
Correlates of Sub-Optimal Feeding Practices among under-5 Children amid Escalating Crises in Lebanon: A National Representative Cross-Sectional Study

 , ,
, , 
Abstract
:1. Introduction
1.1. Prevalence of Breastfeeding
1.2. Complementary Feeding Practices
1.3. Prevalence of Malnutrition
1.4. Justification and Purpose of the Study
2. Materials and Methods
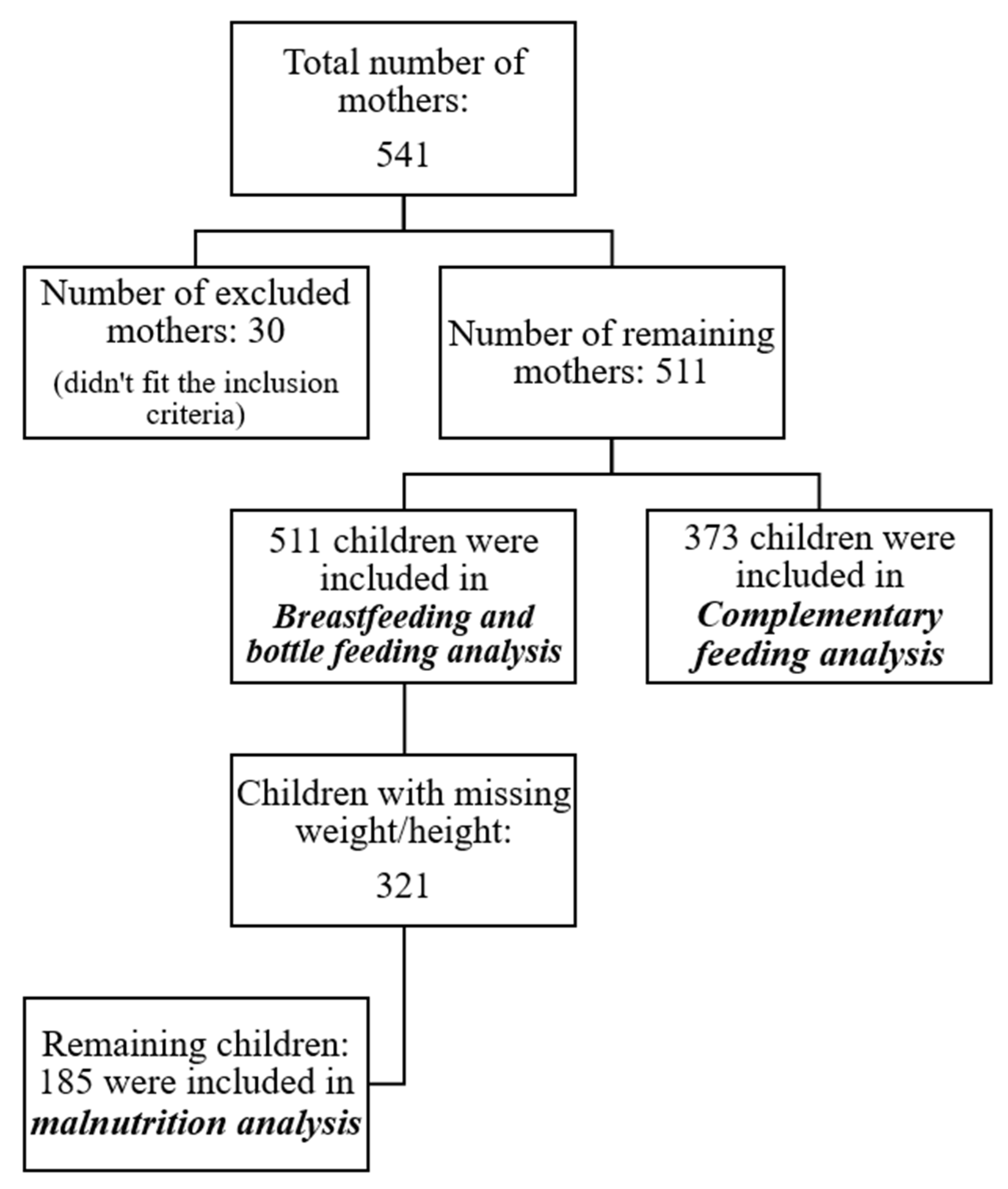
2.1. Study Design and Sampling Technique
2.2. Sample Size Calculation
2.3. Ethical Consideration
2.4. Data Collection
2.4.1. Assessment of Feeding Patterns and Their Correlates
2.4.2. Assessment of Malnutrition
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Prevalence of Malnutrition (Stunting, Wasting, Overweight and Underweight) and Feeding Patterns (Ever Breastfeeding, Exclusive Breastfeeding, Bottle Feeding, Continued Breastfeeding, Mixed Milk Feeding, and Introduction of Solid, Semi-Solid or Soft Foods)
3.3. Determinants of Breastfeeding, Bottle Feeding, and Complementary Feeding Practices
3.4. Multivariate Analyses
4. Discussion
4.1. Breastfeeding and Bottle-Feeding Practices
4.1.1. Comparison with National Data
4.1.2. Comparison with other EMR Countries
4.1.3. Comparison with Other International Studies
4.1.4. Complementary Feeding Practices
4.1.5. Correlates of Breastfeeding, Formula Feeding, and Complementary Feeding Practices
4.2. Malnutrition Data
4.2.1. Comparison with Other National Data
4.2.2. Comparison with Other EMR Countries
4.2.3. Comparison with Other International Studies

{kind=link}
| Countries | Prevalence of Infant Feeding | Prevalence of Malnutrition | References | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| EBF (%) | BOT (%) | CBF (%) | MixMF (%) | CF (%) | Stunting (%) | Under-Weight (%) | Wasting (%) | Overweight (%) | Obesity (%) | ||
| Lebanon (Current study) (2021, during the crisis) | 0–6 m: 59.1 | At birth: 25.8 At <1 m: 20.1 At <6 m: 13.6 6–12 m: 7.3 At >12 m: 7.1 | >12 m: 19 | At birth: 29 | At 4 m: 14.8 4–6 m: 37 At 6 m: 47.1 | 8.4 | 0.5 | 6.7 | 16.8 | 8.9 | Current study. |
| Lebanon (2021) | 0–6 m: 32.4 | NA | 12–23 m: 21.9 | <6 m: 39 | 6–8 m: 78.5 | 7 | 3.7 | 1.8 | 3.7 | 1.2 | [25] |
| Lebanon (2019, before the crisis) | At 40 d: 27 At 6 m: 30 | Birth-40 d: 52.9 40 d-6 m: 21.9 At 4 m: 13.8 At >6 m: 10.7 | >6 m: 23 | At birth: 10.6 | At <4 m: 1.3 4–6 m: 39.3 At 6 m:39.1 | 9.3 | 9.3 | 6.25 | 24.45 | NA | [26] |
| Lebanon (2016) | At ≤1 m: 62.2 2–3 m: 20.83 4–6 m: 16.54 | At 1 d: 51.6 | >6 m: 0.4 | NA | NA | NA | NA | NA | NA | NA | [27] |
| Lebanon (2011–2012) | At 40 d: 41.5 At 6 m: 12.3 | At 40 d: 20.2 | NA | At 40 d: 38.1 At 6 m: 38.4 | At 6 m: 40.1 | NA | NA | NA | NA | NA | [28] |
| Lebanon (2011–2012) | NA | NA | NA | NA | NA | NA | NA | NA | 6.5 | 2.7 | [58] |
| Lebanon (2010) | At <2: 40 4–5 m: 2 | NA | NA | NA | NA | NA | NA | NA | NA | NA | [29] |
| Lebanon (2003–2004) | NA | NA | NA | NA | At 4 m: 41.6 At 5 m: 11.3 At 6 m: 13.4 | NA | NA | NA | NA | NA | [30] |
| Lebanon (UNICEF database, 2004) * | NA | NA | 12–23 m: 14.3 | NA | NA | 16.5 | NA | 6.6 | 16.7 | NA | [32] |
| Lebanon (UNICEF/WHO/World Bank database, 2000–2020) * | NA | NA | NA | NA | NA | In 2000: 16 In 2020: 10.4 | NA | NA | In 2000: 17.6 In 2020: 19.7 | NA | [11] |
| EMR (UNICEF/WHO/World Bank database, 2000–2020) * | NA | NA | NA | NA | NA | In 2000: 33.8 In 2020: 26.2 | NA | In 2020: 7.4 | In 2000: 7.2 In 2020: 7.7 | NA | [11] |
| Algeria * | In 2020: 9.3% | In 2019: 2.7 | In 2020: 12.9% | ||||||||
| Egypt * | In 2020: 22.3 | In 2014: 9.5 | In 2020: 17.8 | ||||||||
| Bahrain * | In 2020: 5.1 | In 1995: 6.6 | In 2020: 6.4 | ||||||||
| Iraq * | In 2020: 11.6 | In 2018: 3 | In 2020: 9 | ||||||||
| Kuwait * | In 2020: 6 | In 2017: 2.5 | In 2020: 7.1 | ||||||||
| Oman * | In 2020: 12.2 | In 2017: 9.3 | In 2020: 4.8 | ||||||||
| Qatar * | In 2020: 4.6 | In 1995: 2.1 | In 2020: 13.9 | ||||||||
| Saudi Arabia * | In 2020: 3.9 | In 2004: 11.8 | In 2020: 7.6 | ||||||||
| Syrian Arab Republic * | In 2020: 29.6 | In 2010: 11.5 | In 2020: 18.2 | ||||||||
| Palestine * | NA | In 2020: 1.3 | In 2020: 8.5 | ||||||||
| Tunisia * | In 2020: 8.6 | In 2018: 2.1 | In 2020: 16.5 | ||||||||
| EMR (UNICEF database, 2014–2020) * | 0–5 m: 44 | NA | 12–23 m: 58 | NA | 6–8 m: 68 | NA | NA | NA | NA | NA | [32] |
| Egypt (2014) * | 39.5 | - | - | - | - | - | - | - | - | - | |
| Iran (2010) * | 53.1 | ||||||||||
| Iraq (2018) * | 25.8 | ||||||||||
| Morocco (2017) * | 27.8 | ||||||||||
| Oman (2017) * | 23.2 | ||||||||||
| Palestine (2020) * | 38.9 | ||||||||||
| Syrian Arab Republic (2019) * | 28.5 | ||||||||||
| Tunisia (2018) * | 13.5 | ||||||||||
| Yemen (2013) * | 9.7 | ||||||||||
| Algeria (2019) * | 28.6 | ||||||||||
| EMR (2018) | 29.3 | NA | NA | NA | NA | 28 | 18 | 8.69 | 8.42 | [60] | |
| Iran (2018) | NA | NA | NA | NA | NA | 8.45 | 7.63 | 8.04 | 1.23 | NA | [59] |
| Saudi Arabia (2019) | 0–6 m: 27.6 | NA | For 2 y: 20.4 | 74.3 | NA | NA | NA | NA | NA | NA | [34] |
| Sudan (2018–2019) | 62.31 | NA | Up to 2 y: 73.29 | NA | NA | 36.35 | 29.16 | 13.6 | 2.14 | 0.85 | [37] |
| Jordan (2000–2018) | In 2017–2018: 0–5 m: 25.4 | NA | In 2017–2018: 12–23 m: 26.1 | NA | In 2017–2018: 6–8 m: 83 | In 2012: 7.7 | In 2012: 3 | In 2012: 2.4 | In 2012: 4.7 | [35] | |
| Rural setting, Pakistan (2017–2018) | NA | NA | NA | NA | NA | 81.1 | 57.3 | 18.2 | NA | NA | [61] |
| Qatar (2017) | 1–3 m: 40 4–6 m: 20 | NA | ≥12 m: 34.8 | NA | NA | NA | NA | NA | NA | NA | [38] |
| Iran (2017) | NA | NA | NA | NA | NA | NA | NA | NA | 9 | 8 | [64] |
| Abu Dhabi, United Arab Emirates (2014–2015) | 0–6 m: 16.9 | NA | NA | NA | NA | NA | NA | NA | NA | NA | [36] |
| Yemen (2013) | NA | NA | NA | NA | NA | 47 | 39 | 16 | NA | NA | [62] |
| Somalia (2007–2010) | NA | NA | NA | NA | NA | 31 | NA | 21 | NA | NA | [63] |
| Global (UNICEF database, 2000–2020) * | NA | NA | NA | NA | NA | In 2000: 33.1 In 2020: 22 | NA | In 2020: 6.7 | In 2000: 5.4 In 2020: 5.7 | NA | [11] |
| Global (UNICEF/WHO/World Bank database, 2014–2020) * | 0–5 m: 44 | NA | 12–23 m: 65 | NA | 6–8 m: 73 | NA | NA | NA | NA | NA | [32] |
| Region of the Americas (2000–2020) * | In 2014–2020: 32 | NA | In 2014–2020: 12–23 m: 31 | NA | NA | In 2020: 8.9 | NA | In 2020: 0.7 | In 2020: 8 | NA | [32] |
| Europe Region (2000–2020) * | NA | NA | NA | NA | NA | In 2020: 5.7 | NA | NA | In 2020: 7.9 | NA | [32] |
| Albania (2017) * | 36.5 | ||||||||||
| Belarus (2019) * | 21.7 | ||||||||||
| Montenegro (2018) * | 19.5 | ||||||||||
| Republic of Moldova (2012) * | 36.4 | ||||||||||
| Romania (2004) * | 15.8 | ||||||||||
| Serbia (2019) * | 23.6 | ||||||||||
| Ukraine (2012) * | 19.7 | ||||||||||
| Western Pacific Region (2000–2020) * | In 2014–2020: 0–5 m: 26 | NA | NA | NA | In 2014–2020: 6–8 m: 84 | In 2020: 9.3 | NA | In 2020: 2.1 | In 2020: 7.5 | NA | [32] |
| Latin America and the Caribbean (2015) | NA | NA | NA | NA | NA | NA | NA | NA | NA | 9.2 | [67]. |
| Central and Eastern Europe and Central Asia (2015) | NA | NA | NA | NA | NA | NA | NA | NA | NA | 10.9 | [67] |
| Italy (2019) | At 3 m: 68 | At 3 m: 17 | NA | NA | At 3 m: 14 | NA | NA | NA | NA | NA | [42] |
| Nepal (2017–2018) | 0–6 m: 23.2 | NA | NA | 0–6 m: 48.6 | <5 m: 22.5 | NA | NA | NA | NA | NA | [40] |
| Peru (2009–2016) | NA | NA | NA | NA | NA | 14.4 | 0.3 | 0.1 | NA | NA | [65] |
| Spain (2014–2015) | At 6 m: 28.2 | NA | NA | NA | NA | NA | NA | NA | NA | NA | [39] |
| Bangladesh Vietnam Ethiopia (2010–2014) | 72 18 48 | NA | NA | NA | NA | NA | NA | NA | NA | NA | [41] |
| Brazil (2009–2017) | NA | NA | NA | NA | NA | In 2009: 13.7 In 2017: 12.4 | NA | In 2009: 5.7 In 2017: 5.1 | In 2009: 11.6 In 2017: 12.6 | [66] | |
4.3. Summary
4.4. Limits and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclaimer
References
- Brockway, M.; Benzies, K.; Hayden, K.A. Interventions to Improve Breastfeeding Self-Efficacy and Resultant Breastfeeding Rates: A Systematic Review and Meta-Analysis. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2017, 33, 486–499. [Google Scholar] [CrossRef] [PubMed]
- Office of the Surgeon General (US); Centers for Disease Control and Prevention (US); Office on Women’s Health (US). The Importance of Breastfeeding. In The Surgeon General’s Call to Action to Support Breastfeeding; Office of the Surgeon General (US): Rockville, MD, USA, 2011. Available online: https://www.ncbi.nlm.nih.gov/books/NBK52687/ (accessed on 10 March 2022).
- Camacho, E.M.; Hussain, H. Cost-effectiveness evidence for strategies to promote or support breastfeeding: A systematic search and narrative literature review. BMC Pregnancy Childbirth 2020, 20, 757. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Infant and Young Child Feeding. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding (accessed on 14 December 2021).
- Bhattacharjee, N. Mapping Inequalities in Exclusive Breastfeeding in Low- and Middle-Income Countries, 2000–2018. Institute for Health Metrics and Evaluation, 2021. Available online: https://www.healthdata.org/research-article/mapping-inequalities-exclusive-breastfeeding-low-and-middle-income-countries-2000 (accessed on 10 March 2022).
- Zong, X.; Wu, H.; Zhao, M.; Magnussen, C.G.; Xi, B. Global prevalence of WHO infant feeding practices in 57 LMICs in 2010-2018 and time trends since 2000 for 44 LMICs. EClinicalMedicine 2021, 37, 100971. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Countries Failing to Stop Harmful Marketing of Breast-Milk Substitutes, Warn WHO and UNICEF, Agencies Encourage Women to Continue to Breastfeed during the COVID-19 Pandemic. 2020. Available online: https://www.unicef.org/press-releases/countries-failing-stop-harmful-marketing-breast-milk-substitutes-warn-who-and-unicef (accessed on 16 December 2021).
- UNICEF. Improving Young Children’s Diets during the Complementary Feeding Period. 2020. Available online: https://www.unscn.org/en/news-events/recent-news?idnews=2030/ (accessed on 10 March 2022).
- United Nations Children’s Fund Division of Data Analysis Planning and Monitoring. Global UNICEF Global Databases: Infant and Young Child Feeding; New York, NY, USA, 2021. Available online: https://data.unicef.org/resources/dataset/infant-young-child-feeding/ (accessed on 26 May 2022).
- UNICEF. Malnutrition. 2021. Available online: https://data.unicef.org/topic/nutrition/malnutrition/ (accessed on 13 February 2022).
- UNICEF; WHO; World Bank Group Joint Child Malnutrition Estimates. Levels and Trends in Child Malnutrition. Available online: https://www.who.int/data/gho/data/themes/topics/joint-child-malnutrition-estimates-unicef-who-wb (accessed on 13 February 2022).
- Oueidat, H.; Charafeddine, L.; Nimer, H.; Hussein, H.; Nabulsi, M. Knowledge and attitudes of Lebanese women towards Baby Friendly Hospital Initiative practices. PLoS ONE 2020, 15, e0238730. [Google Scholar] [CrossRef]
- UNICEF. Ministry of Public Health Launches the National Campaign to Support Breastfeeding. 2015. Available online: https://www.unicef.org/lebanon/press-releases/ministry-public-health-launches-national-campaign-support-breastfeeding (accessed on 8 January 2022).
- Al Jawaldeh, A.A.; Doggui, R.; Borghi, E.; Aguenaou, H.; Ammari, L.E.; Abul-Fadl, A.; McColl, K. Tackling Childhood Stunting in the Eastern Mediterranean Region in the Context of COVID-19. Children 2020, 7, 239. [Google Scholar] [CrossRef]
- UNICEF. Lebanon: Escalating Crisis Puts Children at Risk as the Majority of Families Cannot Afford to Meet the Basic Needs of Their Children. 2021. Available online: https://www.unicef.org/press-releases/lebanon-escalating-crisis-puts-children-risk-majority-families-cannot-afford-meet#_ftn1 (accessed on 6 April 2022).
- Centers for Disease Control and Prevention. Epi info 7. Available online: http://wwwn.cdc.gov/epiinfo/7/index.htm (accessed on 10 March 2022).
- Lebanon Statistics on Women of Reproductive Age (15–49 years)-2019–2020. Available online: https://moph.gov.lb/userfiles/files/Statistics2019.pdf (accessed on 10 March 2022).
- Neves, P.A.; Barros, A.J.; Baker, P.; Piwoz, E.; Santos, T.M.; Gatica-Domínguez, G.; Vaz, J.S.; Rollins, N.; Victora, C.G. Consumption of breast milk, formula and other non-human milk by children aged under 2 years: Analysis of eighty-six low- and middle-income countries. Public Health Nutr. 2020, 16, 1–9. [Google Scholar] [CrossRef]
- CDC. “Questionnaires: Breastfeeding and Infant Feeding Practices.” Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/breastfeeding/data/ifps/questionnaires.htm (accessed on 28 December 2019).
- Fein, S.; Labiner-Wolfe, J.; Shealy, K.; Li, R.; Chen, J.; Grummer-Strawn, L. Infant Feeding Practices Study II: Study Methods. Pediatrics 2008, 122, S28–S35. [Google Scholar] [CrossRef] [Green Version]
- Medecin Sans Frontiers. 2021. Available online: https://www.msf.org/lebanon-overlapping-crises-increase-needs-and-worsen-access-care (accessed on 10 March 2022).
- World Health Organization (WHO). Child Growth Standards. WHO Anthro Survey Analyser and Other Tools. 2019. Available online: https://www.who.int/tools/child-growth-standards/software (accessed on 18 May 2022).
- World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization, 2006. Available online: https://apps.who.int/iris/handle/10665/43413 (accessed on 14 December 2021).
- UNICEF. UNICEF Report, Lebanon: Children’s Futures on the Line. 2021. Available online: https://www.unicef.org/lebanon/reports/lebanon-childrens-future-line (accessed on 10 March 2022).
- National Nutrition SMART SURVEY REPORT. Lebanon Nutrition Sector. 2021. Available online: https://www.unicef.org/lebanon/media/7921/file/National%20Nutrition%20SMART%20Survey%20Report%20.pdf (accessed on 10 March 2022).
- Abi Khalil, H.; Hawi, M.; Hoteit, M. Feeding Patterns, Mother-Child Dietary Diversity and Prevalence of Malnutrition among Under-Five Children in Lebanon: A Cross-Sectional Study Based on Retrospective Recall. Front. Nutr. 2022, 9, 815000. [Google Scholar] [CrossRef]
- Mattar, L.; Hobeika, M.; Zeidan, R.K.; Salameh, P.; Issa, C. Breastfeed for a Healthier Lebanon study group Determinants of Exclusive and Mixed Breastfeeding Durations and Risk of Recurrent Illnesses in Toddlers Attending Day Care Programs Across Lebanon. J. Pediatric Nurs. 2019, 45, e24–e34. [Google Scholar] [CrossRef]
- Chehab, R.F.; Nasreddine, L.; Zgheib, R.; Forman, M.R. Exclusive breastfeeding during the 40-day rest period and at six months in Lebanon: A cross-sectional study. Int. Breastfeed. J. 2020, 15, 45. [Google Scholar] [CrossRef]
- Akik, C.; Ghattas, H.; Filteau, S.; Knai, C. Barriers to breastfeeding in Lebanon: A policy analysis. J. Public Health Policy 2017, 38, 314–326. [Google Scholar] [CrossRef] [PubMed]
- Batal, M.; Boulghourjian, C.; Akik, C. Complementary feeding patterns in a developing country: A cross-sectional study across Lebanon/Alimentation de complément dans un pays en voie de développement: Une étude transversale au Liban. East. Mediterr. Health J. 2010, 16, 180–186. [Google Scholar] [CrossRef] [PubMed]
- WHO EMRO. Exclusive Breastfeeding under 6 Months (%). Available online: https://rho.emro.who.int/index.php/Indicator/TermID/30 (accessed on 8 January 2022).
- United Nations Children’s Fund, Division of Data, Analysis, Planning and Monitoring Global. UNICEF Global Databases: Infant and Young Child Feeding: Exclusive Breastfeeding, Continued Breastfeeding, Introduction to Solids, Semi-Solids and Soft Foods; New York, NY, USA, 2021. Available online: https://data.unicef.org/resources/dataset/infant-young-child-feeding/ (accessed on 8 January 2022).
- Arab News. 2022. Available online: https://www.arabnews.com/node/1877411/middle-east/ (accessed on 5 April 2022).
- Hegazi, M.A.; Allebdi, M.; Almohammadi, M.; Alnafie, A.; Al-Hazmi, L.; Alyoubi, S. Factors associated with exclusive breastfeeding in relation to knowledge, attitude and practice of breastfeeding mothers in Rabigh community, Western Saudi Arabia. World J. Pediatrics 2019, 15, 601–609. [Google Scholar] [CrossRef]
- Al-Awwad, N.J.; Ayoub, J.; Barham, R.; Sarhan, W.; Al-Holy, M.; Abughoush, M.; Al-Hourani, H.; Olaimat, A.; Al-Jawaldeh, A. Review of the Nutrition Situation in Jordan: Trends and Way Forward. Nutrients 2022, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Al Ketbi, M.I.; Al Noman, S.; Al Ali, A.; Darwish, E.; Al Fahim, M.; Rajah, J. Knowledge, attitudes, and practices of breastfeeding among women visiting primary healthcare clinics on the island of Abu Dhabi, United Arab Emirates. Int. Breastfeed. J. 2018, 13, 26. [Google Scholar] [CrossRef] [Green Version]
- Abu-Manga, M.; Al-Jawaldeh, A.; Qureshi, A.B.; Ali, A.M.E.; Pizzol, D.; Dureab, F. Nutrition Assessment of Under-Five Children in Sudan: Tracking the Achievement of the Global Nutrition Targets. Children 2021, 8, 363. [Google Scholar] [CrossRef]
- Nasser, A.; Omer, F.; Al-Lenqawi, F.; Al-awwa, R.; Khan, T.; El-Heneidy, A.; Kurdi, R.; Al-Jayyousi, G. Predictors of Continued Breastfeeding at One Year among Women Attending Primary Healthcare Centers in Qatar: A Cross-Sectional Study. Nutrients 2018, 10, 983. [Google Scholar] [CrossRef] [Green Version]
- Suárez-Cotelo, M.; Movilla-Fernández, M.J.; Pita-García, P.; Arias, B.F.; Novío, S. Breastfeeding knowledge and relation to prevalence. Rev. Da Esc. De Enferm. Da USP 2019, 53, e03433. [Google Scholar] [CrossRef]
- Dharel, D.; Dhungana, R.; Basnet, S.; Gautam, S.; Dhungana, A.; Dudani, R.; Bhattarai, A. Breastfeeding practices within the first six months of age in mid-western and eastern regions of Nepal: A health facility-based cross-sectional study. BMC Pregnancy Childbirth 2020, 20, 59. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.H.; Kim, S.S.; Tran, L.M.; Menon, P.; Frongillo, E.A. Early breastfeeding practices contribute to exclusive breastfeeding in Bangladesh, Vietnam and Ethiopia. Matern. Child Nutr. 2020, 16, e13012. [Google Scholar] [CrossRef] [Green Version]
- Gianni, M.L.; Bettinelli, M.E.; Manfra, P.; Sorrentino, G.; Bezze, E.; Plevani, L.; Cavallaro, G.; Raffaeli, G.; Crippa, B.L.; Colombo, L.; et al. Breastfeeding Difficulties and Risk for Early Breastfeeding Cessation. Nutrients 2019, 11, 2266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, S.; Getinet, T.; Solomon, S.; Jones, A.D. Prevalence of initiation of complementary feeding at 6 months of age and associated factors among mothers of children aged 6 to 24 months in Addis Ababa, Ethiopia. BMC Nutr. 2018, 4, 54. [Google Scholar] [CrossRef] [PubMed]
- Nabulsi, M.; Tamim, H.; Shamsedine, L.; Charafeddine, L.; Yehya, N.; Kabakian-Khasholian, T.; Masri, S.; Nasser, F.; Ayash, S.; Ghanem, D. A multi-component intervention to support breastfeeding in Lebanon: A randomized clinical trial. PLoS ONE 2019, 14, e0218467. [Google Scholar] [CrossRef] [PubMed]
- Nabulsi, M. Why Are Breastfeeding Rates Low in Lebanon? A Qualitative Study. 2021. Available online: https://www.researchgate.net/publication/51605969_Why_are_breastfeeding_rates_low_in_Lebanon_A_qualitative_study (accessed on 9 May 2021).
- Grzywacz, G.J.; Tucker, J.; Clinch, R.C.; Arcury, A.T. Individual and job-related variation in infant feeding practices among working mothers. Am. J. Health Behav. 2010, 34, 186–196. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. Breastfeeding Support in the Work Place. Available online: https://www.unicef.org/media/73206/file/Breastfeeding-room-guide.pdf (accessed on 19 December 2021).
- Mannion, C.A.; Hobbs, A.J.; McDonald, S.W.; Tough, S.C. Maternal perceptions of partner support during breastfeeding. Int. Breastfeed. J. 2013, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Cinar, N.; Kose, D.; Alvur, M.; Dogu, O. Mothers’ Attitudes toward Feeding Twin Babies in the First Six Months of Life: A Sample from Sakarya, Turkey. Iran. J. Pediatrics 2016, 26, e5413. [Google Scholar] [CrossRef] [Green Version]
- Helle, C.; Hillesund, E.R.; Øverby, N.C. Timing of complementary feeding and associations with maternal and infant characteristics: A Norwegian cross-sectional study. PLoS ONE 2018, 13, e0199455. [Google Scholar] [CrossRef]
- Brown, A.; Rowan, H. Maternal and infant factors associated with reasons for introducing solid foods. Matern. Child Nutr. 2016, 12, 500–515. [Google Scholar] [CrossRef]
- Grote, V.; Schiess, S.A.; Closa-Monasterolo, R.; Escribano, J.; Giovannini, M.; Scaglioni, S.; Stolarczyk, A.; Gruszfeld, D.; Hoyos, J.; Poncelet, P.; et al. The introduction of solid food and growth in the first 2 y of life in formula-fed children: Analysis of data from a European cohort study. Am. J. Clin. Nutr. 2011, 94, 1785S–1793S. [Google Scholar] [CrossRef] [Green Version]
- da Costa, T.H.; Haisma, H.; Wells, J.C.; Mander, A.P.; Whitehead, R.G.; Bluck, L.J. How much human milk do infants consume? Data from 12 countries using a standardized stable isotope methodology. J. Nutr. 2010, 140, 2227–2232. [Google Scholar] [CrossRef] [Green Version]
- Schrempft, S.; van Jaarsveld, C.H.; Fisher, A.; Wardle, J. Family and infant characteristics associated with timing of core and non-core food introduction in early childhood. Eur. J. Clin. Nutr. 2013, 67, 652–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holand, B.L.; de Oliveira Agostini, C.; Pacheco, M.; de Leon, D.; Drehmer, M.; Bosa, V.L. Association between breastfeeding and complementary feeding in pre-pandemic and pandemic COVID-19 times: Maternar cohort study. J. De Pediatr. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zanardo, V.; Tortora, D.; Guerrini, P.; Garani, G.; Severino, L.; Soldera, G.; Straface, G. Infant feeding initiation practices in the context of COVID-19 lockdown. Early Hum. Dev. 2021, 152, 105286. [Google Scholar] [CrossRef] [PubMed]
- Widyaningrum, R.; Safitri, R.A.; Ramadhani, K.; Suryani, D.; Syarief, F. Complementary Feeding Practices During COVID-19 Outbreak in Daerah Istimewa Yogyakarta, Indonesia, and Its Related Factor. Asia-Pac. J. Public Health 2021, 33, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, L.; Hwalla, N.; Saliba, A.; Akl, C.; Naja, F. Prevalence and Correlates of Preschool Overweight and Obesity Amidst the Nutrition Transition: Findings from a National Cross-Sectional Study in Lebanon. Nutrients 2017, 9, 266. [Google Scholar] [CrossRef] [Green Version]
- Aghabozorgi, A.R.; Safari, S.; Khadivi, R. The Prevalence Rate of Malnutrition in Children Younger than 5 in Iran in 2018. Int. J. Prev. Med. 2021, 12, 78. [Google Scholar] [CrossRef]
- Nasreddine, L.; Ayoub, J.J.; Al Jawaldeh, A. Review of the nutrition situation in the Eastern Mediterranean Region. East. Mediterr. Health J. 2018, 24, 77–91. [Google Scholar] [CrossRef]
- Menghwar, B.; Laghari, Z.A.; Memon, S.F.; Warsi, J.; Shaikh, S.A.; Baig, N.M. Prevalence of malnutrition in children under five years’ age in District Tharparkar Sindh, Pakistan. JPMA J. Pak. Med. Assoc. 2022, 72, 33–36. [Google Scholar] [CrossRef]
- Al-Zangabila, K.; Poudel Adhikari, S.; Wang, Q.; Sunil, T.S.; Rozelle, S.; Zhou, H. Alarmingly high malnutrition in childhood and its associated factors: A study among children under 5 in Yemen. Medicine 2021, 100, e24419. [Google Scholar] [CrossRef]
- Kinyoki, D.K.; Berkley, J.A.; Moloney, G.M.; Kandala, N.B.; Noor, A.M. Predictors of the risk of malnutrition among children under the age of 5 years in Somalia. Public Health Nutr. 2015, 18, 3125–3133. [Google Scholar] [CrossRef] [Green Version]
- Mansori, K.; Khateri, S.; Moradi, Y.; Khazaei, Z.; Mirzaei, H.; Hanis, S.M.; Aliabadi, M.A.; Ranjbaran, M.; Varse, F.; Parang, S. Prevalence of obesity and overweight in Iranian children aged less than 5 years: A systematic review and meta-analysis. Korean J. Pediatrics 2019, 62, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Quispe, D.; Hernández-Vásquez, A.; Miranda, J.J.; Anza-Ramirez, C.; Carrillo-Larco, R.M.; Pomati, M.; Nandy, S.; Bernabe-Ortiz, A. Urbanization in Peru is inversely associated with double burden of malnutrition: Pooled analysis of 92,841 mother-child pairs. Obesity 2021, 29, 1363–1374. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Silva, R.D.C.; Silva, N.D.J.; Felisbino-Mendes, M.S.; Falcão, I.R.; Andrade, R.d.C.S.d.; Silva, S.A.; Nilson, E.A.F.; Spaniol, A.M.; Fiaccone, R.L.; Paixão, E.; et al. Time trends and social inequalities in child malnutrition: Nationwide estimates from Brazil’s food and nutrition surveillance system, 2009–2017. Public Health Nutr. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Di Cesare, M.; Sorić, M.; Bovet, P.; Miranda, J.J.; Bhutta, Z.; Stevens, G.A.; Laxmaiah, A.; Kengne, A.P.; Bentham, J. The epidemiological burden of obesity in childhood: A worldwide epidemic requiring urgent action. BMC Med. 2019, 17, 212. [Google Scholar] [CrossRef] [Green Version]
- Force, N.T. Call for Action on Infant and Young Child Feeding and Nutrition in the Response to the Beirut Port Explosion. 2020. Available online: https://www.accioncontraelhambre.org/sites/default/files/documents/lebanon_nutrition_taskforce_sep2020.pdf (accessed on 19 May 2022).

| Characteristics of Mothers | Mean ± SD |
| Age (years) | 30.25 ± 4.98 |
| Weight (kg) | 66.40 ± 12.66 |
| Height (m) | 1.63 ± 0.06 |
| BMI (kg/m2) | 24.85 ± 4.53 |
| Household crowding index | 1.03 ± 0.40 |
| Characteristics of mothers | n(%) |
| Number of children (n = 511) | |
| 1 child | 241 (47.2) |
| 2–3 children | 238 (46.6) |
| >3 children | 32 (6.2) |
| Marital Status (n = 511) | |
| Married | 509 (99.6) |
| Divorced | 2 (0.4) |
| Governorate (n = 511) | |
| Beirut and Mount Lebanon | 288 (56.4) |
| North and Akkar | 124 (24.2) |
| Beqaa and Baalbeck/Hermel | 39 (7.6) |
| South and Nabatieh | 60 (11.8) |
| Family income (n = 510) | |
| Less than 750,000 LBP | 44 (8.6) |
| Between 750,000 LBP and 2,250,000 LBP | 304 (59.6) |
| More than 2,250,000 LBP | 162 (31.8) |
| Currently working (n = 511) | |
| Yes | 219 (42.8) |
| No | 292 (57.2) |
| Healthcare worker among working mothers (n = 219) | |
| Yes | 56 (25.6) |
| No | 163 (74.4) |
| Has twins or triplets (n = 511) | |
| Yes | 26 (5) |
| No | 485 (95) |
| Educational level of the spouse (n = 511) | |
| Illiterate | 3 (0.6) |
| School level | 233 (45.7) |
| University level | 275 (53.7) |
| COVID-19 infection (n = 511) | |
| Yes | 123 (24.1) |
| No | 388 (75.9) |
| Under-5 Children | Overall n (%) | Female (54.8%) n (%) | Male (45.2%) n (%) | p-Value |
|---|---|---|---|---|
| Age (month) (Mean ± SD) | (n = 492) | (n = 271) | (n = 221) | 0.312 |
| 18.7 ± 15.5 | 18 ± 15.5 | 19.5 ± 15.6 | ||
| Weight at birth (g) (Mean ± SD) | (n = 507) | (n = 277) | (n = 230) | <0.001 |
| 3168.9 ± 617.9 | 3074.18 ± 622.2 | 3283.35 ± 594.2 | ||
| Height at birth (cm) (Mean ± SD) | (n = 478) | (n= 260) | (n = 218) | 0.312 |
| 49.5 ± 5.2 | 49.2 ± 4.74 | 49.8 ± 5.7 | ||
| COVID-19 infection | (n= 510) | (n = 281) | (n = 229) | 0.131 |
| Yes | 83 (16.4) | 52 (18.6) | 31 (13.7) | |
| No | 427 (83.6) | 229 (81.4) | 198 (86.3) |
| Anthropometric Indices | Categories | Overall n (%) * | Female n (%) | Male n (%) | p-Value |
|---|---|---|---|---|---|
| HAZ | (Mean ± SD) * | 0.4 ± 1.93 | 0.4 ± 2 | 0.4 ± 1.85 | 0.059 |
| HAZ | (n = 179) | (n = 107) | (n = 72) | 0.026 | |
| Normal | 158 (88.2) | 92 (86) | 66 (91.7) | ||
| Stunting (HAZ < −2 SD to −3 SD) | 15 (8.4) | 9 (8.4) | 6 (8.3) | ||
| Severe Stunting (HAZ < −3 SD) | 6 (3.4) | 6 (5.6) | 0 (0) | ||
| WHZ | (Mean ± SD) | 0.5 ± 1.76 | 0.4 ± 1.67 | 0.5 ± 1.89 | 1 |
| WHZ | (n = 179) | (n = 105) | (n = 74) | 0.093 | |
| Normal | 118 (65.9) | 73 (69.5) | 45 (60.7) | ||
| Wasting (HAZ < −2 SD to −3 SD) | 12 (6.7) | 7 (6.7) | 5 (6.8) | ||
| Severe Wasting (HAZ < −3 SD) | 3 (1.7) | 2 (1.9) | 1 (1.4) | ||
| Overweight (HAZ > 2 SD) | 30 (16.8) | 15 (14.3) | 15 (20.3) | ||
| Obese (HAZ > 3 SD) | 16 (8.9) | 8 (7.6) | 8 (10.8) | ||
| WAZ | (Mean ± SD) | 0.6 ± 1.17 | 0.6 ± 1.09 | 0.7 ± 1.27 | 0.028 |
| WAZ | (n = 184) | (n = 109) | (n = 75) | 0.795 | |
| Normal | 183 (99.5) | 109 (100) | 74 (98.7) | ||
| Underweight (HAZ < −2 SD to −3 SD) | 1 (0.5) | 0 (0) | 1(1.3) | ||
| Feeding patterns | |||||
| Ever breastfeeding | (n = 511) | (n = 281) | (n = 230) | 0.226 | |
| Yes | 486 (95.1) | 270 (96.1) | 216 (94.1) | ||
| No | 25 (4.9) | 11 (3.9) | 14 (5.9) | ||
| Exclusive breastfeeding | (n = 486) | (n = 270) | (n = 216) | 0.243 | |
| <6 months | 287 (59.1) | 166 (61.5) | 121 (56.1) | ||
| >6 months | 199 (40.9) | 104 (38.5) | 95 (43.9) | ||
| Continued breastfeeding | (n = 511) | (n = 281) | (n = 230) | 0.034 | |
| >12 months | 97 (19) | 53 (18.9) | 44 (19) | ||
| Bottle feeding | (n = 511) | (n = 282) | (n = 229) | 0.716 | |
| Yes | 285 (55.8) | 155 (55.1) | 130 (56.7) | ||
| No | 226 (44.2) | 127 (45) | 99 (43.3) | ||
| Initiation of bottle feeding | (n = 511) | (n = 281) | (n = 230) | 0.073 | |
| At birth | 132 (25.8) | 68 (24.1) | 64 (27.8) | ||
| <1 month | 102 (20.3) | 64 (22.9) | 38 (16.7) | ||
| <6 months | 70 (13.6) | 34 (12) | 36 (15.5) | ||
| 6–12 months | 37 (7.3) | 26 (9.3) | 11 (4.7) | ||
| >12 months | 37 (7.1) | 23 (8.1) | 14 (5.9) | ||
| No initiation of bottle feeding | 133 (26.2) | 66 (23.6) | 67 (29.4) | ||
| Feeding pattern since birth | (n = 511) | (n = 281) | (230) | 0.415 | |
| Breastfeeding only | 337 (65.9) | 191 (67.9) | 146 (63.5) | ||
| Bottle feeding only | 25 (5.1) | 11 (4.1) | 15 (6.3) | ||
| Mixed milk feeding: breastfeeding + bottle feeding | 148 (29) | 79 (28) | 69 (30.2) | ||
| Introduction of solid, semi-solid or soft foods | (n = 373) | (n = 213) | (n = 160) | 0.008 | |
| At 4 months | 55 (14.8) | 31 (14.4) | 24 (15.4) | ||
| 4–6 months (6 not included) | 138 (37) | 64 (30.1) | 74 (46.1) | ||
| At 6 months | 176 (47.1) | 115 (53.9) | 61 (38) | ||
| >1 year | 4 (1.1) | 3 (1.6) | 1 (0.5) | ||
| Study Variables | Breastfeeding (n = 511) | Exclusive Breastfeeding (n = 486) | Bottle Feeding (n = 511) | Complementary Feeding (n = 373) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Yes (n = 486) | No (n = 25) | p-Value | n | <6 Months (n = 287) | ≥6 Months (n = 199) | p-Value | n | Yes (n = 285) | No (n = 226) | p-Value | n | <6 Months (n = 193) | ≥6 Months (n = 180) | p-Value | |
| n (%) + | n (%) + | n (%) + | n (%) + | n (%) + | n (%) + | n (%) + | n (%) + | |||||||||
| Gender of the younger children | 511 | 0.305 | 486 | 0.266 | 285 | 372 | 0.001 | |||||||||
| Boy | 216 (93.9) | 14 (6.1) | 121 (56.2) | 94 (43.7) | 130 (56.5) | 100 (43.5) | 98 (61.6) | 61 (38.4) | ||||||||
| Girl | 270 (96.1) | 11 (3.9) | 166 (61.3) | 105 (38.7) | 155 (55.2) | 126 (44.8) | 0.758 | 95 (44.6) | 118 (55.4) | |||||||
| Number of children | 511 | 0.195 | 486 | 0.490 | ||||||||||||
| 1 or 2 child | 390 (94.4) | 23 (5.6) | 233 (59.7) | 157 (40.3) | ||||||||||||
| 3 or more child | 96 (98.0) | 2 (2.0) | 54 (56.2) | 42 (43.8) | ||||||||||||
| Governorate | 511 | 0.005 | 486 | 0.181 | 294 | 0.071 | 372 | 0.864 | ||||||||
| Beirut and Mount Lebanon | 278 (96.5) | 10 (3.5) | 162 (58.3) | 116 (41.7) | 157 (54.5) | 131 (45.5) | 108 (51.2) | 103 (48.8) | ||||||||
| North and Akkar | 110 (89.4) | 14 (10.6) | 65 (59.1) | 45 (40.9) | 79 (56.5) | 54 (43.5) | 47 (51.6) | 44 (48.4) | ||||||||
| Beqaa and Baalbeck/Hermel | 39 (100.0) | 0 (0.0) | 29 (74.4) | 10 (25.6) | 29 (74.4) | 10 (25.6) | 16 (59.3) | 11 (40.7) | ||||||||
| South and Nabatieh | 36 (95.3) | 24 (4.7) | 31 (52.5) | 28 (47.5) | 29 (48.3) | 31 (51.7) | 21 (48.8) | 22 (51.2) | ||||||||
| Family income | 510 | 0.230 | 486 | 0.010 | 285 | 0.386 | 372 | 0.102 | ||||||||
| Less than 750,000 LBP | 42 (95.5) | 2 (4.5) | 30 (71.4) | 12 (28.6) | 24 (54.5) | 20 (45.5) | 10 (34.5) | 19 (65.5) | ||||||||
| Between 750,000 LBP and 2,250,000 LBP | 286 (94.1) | 18 (5.9) | 178 (62.2) | 108 (37.8) | 177 (58.2) | 127 (41.8) | 112 (51.6) | 105 (48.4) | ||||||||
| More than 2,250,000 LBP | 158 (97.5) | 4 (2.5) | 79 (50.0) | 79 (50.0) | 84 (51.5) | 79 (48.5) | 71 (56.3) | 55 (43.7) | ||||||||
| Education of the husband | 511 | 0.725 ++ | 486 | 0.001 ++ | 285 | 0.059 ++ | 372 | 0.185 ++ | ||||||||
| Illiterate | 3 (100.0) | 0 (0.0) | 1 (33.3) | 2 (66.7) | 3 (100.0) | 0 (0.0) | 2 (66.7) | 1 (33.3) | ||||||||
| School level | 221 (94.8) | 12 (5.2) | 149 (67.4) | 72 (32.6) | 139 (59.7) | 94 (40.3) | 92 (56.4) | 71 (43.6) | ||||||||
| University level | 263 (95.6) | 12 (4.4) | 137 (52.3) | 125 (47.7) | 143 (52.0) | 132 (48.0) | 98 (47.6) | 108 (52.4) | ||||||||
| Mother currently working | 219 | 206 (94) | 13 (6) | 0.344 | 206 | 127 (61.7) | 79 (38.3) | 0.318 | 219 | 136 (62.1) | 83 (37.9) | 0.013 | 92 | 56 (60.9) | 36 (39.1) | 0.159 |
| Mother as healthcare worker | 56 | 48 (85.7) | 8 (14.3) | 0.003 | 48 | 31 (64.6) | 17 (35.4) | 0.569 | 56 | 43 (76.8) | 13 (23.2) | 0.002 | 44 | 26 (59.1) | 18 (40.9) | 0.334 |
| Mother has twins or triplets | 26 | 23 (88.5) | 3 (11.5) | 0.128 | 23 | 21 (91.3) | 2 (8.7) | 0.002 | 25 | 22 (88.0) | 3 (12.0) | 0.001 | 19 | 9 (47.4) | 10 (52.6) | 0.815 |
| Mother breastfed as a baby | 406 | 393 (96.8) | 13 (3.2) | 0.001 ++ | 393 | 237 (60.3) | 156 (39.7) | 0.378 | 407 | 228 (56.0) | 179 (44.0) | 0.890 | 292 | 152 (52.1) | 140 (47.9) | 0.578 |
| Paediatrician favoured breastfeeding | 390 | 372 (95.4) | 18 (4.6) | 0.034 ++ | 373 | 216 (57.9) | 157 (42.1) | 0.497 | 390 | 208 (53.3) | 182 (46.7) | 0.111 | 287 | 146 (50.9) | 141 (49.1) | 0.917 |
| Husband favoured breastfeeding | 360 | 354 (98.3) | 6 (1.7) | <0.001 | 354 | 186 (52.5) | 168 (47.5) | <0.001 | 359 | 172 (47.9) | 187 (52.1) | <0.001 | 256 | 132 (51.6) | 124 (48.4) | 0.918 |
| Family supported breastfeeding | 379 | 370 (97.6) | 9 (2.4) | <0.001 | 370 | 206 (55.7) | 164 (44.3) | 0.009 | 379 | 200 (52.8) | 179 (47.2) | 0.025 | 269 | 132 (49.1) | 137 (50.9) | 0.132 |
| Baby breastfed at hospital | 483 | 465 (96.3) | 18 (3.7) | <0.001 | 457 | 265 (58.0) | 192 (42.0) | 0.125 | 463 | 253 (54.6) | 210 (45.4) | 0.128 | 334 | 176 (52.7) | 158 (47.3) | 0.234 |
| Mother with COVID-19 history | 511 | 117 (95.1) | 6 (4.9) | 0.993 | 486 | 66 (56.4) | 51 (43.6) | 0.505 | 123 | 78 (63.4) | 45 (36.6) | 0.05 | 92 | 56 (60.9) | 36 (39.1) | 0.041 |
| Age of the younger child | 275 | 0.375 | 362 | 0.188 | ||||||||||||
| [0–6] months | 72 (58.1) | 52 (41.9) | 40 (64.5) | 22 (35.5) | ||||||||||||
| [6–12] months | 56 (53.3) | 49 (46.7) | 47 (48.5) | 50 (51.5) | ||||||||||||
| [1–3] years | 94 (52.5) | 85 (47.5) | 72 (49.7) | 73 (50.3) | ||||||||||||
| [3–5] years | 53 (63.1) | 31 (36.9) | 29 (50.0) | 29 (50.0) | ||||||||||||
| Baby age when stopping breastfeeding | 274 | <0.001 | 362 | 0.050 | ||||||||||||
| Less than 6 months | 144 (91.1) | 14 (8.9) | 78 (58.6) | 55 (41.4) | ||||||||||||
| 6 months and more | 130 (38.3) | 209 (61.7) | 109 (47.6) | 120 (52.4) | ||||||||||||
| Baby fed infant formula at hospital | 185 | 114 (61.6) | 71 (38.4) | <0.001 | ||||||||||||
| Model 1. Logistic regression taking breastfeeding (Yes vs. No (reference)) as the dependent variable (n = 511) | ||
| aOR (95% CI) | p-value | |
| Current residency (North and Akkar) | 0.31 (0.13–0.71) | 0.006 |
| Mother breastfed as a baby | 4.43 (1.90–10.33) | 0.001 |
| Healthcare worker mother | 0.18 (0.55–0.58) | 0.004 |
| Family supporting breastfeeding | 5.46 (2.34–12.75) | <0.001 |
| Husband supporting breastfeeding | 8.84 (3.38–23.10) | <0.001 |
| Baby breastfed at hospital | 8.20 (3.03–22.17) | <0.001 |
| Variables entered in the model: Current residency, healthcare worker mother, mother breastfed as a baby, paediatrician supporting breastfeeding, husband supporting breastfeeding, family supported breastfeeding, baby breastfed at hospital | ||
| Model 2. Logistic regression taking exclusive breastfeeding (<6 months (reference) vs. ≥ 6 months) as the dependent variable (n = 486) | ||
| aOR (95% CI) | p-value | |
| Mother having twins or triplets | 0.14 (0.29–0.71) | 0.018 |
| Husband supporting breastfeeding | 3.07 (1.90–4.92) | <0.001 |
| Variables entered in the model: Husband supporting breastfeeding, family supporting breastfeeding, family income, having twins or triplets, educational level of the husband. | ||
| Model 3. Logistic regression taking the bottle feeding (Yes vs. No (reference)) as the dependent variable (n = 511) | ||
| aOR (95% CI) | p-value | |
| Husband supporting breastfeeding | 0.39 (0.18–0.84) | 0.017 |
| Baby age when fully weaned (>6 months) | 0.007 (0.001–0.084) | <0.001 |
| Variables entered in the model: Occupation of the mother, health care worker mother, husband supporting breastfeeding, baby age when fully weaned, family supporting breastfeeding, mother breastfed as a baby, mother with COVID-19 history. | ||
| Model 4. Logistic regression taking the age of introduction of complementary foods (before 6 months (reference) vs. At 6 months and more) as the dependent variable (n = 373) | ||
| aOR (95% CI) | p-value | |
| Baby gender (Male) | 2.119 (1.37–3.27) | 0.001 |
| Baby fed infant formula at hospital | 0.5 (0.32–0.77) | 0.02 |
| Mother with COVID-19 history | 0.58 (0.35–0.95) | 0.032 |
| Variables entered in the model: Baby gender, baby fed infant formula at hospital, mother with COVID-19 history. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoteit, M.; Ibrahim, C.; Saadeh, D.; Al-Jaafari, M.; Atwi, M.; Alasmar, S.; Najm, J.; Sacre, Y.; Hanna-Wakim, L.; Al-Jawaldeh, A. Correlates of Sub-Optimal Feeding Practices among under-5 Children amid Escalating Crises in Lebanon: A National Representative Cross-Sectional Study. Children 2022, 9, 817. https://doi.org/10.3390/children9060817
Hoteit M, Ibrahim C, Saadeh D, Al-Jaafari M, Atwi M, Alasmar S, Najm J, Sacre Y, Hanna-Wakim L, Al-Jawaldeh A. Correlates of Sub-Optimal Feeding Practices among under-5 Children amid Escalating Crises in Lebanon: A National Representative Cross-Sectional Study. Children. 2022; 9(6):817. https://doi.org/10.3390/children9060817
Chicago/Turabian StyleHoteit, Maha, Carla Ibrahim, Danielle Saadeh, Marwa Al-Jaafari, Marwa Atwi, Sabine Alasmar, Jessica Najm, Yonna Sacre, Lara Hanna-Wakim, and Ayoub Al-Jawaldeh. 2022. "Correlates of Sub-Optimal Feeding Practices among under-5 Children amid Escalating Crises in Lebanon: A National Representative Cross-Sectional Study" Children 9, no. 6: 817. https://doi.org/10.3390/children9060817
APA StyleHoteit, M., Ibrahim, C., Saadeh, D., Al-Jaafari, M., Atwi, M., Alasmar, S., Najm, J., Sacre, Y., Hanna-Wakim, L., & Al-Jawaldeh, A. (2022). Correlates of Sub-Optimal Feeding Practices among under-5 Children amid Escalating Crises in Lebanon: A National Representative Cross-Sectional Study. Children, 9(6), 817. https://doi.org/10.3390/children9060817