
Management of Sporadic Vestibular Schwannomas in Children—Volumetric Analysis and Clinical Outcome Assessment

Abstract
:1. Introduction
2. Materials and Methods
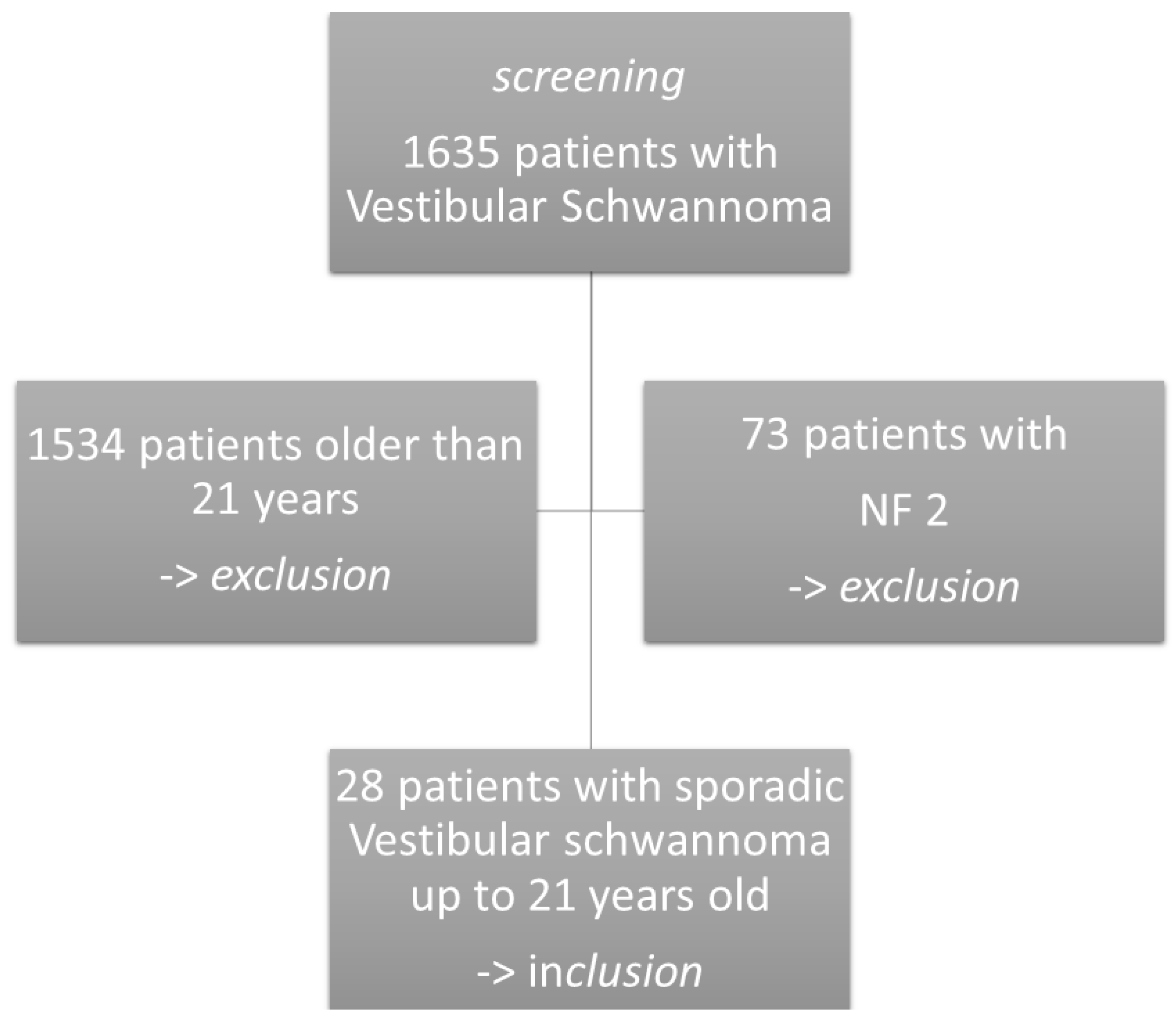
2.1. Inclusion
2.2. Analysis
2.3. Testing for NF2
2.4. Tumor Volumetry
2.5. Statistical Analysis
3. Results
3.1. Pre- and Post-operative Assessment
3.1.1. Symptomatology and Tumor Size
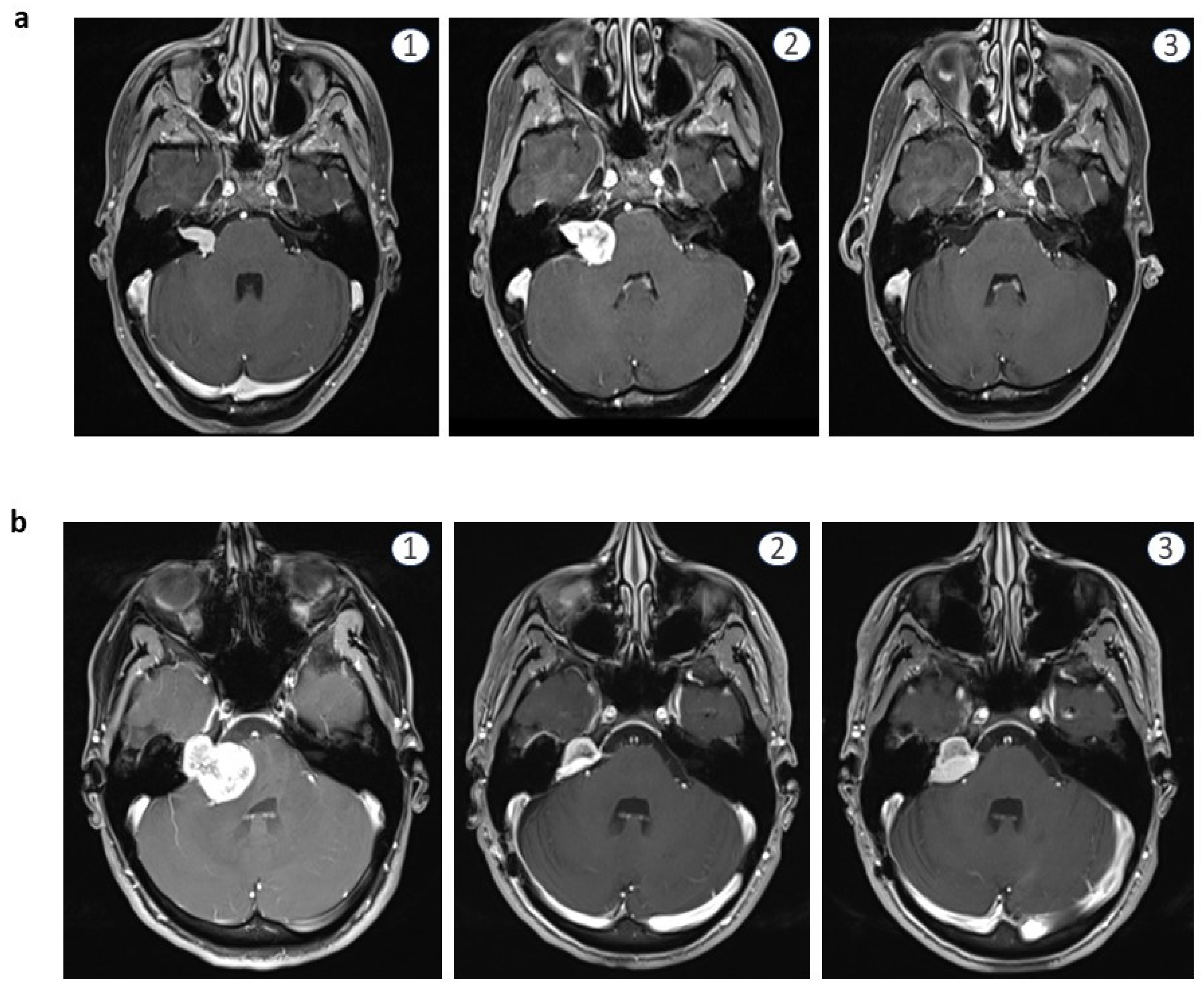
3.1.2. Growth Rate and Imaging
3.1.3. Hearing
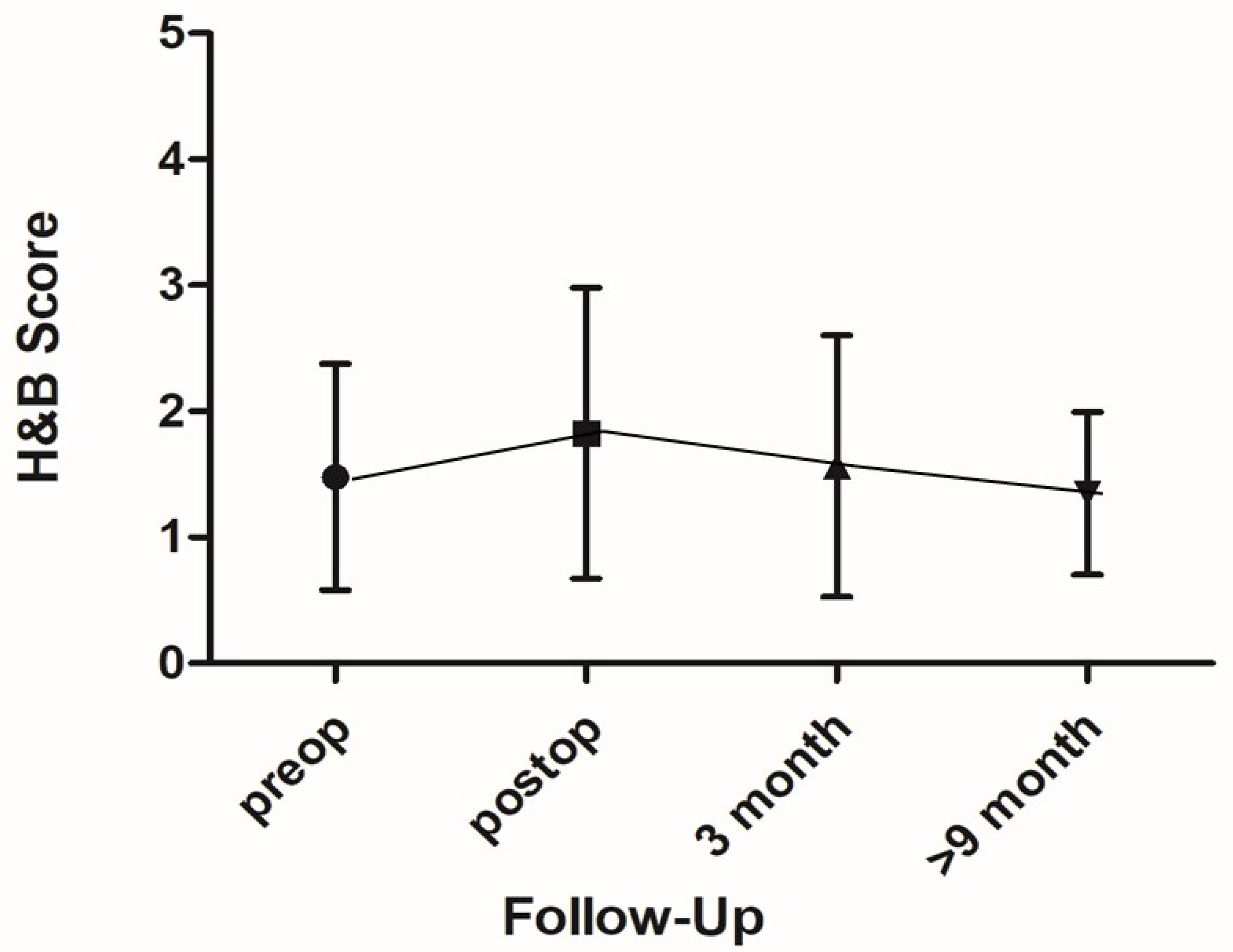
3.1.4. Facial Nerve
3.1.5. Other Cranial Nerves
3.2. Non-Operative Cases
3.3. Grade of Surgery and Effects on Tumor Growth
3.3.1. Gross Total Resection (GTR)
3.3.2. Subtotal Resection (STR)
3.3.3. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, E.P.; Crane, B.T. The management and imaging of vestibular schwannomas. AJNR Am. J. Neuroradiol. 2017, 38, 2034–2043. [Google Scholar] [CrossRef]
- Mazzoni, A.; Dubey, S.P.; Poletti, A.M.; Colombo, G. Sporadic acoustic neuroma in pediatric patients. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 1569–1572. [Google Scholar] [CrossRef]
- Holman, M.A.; Schmitt, W.R.; Carlson, M.L. Pediatric cerebellopontine angle and internal auditory canal tumors: Clinical article. J. Neurosurg. Pediatr. 2013, 12, 317–324. [Google Scholar] [CrossRef]
- Rosahl, S.; Esser, D. Surgical indications and complications management in vestibular schwannoma. HNO 2017, 65, 388–394. [Google Scholar] [CrossRef]
- Cunningham, C.D., 3rd; Friedman, R.A.; Brackmann, D.E.; Hitselberger, W.E.; Lin, H.W. Neurotologic skull base surgery in pediatric patients. Otol. Neurotol. 2005, 26, 231–236. [Google Scholar] [CrossRef]
- Gugel, I.; Grimm, F.; Teuber, C.; Zipfel, J.; Tatagiba, M.; Mautner, V.F.; Schuhmann, M.U.; Kluwe, L. Presenting symptoms in children with neurofibromatosis type 2. Childs Nerv. Syst. 2020, 10, 2463–2470. [Google Scholar] [CrossRef]
- Gugel, I.; Grimm, F.; Zipfel, J.; Teuber, C.; Ernemann, U.; Kluwe, L.; Tatagiba, M.; Mautner, V.F.; Schuhmann, M.U. Age at onset and presenting symptoms of neurofibromatosis type 2 as prognostic factors for clinical course of vestibular schwannomas. Cancers 2020, 12, 2355. [Google Scholar] [CrossRef]
- Wang, J.; Xu, Y.; Lei, T.; Zeng, L. Treatment decision-making for sporadic small vestibular schwannoma in a pediatric patient: A case report and literature review. Oncol. Lett. 2015, 9, 2371–2373. [Google Scholar] [CrossRef] [Green Version]
- Truy, E.; Furminieux, V.; Dubreuil, C. Acoustic neuroma in children. Report of 5 cases. Ann. Otolaryngol. Chir. Cervicofac. 1999, 116, 92–97. [Google Scholar]
- Allcutt, D.A.; Hoffman, H.J.; Isla, A.; Becker, L.E.; Humphreys, R.P. Acoustic schwannomas in children. Neurosurgery 1991, 29, 14–18. [Google Scholar] [CrossRef]
- Walcott, B.P.; Sivarajan, G.; Bashinskaya, B.; Anderson, D.E.; Leonetti, J.P.; Origitano, T.C. Sporadic unilateral vestibular schwannoma in the pediatric population. Clinical article. J. Neurosurg. Pediatr. 2009, 4, 125–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pothula, V.B.; Lesser, T.; Mallucci, C.; May, P.; Foy, P. Vestibular schwannomas in children. Otol. Neurotol. 2001, 22, 903–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harun, A.; Agrawal, Y.; Tan, M.; Niparko, J.K.; Francis, H.W. Sex and age associations with vestibular schwannoma size and presenting symptoms. Otol. Neurotol. 2012, 33, 1604–1610. [Google Scholar] [CrossRef]
- Yin, L.; Ma, Z.; Li, C.; Luo, S. Unilateral vestibular schwannomas in childhood without evidence of neurofibromatosis: Experience of 10 patients at a single institute. Turk. Neurosurg. 2017, 27, 333–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özek, M.M.; Cinalli, G.; Maixner, W.J.; Sainte-Rose, C. Posterior Fossa Tumors in Children; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Chen, H.; Zhang, X.; Zhang, Z.; Yang, T.; Wang, Z.; Wu, H. The role of NF2 gene mutations and pathogenesis-related proteins in sporadic vestibular schwannomas in young individuals. Mol. Cell Biochem. 2014, 392, 145–152. [Google Scholar] [CrossRef]
- Evans, D.G. Neurofibromatosis 2. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Stephens, K., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Malina, G.E.K.; Heiferman, D.M.; Riedy, L.N.; Szujewski, C.C.; Rezaii, E.G.; Leonetti, J.P.; Anderson, D.E. Pediatric vestibular schwannomas: Case series and a systematic review with meta-analysis. J. Neurosurg. Pediatr. 2020, 26, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Gugel, I.; Grimm, F.; Teuber, C.; Kluwe, L.; Mautner, V.F.; Tatagiba, M.; Schuhmann, M.U. Management of NF2-associated vestibular schwannomas in children and young adults: Influence of surgery and clinical factors on tumor volume and growth rate. J. Neurosurg. Pediatr. 2019, 24, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Teppo, H.; Heikkinen, J.; Laitakari, K.; Alho, O.P. Diagnostic delays in vestibular schwannoma. J. Laryngol. Otol. 2009, 123, 289–293. [Google Scholar] [CrossRef]
- Kapitanov, D.N.; Shimansky, V.N.; Kolycheva, M.V.; Shevchenko, K.V.; Lebedeva, M.A.; Chernikova, N.A.; Shelesko, E.V. The causes of late diagnostics of vestibular shwannomas. Vestn. Otorinolaringol. 2019, 84, 36–41. [Google Scholar] [CrossRef]
- Régis, J.; Carron, R.; Delsanti, C.; Porcheron, D.; Thomassin, J.M.; Murracciole, X.; Roche, P.H. Radiosurgery for vestibular schwannomas. Neurosurg. Clin. N. Am. 2013, 24, 521–530. [Google Scholar] [CrossRef]
- Varughese, J.K.; Breivik, C.N.; Wentzel-Larsen, T.; Lund-Johansen, M. Growth of untreated vestibular schwannoma: A prospective study. J. Neurosurg. 2012, 116, 706–712. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Song, G.; Wang, X.; Li, M.; Chen, G.; Guo, H.; Bao, Y.; Liang, J. Comparison of surgical outcomes in cystic and solid vestibular schwannomas: A systematic review and meta-analysis. Neurosurg. Rev. 2021, 44, 1889–1902. [Google Scholar] [CrossRef]
- Park, H.H.; Park, S.H.; Oh, H.C.; Jung, H.H.; Chang, J.H.; Lee, K.S.; Chang, W.S.; Hong, C.K. The behavior of residual tumors following incomplete surgical resection for vestibular schwannomas. Sci. Rep. 2021, 11, 4665. [Google Scholar] [CrossRef]
- Falcioni, M.; Romano, G.; Aggarwal, N.; Sanna, M. Cerebrospinal fluid leak after retrosigmoid excision of vestibular schwannomas. Otol. Neurotol. 2008, 29, 384–386. [Google Scholar] [CrossRef]
- Huang, X.; Xu, M.; Xu, J.; Zhou, L.; Zhong, P.; Chen, M.; Ji, K.; Chen, H.; Mao, Y. Complications and Management of Large Intracranial Vestibular Schwannomas Via the Retrosigmoid Approach. World Neurosurg. 2017, 99, 326–335. [Google Scholar] [CrossRef]
- Janz, T.A.; Camilon, P.R.; Cheung, A.Y.; Nguyen, S.A.; Meyer, T.A.; McRackan, T.R.; Lambert, P.R. Characteristics and outcomes of pediatric vestibular schwannomas. Otol. Neurotol. 2019, 40, 1047–1053. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| # | Sex | Age | Tumor Size (Hannover) | Growth (cm3 and %) | Bone Erosion | Cystic Tumor | GR | H&B | GTR/STR | Growth (cm3) | Growth in %/Month (postp) | GR | H&B | Recurrence (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| preoperative | postoperative | |||||||||||||
| 1 | f | 15 | T2 | - | - | 2 | 1 | GTR | 3 | 1 | ||||
| 2 | f | 17 | T4a | - | - | 4 | 1 | GTR | 4 | 1 | ||||
| 3 | m | 16 | T2 | - | - | 3 | 1 | GTR | 3 | 1 | ||||
| 4 | f | 18 | T2 | 0.207 (54.9%) | - | - | 3 | 0 | GTR | 3 | 1 | |||
| 5 | m | 13 | T4b | 1.02 (17%) | yes | - | 4 | 3 | STR | 0.312 | 0.013 (4.81%) | 4 | 3 | 24 |
| 6 | f | 15 | T4b | yes | - | 3 | 3 | STR | 1.344 | 0.112 (5.35%) | 3 | 3 | 12 | |
| 7 | m | 6 | T4a | - | yes | 4 | 4 | GTR | 4 | 4 | ||||
| 8 | f | 16 | T4a | yes | yes | 4 | 3 | GTR | 4 | 3 | ||||
| 9 | f | 17 | T4a | - | - | 1 | 2 | STR | 0.08 | 0.003 (1.15%) | 1 | 2 | 24 | |
| 10 | m | 16 | T2 | - | - | 2 | 1 | GTR | 2 | 1 | ||||
| 11 | f | 11 | T3a | - | - | 1 | 1 | STR | 0.005 | 0.002 (0.55%) | 4 | 24 | ||
| 12 | m | 20 | t3a | - | - | 1 | 1 | GTR | 1 | 1 | ||||
| 13 | m | 18 | T2 | - | - | 3 | 1 | GTR | 4 | 1 | ||||
| 14 | f | 16 | T1 | - | - | 1 | 1 | GTR | 2 | 1 | ||||
| 15 | f | 15 | T4a | - | yes | 3 | 2 | STR | 0.053 | 0.004 (3.0%) | 4 | 3 | 12 | |
| 16 | f | 14 | T2 | - | - | 3 | 1 | no surgery | ||||||
| 17 | f | 13 | T1 | - | - | 2 | 1 | no surgery | ||||||
| 18 | m | 15 | T1 | 0.672 (364.8%) | - | - | 1 | 1 | no surgery | |||||
| 19 | f | 15 | T3b | 1.82 (1260%) | - | - | 1 | 1 | no no surgery | |||||
| 20 | f | 19 | T3a | 2.6 (325%) | - | - | 3 | 1 | GTR | 4 | ||||
| 21 | m | 20 | T3a | 1.1 (70%) | - | - | 1 | 1 | GTR | 5 | 2 | |||
| 22 | m | 19 | T3a | - | - | 3 | 1 | GTR | 4 | 1 | ||||
| 23 | f | 12 | T1 | 0.189 (84%) | - | - | 3 | 1 | GTR | 3 | 1 | |||
| 24 | f | 16 | T1 | 0.204 (96%) | - | - | 1 | 1 | GTR | 1 | 1 | |||
| 25 | m | 19 | T3a | - | - | 3 | 1 | GTR | 4 | 1 | ||||
| 26 | m | 15 | T2 | - | - | 2 | 1 | no surgery | ||||||
| 27 | f | 21 | T2 | - | - | 3 | 1 | GTR | 3 | 1 | ||||
| 28 | f | 21 | T2 | - | yes | 2 | 1 | GTR | 5 | 1 | ||||
| Preoperative | Postoperative | |||||
|---|---|---|---|---|---|---|
| # | GR | H&B | Growth Rate cm3/Month and %/Month | GR | H&B | Growth Rate cm3/Month and %/Month |
| 1 | 2 | 1 | na | 3 | 1 | - |
| 2 | 4 | 1 | na | 4 | 1 | - |
| 3 | 3 | 1 | na | 3 | 1 | - |
| 4 | 3 | 1 | 0.023 (6.1%) | 3 | 1 | - |
| 5 | 4 | 3 | 0.06 (1%) | 4 | 3 | 0.013 (4.81%) |
| 6 | 3 | 3 | na | 3 | 3 | 0.112 (5.35%) |
| 7 | 4 | 4 | na | 4 | 4 | - |
| 8 | 4 | 3 | na | 4 | 3 | - |
| 9 | 1 | 2 | na | 1 | 2 | 0.003 (1.15%) |
| 10 | 2 | 1 | na | 2 | 1 | - |
| 11 | 1 | 1 | na | na | 4 | 0.002 (0.55%) |
| 12 | 1 | 1 | na | 1 | 1 | - |
| 13 | 3 | 1 | na | 4 | 1 | - |
| 14 | 1 | 1 | na | 2 | 1 | - |
| 15 | 3 | 2 | na | 4 | 3 | 0.004 (3.0%) |
| 20 | 3 | 1 | 0.1 (12.5%) | na | 4 | - |
| 21 | 1 | 1 | 0.22 (14.0%) | 5 | 2 | - |
| 22 | 3 | 1 | na | 4 | 1 | - |
| 23 | 3 | 1 | 0.009 (4.0%) | 3 | 1 | - |
| 24 | 1 | 1 | 0.017 (8.0%) | 1 | 1 | - |
| 25 | 3 | 1 | na | 4 | 1 | - |
| 27 | 3 | 1 | na | 3 | 1 | - |
| 28 | 2 | 1 | na | 5 | 1 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zipfel, J.; Gorbachuk, M.; Gugel, I.; Tatagiba, M.; Schuhmann, M.U. Management of Sporadic Vestibular Schwannomas in Children—Volumetric Analysis and Clinical Outcome Assessment. Children 2022, 9, 490. https://doi.org/10.3390/children9040490
Zipfel J, Gorbachuk M, Gugel I, Tatagiba M, Schuhmann MU. Management of Sporadic Vestibular Schwannomas in Children—Volumetric Analysis and Clinical Outcome Assessment. Children. 2022; 9(4):490. https://doi.org/10.3390/children9040490
Chicago/Turabian StyleZipfel, Julian, Mykola Gorbachuk, Isabel Gugel, Marcos Tatagiba, and Martin U. Schuhmann. 2022. "Management of Sporadic Vestibular Schwannomas in Children—Volumetric Analysis and Clinical Outcome Assessment" Children 9, no. 4: 490. https://doi.org/10.3390/children9040490
APA StyleZipfel, J., Gorbachuk, M., Gugel, I., Tatagiba, M., & Schuhmann, M. U. (2022). Management of Sporadic Vestibular Schwannomas in Children—Volumetric Analysis and Clinical Outcome Assessment. Children, 9(4), 490. https://doi.org/10.3390/children9040490