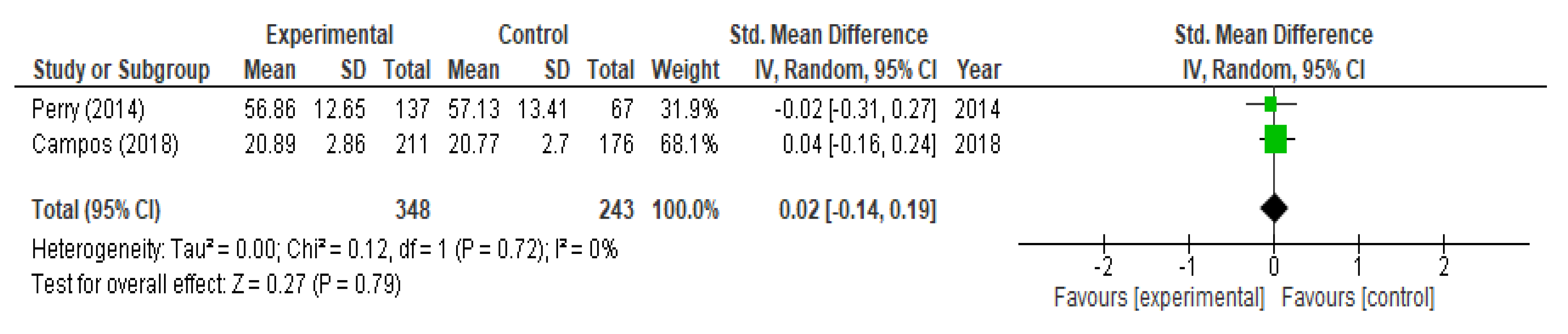
3.5. Evaluation of Help-Seeking
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Levels of Evidence | |
|---|---|
| 1++ | High-quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias |
| 1+ | Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias |
| 1− | Meta-analyses, systematic reviews, or RCTs with a high risk of bias |
| 2++ | High-quality systematic reviews of case control or cohort or studies High-quality case control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal |
| 2+ | Well-conducted case control or cohort studies with a low risk of confounding or bias and a moderate probability that the relationship is causal |
| 2− | Case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal |
| 3 | Non-analytic studies, e.g., case reports, case series |
| 4 | Expert opinion |
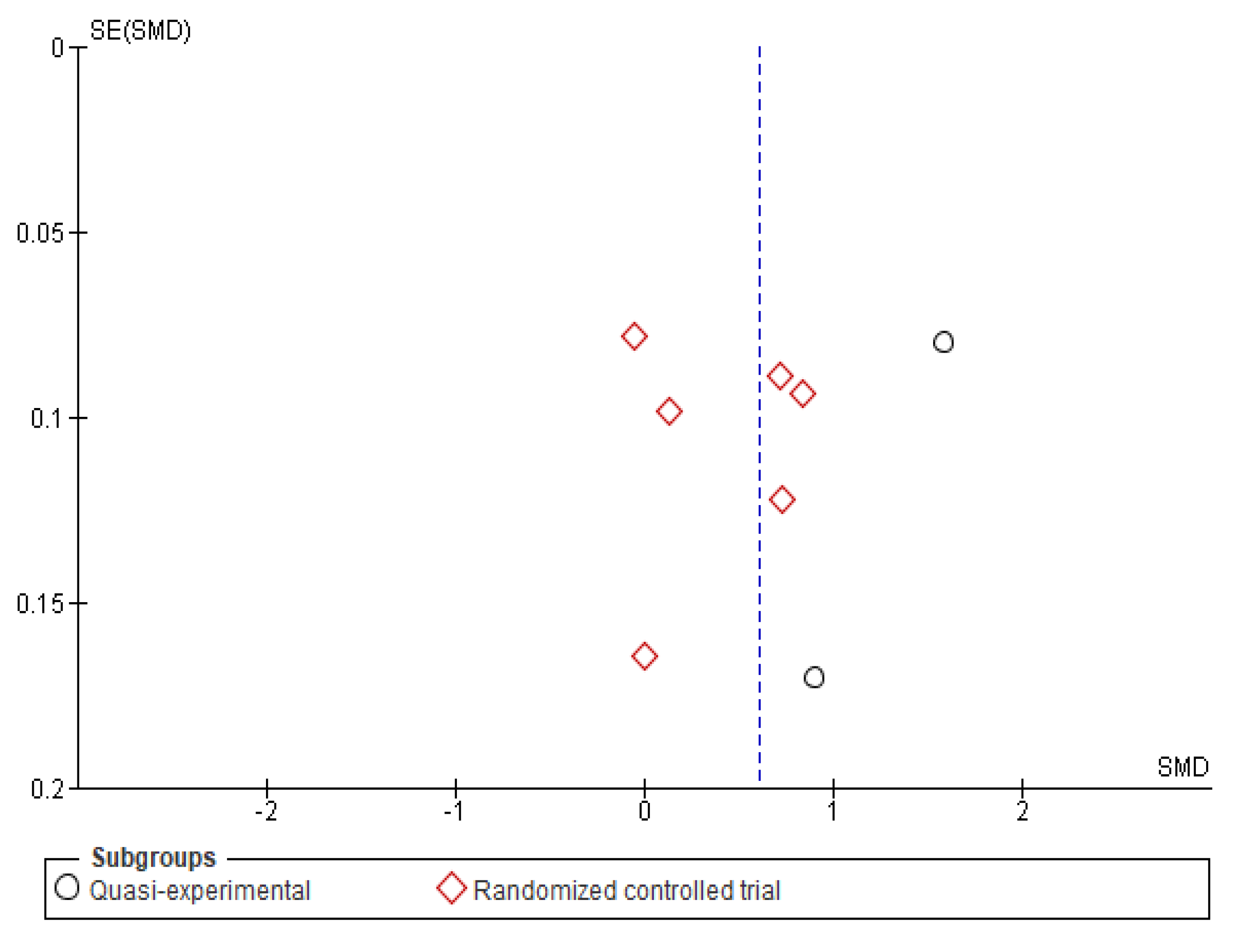
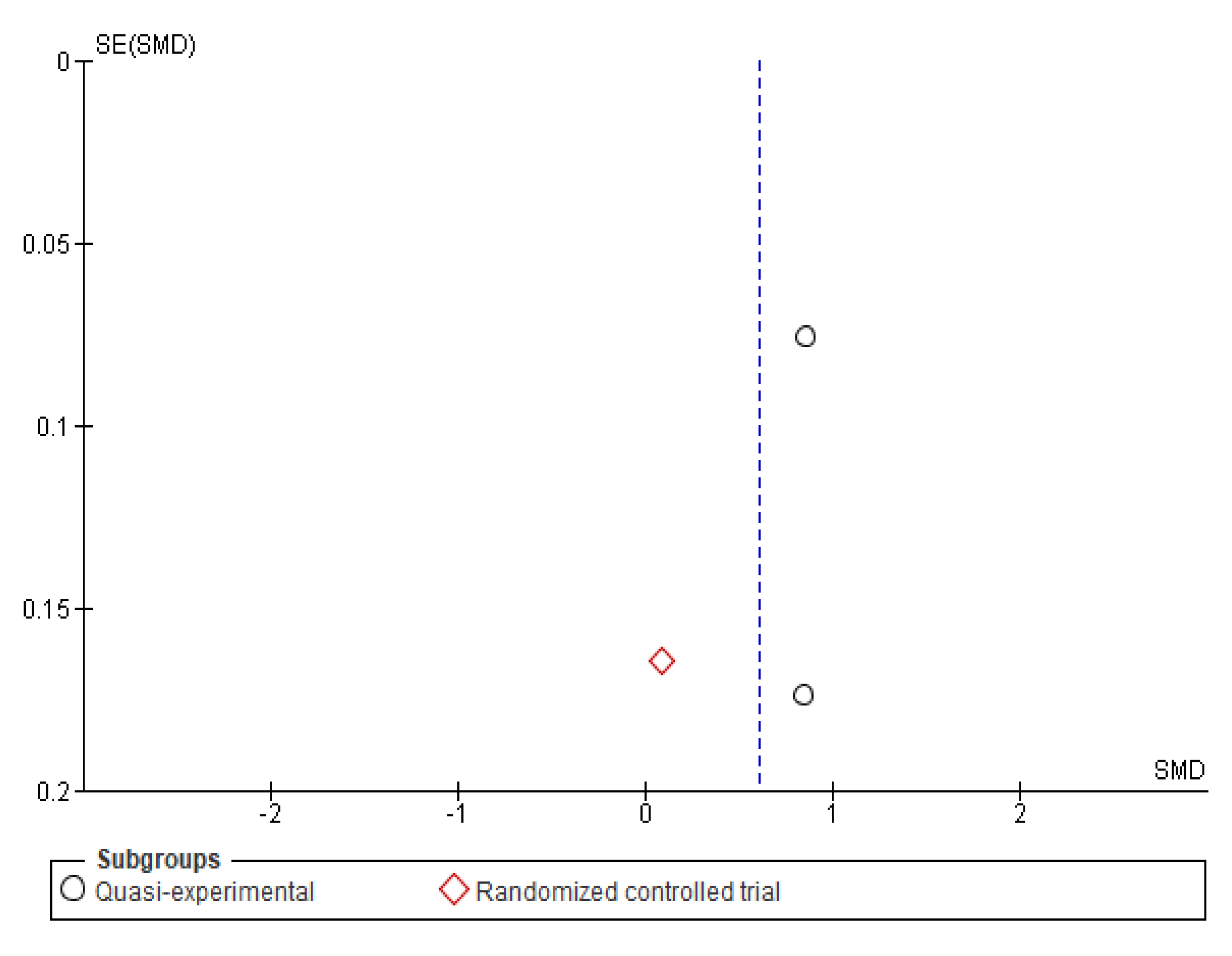
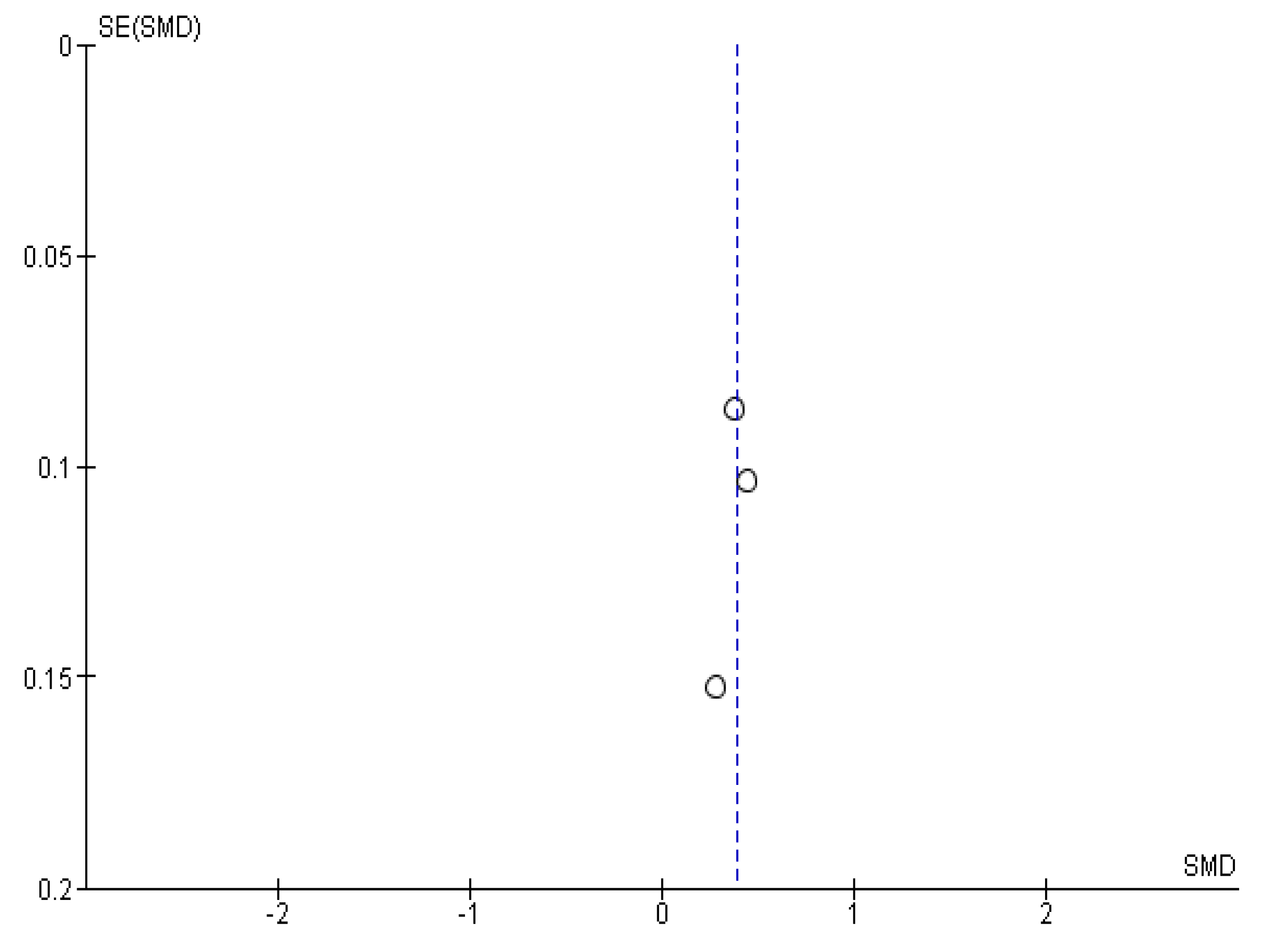
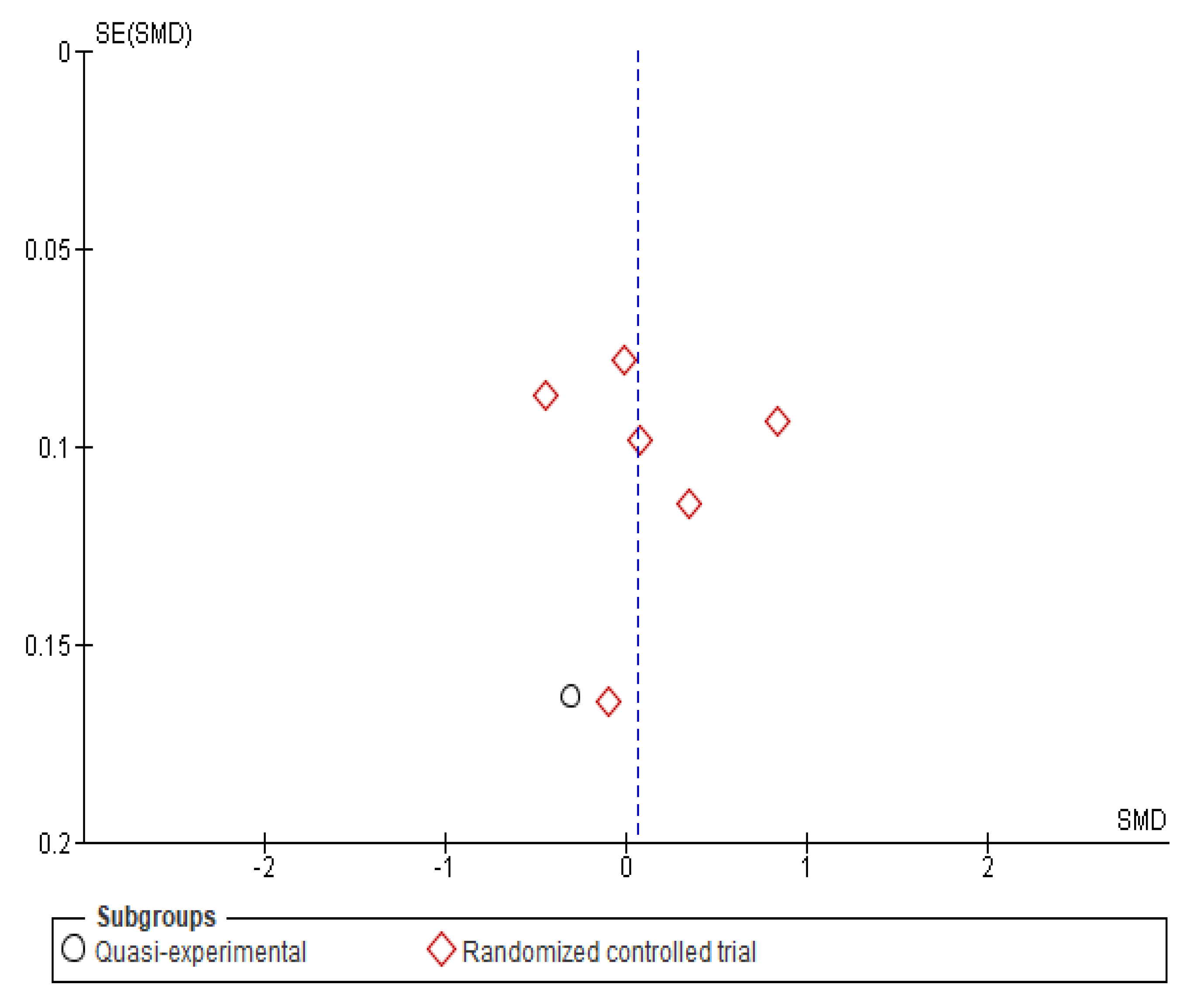
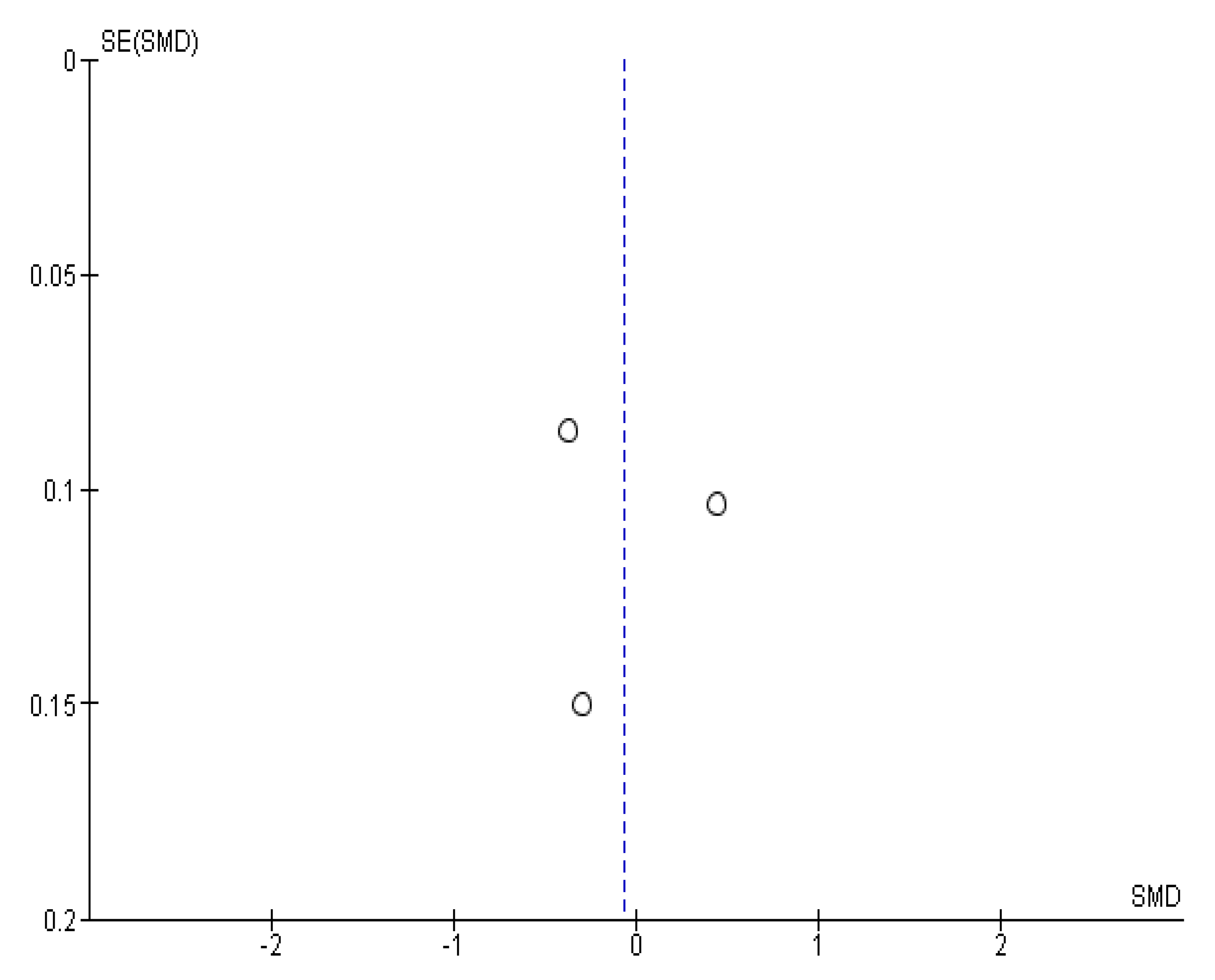
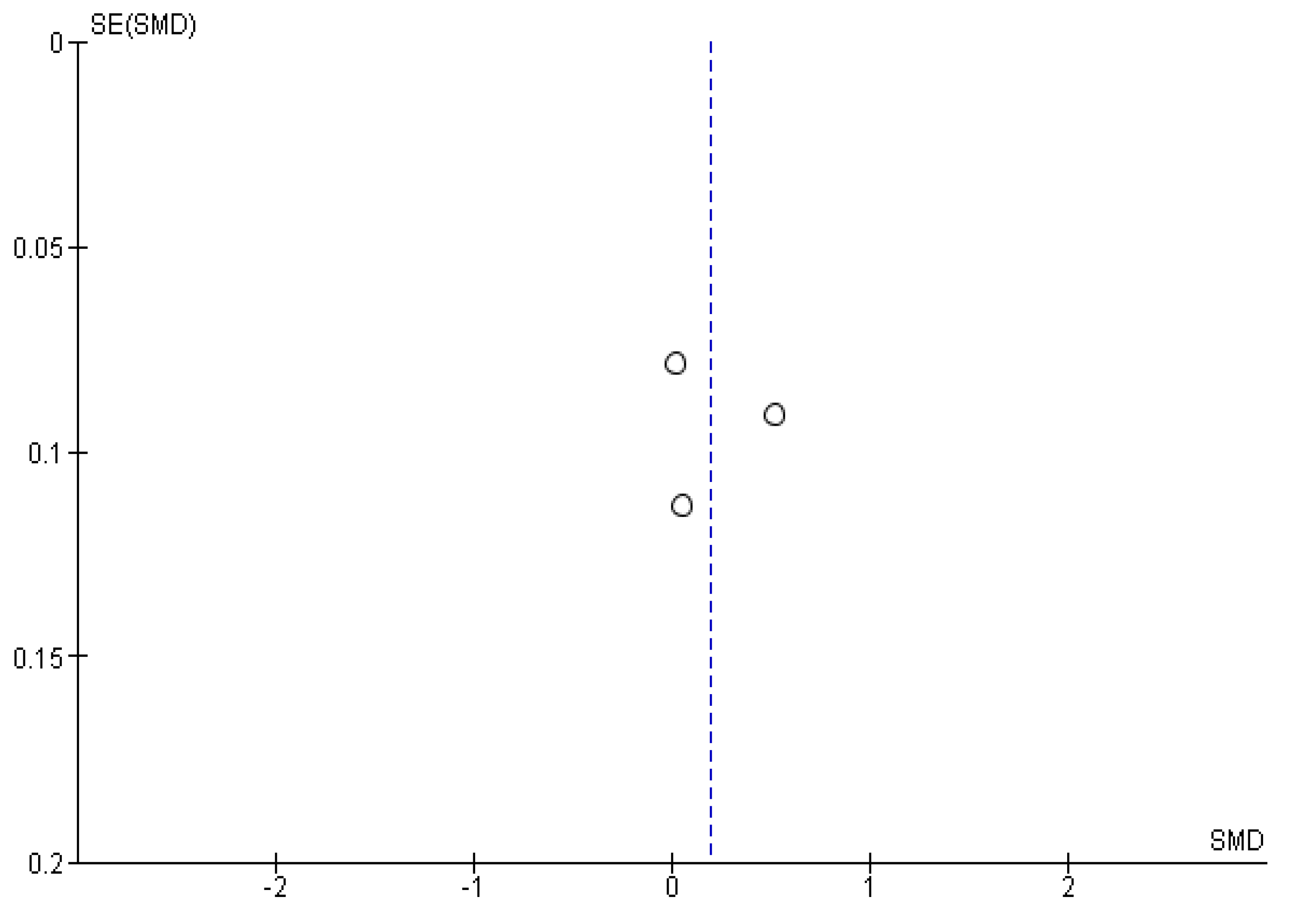
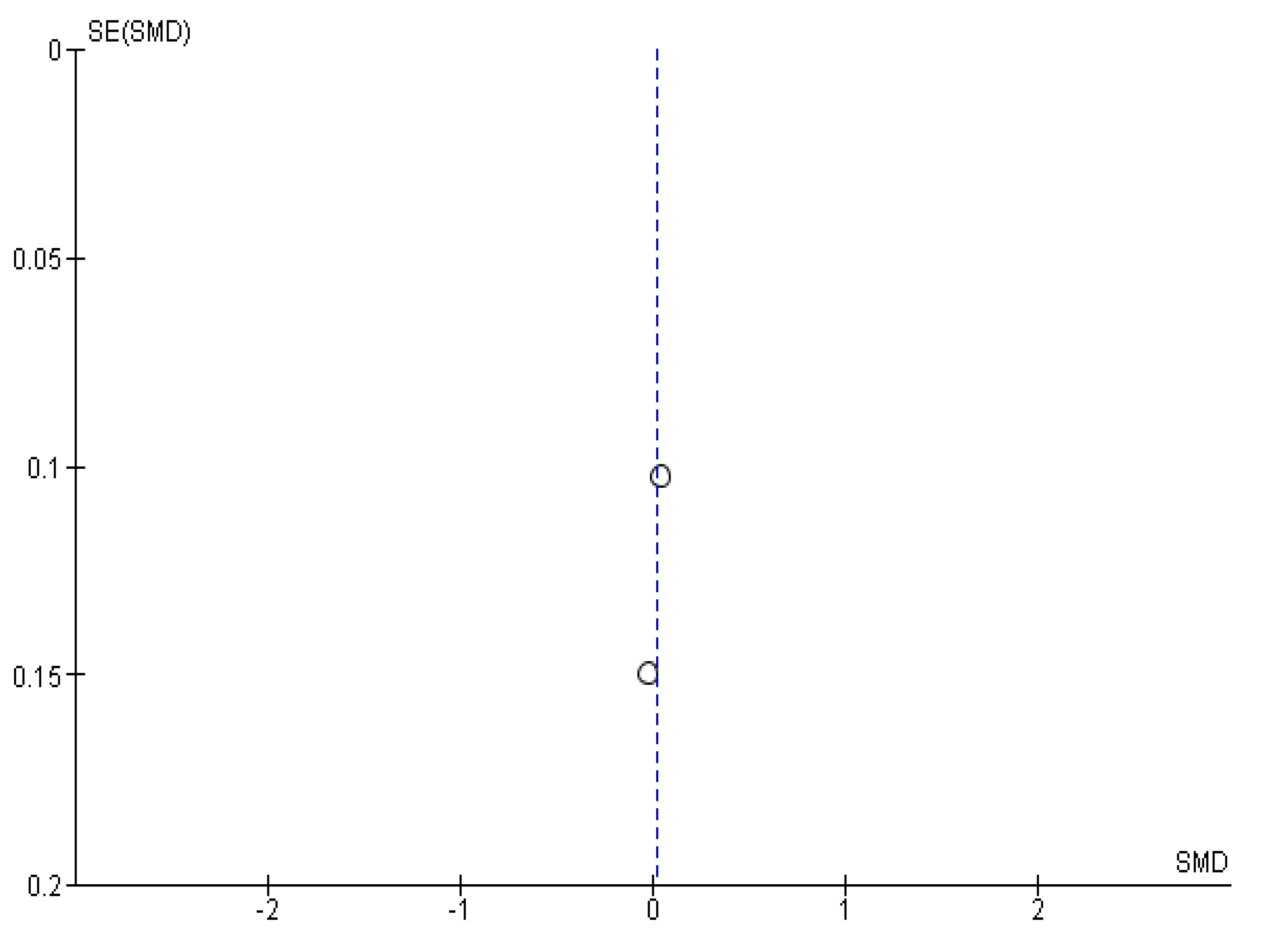
Appendix B. Funnel Plots







References
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, Y.; Hayden, J.A.; Kutcher, S.; Zygmunt, A.; McGrath, P. The Effectiveness of School Mental Health Literacy Programs to Address Knowledge, Attitudes and Help Seeking among Youth. Early Interv. Psychiatry 2013, 7, 109–121. [Google Scholar] [CrossRef] [PubMed]
- WHO. Salud Mental del Adolescente. Available online: https://www.who.int/es/news-room/fact-sheets/detail/adolescent-mental-health (accessed on 9 March 2022).
- Thornicroft, G. Most People with Mental Illness Are Not Treated. Lancet 2007, 370, 807–808. [Google Scholar] [CrossRef]
- European Commision. EU-Compass for Action on Mental Health and Well-Being. Available online: https://ec.europa.eu/health/non_communicable_diseases/mental_health/eu_compass_es (accessed on 23 December 2021).
- OECD/European Union. Health at a Glance: Europe 2018 State of Health in the Eu Cycle; OECD/European Union: Brussels, Belgium, 2018. [Google Scholar] [CrossRef]
- WHO. Plan de Acción Sobre Salud Mental 2013–2020. Available online: https://apps.who.int/iris/handle/10665/97488 (accessed on 23 December 2021).
- WHO. Comprehensive Mental Health Action Plan 2013–2030. Available online: https://apps.who.int/iris/handle/10665/345301 (accessed on 9 March 2022).
- Jorm, A.F.; Korten, A.E.; Jacomb, P.A.; Christensen, H.; Rodgers, B.; Pollitt, P. “Mental Health Literacy”: A Survey of the Public’s Ability to Recognise Mental Disorders and Their Beliefs about the Effectiveness of Treatment. Med. J. Aust. 1997, 166, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Kutcher, S.; Bagnell, A.; Wei, Y. Mental Health Literacy in Secondary Schools: A Canadian Approach. Child Adolesc. Psychiatr. Clin. N. Am. 2015, 24, 233–244. [Google Scholar] [CrossRef]
- Kutcher, S.; Wei, Y.; Coniglio, C. Mental Health Literacy: Past, Present, and Future. Can. J. Psychiatry. Rev. Can. de Psychiatr. 2016, 61, 154. [Google Scholar] [CrossRef] [Green Version]
- Jorm, A.F. Mental Health Literacy; Empowering the Community to Take Action for Better Mental Health. Am. Psychol. 2012, 67, 231–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seedaket, S.; Turnbull, N.; Phajan, T.; Wanchai, A. Improving Mental Health Literacy in Adolescents: Systematic Review of Supporting Intervention Studies. Trop. Med. Int. Health 2020, 25, 1055–1064. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Booth, A. PROSPERO: International Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/ (accessed on 9 March 2022).
- Scottish Intercollegiate Guidelines Network. SIGN 50. Edinburgh, Scotland. Scottish Intercollegiate Guidelines Network 2011. Available online: https://www.sign.ac.uk/assets/sign50_2011.pdf (accessed on 9 March 2022).
- Kazdin, A.E. Single Case Research Designs Methods for Clinical and Applied Settings. Available online: https://es.scribd.com/document/467726259/Single-Case-Research-Designs-Methods-For-Clinical-And-Applied-Settings-by-Alan-E-Kazdin-z-lib-org-pdf (accessed on 9 March 2022).
- Cohen, J. Some Statistical Issues in Psychological Research. Available online: https://www.coursehero.com/file/p7c9i472/Cohen-J-1965-Some-statistical-issues-in-psychological-research-In-B-B-Wolman-Ed/ (accessed on 9 March 2022).
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, Y.; Petrie, K.; Buckley, H.; Cavanagh, L.; Clarke, D.; Winslade, M.; Hadzi-Pavlovic, D.; Manicavasagar, V.; Christensen, H. Effects of a Classroom-Based Educational Resource on Adolescent Mental Health Literacy: A Cluster Randomized Controlled Trial. J. Adolesc. 2014, 37, 1143–1151. [Google Scholar] [CrossRef]
- Milin, R.; Kutcher, S.; Lewis, S.P.; Walker, S.; Wei, Y.; Ferrill, N.; Armstrong, M.A. Impact of a Mental Health Curriculum on Knowledge and Stigma Among High School Students: A Randomized Controlled Trial. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 383–391.e1. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, K.; Patterson, P.; Torgerson, C.; Turner, E.; Jenkinson, D.; Birchwood, M. Impact of Contact on Adolescents’ Mental Health Literacy and Stigma: The SchoolSpace Cluster Randomised Controlled Trial. BMJ Open 2016, 6, e009435. [Google Scholar] [CrossRef] [Green Version]
- Campos, L.; Dias, P.; Duarte, A.; Veiga, E.; Dias, C.C.; Palha, F. Is It Possible to “Find Space for Mental Health” in Young People? Effectiveness of a School-Based Mental Health Literacy Promotion Program. Int. J. Environ. Res. Public Health 2018, 15, 1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto-Foltz, M.D.; Logsdon, M.C.; Myers, J.A. Feasibility, Acceptability, and Initial Efficacy of a Knowledge-Contact Program to Reduce Mental Illness Stigma and Improve Mental Health Literacy in Adolescents. Soc. Sci. Med. 2011, 72, 2011. [Google Scholar] [CrossRef] [Green Version]
- Casañas, R.; Arfuch, V.M.; Castellví, P.; Gil, J.J.; Torres, M.; Pujol, A.; Castells, G.; Teixidó, M.; San-Emeterio, M.T.; Sampietro, H.M.; et al. “EspaiJove.Net”- A School-Based Intervention Programme to Promote Mental Health and Eradicate Stigma in the Adolescent Population: Study Protocol for a Cluster Randomised Controlled Trial. BMC Public Health 2018, 18, 939. [Google Scholar] [CrossRef] [PubMed]
- Skre, I.; Friborg, O.; Breivik, C.; Johnsen, L.I.; Arnesen, Y.; Wang, C.E.A. A School Intervention for Mental Health Literacy in Adolescents: Effects of a Non-Randomized Cluster Controlled Trial. BMC Public Health 2013, 13, 873. [Google Scholar] [CrossRef] [Green Version]
- Bella-Awusah, T.; Adedokun, B.; Dogra, N.; Omigbodun, O. The Impact of a Mental Health Teaching Programme on Rural and Urban Secondary School Students’ Perceptions of Mental Illness in Southwest Nigeria. J. Child Adolesc. Ment. Health 2014, 26, 207–215. [Google Scholar] [CrossRef]
- Mcluckie, A.; Kutcher, S.; Wei, Y.; Weaver, C. Sustained Improvements in Students’ Mental Health Literacy with Use of a Mental Health Curriculum in Canadian Schools. BMC Psychiatry 2014, 14, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutcher, S.; Wei, Y.; Morgan, C. Successful Application of a Canadian Mental Health Curriculum Resource by Usual Classroom Teachers in Significantly and Sustainably Improving Student Mental Health Literacy. Can. J. Psychiatry. Rev. Can. Psychiatr. 2015, 60, 580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojio, Y.; Yonehara, H.; Taneichi, S.; Yamasaki, S.; Ando, S.; Togo, F.; Nishida, A.; Sasaki, T. Effects of School-Based Mental Health Literacy Education for Secondary School Students to Be Delivered by School Teachers: A Preliminary Study. Psychiatry Clin. Neurosci. 2015, 69, 572–579. [Google Scholar] [CrossRef]
- Patalay, P.; Annis, J.; Sharpe, H.; Newman, R.; Main, D.; Ragunathan, T.; Parkes, M.; Clarke, K. A Pre-Post Evaluation of OpenMinds: A Sustainable, Peer-Led Mental Health Literacy Programme in Universities and Secondary Schools. Prev. Sci. 2017, 18, 995–1005. [Google Scholar] [CrossRef] [Green Version]
- Ojio, Y.; Foo, J.C.; Usami, S.; Fuyama, T.; Ashikawa, M.; Ohnuma, K.; Oshima, N.; Ando, S.; Togo, F.; Sasaki, T. Effects of a School Teacher-Led 45-Minute Educational Program for Mental Health Literacy in Pre-Teens. Early Interv. Psychiatry 2019, 13, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Lindow, J.C.; Hughes, J.L.; South, C.; Minhajuddin, A.; Gutierrez, L.; Bannister, E.; Trivedi, M.H.; Byerly, M.J. The Youth Aware of Mental Health Intervention: Impact on Help Seeking, Mental Health Knowledge, and Stigma in U.S. Adolescents. J. Adolesc. Health 2020, 67, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Ojio, Y.; Foo, J.C.; Michigami, E.; Usami, S.; Fuyama, T.; Onuma, K.; Oshima, N.; Ando, S.; Togo, F.; et al. A Quasi-Cluster Randomized Controlled Trial of a Classroom-Based Mental Health Literacy Educational Intervention to Promote Knowledge and Help-Seeking/Helping Behavior in Adolescents. J. Adolesc. 2020, 82, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Ebbinghaus, H. Memory: A Contribution to Experimental Psychology; Teachers College Columbia University: New York, NY, USA, 1913. [Google Scholar]
- Richards, B.A.; Frankland, P.W. The Persistence and Transience of Memory. Neuron 2017, 94, 1071–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansfield, R.; Patalay, P.; Humphrey, N. A Systematic Literature Review of Existing Conceptualisation and Measurement of Mental Health Literacy in Adolescent Research: Current Challenges and Inconsistencies. BMC Public Health 2020, 20, 607. [Google Scholar] [CrossRef]
- Nobre, J.; Oliveira, A.P.; Monteiro, F.; Sequeira, C.; Ferré-Grau, C. Promotion of Mental Health Literacy in Adolescents: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 9500. [Google Scholar] [CrossRef]
- Freţian, A.M.; Graf, P.; Kirchhoff, S.; Glinphratum, G.; Bollweg, T.M.; Sauzet, O.; Bauer, U. The Long-Term Effectiveness of Interventions Addressing Mental Health Literacy and Stigma of Mental Illness in Children and Adolescents: Systematic Review and Meta-Analysis. Int. J. Public Health 2021, 66, 1661. [Google Scholar] [CrossRef] [PubMed]
- Thai, T.T.; Vu, N.L.L.T.; Bui, H.H.T. Mental Health Literacy and Help-Seeking Preferences in High School Students in Ho Chi Minh City, Vietnam. Sch. Ment. Health 2020, 12, 378–387. [Google Scholar] [CrossRef]
- Kutcher, S.; Perkins, K.; Gilberds, H.; Udedi, M.; Ubuguyu, O.; Njau, T.; Chapota, R.; Hashish, M. Creating Evidence-Based Youth Mental Health Policy in Sub-Saharan Africa: A Description of the Integrated Approach to Addressing the Issue of Youth Depression in Malawi and Tanzania. Front. Psychiatry 2019, 10, 542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korhonen, J.; Axelin, A.; Grobler, G.; Lahti, M. Content Validation of Mental Health Literacy Scale (MHLS) for Primary Health Care Workers in South Africa and Zambia—A Heterogeneous Expert Panel Method. Glob. Health Action 2019, 12, 1668215. [Google Scholar] [CrossRef] [PubMed] [Green Version]








| Author (Year) Country | Design | Education Stage | Age | N | Follow-Up | Intervention | Evaluation Tools | Sign |
|---|---|---|---|---|---|---|---|---|
| Perry (2014) [21] Australia | RCT | Secondary | 13–16 years | IG (n = 207) CG (n = 173) | Pre, post, and at 6 months | IG: Headstrong (10 h): Given by teachers at the educational center CG: Usual intervention |
| 1++ |
| Milin (2016) [22] Canada | RCT | Secondary | 16–18 years | IG (n = 362) CG (n = 172) | Pre and post (between 1 and 2 months) | IG: The Guide (6 h): Given by teachers at the educational center CG: Usual intervention |
| 1+ |
| Chisholm (2016) [23] United Kingdom | RCT | Secondary | 12–13 years | IG (n = 354) CG (n = 303) | Pre and post at 2 weeks | IG: School Space (4 h and 45 mins): Given by researchers and teachers at the educational center in contact with a patient; CG: Change contact for mental health record |
| 1++ |
| Campos (2018) [24] Portugal | RCT | Secondary | 12–14 years | IG (n =259) CG (n =284) | Pre, post at 1 week, and 6 months | IG: Finding Space (3 h): Given by expert psychologist and student of Psychology Master’s Degree; CG: Usual intervention |
| 1+ |
| Pinto-Foltz (2019) [25] United States | RCT | Secondary | 13–17 years | IG (n = 95) CG (n = 61) | Pre, post, at 1 and 2 months | IG: In Our Own Voice (1 h): Given by individuals with mental health problems (older than 18 years); CG: No intervention |
| 1− |
| Casañas (2021) [26] Spain | RCT | Secondary | 13–15 years | IG (n = 295) CG (n = 251) | Pre, post, at 6 and 12 months | IG: EspaiJove.net Program (7 h): Given by mental health nurses CG: No intervention |
| 1++ |
| Skre (2013) [27] Norway | QE | Secondary | 13–16 years | IG (n = 520) CG (n = 550) | Pre and post at 2 months | IG: Mental health for everyone (3 days): Given by teachers at the educational center; CG: Usual intervention |
| 2++ |
| Bella-Awusah (2014) [28] Nigeria | QE | Secondary | 10–18 years | IG (n = 78) CG (n = 76) | Pre, post, and at 6 months | Dogra 2005 Adaptation Program (3 h): Given by researchers CG: Usual intervention |
| 2+ |
| Mcluckie (2014) [29] Canada | QE without CG | Secondary | 14–15 years | n = 265 | Pre, post, and at 2 months | The Guide (10–12 h): Given by teachers at the educational center |
| 2++ |
| Kutcher (2015) [30] Canada | QE without CG | Secondary | 14–15 years | n = 175 | Pre, post, and at 2 months | The Guide (10–12 h): Given by teachers at the educational center |
| 2+ |
| Ojio(2015) [31] Japan | QE without CG | Secondary | 14–15 years | n = 118 | Pre, post, and at 3 months | The Short MHL Program for Teens (1 h and 40 min): Given by teachers at the educational center |
| 2++ |
| Patalay (2017) [32] United Kingdom | QE without CG | Secondary | 13–15 years | n = 234 | Pre and post | Open Minds (1 h and 40 min): Given by medical students |
| 2++ |
| Ojio (2019) [33] Japan | QE without CG | Primary | 10–12 years | n = 662 | Pre, post, and at 3 months | The Short MHL Program for Pre-Teens (45 min): Given by teachers at the educational center |
| 2+ |
| Lindow (2020) [34] United States | QE without CG | Secondary | 12–18 years | n = 436 | Pre and post at 3 months | Youth Aware of Mental Health (4 h and 10 min: Given by personnel trained by researchers at the educational center |
| 2+ |
| Yamaguchi (2020) [35] Japan | QE | Secondary | 15–16 years | IG (n = 364) CG (n = 611) | Pre, post, and at 2 months | IG: Short MHL Program (SMHLP) (50 min): Given by teachers at the educational center CG: Usual intervention |
| 2++ |
| StMeanDiff | Coef. | Std. Err. | t | P > |t| | [95% Conf. Interval] |
|---|---|---|---|---|---|
| Length | −0.031 | 0.040 | −0.78 | 0.450 | −0.118; 0.056 |
| Cons | 0.691 | 0.213 | 3.24 | 0.007 | 0.226; 1.155 |
| REML estimate of between-study variance | Number of obs = 14 | ||||
| % residual variation due to heterogeneity | Tau2 = 0.2005 | ||||
| Proportion of between-study variance explained | I-squared res = 95.15% | ||||
| With Knapp-Hartung modification | Adj R-squared = −2.42% | ||||
| StMeanDiff | Coef. | Std. Err. | t | P > |t| | [95% Conf. Interval] |
|---|---|---|---|---|---|
| Length | −0.007 | 0.048 | −0.14 | 0.890 | −0.118; 0.104 |
| Cons | 0.118 | 0.298 | 0.39 | 0.704 | −0.571; 0.806 |
| REML estimate of between-study variance | Number of obs = 10 | ||||
| % residual variation due to heterogeneity | Tau2 = 0.1778 | ||||
| Proportion of between-study variance explained | I-squared res = 94.43% | ||||
| With Knapp-Hartung modification | Adj R-squared = −12.22% | ||||
| StMeanDiff | Coef. | Std. Err. | t | P > |t| | [95% Conf. Interval] |
|---|---|---|---|---|---|
| Length | −0.033 | 0.033 | −1.00 | 0.392 | −0.138; 0.072 |
| Cons | 0.325 | 0.221 | 1.46 | 0.239 | −0.381; 1.03 |
| REML estimate of between-study variance | Number of obs = 5 | ||||
| % residual variation due to heterogeneity | Tau2 = 0.0426 | ||||
| Proportion of between-study variance explained | I-squared res =82.93% | ||||
| With Knapp-Hartung modification | Adj R-squared = 0.61% | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amado-Rodríguez, I.D.; Casañas, R.; Mas-Expósito, L.; Castellví, P.; Roldan-Merino, J.F.; Casas, I.; Lalucat-Jo, L.; Fernández-San Martín, M.I. Effectiveness of Mental Health Literacy Programs in Primary and Secondary Schools: A Systematic Review with Meta-Analysis. Children 2022, 9, 480. https://doi.org/10.3390/children9040480
Amado-Rodríguez ID, Casañas R, Mas-Expósito L, Castellví P, Roldan-Merino JF, Casas I, Lalucat-Jo L, Fernández-San Martín MI. Effectiveness of Mental Health Literacy Programs in Primary and Secondary Schools: A Systematic Review with Meta-Analysis. Children. 2022; 9(4):480. https://doi.org/10.3390/children9040480
Chicago/Turabian StyleAmado-Rodríguez, Isaac Daniel, Rocio Casañas, Laia Mas-Expósito, Pere Castellví, Juan Francisco Roldan-Merino, Irma Casas, Lluís Lalucat-Jo, and Mª Isabel Fernández-San Martín. 2022. "Effectiveness of Mental Health Literacy Programs in Primary and Secondary Schools: A Systematic Review with Meta-Analysis" Children 9, no. 4: 480. https://doi.org/10.3390/children9040480
APA StyleAmado-Rodríguez, I. D., Casañas, R., Mas-Expósito, L., Castellví, P., Roldan-Merino, J. F., Casas, I., Lalucat-Jo, L., & Fernández-San Martín, M. I. (2022). Effectiveness of Mental Health Literacy Programs in Primary and Secondary Schools: A Systematic Review with Meta-Analysis. Children, 9(4), 480. https://doi.org/10.3390/children9040480