
A Selective Screening Strategy Performed in Pre-School Children and Siblings to Detect Familial Hypercholesterolemia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Recruitment of Study Population
- (1)
- Do you have elevated blood fats (=total cholesterol, triglycerides, LDL-cholesterol)?
- (2)
- Do you take cholesterol-lowering medication?
- O Yes O No
- If the answer to this question is yes, please specify medication (indicate medication and daily dosage): _________________________________________________
- (3)
- Do you have fatty skin growths/deposits (=xanthomas, xanthelasms) above all in the areas of the Achilles tendon/hands/knees or eyes?
- (4)
- Do you suffer from heart diseases (=calcification/narrowing of the coronary vessels, heart attack), narrowing of large vessels (e.g., main artery, carotid artery) or cerebral circulatory disorders (=stroke)?
- (5)
- Do close relatives (first and second grade*) have:
2.2. Lipid Screening Test
2.3. Statistical Analysis
3. Results
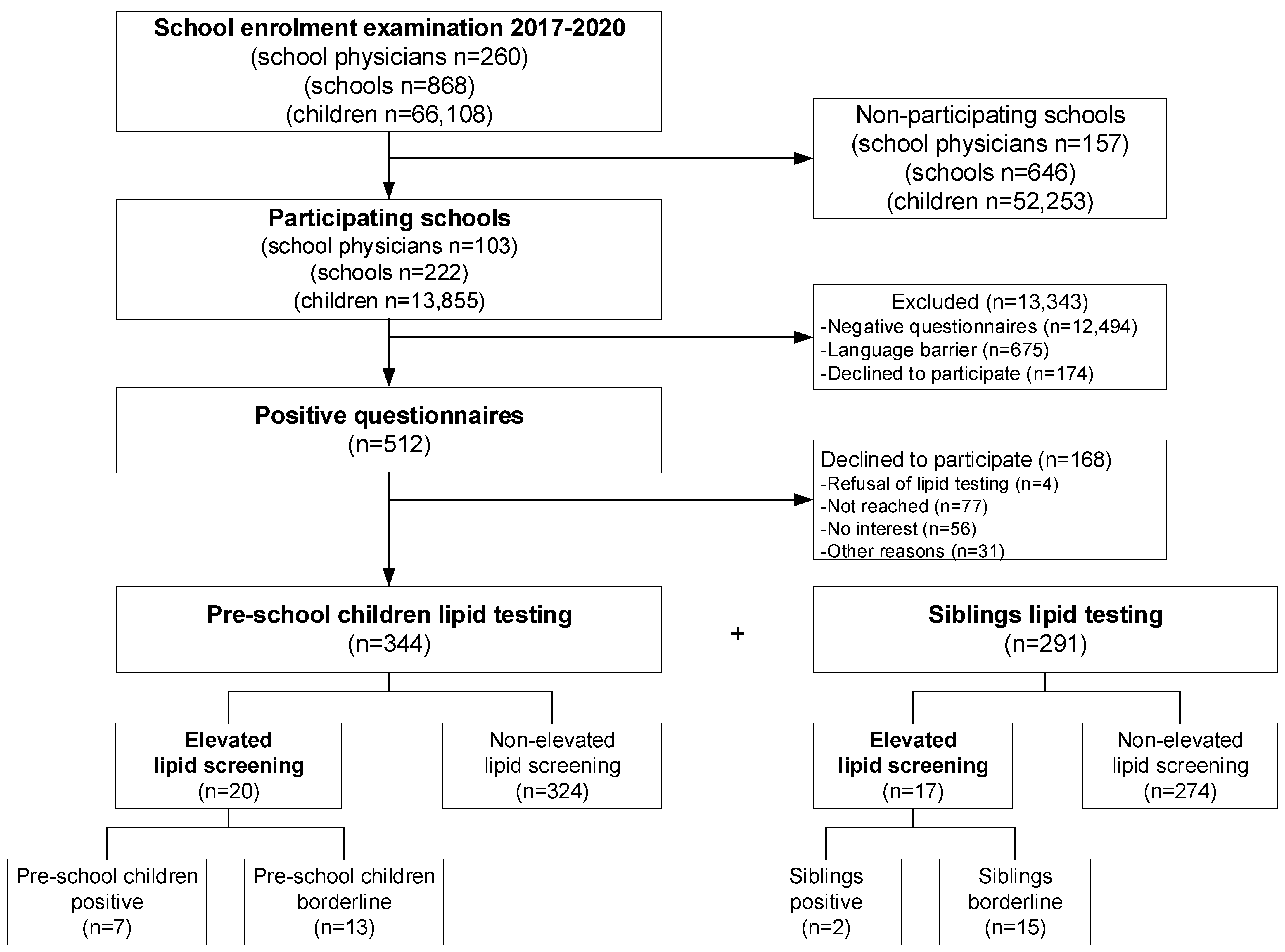
3.1. FH-Screening Strategy
3.2. Pre-School Children and Their Siblings
3.3. Venous Blood Measurement and Genetic Testing
4. Discussion
4.1. Selective Screening Strategy
4.2. Benefits of This Type of Lipid Screening Test
4.3. Outcome of Genetic Testing
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiegman, A. Lipid Screening, Action, and Follow-up in Children and Adolescents. Curr. Cardiol. Rep. 2018, 20, 80. [Google Scholar] [CrossRef] [PubMed]
- Nordestgaard, B.G.; Chapman, M.J.; Humphries, S.E.; Ginsberg, H.N.; Masana, L.; Descamps, O.S.; Wiklund, O.; Hegele, R.A.; Raal, F.J.; Defesche, J.C.; et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: Guidance for clinicians to prevent coronary heart disease: Consensus statement of the European Atherosclerosis Society. Eur. Heart J. 2013, 34, 3478–3490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watts, G.F.; Gidding, S.; Wierzbicki, A.S.; Toth, P.P.; Alonso, R.; Brown, W.V.; Bruckert, E.; Defesche, J.; Lin, K.K.; Livingston, M.; et al. Integrated guidance on the care of familial hypercholesterolaemia from the International FH Foundation. Int. J. Cardiol. 2014, 171, 309–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watts, G.F.; Gidding, S.S.; Mata, P.; Pang, J.; Sullivan, D.R.; Yamashita, S.; Raal, F.J.; Santos, R.D.; Ray, K.K. Familial hypercholesterolaemia: Evolving knowledge for designing adaptive models of care. Nat. Rev. Cardiol. 2020, 17, 360–377. [Google Scholar] [CrossRef] [PubMed]
- Usifo, E.; Leigh, S.E.; Whittall, R.A.; Lench, N.; Taylor, A.; Yeats, C.; Orengo, C.A.; Martin, A.C.; Celli, J.; Humphries, S.E. Low-density lipoprotein receptor gene familial hypercholesterolemia variant database: Update and pathological assessment. Ann. Hum. Genet. 2012, 76, 387–401. [Google Scholar] [CrossRef]
- Humphries, S.E.; Norbury, G.; Leigh, S.; Hadfield, S.G.; Nair, D. What is the clinical utility of DNA testing in patients with familial hypercholesterolaemia? Curr. Opin. Lipidol. 2008, 19, 362–368. [Google Scholar] [CrossRef]
- Motazacker, M.M.; Pirruccello, J.; Huijgen, R.; Do, R.; Gabriel, S.; Peter, J.; Kuivenhoven, J.A.; Defesche, J.C.; Kastelein, J.J.; Hovingh, G.K.; et al. Advances in genetics show the need for extending screening strategies for autosomal dominant hypercholesterolaemia. Eur. Heart J. 2012, 33, 1360–1366. [Google Scholar] [CrossRef] [Green Version]
- Wiegman, A.; Gidding, S.S.; Watts, G.F.; Chapman, M.J.; Ginsberg, H.N.; Cuchel, M.; Ose, L.; Averna, M.; Boileau, C.; Boren, J.; et al. Familial hypercholesterolaemia in children and adolescents: Gaining decades of life by optimizing detection and treatment. Eur. Heart J. 2015, 36, 2425–2437. [Google Scholar] [CrossRef] [Green Version]
- Scientific Steering Committee on behalf of the Simon Broome Register Group. Risk of fatal coronary heart disease in familial hypercholesterolaemia. BMJ 1991, 303, 893–896. [Google Scholar] [CrossRef] [Green Version]
- Daniels, S.R.; Gidding, S.S.; de Ferranti, S.D.; National Lipid Association Expert Panel on Familial Hypercholesterolemia. Pediatric aspects of familial hypercholesterolemias: Recommendations from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J. Clin. Lipidol. 2011, 5 (Suppl. 3), S30–S37. [Google Scholar] [CrossRef]
- Kusters, D.M.; de Beaufort, C.; Widhalm, K.; Guardamagna, O.; Bratina, N.; Ose, L.; Wiegman, A. Paediatric screening for hypercholesterolaemia in Europe. Arch. Dis. Child. 2012, 97, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Klancar, G.; Groselj, U.; Kovac, J.; Bratanic, N.; Bratina, N.; Trebusak Podkrajsek, K.; Battelino, T. Universal Screening for Familial Hypercholesterolemia in Children. J. Am. Coll. Cardiol. 2015, 66, 1250–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreissl, A.; Walleczek, N.; Espina, P.R.; Hallwirth, U.; Greber-Platzer, S. Selective screening for familial hypercholesterolemia in Austrian children—First year results. BMC Pediatr. 2019, 19, 208. [Google Scholar] [CrossRef] [PubMed]
- Groselj, U.; Kovac, J.; Sustar, U.; Mlinaric, M.; Fras, Z.; Podkrajsek, K.T.; Battelino, T. Universal screening for familial hypercholesterolemia in children: The Slovenian model and literature review. Atherosclerosis 2018, 277, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.C.; Hopkins, P.N.; Toth, P.P.; Ballantyne, C.M.; Rader, D.J.; Robinson, J.G.; Daniels, S.R.; Gidding, S.S.; de Ferranti, S.D.; Ito, M.K.; et al. Familial hypercholesterolemia: Screening, diagnosis and management of pediatric and adult patients: Clinical guidance from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J. Clin. Lipidol. 2011, 5, 133–140. [Google Scholar] [CrossRef]
- Ibrahim, S.; Reeskamp, L.F.; Stroes, E.S.G.; Watts, G.F. Advances, gaps and opportunities in the detection of familial hypercholesterolemia: Overview of current and future screening and detection methods. Curr. Opin. Lipidol. 2020, 31, 347–355. [Google Scholar] [CrossRef]
- Kose, E.; Kose, M.; Ozturk, S.I.; Ozcan, E.; Onay, H.; Ozkan, B. Cascade screening and treatment of children with familial hypercholesterolemia in Turkey. J. Pediatr. Endocrinol. Metab. 2020, 33, 1251–1256. [Google Scholar] [CrossRef]
- Langslet, G.; Ose, L. Screening methods in the diagnosis and assessment of children and adolescents with familial hypercholesterolemia. Expert Rev. Cardiovasc. Ther. 2013, 11, 1061–1066. [Google Scholar] [CrossRef] [Green Version]
- Knowles, J.W.; Rader, D.J.; Khoury, M.J. Cascade Screening for Familial Hypercholesterolemia and the Use of Genetic Testing. JAMA 2017, 318, 381–382. [Google Scholar] [CrossRef]
- Pears, R.; Griffin, M.; Futema, M.; Humphries, S.E. Improving the cost-effectiveness equation of cascade testing for familial hypercholesterolaemia. Curr. Opin. Lipidol. 2015, 26, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.P.; Davis, S.; Matches, S.; Shah, D.; Leung-Pineda, V.; Mou, M.; Hamilton, L.; McNeal, C.J.; Bowman, W.P. Universal cholesterol screening of children in community-based ambulatory pediatric clinics. J. Clin. Lipidol. 2015, 9 (Suppl. 5), S88–S92. [Google Scholar] [CrossRef] [PubMed]
- Neil, H.A.; Hammond, T.; Huxley, R.; Matthews, D.R.; Humphries, S.E. Extent of underdiagnosis of familial hypercholesterolaemia in routine practice: Prospective registry study. BMJ 2000, 321, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umans-Eckenhausen, M.A.; Defesche, J.C.; Sijbrands, E.J.; Scheerder, R.L.; Kastelein, J.J. Review of first 5 years of screening for familial hypercholesterolaemia in the Netherlands. Lancet 2001, 357, 165–168. [Google Scholar] [CrossRef]
- Mackie, T.I.; Tse, L.L.; de Ferranti, S.D.; Ryan, H.R.; Leslie, L.K. Treatment decision making for adolescents with familial hypercholesterolemia: Role of family history and past experiences. J. Clin. Lipidol. 2015, 9, 583–593. [Google Scholar] [CrossRef]
- Marks, D.; Thorogood, M.; Neil, H.A.; Humphries, S.E. A review on the diagnosis, natural history, and treatment of familial hypercholesterolaemia. Atherosclerosis 2003, 168, 1–14. [Google Scholar] [CrossRef]
- Martin, A.C.; Gidding, S.S.; Wiegman, A.; Watts, G.F. Knowns and unknowns in the care of pediatric familial hypercholesterolemia. J. Lipid Res. 2017, 58, 1765–1776. [Google Scholar] [CrossRef] [Green Version]
- Sacks, F.M.; Lichtenstein, A.H.; Wu, J.H.Y.; Appel, L.J.; Creager, M.A.; Kris-Etherton, P.M.; Miller, M.; Rimm, E.B.; Rudel, L.L.; Robinson, J.G.; et al. Dietary Fats and Cardiovascular Disease: A Presidential Advisory from the American Heart Association. Circulation 2017, 136, e1–e23. [Google Scholar] [CrossRef]
- de Ferranti, S.D. Familial hypercholesterolemia in children and adolescents: A clinical perspective. J. Clin. Lipidol. 2015, 9 (Suppl. 5), S11–S19. [Google Scholar] [CrossRef]
- Board, J.B.S. Joint British Societies’ consensus recommendations for the prevention of cardiovascular disease (JBS3). Heart 2014, 100 (Suppl. 2), ii1–ii67. [Google Scholar] [CrossRef]
- Reynolds, T.M.; Pottle, A.; Quoraishi, S.H. Current Perspectives on the Attainment of Lipid Modification Goals Relating to the Use of Statins and Ezetimibe for the Prevention of Cardiovascular Disease in the United Kingdom. Vasc. Health Risk Manag. 2021, 17, 227–237. [Google Scholar] [CrossRef]
- Soran, H.; Cooper, J.A.; Durrington, P.N.; Capps, N.; McDowell, I.F.W.; Humphries, S.E.; Neil, A.; Simon Broome Familial Hyperlipidaemia Register Group. Non-HDL or LDL cholesterol in heterozygous familial hypercholesterolaemia: Findings of the Simon Broome Register. Curr. Opin. Lipidol. 2020, 31, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.G.; Wang, S.; Smith, B.J.; Jacobson, T.A. Meta-analysis of the relationship between non-high-density lipoprotein cholesterol reduction and coronary heart disease risk. J. Am. Coll. Cardiol. 2009, 53, 316–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Futema, M.; Ramaswami, U.; Tichy, L.; Bogsrud, M.P.; Holven, K.B.; Roeters van Lennep, J.; Wiegman, A.; Descamps, O.S.; De Leener, A.; Fastre, E.; et al. Comparison of the mutation spectrum and association with pre and post treatment lipid measures of children with heterozygous familial hypercholesterolaemia (FH) from eight European countries. Atherosclerosis 2021, 319, 108–117. [Google Scholar] [CrossRef]
- Sjouke, B.; Tanck, M.W.T.; Fouchier, S.W.; Defesche, J.C.; Hutten, B.A.; Wiegman, A.; Kastelein, J.J.P.; Hovingh, G.K. Children with hypercholesterolemia of unknown cause: Value of genetic risk scores. J. Clin. Lipidol. 2016, 10, 851–859. [Google Scholar] [CrossRef] [PubMed]
- van der Graaf, A.; Avis, H.J.; Kusters, D.M.; Vissers, M.N.; Hutten, B.A.; Defesche, J.C.; Huijgen, R.; Fouchier, S.W.; Wijburg, F.A.; Kastelein, J.J.; et al. Molecular basis of autosomal dominant hypercholesterolemia: Assessment in a large cohort of hypercholesterolemic children. Circulation 2011, 123, 1167–1173. [Google Scholar] [CrossRef] [Green Version]
- Awan, Z.; Choi, H.Y.; Stitziel, N.; Ruel, I.; Bamimore, M.A.; Husa, R.; Gagnon, M.H.; Wang, R.H.; Peloso, G.M.; Hegele, R.A.; et al. APOE p.Leu167del mutation in familial hypercholesterolemia. Atherosclerosis 2013, 231, 218–222. [Google Scholar] [CrossRef]
- Olmastroni, E.; Gazzotti, M.; Arca, M.; Averna, M.; Pirillo, A.; Catapano, A.L.; Casula, M.; Groupdagger, L.S. Twelve Variants Polygenic Score for Low-Density Lipoprotein Cholesterol Distribution in a Large Cohort of Patients with Clinically Diagnosed Familial Hypercholesterolemia With or Without Causative Mutations. J. Am. Heart Assoc. 2022, 11, e023668. [Google Scholar] [CrossRef]
- Khera, A.V.; Won, H.H.; Peloso, G.M.; Lawson, K.S.; Bartz, T.M.; Deng, X.; van Leeuwen, E.M.; Natarajan, P.; Emdin, C.A.; Bick, A.G.; et al. Diagnostic Yield and Clinical Utility of Sequencing Familial Hypercholesterolemia Genes in Patients with Severe Hypercholesterolemia. J. Am. Coll. Cardiol. 2016, 67, 2578–2589. [Google Scholar] [CrossRef]


{kind=link}
| All Years 2017–2020 | 1st Year 2017 | 2nd Year 2018 | 3rd Year 2019 | 4th Year 2020 | |
|---|---|---|---|---|---|
| Number of schools | 868 | 215 | 214 | 251 | 188 |
| Participating schools | 222 (26%) | 76 (35%) | 100 (47%) | 32 (13%) | 14 (7%) |
| Number of school physicians | 260 | 63 | 67 | 69 | 61 |
| Participating school physicians | 103 (40%) | 37 (59%) | 35 (52%) | 19 (28%) | 12 (20%) |
| Number of children started school | 66.108 | 18.152 | 15.214 | 15.223 | 17.519 |
| Participating children | 13.855 (21%) | 6325 (35%) | 3842 (25%) | 2468 (16%) | 1220 (7%) |
| Positive questionnaires | 512 (4%) | 229 (4%) | 228 (6%) | 37 (1%) | 18 (1%) |
| Pre-school children lipid testing | 344 (67%) | 133 (58%) | 156 (68%) | 37 (100%) | 18 (100%) |
| Pre-school children elevated LDL-C/non-HDL-C | 20 (6%) | 9 (7%) | 3 (2%) | 6 (17%) | 2 (11%) |
| Pre-school children positive | 7 (2%) | 3 (2%) | 1 (1%) | 3 (8%) | 0 (0%) |
| Pre-school children borderline | 13 (4%) | 6 (5%) | 2 (1%) | 3 (8%) | 2 (11%) |
| Siblings lipid testing | 291 | 85 | 154 | 35 | 17 |
| Siblings elevated LDL-C/non-HDL-C | 17 (6%) | 4 (5%) | 3 (2%) | 4 (11%) | 6 (35%) |
| Siblings positive | 2 (1%) | 0 (0%) | 0 (0%) | 2 (6%) | 0 (0%) |
| Siblings borderline | 15 (5%) | 4 (5%) | 3 (2%) | 2 (6%) | 6 (35%) |
| Mothers (n = 344) | Fathers (n = 344) | |||||
|---|---|---|---|---|---|---|
| Questions | Yes | No | Not Measured/ Unknown | Yes | No | Not Measured/ Unknown |
| Hypercholesterolemia | 79 (23%) | 211 (61%) | 54 (16%) | 143 (42%) | 145 (42%) | 56 (16%) |
| Statin intake | 11 (3%) | 329 (96%) | 4 (1%) | 57 (16%) | 267 (78%) | 20 (6%) |
| Xanthomas/xanthelasma | 6 (2%) | 333 (97%) | 5 (1%) | 7 (2%) | 316 (92%) | 21 (6%) |
| Coronary heart disease | 11 (3%) | 329 (96%) | 4 (1%) | 33 (10%) | 296 (86%) | 15 (4%) |
| Relatives-hypercholesterolemia | 201 (58%) | 124 (36%) | 19 (6%) | 155 (45%) | 142 (41%) | 47 (14%) |
| Relatives-premature heart attack/stroke | 102 (30%) | 201 (58%) | 41 (12%) | 52 (15%) | 122 (36%) | 170 (49%) |
| Pre-School Children | Pre-School Children Elevated Lipid Screening | Siblings | Siblings Elevated Lipid Screening | |
|---|---|---|---|---|
| N | 344 | 20 | 291 | 17 |
| Male N (%) | 178 (52%) | 8 (40%) | 127 (44%) | 7 (41%) |
| Age (years) | 6 (5–8) | 6 (5–8) | 7 (1–28) | 4 (1–16) |
| Height (cm) | 118 (100–145) | 117 (110–127) | 127 (68–190) | 110 (68–176) |
| Weight (kg) | 22 (13–55) | 21 (17–34) | 26 (7–90) | 28 (7–70) |
| BMI (kg/m²) | 16 (11–31) | 16 (13–22) | 17 (9–35) | 17 (11–30) |
| LDL-C (mg/dL) | 76 (14–216) | 151 (111–216) | 71 (8–185) | 141 (111–185) |
| non-HDL-C (mg/dL) | 100 (47–235) | 175 (150–325) | 103 (49–212) | 172 (141–212) |
| TC (mg/dL) | 159 (99–313) | 235 (206–313) | 160 (99–282) | 230 (177–282) |
| HDL-C (mg/dL) | 58 (22–101) | 58 (42–86) | 56 (20–101) | 57 (27–100) |
| TG (mg/dL) | 114 (44–510) | 109 (47–249) | 125 (44–491) | 145 (44–247) |
| C/HDL ratio | 2.7 (1.6–6.0) | 4.0 (2.9–5.5) | 2.9 (1.6–8.0) | 3.8 (2.6–8.0) |
| Lipid Screening Test | Venous Blood Sampling | Genetic Testing | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | TC (mg/dL) | LDL-C (mg/dL) | HDL-C (mg/dL) | TG (mg/dL) | Non-HDL (mg/dL) | C/HDL Ratio | TC (mg/dL) | LDL-C (mg/dL) | HDL-C (mg/dL) | TG (mg/dL) | Positive for Familial Hypercholesterolemia |
| 18_2017 | 275 | 210 | 50 | 76 | 225 | 5.5 | 253 | 189 | 50 | 70 | LDLR: E4: c.662A>G, p.Asp221Gly in heterozygous (het)-form |
| 45_2017 | 281 | 193 | 74 | 72 | 207 | 3.8 | 245 | 164 | 69 | 61 | APOB: E26: c.10580G>A, p.Arg3527Gln in het-form |
| 87_2017 | 226 | 152 | 58 | 82 | 168 | 3.9 | 254 | 176 | 66 | 59 | LDLR: E6: c.858C>A, p.Ser286Arg in het-form |
| 92S3_2017 | 238 | 148 | 66 | 118 | 172 | 3.6 | 235 | 166 | 58 | 57 | LDLR: E5: c.798T>GA, p.Asp266Glu in het-form |
| 21_2018 | 260 | 161 | 79 | 99 | 181 | 3.3 | 301 | 209 | 81 | 54 | LDLR: E17:c.2483A>G, p.Tyr828Cys in het-form |
| 61S2_2018 | 194 | 123 | 50 | 105 | 144 | 3.9 | 179 | 118 | 45 | 82 | LDLR: E10: c.1414G>A, p.Asp472Asn in het-form |
| 19_2019 | 313 | 216 | 78 | 96 | 235 | 4 | 352 | 261 | 73 | 91 | LDLR: E10: c.1474G>A, p.Asp492Asn in het-form |
| 19S1_2019 | 264 | 181 | 52 | 157 | 212 | 5.1 | 262 | 196 | 49 | 87 | LDLR: E10: c.1474G>A, p.Asp492Asn in het-form |
| Lipid Screening Test | Venous Blood Sampling | Genetic Testing | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | TC (mg/dL) | LDL-C (mg/dL) | HDL-C (mg/dL) | TG (mg/dL) | Non-HDL (mg/dL) | C/HDL Ratio | TC (mg/dL) | LDL-C (mg/dL) | HDL-C (mg/dL) | TG (mg/dL) | New Genetic Variants |
| 96_2017 | 233 | 177 | 42 | 69 | 191 | 5.5 | 270 | 213 | 49 | 39 | LDLR: E11: c.1683-1690delGTGGCCCAinsCCCTATGTTCGCAGGACAGCCT, p.Gln561_Asn564delinsHisProArgTyrValArgArgThrAlaTyr in het-form; known mutation associated with low LDL-C: PCSK9: E1: c.137G>T, p.Arg46Leu in het-form |
| 105_2017 | 230 | 141 | 80 | 47 | 150 | 2.9 | 207 | 131 | 68 | 38 | PCSK9: E1: c.75C>T, p.Pro25= in het-form |
| 108_2017 | 218 | 129 | 54 | 176 | 164 | 4 | 219 | 151 | 42 | 131 | LDLR: E7: c.993C>T, p.Asp331 in het-form |
| 5S2_2017 | 230 | 157 | 44 | 143 | 186 | 5.2 | 235 | 159 | 51 | 127 | LDLR: I5: c.817+6C>T in het-form |
| 9_2019 | 297 | 187 | 86 | 120 | 211 | 3.5 | 277 | 196 | 61 | 100 | LDLR: E4: c.386A>C, p.Asp129Ala in het-form |
| 9S1_2019 | 282 | 185 | 80 | 84 | 202 | 3.5 | 286 | 201 | 71 | 70 | LDLR: E4: c.386A>C, p.Asp129Ala in het-form |
| Mutation—not clearly associated with FH | |||||||||||
| 105_2018 | 241 | 155 | 57 | 147 | 184 | 4.2 | 265 | 203 | 47 | 76 | LDLR: I11: c.1706-10G>A in het-form |
| Lipid Screening Test | Venous Blood Sampling | Genetic Testing | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | TC (mg/dL) | LDL-C (mg/dL) | HDL-C (mg/dL) | TG (mg/dL) | Non-HDL (mg/dL) | C/HDL Ratio | TC (mg/dL) | LDL-C (mg/dL) | HDL-C (mg/dL) | TG (mg/dL) | New Genetic Variants |
| 4S1_2019 | 203 | 128 | 60 | 74 | 143 | 3.4 | 202 | 137 | 52 | 65 | LDLRAP1: E7: c.742G>A, p.Val248Ileu in in het-form |
| 143_2018 | 217 | 121 | 71 | 127 | 146 | 3.1 | 222 | 145 | 62 | 74 | LDLRAP1: I1: c.88+31C>A in het-form |
| 143S1_2018 | 213 | 123 | 70 | 101 | 143 | 3.0 | 220 | 146 | 61 | 65 | LDLRAP1 I1: c.88+31C>A in in het-form |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thajer, A.; Baumgartner, M.; Jorda, A.; Hallwirth, U.; Lischka, J.; Greber-Platzer, S. A Selective Screening Strategy Performed in Pre-School Children and Siblings to Detect Familial Hypercholesterolemia. Children 2022, 9, 590. https://doi.org/10.3390/children9050590
Thajer A, Baumgartner M, Jorda A, Hallwirth U, Lischka J, Greber-Platzer S. A Selective Screening Strategy Performed in Pre-School Children and Siblings to Detect Familial Hypercholesterolemia. Children. 2022; 9(5):590. https://doi.org/10.3390/children9050590
Chicago/Turabian StyleThajer, Alexandra, Margot Baumgartner, Anselm Jorda, Ulrike Hallwirth, Julia Lischka, and Susanne Greber-Platzer. 2022. "A Selective Screening Strategy Performed in Pre-School Children and Siblings to Detect Familial Hypercholesterolemia" Children 9, no. 5: 590. https://doi.org/10.3390/children9050590
APA StyleThajer, A., Baumgartner, M., Jorda, A., Hallwirth, U., Lischka, J., & Greber-Platzer, S. (2022). A Selective Screening Strategy Performed in Pre-School Children and Siblings to Detect Familial Hypercholesterolemia. Children, 9(5), 590. https://doi.org/10.3390/children9050590