
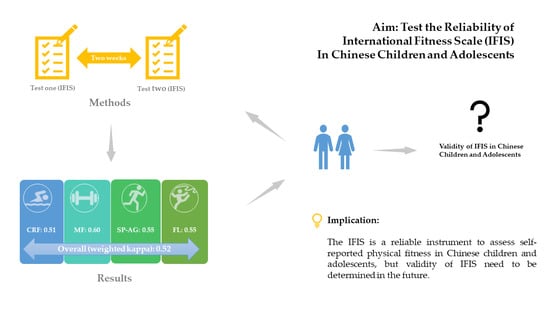
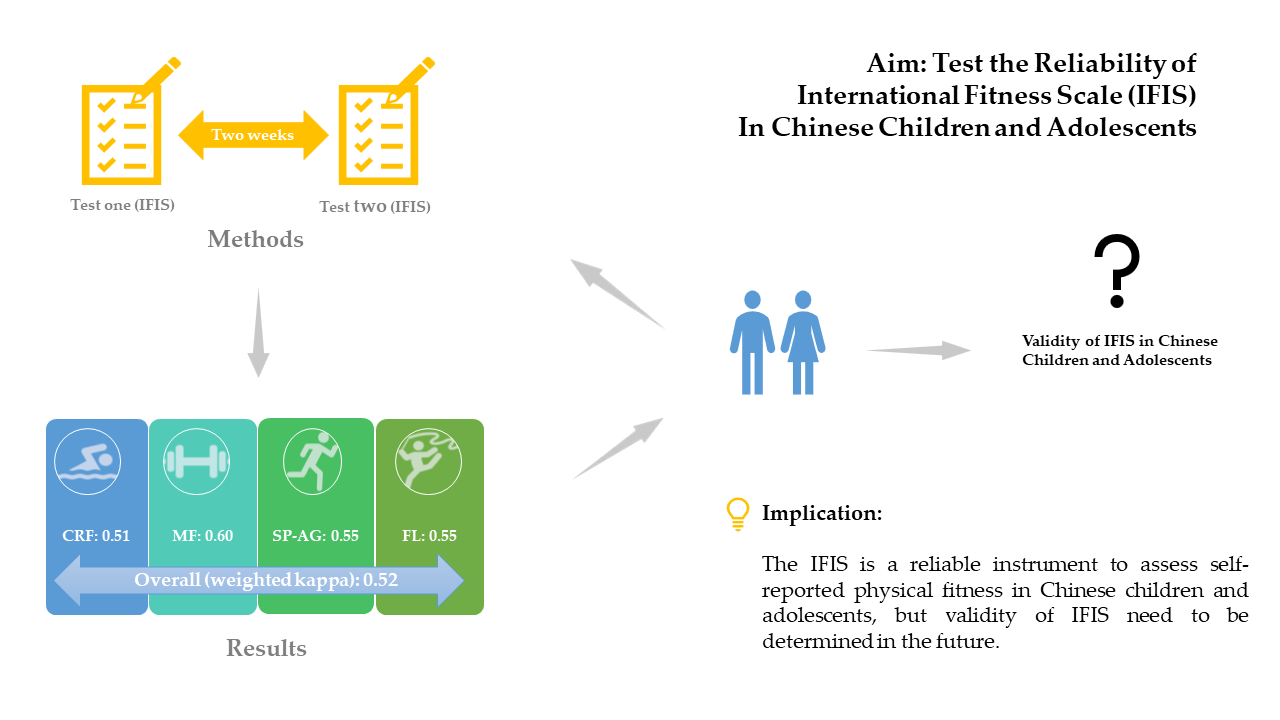
Reliability of International Fitness Scale (IFIS) in Chinese Children and Adolescents

 , , ,
, , ,  , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants and Sampling
2.2. Measures
2.2.1. Demographics
2.2.2. Self-Reported Fitness
2.2.3. Data Collection
2.2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Ortega, F.B.; Artero, E.G.; Ruiz, J.R.; España-Romero, V.; Jiménez-Pavón, D.; Vicente-Rodríguez, G.; Moreno, L.A.; Manios, Y.; Beghin, L.; Ottevaere, C. Physical fitness levels among European adolescents: The HELENA study. Br. J. Sports Med. 2011, 45, 20–29. [Google Scholar] [CrossRef] [Green Version]
- De Moraes, A.C.F.; Vilanova-Campelo, R.C.; Torres-Leal, F.L.; Carvalho, H.B. Is self-reported physical fitness useful for estimating fitness levels in children and adolescents? A reliability and validity study. Medicina 2019, 55, 286. [Google Scholar] [CrossRef] [Green Version]
- Fogelholm, M. Physical Activity, Fitness and Fatness: Relations to Mortality, Morbidity and Disease Risk Factors. A Systematic Review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2009, 11, 202–221. [Google Scholar] [CrossRef]
- Carnethon, M.R. Prevalence and Cardiovascular Disease Correlates of Low Cardiorespiratory Fitness in Adolescents and Adults. JAMA 2005, 294, 2981. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef] [Green Version]
- LaVigne, T.; Hoza, B.; Smith, A.L.; Shoulberg, E.K.; Bukowski, W. Associations Between Physical Fitness and Children’s Psychological Well-Being. J. Clin. Sport Psychol. 2016, 10, 32–47. [Google Scholar] [CrossRef]
- Alvarez-Bueno, C.; Pesce, C.; Cavero-Redondo, I.; Sánchez-López, M.; Martínez-Hortelano, J.; Martinez Vizcaino, V. The Effect of Physical Exercise Activity Interventions on Children’s Cognition and Metacognition: A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 729–738. [Google Scholar] [CrossRef]
- Santana, C.C.A.; Azevedo, L.B.; Cattuzzo, M.T.; Hill, J.O.; Andrade, L.P.; Prado, W.L. Physical fitness and academic performance in youth: A systematic review. Scand. J. Med. Sci. Sports 2017, 27, 579–603. [Google Scholar] [CrossRef] [Green Version]
- Lavie, C.J.; Milani, R.V.; O’Keefe, J.H.; Lavie, T.J. Impact of Exercise Training on Psychological Risk Factors. Prog. Cardiovasc. Dis. 2011, 53, 464–470. [Google Scholar] [CrossRef]
- Bianco, A.; Jemni, M.; Thomas, E.; Patti, A.; Paoli, A.; Ramos Roque, J.; Palma, A.; Mammina, C.; Tabacchi, G. A systematic review to determine reliability and usefulness of the field-based test batteries for the assessment of physical fitness in adolescents—The ASSO Project. Int. J. Occup. Med. Environ. Health 2015, 28, 445–478. [Google Scholar] [CrossRef] [Green Version]
- Marques, A.; Henriques-Neto, D.; Peralta, M.; Martins, J.; Gomes, F.; Popovic, S.; Masanovic, B.; Demetriou, Y.; Schlund, A.; Ihle, A. Field-Based Health-Related Physical Fitness Tests in Children and Adolescents: A Systematic Review. Front. Pediatrics 2021, 9, 155. [Google Scholar] [CrossRef]
- Kolimechkov, S. Physical fitness assessment in children and adolescents: A systematic review. Eur. J. Phys. Educ. Sport Sci. 2017, 3, 65–79. [Google Scholar] [CrossRef]
- Fox, K.R.; Corbin, C.B. The physical self-perception profile: Devlopment and preliminary validation. J. Sport Exerc. Psychol. 1989, 11, 408–430. [Google Scholar] [CrossRef]
- Keith, N.R.; Clark, D.O.; Stump, T.E.; Miller, D.K.; Callahan, C.M. Validity and Reliability of the Self-Reported Physical Fitness (SRFit) Survey. J. Phys. Act. Health 2014, 11, 853–859. [Google Scholar] [CrossRef] [Green Version]
- Merellano-Navarro, E.; Collado-Mateo, D.; García-Rubio, J.; Gusi, N.; Olivares, P.R. Validity of the International Fitness Scale “IFIS” in older adults. Exp. Gerontol. 2017, 95, 77–81. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Espana-Romero, V.; Vicente-Rodriguez, G.; Martínez-Gómez, D.; Manios, Y.; Béghin, L.; Molnar, D.; Widhalm, K.; Moreno, L.A. The International Fitness Scale (IFIS): Usefulness of self-reported fitness in youth. Int. J. Epidemiol. 2011, 40, 701–711. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Vélez, R.; Cruz-Salazar, S.M.; Martínez, M.; Cadore, E.L.; Alonso-Martinez, A.M.; Correa-Bautista, J.E.; Izquierdo, M.; Ortega, F.B.; García-Hermoso, A. Construct validity and test–retest reliability of the International Fitness Scale (IFIS) in Colombian children and adolescents aged 9–17.9 years: The FUPRECOL study. PeerJ 2017, 5, e3351. [Google Scholar] [CrossRef]
- Sánchez-López, M.; Martínez-Vizcaíno, V.; García-Hermoso, A.; Jiménez-Pavón, D.; Ortega, F. Construct validity and test–retest reliability of the International Fitness Scale (IFIS) in spanish children aged 9–12 years. Scand. J. Med. Sci. Sports 2015, 25, 543–551. [Google Scholar] [CrossRef]
- Sánchez-Toledo, P.R.O.; Rubio, J.G.; Merellano-Navarro, E. Propiedades psicométricas de la escala “International Fitness Scale” en adolescentes chilenos. In Retos: Nuevas Tendencias en Educación Física, Deporte y Recreación; Federación Española de Docentes de Educación Física (FEADEF): Valladolid, Spain, 2017; pp. 23–27. [Google Scholar]
- Ortega, F.; Sanchez-Lopez, M.; Solera-Martinez, M.; Fernandez-Sanchez, A.; Sjöström, M.; Martinez-Vizcaino, V. Self-reported and measured cardiorespiratory fitness similarly predict cardiovascular disease risk in young adults. Scand. J. Med. Sci. Sports 2013, 23, 749–757. [Google Scholar] [CrossRef]
- Español-Moya, M.N.; Ramirez-Velez, R. Psychometric validation of the International Fitness Scale (IFIS) in Colombian youth. Rev. Esp. Salud Publica 2014, 88, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Romero-Gallardo, L.; Soriano-Maldonado, A.; Ocón-Hernández, O.; Acosta-Manzano, P.; Coll-Risco, I.; Borges-Cosic, M.; Ortega, F.B.; Aparicio, V.A. International Fitness Scale—IFIS: Validity and association with health-related quality of life in pregnant women. Scand. J. Med. Sci. Sports 2020, 30, 505–514. [Google Scholar] [CrossRef]
- Álvarez-Gallardo, I.C.; Soriano-Maldonado, A.; Segura-Jiménez, V.; Carbonell-Baeza, A.; Estévez-López, F.; McVeigh, J.G.; Delgado-Fernández, M.; Ortega, F.B. International FItness Scale (IFIS): Construct validity and reliability in women with fibromyalgia: The al-Ándalus Project. Arch. Phys. Med. Rehabil. 2016, 97, 395–404. [Google Scholar] [CrossRef]
- Zhu, Z.; Yang, Y.; Kong, Z.; Zhang, Y.; Zhuang, J. Prevalence of physical fitness in Chinese school-aged children: Findings from the 2016 Physical Activity and Fitness in China—The Youth Study. J. Sport Health Sci. 2017, 6, 395–403. [Google Scholar] [CrossRef]
- Chen, X.; Cui, J.; Zhang, Y.; Peng, W. The association between BMI and health-related physical fitness among Chinese college students: A cross-sectional study. BMC Public Health 2020, 20, 444. [Google Scholar] [CrossRef]
- Wang, J. The association between physical fitness and physical activity among Chinese college students. J. Am. Coll. Health 2019, 67, 602–609. [Google Scholar] [CrossRef]
- Dong, Y.; Lau, P.W.C.; Dong, B.; Zou, Z.; Yang, Y.; Wen, B.; Ma, Y.; Hu, P.; Song, Y.; Ma, J. Trends in physical fitness, growth, and nutritional status of Chinese children and adolescents: A retrospective analysis of 1.5 million students from six successive national surveys between 1985 and 2014. Lancet Child Adolesc. Health 2019, 3, 871–880. [Google Scholar] [CrossRef]
- Liu, Y. Promoting physical activity among Chinese youth: No time to wait. J. Sport Health Sci. 2017, 6, 248–249. [Google Scholar] [CrossRef]
- Lu, C.; Stolk, R.P.; Sauer, P.J.J.; Sijtsma, A.; Wiersma, R.; Huang, G.; Corpeleijn, E. Factors of physical activity among Chinese children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 36. [Google Scholar] [CrossRef] [Green Version]
- Beaton, D.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Recommendations for the cross-cultural adaptation of health status measures. N. Y. Am. Acad. Orthop. Surg. 2002, 12, 1–9. [Google Scholar]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Cary, NC, USA, 2015. [Google Scholar]
- Mokkink, L.B.; Prinsen, C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; de Vet, H.; Terwee, C.B.; Mokkink, L. COSMIN methodology for systematic reviews of patient-reported outcome measures (PROMs). User Man. 2018, 78, 1. [Google Scholar]
- Cohen, J. Weighted kappa: Nominal scale agreement provision for scaled disagreement or partial credit. Psychol. Bull. 1968, 70, 213. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.; Anderson, R.; Babin, B.; Black, W. Multivariate Data Analysis: A Global Perspective; Pearson Upper Saddle River: Hoboken, NJ, USA, 2010. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Babic, M.J.; Morgan, P.J.; Plotnikoff, R.C.; Lonsdale, C.; White, R.L.; Lubans, D.R. Physical Activity and Physical Self-Concept in Youth: Systematic Review and Meta-Analysis. Sports Med. 2014, 44, 1589–1601. [Google Scholar] [CrossRef]
- Mota, J.; Guerra, S.; Leandro, C.; Teixeira-Pinto, A.; Ribeiro, J.; Duarte, J. Association of maturation, sex, and body fat in cardiorespiratory fitness. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2002, 14, 707–712. [Google Scholar] [CrossRef]
- Marta, C.C.; Marinho, D.A.; Barbosa, T.M.; Izquierdo, M.; Marques, M.C. Physical fitness differences between prepubescent boys and girls. J. Strength Cond. Res. 2012, 26, 1756–1766. [Google Scholar] [CrossRef]
- Rowland, T.W. Evolution of maximal oxygen uptake in children. Pediatric Fit. 2007, 50, 200–209. [Google Scholar]
- Gao, Z.; Lee, A.; Solmon, M.; Zhang, T. Changes in Middle School Students’ Motivation Toward Physical Education Over One School Year. J. Teach. Phys. Educ. 2009, 28, 378–399. [Google Scholar] [CrossRef]
- Cattuzzo, M.T.; dos Santos Henrique, R.; Ré, A.H.N.; de Oliveira, I.S.; Melo, B.M.; de Sousa Moura, M.; de Araújo, R.C.; Stodden, D. Motor competence and health related physical fitness in youth: A systematic review. J. Sci. Med. Sport 2016, 19, 123–129. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Test One, Mean (SD) | Test Two, Mean (SD) | Weighted Kappa | Std. Errs. | |
|---|---|---|---|---|
| Overall | 3.97 ± 0.88 | 3.95 ± 0.92 | 0.52 | 0.02 |
| CRF | 3.64 ± 0.94 | 3.71 ± 0.93 | 0.51 | 0.02 |
| MF | 3.66 ± 0.93 | 3.67 ± 0.95 | 0.60 | 0.02 |
| SP–AG | 3.79 ± 0.93 | 3.84 ± 0.91 | 0.55 | 0.02 |
| FL | 3.35 ± 1.10 | 3.40 ± 1.09 | 0.55 | 0.02 |
| Test One, Mean (SD) | Test Two, Mean (SD) | Weighted Kappa | Std. Errs. | ||
|---|---|---|---|---|---|
| Boys | overall | 4.11 ± 0.82 | 4.07 ± 0.91 | 0.48 | 0.03 |
| CRF | 3.76 ± 0.96 | 3.84 ± 0.95 | 0.51 | 0.03 | |
| MF | 3.78 ± 0.96 | 3.81 ± 0.99 | 0.58 | 0.03 | |
| SP–AG | 3.95 ± 0.96 | 3.96 ± 0.95 | 0.55 | 0.03 | |
| FL | 3.23 ± 1.10 | 3.26 ± 1.12 | 0.51 | 0.03 | |
| Girls | overall | 3.82 ± 0.90 | 3.81 ± 0.93 | 0.54 | 0.03 |
| CRF | 3.51 ± 0.91 | 3.56 ± 0.89 | 0.49 | 0.03 | |
| MF | 3.52 ± 0.88 | 3.51 ± 0.87 | 0.60 | 0.03 | |
| SP–AG | 3.62 ± 0.86 | 3.70 ± 0.84 | 0.53 | 0.03 | |
| FL | 3.47 ± 1.08 | 3.57 ± 1.04 | 0.60 | 0.03 |
| Test One, Mean (SD) | Test Two, Mean (SD) | Weighted Kappa | Std. Errs. | ||
|---|---|---|---|---|---|
| Children (n = 390) | overall | 4.08 ± 0.86 | 4.11 ± 0.90 | 0.61 | 0.04 |
| CRF | 3.73 ± 0.95 | 3.84 ± 0.93 | 0.61 | 0.03 | |
| MF | 3.77 ± 0.93 | 3.81 ± 0.93 | 0.69 | 0.04 | |
| SP–AG | 3.91 ± 0.93 | 3.98 ± 0.90 | 0.64 | 0.04 | |
| FL | 3.44 ± 1.13 | 3.48 ± 1.12 | 0.66 | 0.03 | |
| Adolescents (n = 544) | overall | 3.89 ± 0.87 | 3.83 ± 0.92 | 0.44 | 0.03 |
| CRF | 3.57 ± 0.94 | 3.62 ± 0.93 | 0.42 | 0.03 | |
| MF | 3.58 ± 0.93 | 3.57 ± 0.95 | 0.52 | 0.03 | |
| SP–AG | 3.71 ± 0.92 | 3.74 ± 0.90 | 0.48 | 0.03 | |
| FL | 3.29 ± 1.06 | 3.34 ± 1.07 | 0.47 | 0.03 |
| Statistics | Boys | Girls | Children | Adolescents | Overall |
|---|---|---|---|---|---|
| χ2 | 1.157 | 13.395 | 4.067 | 1.018 | 3.525 |
| df | 2 | 2 | 2 | 2 | 2 |
| p | 0.561 | 0.001 | 0.131 | 0.601 | 0.172 |
| χ2/df | 0.579 | 6.697 | 2.033 | 0.509 | 1.763 |
| SRMR (95% CI) | 0.011 | 0.043 | 0.027 | 0.010 | 0.015 |
| RMSEA (95% CI) | 0.000 | 0.114 | 0.052 | 0.000 | 0.029 |
| GFI | 0.999 | 0.985 | 0.995 | 0.999 | 0.998 |
| CFI | 1.000 | 0.971 | 0.994 | 1.000 | 0.999 |
| NFI | 0.998 | 0.966 | 0.988 | 0.998 | 0.997 |
| TLI | 1.004 | 0.912 | 0.982 | 1.004 | 0.996 |
| IFI | 1.001 | 0.971 | 0.994 | 1.001 | 0.999 |
| Statistics | Boys | Girls | Children | Adolescents | Overall |
|---|---|---|---|---|---|
| CRF | 0.78 | 0.69 | 0.76 | 0.73 | 0.74 |
| MF | 0.80 | 0.68 | 0.68 | 0.80 | 0.75 |
| SP–AG | 0.77 | 0.74 | 0.74 | 0.78 | 0.77 |
| FL | 0.47 | 0.47 | 0.34 | 0.49 | 0.43 |
| CR | 0.80 | 0.74 | 0.73 | 0.80 | 0.77 |
| AVE | 0.52 | 0.43 | 0.43 | 0.51 | 0.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bao, R.; Chen, S.; Kastelic, K.; Drenowatz, C.; Li, M.; Zhang, J.; Wang, L. Reliability of International Fitness Scale (IFIS) in Chinese Children and Adolescents. Children 2022, 9, 531. https://doi.org/10.3390/children9040531
Bao R, Chen S, Kastelic K, Drenowatz C, Li M, Zhang J, Wang L. Reliability of International Fitness Scale (IFIS) in Chinese Children and Adolescents. Children. 2022; 9(4):531. https://doi.org/10.3390/children9040531
Chicago/Turabian StyleBao, Ran, Sitong Chen, Kaja Kastelic, Clemens Drenowatz, Minghui Li, Jialin Zhang, and Lei Wang. 2022. "Reliability of International Fitness Scale (IFIS) in Chinese Children and Adolescents" Children 9, no. 4: 531. https://doi.org/10.3390/children9040531
APA StyleBao, R., Chen, S., Kastelic, K., Drenowatz, C., Li, M., Zhang, J., & Wang, L. (2022). Reliability of International Fitness Scale (IFIS) in Chinese Children and Adolescents. Children, 9(4), 531. https://doi.org/10.3390/children9040531