
Social Humanoid Robots for Children with Autism Spectrum Disorders: A Review of Modalities, Indications, and Pitfalls


 ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Social Humanoid Commercial Robots
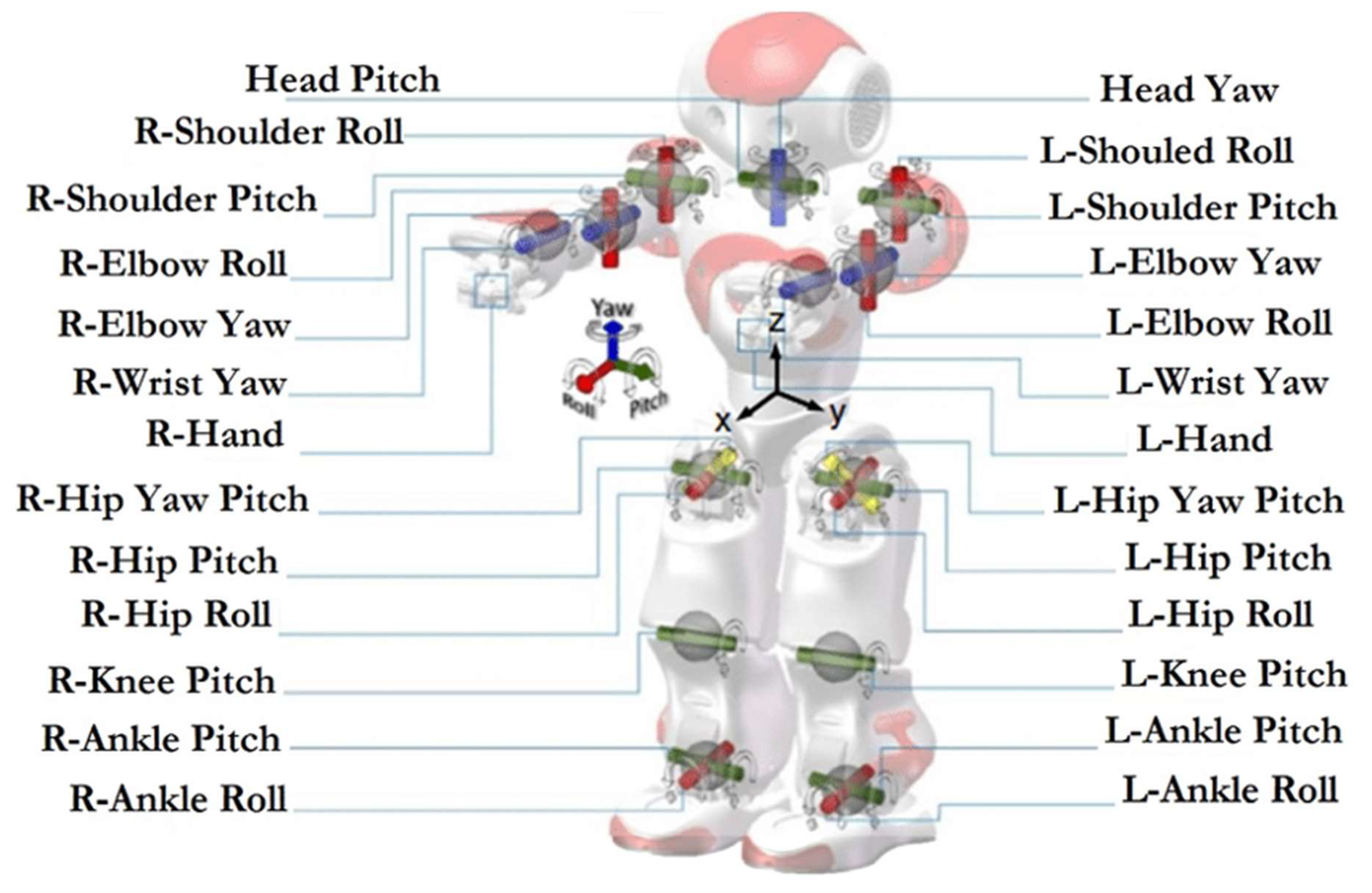
2.1. NAO Robot
- Sonar to interpret the distance to objects or subjects.
- Tactile sensors on the hands and head.
- A camera (two OV5640 2592 × 1944) and microphones for voice and facial recognition.
- Speakers to listen to sounds that can be reproduced by the robot itself.
- Stepper-motors to represent the robot’s movements.
- Stepper-motors (see Figure 1) that allow movements very similar to a human being’s prehensile hands.
- An ethernet and wireless network card.
2.1.1. NAO: Clinical Validation
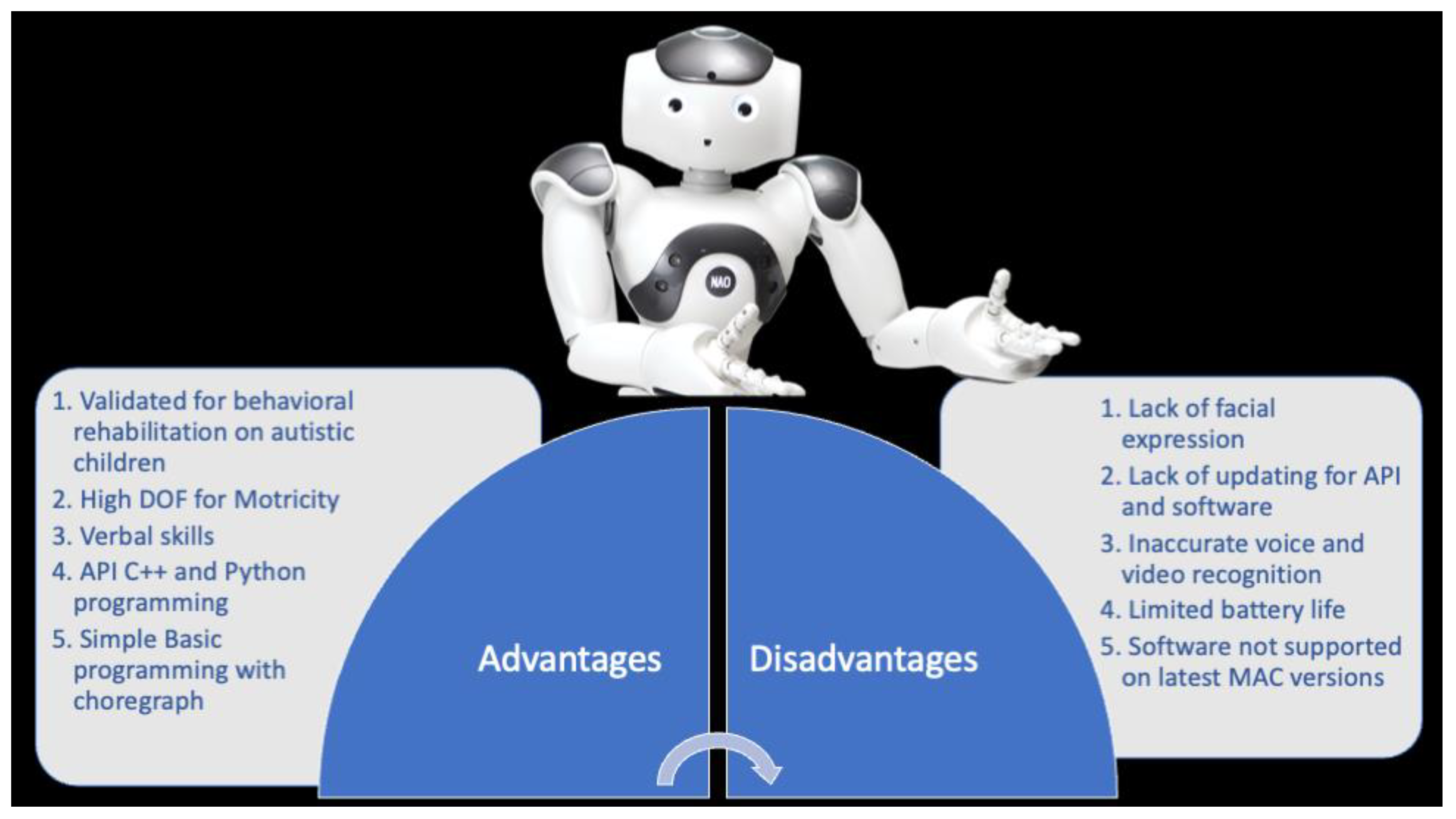
2.1.2. NAO: Advantages vs. Disadvantages
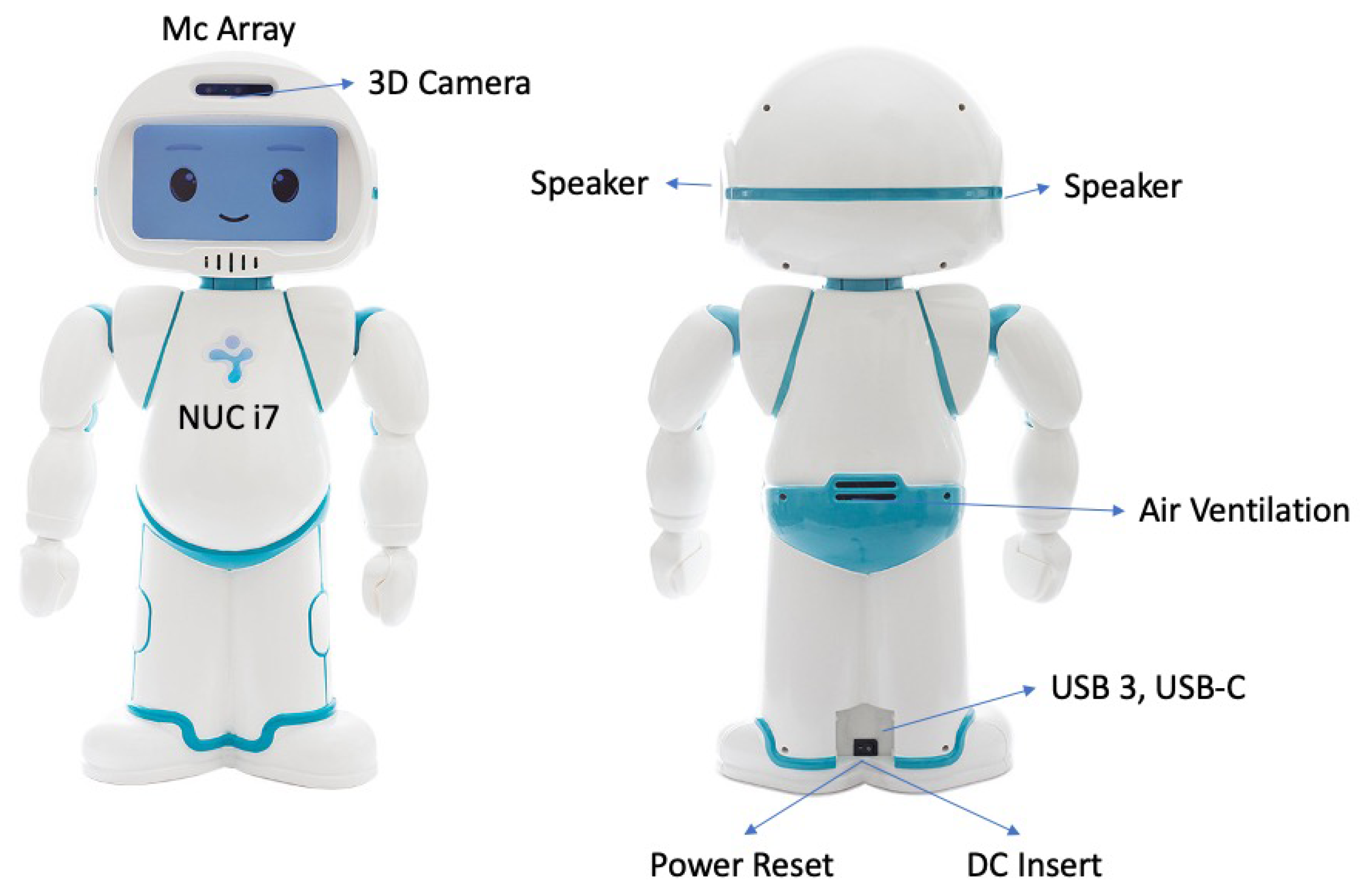
2.2. QTrobot
- An 8th Gen quad-core Intel® CoreTM i5/i7 processor up to 4 × 4.5 GHz, up to 32 GB DDR4 RAM, and up to 512 GB M.2 SSD.
- A camera (RealSenseTM depth camera D435; field of view ≈ 87° × 58° × 95°) and microphones (four digital microphones; supports far-field voice capture; microphones: ST MP34DT01TR-M; sensitivity: −26 dBFS) for voice and facial recognition.
- Speakers to listen to sounds that can be reproduced by the robot itself (audio amplifier: stereo 2.8 W Class D; speaker frequency rate: 800~7000 Hz).
- Facial Display (8 inch TFT 800 × 480 LCD).
- An ethernet and wireless network card.
2.2.1. QTrobot: Clinical Validation
2.2.2. Qtrobot: Advantages vs. Disadvantages
2.3. KASPAR
- SENSORS Cameras in eyes. Force-sensing resistor or capacitive touch sensors.
- ACTUATORS Dynamixel AX-12A robot servos and RC servos.
- POWER One 12-V 7-Ah lead acid battery, 4 hours of operation.
- COMPUTING Controlled by external PC via USB. Or wirelessly using on-board mini PC.
- SOFTWARE Custom Java software. YARP, C++, and Python interfaces optional.
- DEGREES OF FREEDOM (DOF) 17 (Arm: 4 DoF x 2; Neck: 3 DoF; Mouth: 2 DoF; Eyes: 2 DoF; Eyelids: 1 DoF; Torso: 1 DoF)
- MATERIALS Fiberglass body; aluminum frame and head parts; silicone rubber face.
2.3.1. KASPAR: Clinical Validation
2.3.2. KASPAR: Advantages vs. Disadvantages
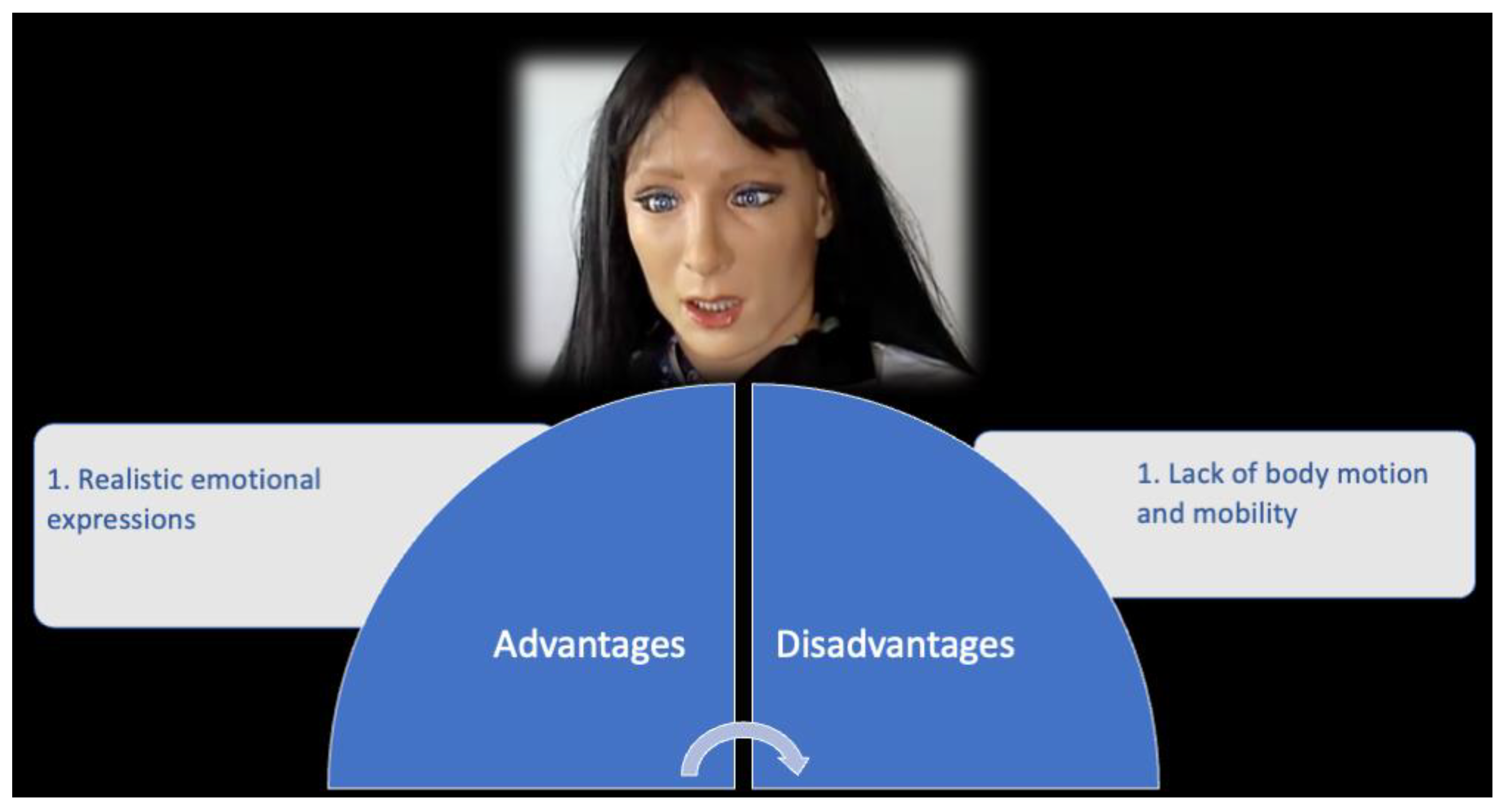
2.4. FACE (Facial Automaton for Conveying Emotions)
- SENSORS External cameras and microphones positioned next to the android (used for teleoperation).
- ACTUATORS Pneumatic actuators in the face (eyes, forehead, eyebrows, eyelids, and cheeks) and body (neck and shoulder).
- POWER Standard 110-V/220-V power supply
- COMPUTING Custom server and control infrastructure
- SOFTWARE Windows OS and Java-based application
- DEGREES OF FREEDOM (DOF) 12
- MATERIALS Metal skeleton, silicone skin for hands and face, wig made of human and artificial hair.
2.4.1. FACE: Clinical Validation
2.4.2. FACE: Advantages vs. Disadvantages
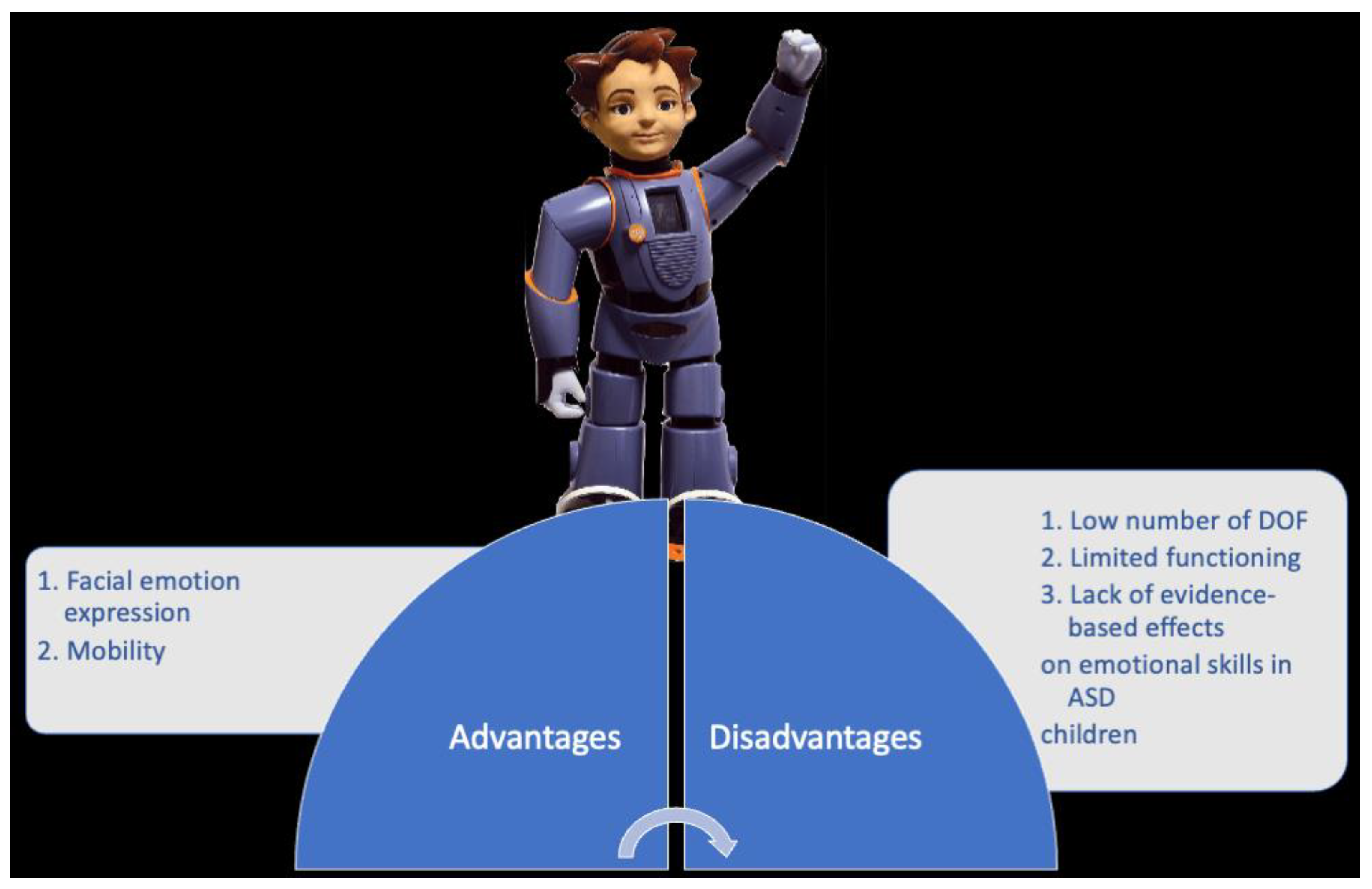
2.5. ZENO
- SENSORSvTwo 720p, 30fps HD cameras (one in each motorized eye).
- Three-axis gyroscope, three-axis accelerometer, compass.
- Twenty one joint load sensors, 30 joint position sensors, two cliff sensors, two ground contact sensors, two infrared obstacle-detection sensors, two bump sensors (feet), grip-load sensors in the hands. Three microphones.
- ACTUATORS Three Cirrus CS-101 STD 4-gram micro servos. Five Hitec HS-65MG motors (Frubber actuators). Dynamixel RX-64 (legs, hips, shoulders). Dynamixel RX-28 servos (waist).
- POWER Two 18.5-V lithium-ion batteries, 1 hour of operation
- COMPUTING 1 GHz Vortex86DX CPU, 1 GB RAM, Wi-Fi, Ethernet
- SOFTWARE Linux Ubuntu
- DEGREES OF FREEDOM (DOF) 36 (Arms: 12 DoF; Legs: 12 DoF; Waist: 1 DoF; Neck: 3 DoF; Face: 8 DoF)
- MATERIALS Frubber, plastic, and aluminum
2.5.1. ZENO: Clinical Validation
2.5.2. ZENO: Advantages vs. Disadvantages
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Sharma, S.R.; Gonda, X.; Tarazi, F.I. Autism Spectrum Disorder: Classification, diagnosis and therapy. Pharmacol. Ther. 2018, 190, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Leekam, S. Social cognitive impairment and autism: What are we trying to explain? Philos. Trans. R Soc. Lond. B Biol. Sci. 2016, 371, 20150082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkovits, L.; Eisenhower, A.; Blacher, J. Emotion regulation in young children with autism spectrum disorders. J. Autism Dev. Disord. 2017, 47, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Maglione, M.A.; Gans, D.; Das, L.; Timbie, J.; Kasari, C.; Technical Expert Panel; HRSA Autism Intervention Research—Behavioral (AIR-B) Network. Nonmedical interventions for children with ASD: Recommended guidelines and further research needs. Pediatrics 2012, 130, S169–S178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quirmbach, L.M.; Lincoln, A.J.; Feinberg-Gizzo, M.J.; Ingersoll, B.R.; Andrews, S.M. Social stories: Mechanisms of effectiveness in increasing game play skills in children diagnosed with autism spectrum disorder using a pretest posttest repeated measures randomized control group design. J. Autism Dev. Disord. 2009, 39, 299–321. [Google Scholar] [CrossRef]
- Sartorato, F.; Przybylowski, L.; Sarko, D.K. Improving therapeutic outcomes in autism spectrum disorders: Enhancing social communication and sensory processing through the use of interactive robots. J. Psychiatr. Res. 2017, 90, 1–11. [Google Scholar] [CrossRef]
- Pennisi, P.; Tonacci, A.; Tartarisco, G.; Billeci, L.; Ruta, L.; Gangemi, S.; Pioggia, G. Autism and social robotics: A systematic review. Autism Res. 2016, 9, 165–183. [Google Scholar] [CrossRef]
- Yun, S.S.; Choi, J.; Park, S.K.; Bong, G.Y.; Yoo, H. Social skills training for children with autism spectrum disorder using a robotic behavioral intervention system. Autism Res. 2017, 10, 1306–1323. [Google Scholar] [CrossRef]
- Provoost, S.; Lau, H.M.; Ruwaard, J.; Riper, H. Embodied conversational agents in clinical psychology: A scoping review. J. Med. Internet Res. 2017, 19, 6553. [Google Scholar] [CrossRef] [Green Version]
- Saleh, M.A.; Hanapiah, F.A.; Hashim, H. Robot applications for autism: A comprehensive review. Disabil. Rehabil. Assist. Technol. 2021, 16, 580–602. [Google Scholar] [CrossRef] [PubMed]
- Marino, F.; Chilà, P.; Sfrazzetto, S.T.; Carrozza, C.; Crimi, I.; Failla, C.; Busà, M.; Bernava, G.; Tartarisco, G.; Vagni, D.; et al. Outcomes of a Robot-Assisted Social-Emotional Understanding Intervention for Young Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2020, 50, 1973–1987. [Google Scholar] [CrossRef] [PubMed]
- van den Berk-Smeekens, I.; de Korte, M.W.; van Dongen-Boomsma, M.; Oosterling, I.J.; den Boer, J.C.; Barakova, E.I.; Lourens, T.; Glennon, J.C.; Staal, W.G.; Buitelaar, J.K. Pivotal Response Treatment with and without robot-assistance for children with autism: A randomized controlled trial. Eur. Child. Adolesc. Psychiatry 2021, 9, 79. [Google Scholar] [CrossRef] [PubMed]
- Scassellati, B.; Admoni, H.; Matarić, M. Robots for use in autism research. Annu. Rev. Biomed. Eng. 2012, 14, 275–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huijnen, C.A.G.J.; Lexis, M.A.S.; Jansens, R.; de Witte, L.P. Mapping Robots to Therapy and Educational Objectives for Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2016, 46, 2100–2114. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.P.; Myers, S.M.; American Academy of Pediatrics Council on Children With Disabilities. Identification and evaluation of children with autism spectrum disorders. Pediatrics 2007, 120, 1183–1215. [Google Scholar] [CrossRef] [Green Version]
- Fabio, R.A.; Esposito, S.; Carrozza, C.; Pino, G.; Caprì, T. Correlations between facial emotion recognition and cognitive flexibility in autism spectrum disorder. Adv. Autism 2020, 6, 95–204. [Google Scholar] [CrossRef]
- Woo, H.; LeTendre, G.K.; Pham-Shouse, T.; Xiong, Y. The Use of Social Robots in Classrooms: A Review of Field-based Studies. Educ. Res. Rev. 2021, 33, 100–388. [Google Scholar] [CrossRef]
- Estévez, D.; Terrón-López, M.-J.; Velasco-Quintana, P.J.; Rodríguez-Jiménez, R.-M.; Álvarez-Manzano, V. A Case Study of a Robot-Assisted Speech Therapy for Children with Language Disorders. Sustainability 2021, 13, 2771. [Google Scholar] [CrossRef]
- Tleubayev, B.; Zhexenova, Z.; Zhakenova, A.; Sandygulova, A. Robot-assisted therapy for children with ADHD and ASD: A pilot study. In Proceedings of the 2019 2nd International Conference on Service Robotics Technologies, ICSRT, Beijing, China, 22−24 March 2019. [Google Scholar]
- Real, M.J.; Ochoa, A.; Escobedo, D.; Estrada-Medrano, R.; Martínez, E.; Maciel, R.; Larios-Rosillo, V.M. Recognition of Colors through Use of a Humanoid Nao Robot in Therapies for Children with Down Syndrome in a Smart City. Res. Comput. Sci. 2019, 148, 239–252. [Google Scholar]
- Costa, A.; Kirsten, L.; Charpiot, L.; Steffgen, G. Mental health benefits of a robot-mediated emotional ability training for children with autism: An exploratory study. In Proceedings of the IEEE International Symposium on Robot and Human Interactive Communication (RO-MAN), Montreal, QC, Canada, 1 May 2019. [Google Scholar]
- Costa, A.P.; Charpiot, L.; Lera, F.J.; Ziafati, P.; Nazarikhorram, A.; van der Torre, L.; Steffgen, G. More Attention and Less Repetitive and Stereotyped Behaviors using a Robot with Children with Autism. In Proceedings of the 27th IEEE International Symposium on Robot and Human Interactive Communication (RO-MAN), Chicago, IL, USA, 5 March 2018. [Google Scholar]
- Duquette, A.; Michaud, F.; Mercier, H. Exploring the use of a mobile robot as an imitation agent with children with low-functioning autism. Auton. Robot. 2008, 24, 147–157. [Google Scholar] [CrossRef]
- Feil-Seifer, D.; Mataric’, M. Robot-assisted therapy for children with autism spectrum disorders. In Proceedings of the 7th International Conference on Interaction Design and Children, Chicago, IL, USA, 11−13 June 2008. [Google Scholar]
- Kozima, H.; Yano, H. A robot that learns to communicate with human caregivers. In Proceedings of the First International Workshop on Epigenetic Robotics, Lund, Sweden, 17−18 September 2001. [Google Scholar]
- Melo, M.; Mota, F.; Albuquerque, V.; Alexandria, A. Development of a Robotic Airboat for Online Water Quality Monitoring in Lakes. Robotics 2019, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Marinoiu, E.; Zanfir, M.; Olaru, V.; Sminchisescu, C. 3D human sensing, action and emotion recognition in robot assisted therapy of children with autism. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 2158–2167. [Google Scholar]
- Dautenhahn, K.; Nehaniv, C.L.; Walters, M.L.; Robins, B.; Kose-Bagci, H.; Assif, N.; Blow, M. KASPAR–a minimally expressive humanoid robot for human–robot interaction research. Appl. Bionics Biomech. 2009, 6, 369–397. [Google Scholar] [CrossRef] [Green Version]
- Robins, B.; Dautenhahn, K.; Boekhorst, R.T.; Billard, A. Robotic assistants in therapy and education of children with autism: Can a small humanoid robot help encourage social interaction skills? Univ. Access Inf. Soc. 2005, 4, 105–120. [Google Scholar] [CrossRef]
- Huijnen, C.A.G.J.; Lexis, M.A.S.; Jansens, R.; de Witte, L.P. Roles, Strengths and Challenges of Using Robots in Interventions for Children with Autism Spectrum Disorder (ASD). J. Autism Dev. Disord. 2019, 49, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Pioggia, G.; Sica, M.L.; Ferro, M.; Igliozzi, R.; Muratori, F.; Ahluwalia, A.; De Rossi, D. Human-robot interaction in autism: FACE, an android-based social therapy. In Proceedings of the RO-MAN 2007-the 16th IEEE International Symposium on Robot and Human Interactive Communication, Jeju, Korea, 26–29 August 2007. [Google Scholar]
- Pioggia, G.; Igliozzi, R.; Sica, M.L.; Ferro, M.; Muratori, F.; Ahluwalia, A.; De Rossi, D. Exploring emotional and imitational android-based interactions in autistic spectrum disorders. J. Cyber Ther. Rehabil. 2008, 1, 49–61. [Google Scholar]
- Mori, M. The uncanny valley. Energy 1970, 7, 33–35. [Google Scholar]
- Lecciso, F.; Levante, A.; Fabio, R.A.; Caprì, T.; Leo, M.; Carcagnì, P.; Distante, C.; Mazzeo, P.L.; Spagnolo, P.; Petrocchi, S. Emotional Expression in Children With ASD: A Pre-Study on a Two-Group Pre-Post-Test Design Comparing Robot-Based and Computer-Based Training. Front. Psychol. 2021, 12, 678052. [Google Scholar] [CrossRef]
- McCleery, J.P. Comment on Technology-Based Intervention Research for Individuals on the Autism Spectrum. J. Autism Dev. Disord. 2015, 45, 3832–3835. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puglisi, A.; Caprì, T.; Pignolo, L.; Gismondo, S.; Chilà, P.; Minutoli, R.; Marino, F.; Failla, C.; Arnao, A.A.; Tartarisco, G.; et al. Social Humanoid Robots for Children with Autism Spectrum Disorders: A Review of Modalities, Indications, and Pitfalls. Children 2022, 9, 953. https://doi.org/10.3390/children9070953
Puglisi A, Caprì T, Pignolo L, Gismondo S, Chilà P, Minutoli R, Marino F, Failla C, Arnao AA, Tartarisco G, et al. Social Humanoid Robots for Children with Autism Spectrum Disorders: A Review of Modalities, Indications, and Pitfalls. Children. 2022; 9(7):953. https://doi.org/10.3390/children9070953
Chicago/Turabian StylePuglisi, Alfio, Tindara Caprì, Loris Pignolo, Stefania Gismondo, Paola Chilà, Roberta Minutoli, Flavia Marino, Chiara Failla, Antonino Andrea Arnao, Gennaro Tartarisco, and et al. 2022. "Social Humanoid Robots for Children with Autism Spectrum Disorders: A Review of Modalities, Indications, and Pitfalls" Children 9, no. 7: 953. https://doi.org/10.3390/children9070953
APA StylePuglisi, A., Caprì, T., Pignolo, L., Gismondo, S., Chilà, P., Minutoli, R., Marino, F., Failla, C., Arnao, A. A., Tartarisco, G., Cerasa, A., & Pioggia, G. (2022). Social Humanoid Robots for Children with Autism Spectrum Disorders: A Review of Modalities, Indications, and Pitfalls. Children, 9(7), 953. https://doi.org/10.3390/children9070953